
Abstract
Apathy is a common feature of neurodegenerative disorders but is difficult to study in a clinical trial setting due to practical and conceptual barriers. Principal challenges include a paucity of data regarding apathy in these disorders, an absence of established diagnostic criteria, the presence of confounding factors (eg, coexisting depression), use of concomitant medications, and an absence of a gold-standard apathy assessment scale. Based on a literature search and ongoing collaboration among the authors, we present recommendations for the design of future clinical trials of apathy, suggesting Alzheimer disease and Parkinson disease as models with relevance across a wider array of neuropsychiatric disorders. Recommendations address clarification of the targeted study population (apathy diagnosis and severity at baseline), confounding factors (mood/cognition, behavior, and treatment), outcome measures, study duration, use of comparators and considerations around environment, and the role of the caregiver and patient assent. This review contributes to the search for an optimal approach to study treatment of apathy in neuropsychiatric disorders.
Introduction and Rationale
Apathy is a common and clinically significant neuropsychiatric syndrome frequently reported in neurological and psychiatric disorders including mild cognitive impairment (MCI), Alzheimer disease (AD), Parkinson disease (PD), Huntington disease, stroke, multiple sclerosis, traumatic brain injury, progressive supranuclear palsy, frontotemporal dementia, schizophrenia, and major depression. 1,2 The study of apathy in neuropsychiatric diseases is problematic due to a number of inherent practical and conceptual challenges. This article recommends methods applicable to clinical trials of apathy treatments, suggests AD and PD as models that may have relevance across a wider range of neuropsychiatric disorders, and offers key recommendations for the design of clinical trials in this area.
There are a number of persuasive reasons to study apathy in AD and PD. Both AD and PD are relatively well-defined and common neurodegenerative conditions in the elderly individuals. An estimated 35.6 million people worldwide are reported to have dementia, 3 and an additional 7 to 10 million individuals live with PD. 4 Apathy is present in approximately 25% to 90% of patients with AD and 20% to 70% of patients with PD, 1,5 –9 indicating that many individuals have the consequences of apathy across these large populations.
There is a far larger body of literature concerning apathy in AD and PD relative to other neurodegenerative diseases. Indeed, most research concerning apathy in neurological disorders has focused on these 2 disorders 10,11 or on negative symptoms of schizophrenia, of which apathy (amotivation) is a core component.
Finally, a consistent relationship is reported between high levels of apathy in AD and PD and disease course. Higher levels of apathy are associated with poorer outcomes of cognition, 12 executive functioning, 13,14 functional abilities, 12,15 and caregiver burden. 2,16
Evidence for the effectiveness of pharmacological interventions in the treatment of apathy is mixed. Both methylphenidate 17 and acetylcholinesterase inhibitors 18 have demonstrated efficacy against apathy, while supportive data have been published for memantine, psychostimulants, antiglutamatergics, and dopaminergic agents. 1,19 –22 However, a systematic review of 35 studies showed that there is insufficient evidence that pharmacological treatment improves the symptoms of apathy in neurodegenerative disease. 23 No data published since publication of the review alters this conclusion.
A recent surge of interest in new potential therapeutic options for apathy has created an impetus for the development of a considered methodological approach to clinical trials. Such studies will need to conform to the robust principles of randomized trials.
This article offers key recommendations for the design of clinical studies investigating the management of apathy in AD and PD and, by extension, in a wider range of neuropsychiatric disorders.
Methodology
A semistructured literature search was conducted in the PubMed (Medline) database, followed by retrospective referencing from articles identified and further ad hoc exploratory review. Search terms were (1) motivation OR motivational OR apathy OR apathetic OR drive OR volition OR volitional OR passive OR passivity OR interest OR detachment OR fatigue AND “Alzheimer’s” and (2) motivation OR motivational OR apathy OR apathetic OR drive OR volition OR volitional OR passive OR passivity OR interest OR detachment OR fatigue OR “nonmotor symptoms” AND “Parkinson’s”.
In 2013, a meeting entitled “Methodological Considerations for Clinical Investigations of the Treatment of Apathy in Neurodegenerative Disorders” was convened as the culmination of a long-term collaboration among the authors. Systematic discussion on the key issues relating to the design of clinical trials in apathy led to a consensus on recommendations for future trials in the area. Subjects discussed included use of apathy diagnostic criteria and clinical trial design issues including management of confounding factors, patient populations, and outcome assessments. A review of the current regulatory environment was not included in the discussion.
This article represents the outcome of this process and contributes to the search for an optimal approach to study the treatment of apathy in neuropsychiatric disorders.
Challenges Associated With Studying Apathy in Neuropsychiatric Disorders
Several practical and conceptual difficulties are associated with conducting clinical trials to evaluate treatment effects on apathy in AD and PD. The principle challenges are described subsequently, while our proposed solutions are offered in Recommendations section.
