
Abstract
Aims:
To examine the rates and clinical characteristics of mild cognitive impairment (MCI) in older people with depressive symptoms and to determine the relative contribution of hippocampal volume and MCI to memory change.
Method:
One hundred and fifty-two participants with lifetime Major Depression and remitted or mild symptoms and 28 healthy controls underwent psychiatric and neuropsychological assessments. Magnetic resonance imaging was also conducted in a subset of the patients (n = 81) and healthy controls (n = 18).
Results:
MCI was diagnosed in 75.7% of the patients and was associated with increasing age, medical burden, vascular risk factors, later age of depression onset and smaller hippocampi. Multiple regression showed that both hippocampal volume and MCI diagnosis mediate memory performance in depression.
Conclusions:
MCI occurs in older adults with a history of depression and is not simply due to symptom severity. Memory change is linked to underlying hippocampal atrophy in this patient group.
Introduction
Cognitive deficits in depression are common and typically include impairments in processing speed, executive functions (i.e, “frontal” or higher-order functions), learning and memory. 1 More pronounced cognitive changes may occur in those with later ages of depression onset, greater vascular risk factors and white matter brain lesions. 2 –5 The presence of cognitive impairment in this group is of prognostic significance and is a risk factor for mild cognitive impairment (MCI). 6 This syndrome is characterized by cognitive impairments greater than expected for age and level of education, in the absence of significant functional decline. 7 Approximately 50% of those with predominantly “amnestic” MCI (aMCI) profiles (where there are impairments in the domain of memory) may convert to Alzheimer’s disease (AD) within 5 years. 7 Less prognostic data are known about those who present with impairments in non-memory domains (“non-amnestic” MCI, naMCI), as these presentations are likely to be underpinned by more diverse pathophysiologies and consequently, the disease trajectory may be more variable. 8
In addition to being a risk factor for MCI, depression and MCI often coexist. 6 Of significance, when a person has both MCI and depression, there is an increased risk of conversion to dementia 9,10 and cognitive deficits do not simply resolve with resolution of depressive symptoms. 11 Regardless of underlying etiological mechanisms, it is now widely recognized that depression is a risk factor for AD and in particular vascular dementia. 2,12 However, only a few studies have examined the rates and clinical characteristics of MCI in older adults with depressive disorders. Lee et al. 13 specifically focused on the amnestic subtype in patients with mild to moderate depressive symptoms and showed that 55% of these patients met aMCI criteria. 13 A study by Bhalla and colleagues 14 examined the rates and characteristics of MCI in a remitted sample and found that 48% had either a dementia or MCI diagnosis compared to 28% of age-matched controls. Here, almost two-thirds of the MCI sample (63%) had an amnestic profile, with the large majority (85%) showing deficits across multiple domains. Accordingly, 37% of the MCI sample had the non-amnestic subtype, with approximately equivalent numbers having single (53%) and multiple (47%) cognitive domains affected. 14 Yeh et al. also reported that MCI was evident in around half of those with remitted symptoms but found that amnestic and nonamnestic subtypes were roughly equal in prevalence (28.5% aMCI compared to 23.8% naMCI). 15 Although a dearth of studies have examined the neurobiological underpinnings of such MCI profiles, Yeh et al. 15 visually rated ventricular enlargement on magnetic resonance imaging (MRI) scans. They found that the amnestic subtype tended to have more ventricular enlargement and later ages of depression onset. By contrast, naMCI was associated with greater vascular risk factors. There were no differences in white matter lesions between those with aMCI, naMCI, no MCI, or control participants in their sample. 15
Examining patients in remission as performed in the above-mentioned studies 13 –15 is important to help eliminate the possibility that the “state” effects of depressive symptoms are primarily accounting for changes in cognitive performance. However, it is noted that some degree of cognitive impairment in such samples tends to persist despite resolution of depressive symptoms, 11 and indeed this is of key interest in this study. To our knowledge, no studies have examined MCI in older adults with mild/remitted depression with regard to quantitative measurement of the hippocampus. This research is warranted since reduced hippocampal volume is not only associated with AD but is also associated with later onset of depression, memory impairment, 16 years of cumulative depression, 17 poor clinical outcome, 18 cognitive decline, 19 and progression to dementia 20 longitudinally. In a sample of older adults with remitted (or very mild residual) symptoms, we therefore aimed to (1) ascertain the rates of MCI and its associated subtypes; (2) examine the clinical correlates of MCI; (3) determine whether the MCI subtypes differ in terms of hippocampal size; and (4) determine whether any relationship between MCI diagnosis and memory is influenced by hippocampal volume. We hypothesized that (1) the majority of the sample would meet criteria for MCI; (2) MCI would be associated with smaller hippocampal volumes, vascular risk and later ages of depression onset; (3) smaller hippocampal volumes would be particularly pronounced in the amnestic subtype; and (4) hippocampal volume would mediate the relationship between MCI diagnosis and memory.