Paucity of Data
Compared with the volume of clinical trials for motor disorders in PD and cognition impairment in AD, there are few randomized, controlled treatment studies reporting evaluations of apathy in AD and PD. Further, evaluation tools vary widely, meaning that “best practices” in this area are not established. The Apathy in Dementia Methylphenidate Trial (ADMET) study, which assessed the effects of methylphenidate on apathy in AD, is a good example of a methodologically sound approach to trials for the treatment of apathy in AD and was the starting point for discussions for the current publication. 17,24
Inconsistencies in Definition
A major challenge associated with the study of apathy in neurodegenerative diseases has been the lack of a consensus in the definition of terms and confusion over appropriate diagnostic criteria. For example, interchangeable use of the terms “amotivation,” “apathy,” “avolition,” and “flattened affect” make it difficult to determine whether the same construct is being investigated across studies. 25
Further, we do not know whether the underlying pathophysiology of apathy is the same across neurodegenerative and primary psychiatric disorders nor do we know whether these are clinically distinguishable. Phenomenologically, apathy has considerable overlap with negative symptoms of schizophrenia and is considered a core symptom, covering aspects of overt behavior, cognition, and emotion. 26
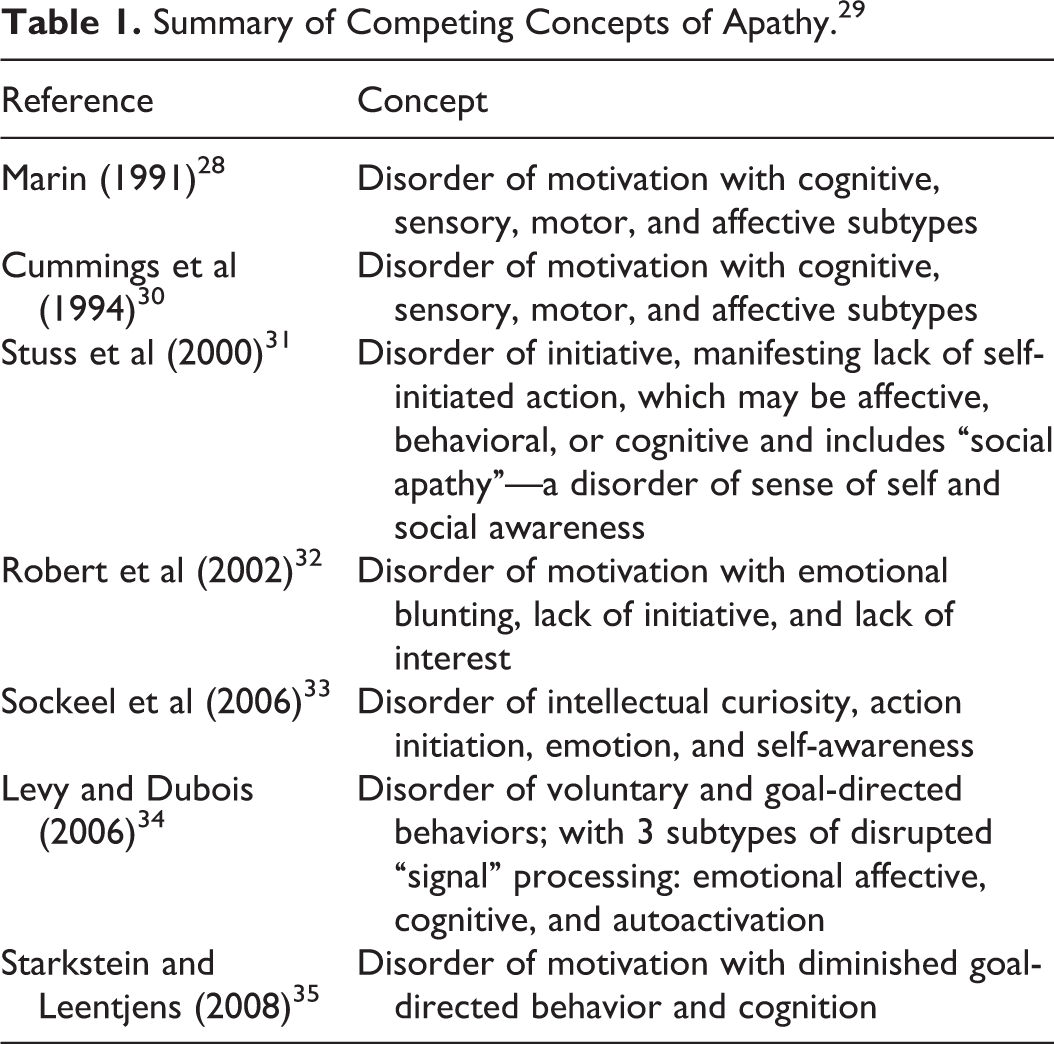
Although motivation is related to goal-directed behavior, 27 apathy comprises multiple dimensions such as interest, activity, motivation, and emotion. Lack of motivation is considered by many to be the most important component of the syndrome of apathy 11,28,29 (Table 1). Recently proposed diagnostic criteria 29 define “apathy” as a loss or diminution of goal-directed behavior, cognition, or emotion, which persists and is accompanied by functional impairment. 36
Summary of Competing Concepts of Apathy. 29
Inconsistencies and contradictions relating to definitions of terms have important implications in defining the preferred clinical trial population for a study of apathy. Recommendations given subsequently regarding the definition of apathy will assist in constructing uniform trial populations and will facilitate the evolution of better approaches.
Confounding Factors
Definitions of depression sometimes incorporate many features of apathy and may lead to overlap in the identification of depression and apathy in AD and PD, potentially confounding apathy assessment at both study entry and exit. Reported prevalence of depression (major or minor) ranges from ∼30% to 50% in AD 37 and ∼3% to 90% in PD. 9,38 –41 Prevalence of apathy in the absence of depression is reported to be between 9.4% and 25% in AD 12,42 and 14% in PD. 38 “Pure” apathy rates (absence of both depression and dementia) in PD are 5.2% and 8.2%, depending on the criteria used. 43,44
Although loss of motivation occurs in both apathy and depression, apathy is considered to be a loss of motivation without dysphoria. 45 Overlap between depression and apathy has been reported in both AD 15 and PD, 49 while Levy et al 8 demonstrated a significant correlation between apathy and depression in PD (r = .34; P = .03). Although the association between apathy and depression in AD is less clear, Starkstein et al 12 reported an unequal frequency of apathy based on the presence of depression (χ2 = 26.8, df = 2, P < .0001), with increased apathy significantly associated with both major and minor depression.
The Diagnostic and Statistical Manual of Mental Disorders (fifth edition; DSM-V) diagnosis of major depressive disorder (MDD) requires 1 or more of the 2 core criteria, that is, (1) depressed mood or (2) loss of interest or pleasure, and a total of at least 5 of the 9 listed symptoms (which include the 2 core symptoms). 46 Of these 9 symptoms, 4 could also be included as symptoms of apathy—change in interest, pleasure, activity, interest—which is itself a cardinal symptom of depression. 39 The DSM allows the diagnosis of depression in the absence of a depressed mood, provided that symptoms of loss of interest or anhedonia are present. 35 Similarly, the International Statistical Classification of Diseases, Tenth Revision and Related Health Problems states that patients with loss of interest but no depressed mood may still qualify for a diagnosis of mild or moderate depression provided they have decreased energy. These definitions may contribute to the high frequency of apparent cooccurrence of depression and apathy.
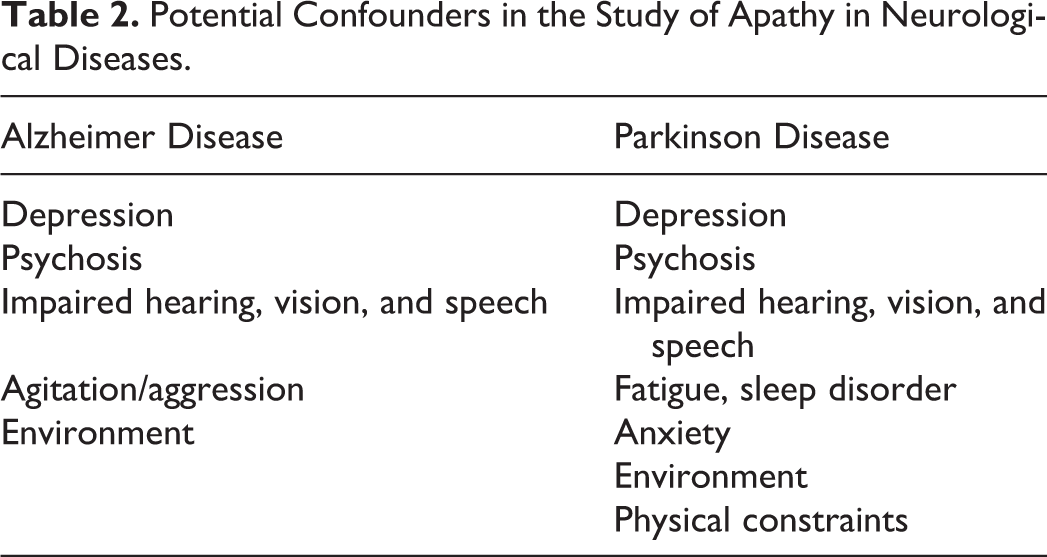
Other potential confounders are summarized in Table 2. Psychotic symptoms (including delusions and hallucinations) are common in AD and may be a significant risk factor for the development of apathy. 47,48 Although agitation may not be a “direct” confounding factor, an “indirect” confounding effect is plausible if patients with agitation (or psychosis) are less able to participate in describing apathy. In addition, agitation and aggression are common in severe AD, creating a potential threat to patients, caregivers, and study staff and possibly reducing the ability to record other symptoms.
Potential Confounders in the Study of Apathy in Neurological Diseases.
Absence of Gold-Standard Assessment Scales
There is currently no widely accepted gold-standard measurement scale for assessing apathy either in isolation or within the context of neuropsychiatric disorders. A number of rating scales have been developed, but most have shortcomings. Several of the rating scales have been adapted into alternative versions for the clinician’s assessment, the patient’s assessment, and the caregiver’s assessment. A clinician’s objective evaluation may be more valid than a patient’s self-rating, 17,49 while a caregiver may be able to provide a more accurate record of the frequency and duration of symptoms. However, caregivers may overestimate the capabilities of patients and ratings may be influenced by their own distress. 50
The 2 most widely used scales in this area are the Neuropsychiatric Inventory (NPI) and the Apathy Evaluation Scale (AES).
The NPI was developed for use in patients with dementia 25,30,51 and is based on responses from a structured interview with caregivers. The NPI assesses 10 or 12 behavioral domains common in dementia, including apathy and dysphoria/depression. Content validity, concurrent validity, inter-rater reliability, and test–retest reliability of the NPI have been established 51 for dementia. The apathy subscale (NPI-apathy) comprises a screening question and 8 subitems that are invoked following a positive response. 30,51 Frequency and severity of symptoms are rated as part of a single score, as well as caregiver distress which is scored separately. 51 A nursing-home version (NPI-NH), an abbreviated version for everyday clinical use (NPI-Q), 52 and a clinician-rated expanded version (NPI-C) 53 have also been developed. Although the NPI-C has been validated against the AES for measuring apathy, of all the domains, apathy had the weakest convergent validity (r = .31) 53 and there is limited experience in trials with this scale.
The AES was developed to assess the behavioral, cognitive, and emotional aspects of apathy. 54 In a recent trial, the AES was relatively insensitive to treatment effects compared with the NPI. 24 The scale comprises 18 core items that assess and quantify the affective, behavioral, and cognitive domains of apathy, with higher scores indicating more severe apathy. Versions for the ratings of clinicians (AES-C), caregivers (AES-I), and patients (AES-S) are available, as well as a 10-item short version of the AES (AES-10) created for use in nursing-home residents. 55
The AES was initially validated in individuals with AD, stroke, MDD, and healthy elderly individuals. 54 It demonstrated high inter-rater reliability and test–retest reliability; there was also a clear discrimination between apathy and depression, and apathy and anxiety on the AES-C and AES-S.
Other alternative measures include the apathy scale (AS) which was derived from the AES and has demonstrated good discriminant validity between apathy and depression in studies involving patients with AD, PD, and stroke. The Lille apathy rating scale (LARS) was chiefly designed for use in patients with PD 33 and has demonstrated good psychometric properties; it has a complex scoring system. 56 The Apathy Inventory is an assessment tool for use in patients with AD and PD, while the Motivation and Energy Inventory was designed for patients with MDD. 32,57 However, use in clinical trials is limited.
Other assessment tools developed for use in patients with neuropsychiatric disorders are less widely used or are not specific for apathy. In addition, these tools have often not been validated in the general population, diminishing their value in diagnosing clinically significant apathy and its changes over time or in response to treatment. Furthermore, the absence of agreed diagnostic definitions has hampered the ability to validate assessment scales in apathy.
Clinical Relevance of Treatment Effect
Because of the small number of randomized controlled trials (RCTs), there is still little consensus on what constitutes a clinically relevant effect in terms of the different assessment scales; statistical significance does not necessarily translate into a meaningful clinical benefit. Furthermore, even a clinically relevant symptomatic effect may not have a long-term effect on outcomes and quality of life (QoL). A prospective trial will need to consider the symptomatic clinical relevance and practical long-term outcome effect of any benefit.
Use of Concomitant Medications
Due to the nature of the target patient characteristics and associated disease states, most patients recruited for studies of apathy in neurodegenerative diseases will be receiving multiple concomitant medications that may be psychoactive. Typical concomitant therapies may include selective serotonin reuptake inhibitors (SSRIs), peripheral anticholinergic drugs (for overactive bladder), cholinesterase inhibitors, antipsychotics and other psychotropics, monoamine oxidase inhibitors (MAOIs), and dopaminergic agents.
Concomitant use of psychotropic drugs and psychostimulants may confound an apathy study, either by their direct effect on apathy or through their effects on confounding symptoms such as depression, and it is therefore important to take these into account when designing a trial.
Optimal Duration of Treatment
Optimal duration of treatment in any trial of apathy in neurodegenerative disorders must allow sufficient duration to observe any treatment effect while not over extending the study so that it is compromised by deterioration due to disease progression, subject attrition, or increasing measurement of variability.
Recommendations
Key challenges associated with designing RCTs to study apathy in neurological and psychiatric disorders are discussed in Challenges Associated With Studying Apathy in Neuropsychiatric Disorders section Recommendations section presents recommendations from the current group to address and overcome these challenges. The optimal trial design balances the necessary trade-offs between ideal trial design and study feasibility.
Study Population and Management of Confounders
Diagnosis of underlying neurological and psychiatric disorder
Entry criteria for trials in this area should include a confirmed diagnosis of established AD or PD, with some consideration of the stage of disease. In later disease states, the prevalence of apathy is higher which facilitates recruitment; however, advanced severity may be associated with practical challenges such as including nursing home residents in the trial.