Methods
Sample
One hundred and fifty-two health-seeking (i.e, seeking assessment and/or treatment for mood or memory concerns) participants (56 male and 96 female) meeting criteria for lifetime Major Depressive Disorder were recruited from the Healthy Brain Ageing Clinic at the Brain & Mind Research Institute, Sydney, Australia. Twenty-eight never depressed and cognitively intact participants (8 male and 20 female) served as a healthy control group. Inclusion criteria: participants were required to speak English fluently and be older than 50 years. This age was chosen in line with our early intervention clinic and agenda for risk factor reduction and also by data demonstrating a long preclinical phase of dementia that even precedes MCI.
7,21,22
Patients were also required to have a 17-item Hamilton Depression Rating Scale (HDRS) score of less than 20 (i.e, in remission or mild symptom severity)
23
; to have had a Major Depressive Episode in the last 5 years; and to be stabilized on medication. Exclusion criteria were significant neurological disorder (other than MCI), head injury with loss of consciousness
Measures
Psychiatric
A geriatric psychiatrist performed a structured clinical assessment to derive clinical history including age of depression onset and medication use. The affective component of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Revised (DSM-IV-TR) 25 was performed to confirm lifetime and current depression diagnoses. Depression severity was clinician rated using the HDRS. 23 The clinician-rated Social and Occupational Functioning Scale 26 was used to assess participants’ current level of everyday functioning on a continuum (0 to 100), whereby higher scores are suggestive of superior levels of functioning. The psychiatrist also rated medical burden using the Cumulative Illness Rating Scale (Geriatric version), 27 and vascular risk factors were noted as being present (1) or absent (0), including hypertension, smoking history, hypercholesterolemia, heart disease and diabetes. 28 These factors were summed to give a vascular risk factor score (range 0-5).
Of the patient sample, 92 participants had early-onset (i.e, age of onset <50 years) depression and 60 participants had late-onset (i.e, age of onset
Self-report
Participants were asked to complete the 15-item Geriatric Depression Scale (GDS) as a measure of self-reported depressive symptoms (score range = 1-15, where higher scores reflect increased symptomatology). 29
Neuropsychological
As described elsewhere, 30 a clinical neuropsychologist administered a comprehensive standardized battery of tests that were chosen for their sensitivity to neuropsychological deficits in affective disorders, MCI and dementia. Various domains of cognition were assessed including processing speed, verbal and nonverbal learning, memory, language, visuospatial functioning and executive functioning 31 (see Supplementary material for information on specific tests used to assess these domains of cognition). For descriptive purposes, predicted intellectual ability (predicted IQ) was estimated using the Wechsler Test of Adult Reading 32 and global cognition was measured using the MMSE. On the basis of our earlier work, 16,33 in this study we were interested in memory in relation to hippocampal volume. The ability to learn and retain unstructured verbal material was assessed using the Rey Auditory Verbal Learning Test (RAVLT). 34 Encoding (summed trials 1-5 of the 15-item word list; RAVLT1-5) was expressed in relation to age and education-adjusted z-scores. 35 Delayed percentage retention was expressed as a z-score adjusted for age and education (trial 7/5 × 100%; RAVLT7/5).