The Mini-Mental State Examination (MMSE) has been widely used to define the level of cognitive impairment and is recommended as an entry criterion with appropriate cutoff values. Typical cutoffs for MMSE are as follows 58 : mild, MMSE >20; moderate, MMSE 20 to 11; severe, MMSE ≤10. Other approaches are generally minor variations of these cutoff definitions (eg, mild, MMSE ≥20; moderate, MMSE 19-10; and severe, MMSE ≤9) 59
Apathy studies in AD have defined cognitive impairment according to the following criteria:
Mild-moderate; that is, MMSE 10 to 26 inclusive 17,60,61 (NB Drye et al) 17 allowed scores above 26 on a case-by-case basis); MMSE ≥10 62 ; MMSE: 10 to 25 (NCT01047254).
Mild; that is, MMSE >18, but <29 (Study NCT00495820)
Mild-severe; that is, MMSE between 5 and 26, inclusive 64
Mild-moderately severe; that is, MMSE >9. 64
On this basis, a cutoff for mild-moderate AD of MMSE 26 to 15 is recommended as a reasonable severity range for most trials; trials of agents that may be of benefit in more advanced patients would adjust the MMSE range accordingly.
In PD trials, the inclusion of patients with and without dementia should be balanced by recruitment considerations.
This group recommends patients be recruited with mild-moderate AD (MMSE 26-15). It is also recommended that mild-moderate dementia in PD (MMSE 26-15) be allowed, but that when nondemented patients with PD are included, outcomes are stratified for dementia status (ie, PD dementia vs PD nondementia).
Apathy diagnosis
Consensus criteria for diagnosis of apathy have been established by an international task force, 29 as follows:
Loss of or diminished motivation in comparison to the patient’s previous level of functioning and which is not consistent with his age or culture. These changes in motivation may be reported by the patient himself or by the observations of others.
Presence of at least 1 symptom in at least 2 of the 3 following domains for a period of at least 4 weeks and present most of the time:
ACTION (loss of, or diminished, goal-directed behavior)
COGNITION (loss of, or diminished, goal-directed cognitive activity)
EMOTION (loss of, or diminished, emotion)
Impairments may reflect loss or diminution of self-initiated/spontaneous behaviors (eg, starting a conversation) or environmentally stimulated behaviors (responding to a conversation).
These symptoms (A-B) cause clinically significant impairment in personal, social, occupational, or other important areas of functioning.
The symptoms (A-B) are not exclusively explained or due to physical disabilities (eg, blindness and loss of hearing), to motor disabilities, to diminished level of consciousness or to the direct physiological effects of a substance (eg, drug of abuse, a medication).
These criteria were developed to correspond with the NPI-C and are a revision of earlier work by Marin et al 54 and Starkstein et al. 65 They have been validated in several disease areas 36,43 and show good inter-rater reliability, concurrent validity (against the NPI and LARS), and high acceptability among patients and clinicians. 36,66
From a practical perspective, these consensus criteria would need to be operationalized for use in a trial setting, and a structured clinical interview created similar to the Structured Interview for Apathy for use in research. 67 A proposal for how these criteria may be adapted and operationalized is provided in Table 3, using examples derived from the NPI-C apathy domain which have been developed specifically in parallel in order to fit with the apathy diagnostic criteria. 82
Proposed Diagnostic Criteria for Apathy (Based on International Task Force Consensus Criteria 29 ).a
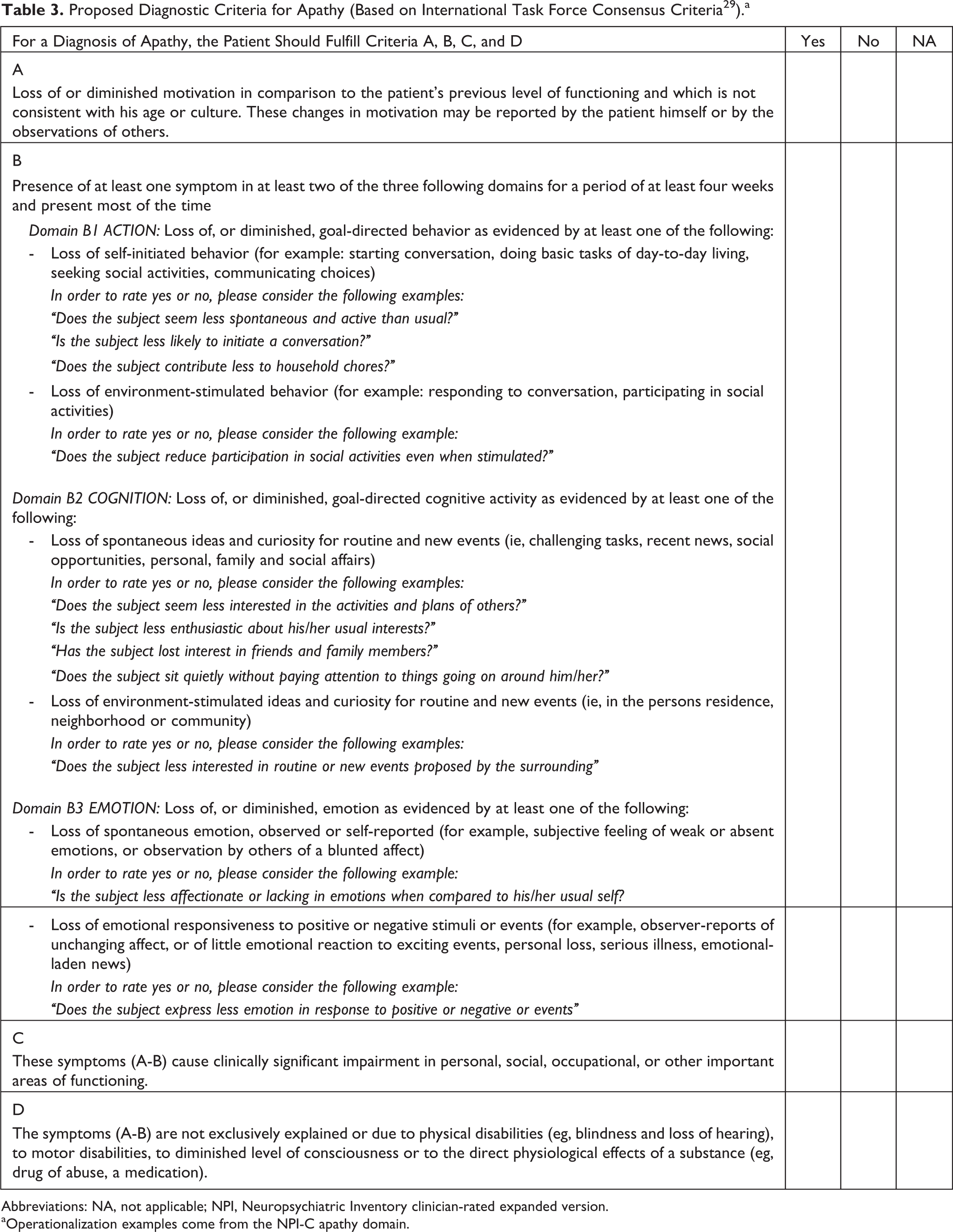
Abbreviations: NA, not applicable; NPI, Neuropsychiatric Inventory clinician-rated expanded version.
aOperationalization examples come from the NPI-C apathy domain.
This group recommends use of operationalized international task force criteria 29 for the diagnosis of apathy at baseline (Table 3).
Apathy severity assessment at baseline
Following a confirmed diagnosis of apathy, it is recommended that specific apathy rating scales be used to define a minimum degree of psychopathology for study entry. The issue of apathy cutoff scores is fundamental to the design of a trial.
Apathy severity criteria at baseline will necessarily be dependent on the specific objectives of individual trials, and the appropriate rating-scale cutoff value will be determined according to the target patient population. However, we present the following considerations with respect to apathy severity cutoff scores at baseline.
One factor that influences the selection of entry criteria in terms of disease severity at baseline is the preferred outcome measure for the study. Although the same instrument can be used to measure disease severity and primary outcome, 83 –85 this may not be ideal due to a potential regression to the mean of the entry score. This threat to study interpretation can be minimized by using 1 instrument to define the severity of the syndrome at baseline and a different tool to measure the treatment outcome.
The scoring for NPI-apathy ranges from 0 (absent) to 12 (severe and very often present). 30,51 In studies involving healthy elderly individuals and those with AD, PD, MDD, schizophrenia, or MCI, a cutoff score for clinically significant apathy has typically been defined as NPI-apathy score ≥4. 36,47,55,85 –90 In the ADMET study, clinical apathy was defined on the NPI-apathy subscale as: (1) frequency of apathy is “very frequently” or (2) the frequency of apathy is “frequently” or “often,” and the severity of the apathy is “moderate” or “marked.” 17 This approach takes into account the fact that some patients may have more frequent but less severe symptoms or less frequent but more severe symptoms. The NPI-apathy score also has the advantage of incorporating a component for caregiver assessment, which provides an additional validity measure.
There is less consensus in the literature surrounding AES cutoff scores, with not all studies reporting the scoring system used. Some authors cite a 0 to 3 scoring system with others using 1 to 4, while reported threshold values for total AES score range from ≥30 to ≥41.5. 25,54,91 –98 In an article by Clarke et al, 91 AES was scored 1 to 4, with a cutoff for the AES-I of 41.5 identified using a receiver–operating curve analysis. This article also reported that optimal psychometric performance was achieved with the AES-I compared with the AES-C or AES-S. Although a score of 41.5 may be considered by some researchers to be high, it is essential that the chosen AES cutoff score be consistent with other entry criteria, including the NPI-apathy. Further research is required to characterize definitively the most appropriate cutoff scores for determining apathy severity at baseline. A score that is high enough to allow demonstration of a treatment effect is balanced against having scores low enough that the screen fail rate for the trial is not unacceptably high.
Further evaluation of the use of rating-scale cutoff scores to determine absolute severity of apathy is required to make a definitive recommendation regarding entry criteria for trials of apathy in neurodegenerative disorders. However, on the basis of information currently available and the need for flexibility according to the specific objectives of individual trials, this group recommends that a value of ≥4 for the NPI-apathy or 41.5 for the AES-I score be adopted as a cutoff value for study inclusion. The ADMET definition of clinical apathy based on the NPI subscale (1. apathy frequency is “very frequently” or 2. apathy frequency is “frequently” or “often,” and apathy severity is “moderate” or “marked”) may also be appropriate.
Confounding factors
Mood/cognition
Although it is recognized that some trials may deliberately include or exclude patients with depression, the management of patients with coexisting depression requires general consideration.
Apathy is known to be a common residual symptom following treatment with the most commonly prescribed antidepressant drugs. 100 –103 Thus, it is important to establish whether, in practice, dysphoria (rather than depression per se) can be reliably separated from apathy or whether other approaches need to be taken such as treating depression and assessing response.
Overall exclusion of all patients with concomitant depression could exclude those who have apathy without a dysphoric component and may therefore restrict the pool of patients. To overcome this, the following options were considered in patients who meet the inclusion criteria for apathy:
Excluding patients with dysphoria items on Beck Depression Inventory-II (BDI-II) and AS. Factor loading analysis across the AS and BDI-II in PD identified 4 factors; 3 of which were identified from the BDI-II. Kirsch-Darrow 7 recommended a modified scoring of the BDI-II and AS so that, in addition to total scores, relevant items would be combined across scales to create subscale scores that map onto the 4 factors; that is, (1) apathy/“loss of motivation” factor; (2) dysphoric mood factor; (3) loss of interest and anhedonia factor; (4) somatic factor. Thus, it may be possible to differentiate dysphoria (rather than depression) from apathy without using overlapping diagnostic approaches. However, appropriate cutoff scores for BDI-II dysphoria would be required.
Excluding patients based on NPI-depression/dysphoria. Appropriate cutoff scores would need to be defined (eg, exclude NPI-depression/dysphoria ≥4).
Assigning a categorical diagnosis (for depression in AD or PD) and, if appropriate, a prospective challenge with an SSRI for 2 months. Treatment responders would be excluded, whereas nonresponders and those whose mood improve but present residual apathy symptoms would be entered.
Excluding all patients with depression or marked depression; an approach that has been adopted in previous trials. 17,103
Including patients having depression with dysphoric symptoms on a stable dose of medication for 3 months prior to randomization who were not expected to require a change in medication during the study. The NPI scale would be used to assess depressive symptoms in these patients at baseline.
Option 5 offers the advantage of maximizing the potential patient pool, while providing flexibility to study effects of medication on dysphoria and depression. Further, this option ensures that all patients at potential risk of depression are managed and treated. Finally, as patients will be required to have stable antidepressant treatment for ≥3 months prior to study entry, simultaneous initiation of both an antidepressant and an antiapathy agent is avoided. The best option of study may also depend on the mechanism of action of the test agent and the anticipated effect on multiple behavioral domains.
This group recommends including pure patients with apathy as well as patients having depression with dysphoric symptoms on a stable dose of medication for 3 months prior to randomization who are not expected to require a change in medication during the study. The NPI scale would be used to assess depressive symptoms in all study participants at baseline. Depression would be monitored throughout the study using an alternative scale, such as the clinician-rated Cornell Scale for Depression in Dementia or the self-rated Geriatric Depression Scale. Trials specifically requiring general inclusion or exclusion of depression, or trials requiring stratification according to presence or absence of depression or dysphoria, should be considered on a case-by-case basis.