Diagnosis of MCI
Diagnosis of MCI was determined by consensus rating of 3 raters including a geriatric psychiatrist and 2 neuropsychologists according to established criteria. 36 Neuropsychological impairments, neuroimaging findings, clinical presentation, and history were taken into account in the diagnosis of MCI. All patients meeting criteria for MCI were health-seeking and had subjective cognitive complaints, either on self-report measures (Everyday Memory Questionnaire—revised) 37 or on clinical interview. Neuropsychological impairments required subjective cognitive complaints as well as decrements of at least 1.5 SDs in at least 1 neuropsychological domain relative to premorbid functioning. 7,36 Further, patients were required to demonstrate preserved basic activities of daily living, rated either by a family member or friend on The Bayer Activities of Daily Living Scale 38 or on clinical interview. For a diagnosis of aMCI, deficits on tests of delayed recall were required to be present (i.e, not merely poor learning). Non-amnestic MCI was diagnosed when deficits were present in domains other than memory storage. Furthermore, both aMCI and naMCI were specified as “single” or “multiple” depending on whether deficits were present in one or more neuropsychological domains. No participant was deemed to have dementia according to DSM-IV-TR criteria. Further, all control participants were administered the neuropsychological battery and deemed to be cognitively intact via this consensus process.
Magnetic Resonance Imaging Acquisition
A subsample of 81 older adults with a history of depression and 18 comparison participants completed the MRI protocol within 2 weeks of the neuropsychological assessment at the Brain & Mind Research Institute using a 3 Tesla General Electric (GE) Discovery MR750 scanner (GE Medical Systems, Milwaukee, Wisconsin) with an 8-channel phased array head coil. The following images were acquired in order: (1) three-dimensional sagittal whole-brain scout for orientation and positioning of subsequent scans; (2) T1-weighted magnetization prepared rapid gradient-echo sequence producing 196 sagittal slices (repetition time = 7.2 ms; echo time = 2.8 ms; flip angle = 10°; matrix 256 × 256; 0.9mm isotropic voxels) for anatomic analysis and MCI diagnosis.
Volume Segmentation Analysis
As described previously, 39 subcortical volumes for the left and right hippocampi were extracted using a semiautomated segmentation routine based on the principles of the Active Shape and Appearance Models within a Bayesian framework as implemented by “FIRST” in FMRIB Software Library (FSL). These regions were specifically selected for their relevance to depression pathophysiology 1 and for comparison to previous literature. White matter, grey matter and cerebrospinal fluid volume were estimated using SIENAX, 40,41 which is also part of the FSL library. Intracranial volume (ICV) was calculated by adding white matter, grey matter and cerebro spinal fluid volume for each participant. In order to normalize the subcortical volumes across all participants, individual differences in brain size were corrected for by dividing the raw segmented volumes by the mean of all participants’ ICV, multiplied by the uncorrected segmented volumes. 42
Statistical Analysis
Data was analyzed using PASW version 18 by IBM. Independent samples t tests (only 2 groups) and one-way analysis of variance were used for between-group comparisons. Normality was assessed using Kolmogorov-Smirnov tests. When assumptions of normality were violated, nonparametric tests were used. Spearman’s ρ coefficients were used for all correlations, unless otherwise stated. Mediation modelling was conducted to examine the relationship between MCI diagnosis, hippocampal volume and memory using simultaneous regression based on theoretical guidelines provided by Baron and Kenny. 43 All analyses were two-tailed with an α level of 0.05. Bonferroni corrections were made for multiple comparisons. When comparing correlations in MCI subgroups, Fisher’s r to z transformations were conducted to determine whether differences in correlations were significant.
Results
Tables 1, 2 and 3 show descriptive data for the sample, including the various subtypes of MCI. There were no significant differences between the older adults with a history of depression (patient group) and the control participants in terms of age, years of education or predicted IQ. However, the patient group had significantly higher depression severity (as measured by HDRS), increased medical burden, lower MMSE and lower social and occupational functioning compared to the control participants (Table 1). On average, depressive symptom severity for the patient group was in the euthymic range (mean HDRS score = 7, range: 0-18).