Behavior
Overlap of behavioral and motor phenomena, such as psychomotor retardation and bradykinesia, may confound any treatment effect, particularly in PD, and should be accounted for as part of the analysis plan.
Inclusion of patients with psychosis, agitation, or aggression in AD may compromise trial participation. Most studies of apathy in AD have excluded patients with psychosis, while the ADMET study and earlier trials tended to exclude patients with agitation or aggression based on an NPI assessment. 17
To control for overlapping behavioral and motor phenomena such as bradykinesia, this group recommends that movement disorders are assessed as a secondary end point, allowing this potential confounder to be accounted for during analysis.
Clinical judgment should be used to exclude patients with psychosis, agitation, or aggression in AD if this would compromise participation or assessment.
Parkinsonism
The diagnosis of apathy overlaps with symptoms of PD (eg, psychomotor slowing and bradykinesia/bradyphrenia). Apathy may be an endogenous symptom or syndrome in PD, but it may also be secondary to, or at least confounded by, associated disability and activity/motor restrictions caused by the illness. 39 For example, apathy is associated with the severity of motor symptoms 104 –106 and Unified Parkinson’s Disease Rating Scale (UPDRS) score. 107 As a measure of apathy in PD, the UPDRS has only limited utility. Although the UPDRS is psychometrically sound 108,109 and item 4 (motivation/initiative) met criteria to be classified as “recommended” by the MDS, 110,111 its single-item rating makes it appropriate only for screening purposes rather than a detailed evaluation of apathy 1,112 and lacks sensitivity when compared with the AS. 112 –114 An MDS-sponsored revision of the UPDRS has been shown to have good psychometric properties 108,109 but requires further psychometric testing. 111 In apathy studies in PD, the UPDRS assessment of motor symptoms has been used as a coprimary (NCT01782222) or secondary end point (NCT01765257). Given the potential confounding role of motor symptoms, a prospective assessment of motor symptom control may be required and the UPDRS would be the instrument of choice. An MDS task force recommended that scales to assess severity of motor symptoms such as UPDRS should be included to help adjust for confounding factors in trials involving patients with PD. 115
To control for the potential confounding role of motor symptoms, it is recommended that motor control be prospectively assessed using the UPDRS.
Treatment
The use of antidepressants in previous trials of apathy is mixed. Many recent RCTs in AD with apathy as the primary outcome have permitted stable doses of antidepressants, including ADMET which allowed SSRIs and serotonin–norepinephrine reuptake inhibitors; trazodone was also excluded (unless used as a sleep aid). 17 However, an earlier pilot study prohibited all psychotropic medications including antidepressants or antipsychotics, 116 while the ongoing study, Bupropion for the Treatment of Apathy in Alzheimer’s Dementia (NCT01047254), also excludes antipsychotics and antidepressants. Where antidepressant therapy is allowed, stable use for a period of either ≥2 or ≥3 months is often specified.
Several studies have demonstrated an effect of stimulant therapy on apathy outcomes. For example, methylphenidate was shown to improve symptoms of apathy in both AD 24,116 –118 and PD. 119
Allowing dementia therapies is important in view of the potential clinical impact on generalizability of outcome. Recent studies of apathy in AD have allowed patients receiving stable doses (≥1-4 months). For example, ADMET permitted stable doses of cholinesterase inhibitors or memantine for ≥ 1 month. However, as the usual initiation of cholinesterase inhibitors is over 2 months, and peak effect for all the drugs from initiation is more than 4 weeks, we recommend a longer prior period of stable dosing of cholinesterase inhibitors than was used in ADMET (Table 4).
Recommendations Relating to Concomitant Medications in Future Trials of Apathy in Neurological Diseases.
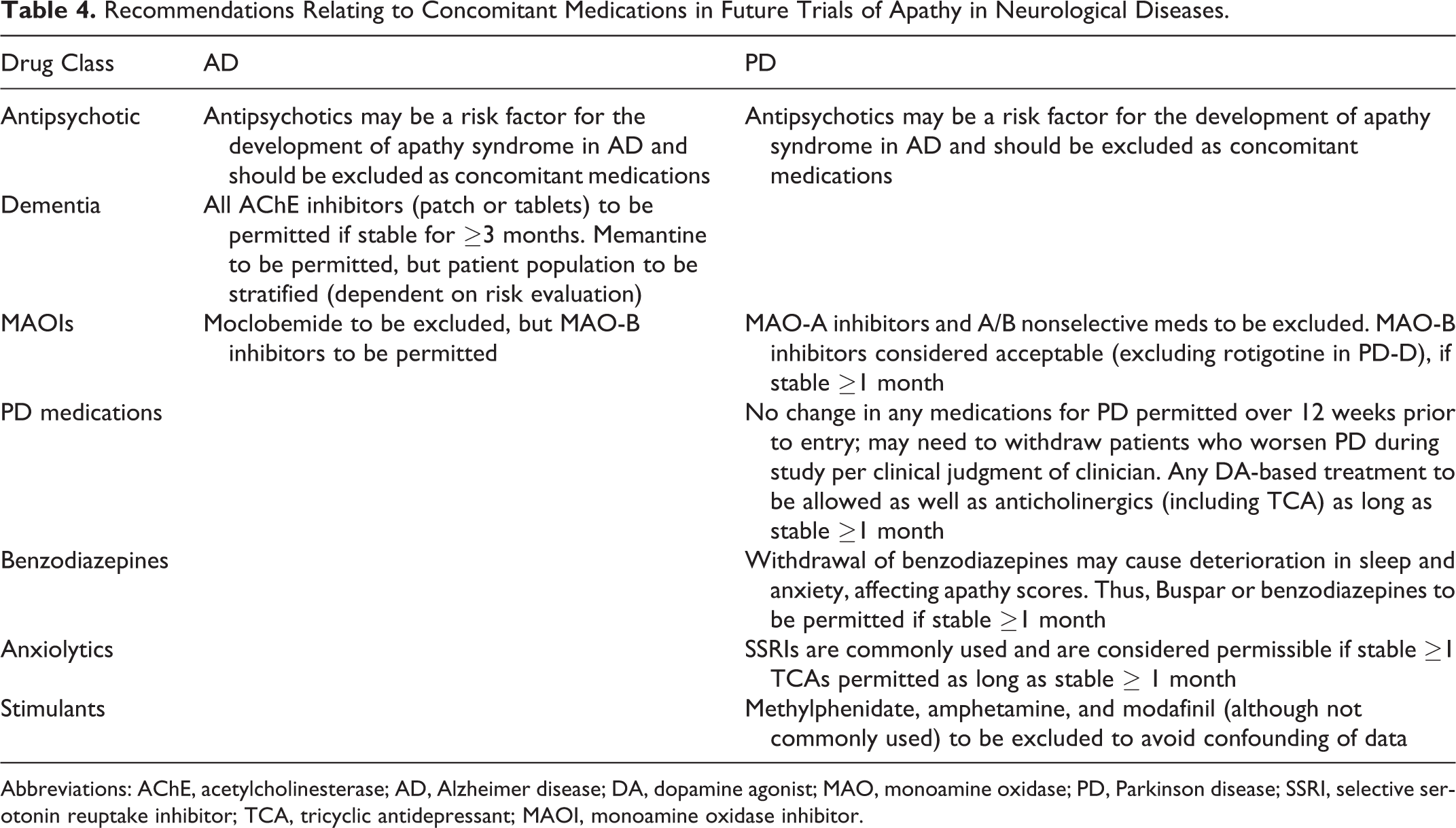
Abbreviations: AChE, acetylcholinesterase; AD, Alzheimer disease; DA, dopamine agonist; MAO, monoamine oxidase; PD, Parkinson disease; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant; MAOI, monoamine oxidase inhibitor.
The use of antipsychotics in AD is currently accompanied by a “black box” warning in the United States regarding mortality risk. Further, the use of antipsychotics may be a risk factor for development of apathy in AD. Antipsychotics are typically excluded in studies of apathy in AD. In the ADMET study, treatment with antipsychotics was excluded, while “other” psychotropic medications were allowed case by case if stable for ≥3 months. 17
There are discrepant findings in the literature about whether deep brain stimulation increases apathy 120 or whether it is unchanged or even improved. 111 However, given the potential effects on apathy it may be advisable to exclude patients with a history of such treatments from apathy treatment studies.
Given that the mainstay of the treatment of motor symptoms of PD is L-DOPA and/or dopamine agonists, these will need to be permitted medications for apathy studies as long as the dose is stable prior to entry (eg, for ≥3 months). Monoamine oxidase inhibitorsand anticholinergics have cognitive or antidepressant side-effects which may impact the assessment of apathy, therefore consideration should be given to excluding (or allowing a stable dose) of these medications. This group recommends that all concomitant medications be allowed with the exception of antipsychotics and any drug which may have a pharmacological interaction that would confound the results. Psychostimulants such as methylphenidate and substrates and modafinil and related agents would necessarily be excluded from trials of antiapathy therapy. Given the potential effects on apathy, it may be advisable to exclude patients with a history of deep brain stimulation from apathy treatment studies. Consideration should be given to excluding (or requiring a stable dose of) MAOI-Bs and anticholinergics. A summary of the group recommendations is provided in Table 4.
Outcome Measures
As discussed in Clinical Relevance of Treatment Effect section, a statistically significant change on an evaluation scale may not achieve a clinically relevant impact on the patient or carer. It is therefore important to consider not only what clinical characteristics should be measured, but also what magnitude of effect is relevant to patients and families.
We recommend that the primary outcome should reflect symptomatic effect and would typically be measured using the NPI-apathy or AES scales. Different studies have suggested that a ≥4-point change or ≥30% decrease in NPI total and subscale scores is clinically relevant, 120 –122 but these cutoffs have not been consistently applied. No equivalent data have been identified for the AES. Further, the ADMET detected statistically significant improvements in NPI-apathy but not in AES-18. 17
Key secondary measures should be selected according to relevance for given study and demonstrate clinical relevance of effect (eg, on activities of daily living [ADL], cognitive effects, caregiver burden, and QoL). Thus, secondary measures will complement the primary outcome and provide supportive information on the real-life significance of any treatment effect. Examples of potential secondary assessments are listed in Table 5.
Potential Secondary Outcome Measures for Future Trials of Apathy in Neurological Diseases.
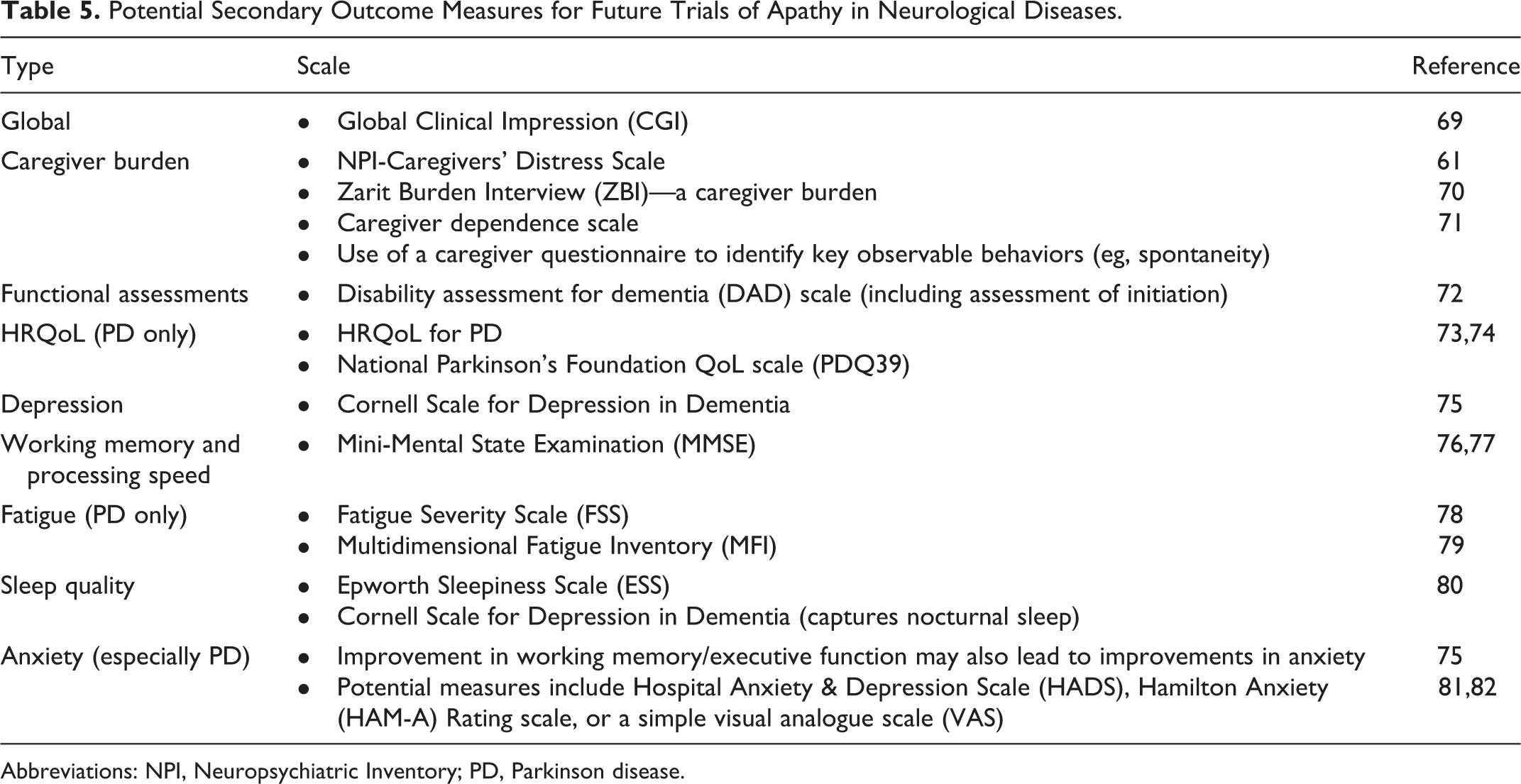
Abbreviations: NPI, Neuropsychiatric Inventory; PD, Parkinson disease.