Demographic, Clinical and Volumetric Data for Control Participants and the Patient Group.a
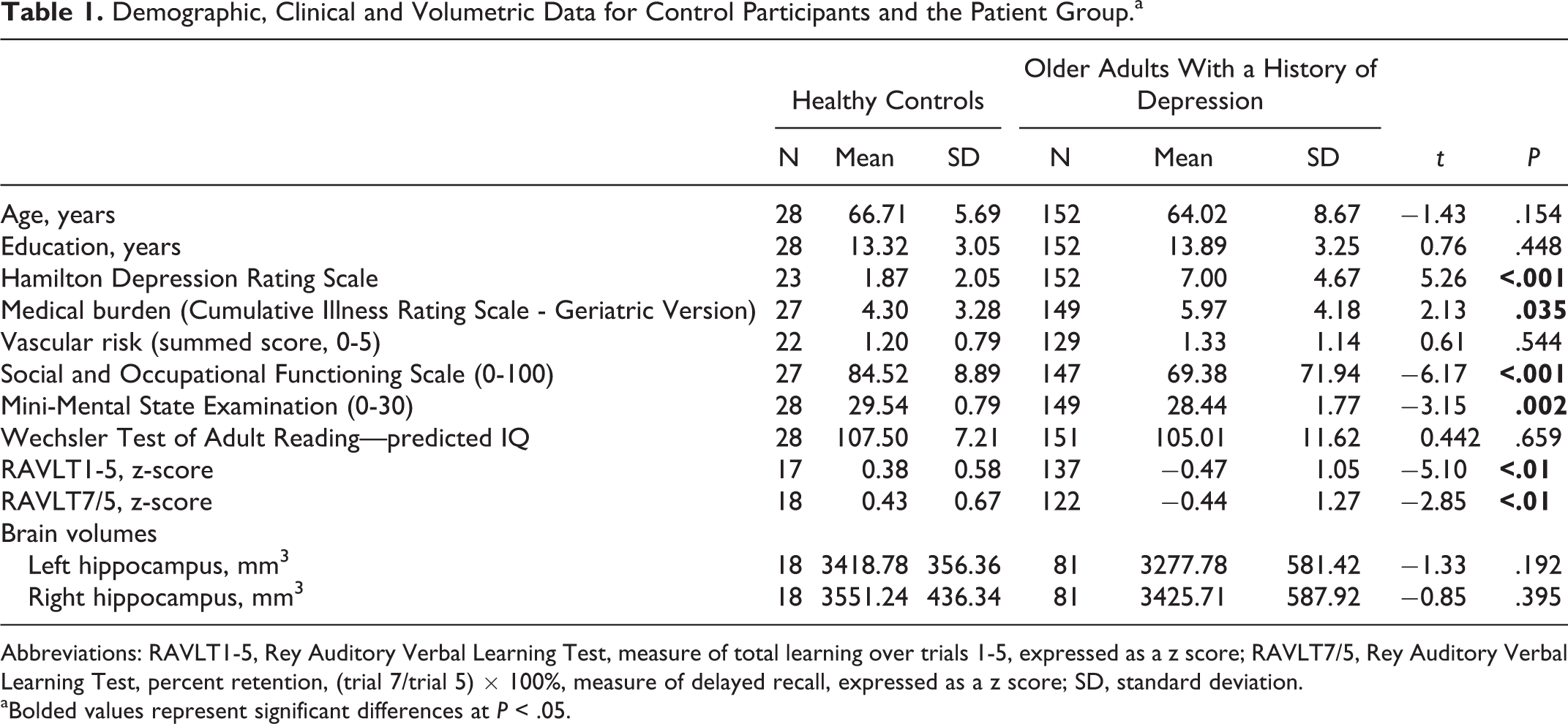
Abbreviations: RAVLT1-5, Rey Auditory Verbal Learning Test, measure of total learning over trials 1-5, expressed as a z score; RAVLT7/5, Rey Auditory Verbal Learning Test, percent retention, (trial 7/trial 5) × 100%, measure of delayed recall, expressed as a z score; SD, standard deviation.
aBolded values represent significant differences at P < .05.