An additional objective requirement for the assessment of apathy could include ambulatory actigraphy. Actigraphy has been shown to act as an effective marker for apathy in individuals with AD and could provide an objective measure of the effect of pharmaceutical agents in such a population. 123
This group recommends that the most appropriate outcome measures should be selected during the trial design stage. The primary outcome should reflect symptomatic effect and would typically be measured using the NPI-apathy or AES scales. Secondary measures should be selected as appropriate for a given study and according to likelihood of detecting a clinically relevant effect.
Required Study Duration
Alzheimer disease
Most RCTs investigating the effect of pharmacological intervention on behavioral and psychological symptoms of dementia in AD are 6 to 12 weeks in duration. 124 –126 In those RCTs with apathy as the primary outcome measure, the treatment durations were: 2 × 2 week cross-over 116 ; 6 weeks 17 ; 8 weeks 127 ; and 12 weeks (ClinicalTrials.gov: NCT01047254 and NCT00495820). The study duration in most RCTs with apathy as the primary outcome measure is also 6 to 12 weeks. 17 ADMET was of sufficient duration (6 weeks) to detect statistically significant improvements in both NPI-apathy and CGI-C but not AES. 17 It is also noted that a longer duration of study might increase the likelihood of worsening apathy in the placebo arm.
Parkinson disease
Apathy-focused trials in PD have typically been 12 weeks (NCT01765257 and NCT00755027) or 19 weeks (NCT01782222) in duration. Improvement in apathy as a secondary measure (using limited assessments as part of NPI and UPDRS) has been demonstrated over 24 to 26 weeks. 23
Based on these previous studies, it is considered that a period of 6 to 8 weeks is sufficient to measure an effect on apathy without risking confounding from deterioration in the background condition. A double-blind continuation period of 3 to 6 months is also suggested in order to capture longer-term findings without contaminating the primary short-term data with an increased drop-out burden, for example. An extended double-blind period may also allow sufficient time to observe additional changes (especially in patients with PD).
Based on previous studies, this group recommends that the primary measure of apathy is assessed within 6 to 8 weeks, followed by a double-blind continuation period of 3 to 6 months to allow sufficient time for study of functionality and ADL assessment. This extended period is recommended to increase the chance of detecting measurable differences in the latter outcomes.
Additional Considerations
Other considerations for the design of RCTs in apathy include use of appropriate comparators, environment, caregiver role, and securing of patient assent or consent.
The separate evaluation of inpatients and outpatients should be considered, as behavioral problems are more frequent in patients in hospital or residential care. 128 –130 It is also recognized that the caregiver’s input is critical to both good patient care and clinical trial performance.
Clinical trials conducted in the area of apathy will typically be placebo controlled, due to lack of approved therapies in this indication.
Finally, a large proportion of patients who have experienced a stroke subsequently present with symptoms of apathy. 131 –133 It is therefore recommended that patients with a history of stroke should be excluded from future AP or PD trials of apathy to maximize information to be derived from the study population. Poststroke apathy might be addressed as a separate indication of apathy-reducing treatments.
In the absence of other suitable controls, this group recommends the use of placebo-controlled trials to evaluate investigative medications for apathy. All participants should have a reliable caregiver who is willing and able to participate fully in the trial. Inpatients and outpatients should be evaluated separately. It is further recommended that patients with AD or PD included in trials should have no history of a clinical stroke.
Discussion
Compared with trials of motor disorders in PD and cognition impairment in AD, comparatively few studies have been conducted to assess the prevalence and impact of apathy in these conditions. This is despite the known correlation between the presence of apathy and poorer functional, social, and disease outcomes. 2,12 –16 One reason for this paucity of data may be the practical challenges associated with designing an appropriate and methodologically valid clinical trial to investigate the impact of apathy in neurodegenerative disorders.
By formalizing a number of recommendations based on ongoing collaboration and discussion among the authors, our aim is that this review will contribute to the development of clinical trial methodology enabling further research into the impact of apathy in neuropsychiatric disorders. Our hope is that these recommendations may ultimately be integrated and tested prospectively in drug development programs.
There are still several areas where it has not proven possible to provide definitive recommendations for future clinical trials, notably in terms of the use of cutoff scores for severity of apathy at baseline and with respect to the management of coexisting depression. We also did not discuss the engagement and contributions of patients or their representatives in clinical trial design. Patient-centered outcomes research is informed by the perspectives, interests, and values of patients throughout the research process and is now recognized as an integral component of health care research. 134,135 However, if nothing more, this review serves to highlight those areas where further research is required before a definitive position can be adopted. It is our hope that an ongoing process of refinement of the recommendations presented through successive clinical trials may ultimately lead to a definitive clinical trial methodology for this complex and neglected area or research.
By focusing initially on AD and PD, 2 highly prevalent conditions which have been extensively studied and in which most we have the greatest body of data relating to apathy, we hope to establish a framework for clinical trials of apathy which will eventually open a route to the wider study of apathy in neurodegenerative diseases in general.
Footnotes
Acknowledgments
The authors would like to thank Rachel Danks, Paul Gandhi, and Julie Wilson at Bridge Medical for their assistance with the preparation of this article.
Authors’ Note
The authors participated in a 1-day meeting, entitled Methodological Considerations for Clinical Investigations of the Treatment of Apathy in Neurodegenerative Disorders in May 2013, which was sponsored by Roche Pharmaceuticals. Drs Cummings, Friedman, Marsh, and Robert received an honorarium for participation in that meeting but not for preparation of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Garibaldi and Macfadden are employees of Roche Pharmaceuticals. Dr Jones is a paid consultant for Bridge Medical.
Funding
The author(s) declared the following financial support for the research, authorship, and/or publication of this article: Editorial assistance was funded by Roche.