Demographic, Clinical and Volumetric Data for the Patients Who Are Cognitively Intact (no MCI) and Those With MCI.a
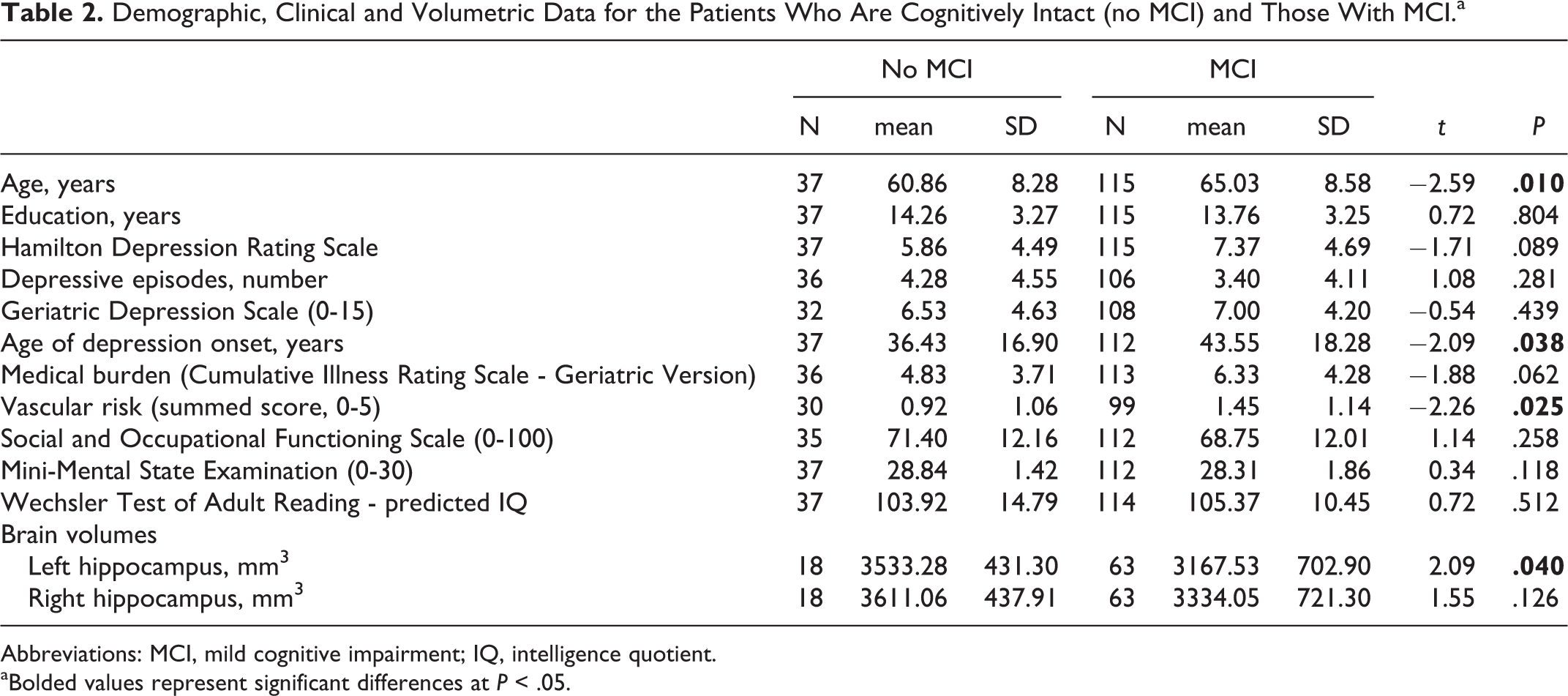
Abbreviations: MCI, mild cognitive impairment; IQ, intelligence quotient.
aBolded values represent significant differences at P < .05.
Demographic, Clinical and Brain Volume Data for Those With naMCI and aMCI.a
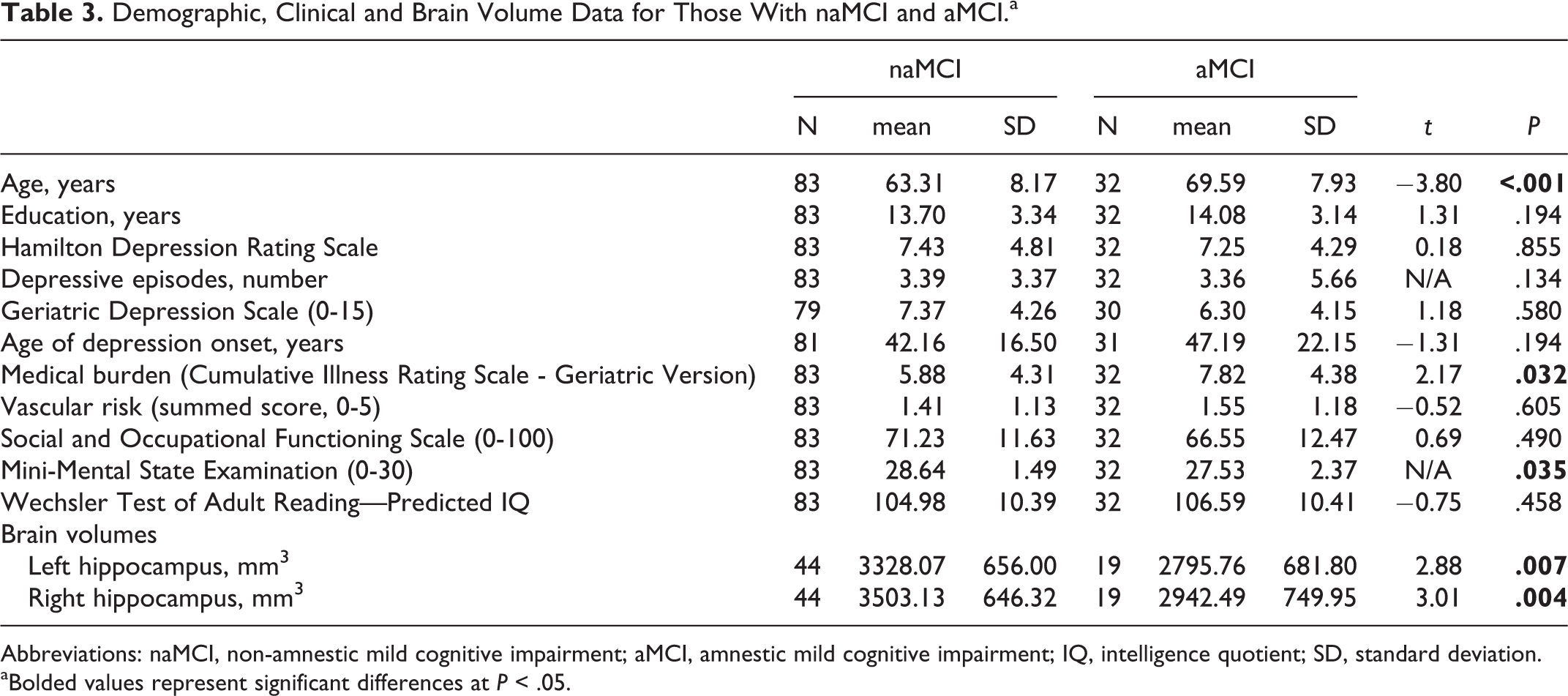
Abbreviations: naMCI, non-amnestic mild cognitive impairment; aMCI, amnestic mild cognitive impairment; IQ, intelligence quotient; SD, standard deviation.
aBolded values represent significant differences at P < .05.
There were no significant differences between the MRI subsample of control participants compared to the rest of the control participants in terms of age, gender, depressive symptom severity, medical burden, vascular risk, social and occupational functioning, MMSE, years of education or predicted IQ. There were no significant differences between the MRI subsample of the patient group compared to the rest of the patient group in terms of age, gender, depression severity, duration of depression (if currently depressed), age of onset of depression, the prevalence of MCI, medical burden, vascular risk, social and occupational functioning, MMSE, years of education or predicted IQ (all P > .05; data not shown).
Comparison of Patients and Controls
Hippocampal size, learning and memory in patients and controls
There was no significant difference in hippocampal volume when comparing the controls to the patient group (Table 1). However, the patient group had significantly lower encoding [RAVLT1-5] and delayed percent retention [RAVLT7/5] on memory tests when compared to control participants (Table 1). Within the patient group, the left hippocampus was significantly smaller in those with MCI compared to those without MCI, while the right hippocampus did not significantly differ (Table 2). There were no significant correlations between hippocampal volume and verbal learning or memory retention for the control participants (data not shown, P > .05).
Depression Sample Only
Patterns of neuropsychological deficits
Within the entire patient group, 39.5% (60 of 152) showed impairments in new learning (
Patterns of MCI
The frequency of MCI in the patient group was 75.7% (115 of 152), with naMCI being most prominent (54.6%; 83 of 152) in comparison to aMCI (21.1%; 32 of 152). There were no differences in gender between MCI subtypes (naMCI, 58% female vs. aMCI, 48% female, χ 2 = 1.5, P > .05). Of those with MCI, multi-domain was more common (79 of 152; 52%), with single-domain MCI evident in only 23.7% of patients (36 of 152).
Relationship between depression, MCI and clinical features
For the patient group, those meeting criteria for MCI did not have significantly greater rates of DSM-IV-TR defined current Major Depression (n = 6, 16.2%) in comparison to those without MCI n = 33, 28.7%; χ 2 = 2.3, P = .131. When examined against continuous variables, Table 2 shows that those with MCI within the patient group were significantly older and had a later age of depression onset. They also had more vascular risk factors and increased medical burden compared to those without MCI. There was no difference between those with and without MCI in terms of the number of depressive episodes, clinician- or self-rated depression severity (i.e, HDRS or GDS), predicted IQ, MMSE, years of education or social and occupational functioning.
Comparison of MCI subtypes
For the patient group, the single- and multi-domain MCI subtypes did not differ on any clinical, cognitive or imaging variables (data not shown, all P > .05), with the exception of age, whereby those with multi-domain MCI were older (t = −2.3, P = .022).
As indicated in Table 3, of those meeting criteria for MCI, there was no difference between aMCI (n = 10, 31.3%) and naMCI (n = 24, 28.9%) in terms of the proportions meeting criteria for current Major Depression (χ 2 = 2.3, P = .128). However, when examined against continuous variables, those with aMCI were more likely to be older, have increased medical burden and lower MMSE scores (the older age of the MCI group compared to no MCI is thus likely to be attributed to the aMCI subtype). However, summed vascular risk factors did not differ between participants with aMCI and naMCI. There was no difference between aMCI and naMCI subtypes in the number of depressive episodes, age of onset of depression, depression severity (HDRS or GDS), predicted IQ, years of education or levels of social and occupational functioning. In terms of brain changes, patients with aMCI had significantly smaller left and right hippocampi compared to those with naMCI. Hence, it should also be noted that the hippocampal volume reduction found in MCI compared to no MCI is also likely to be attributable to the aMCI subgroup.
Association between hippocampal volumes and age of depression onset
For the whole patient group, a later age of depression onset was associated with smaller left (ρ = −0.4, P < .001) and right (ρ = −0.3, P = .002) hippocampal volumes. Although the magnitude of the correlation coefficient was similar across MCI subtypes, Fisher’s r to z transformation showed that the relationship between hippocampal volume and age of onset did not differ between those with and without MCI (left: z = 0.3, P = .780, right: z = 0.3, P = .803). In order to ensure that hippocampal volume changes did not merely reflect antidepressant use, we compared volumes between those taking (n = 56) and not taking (n = 24) antidepressants and there were no differences in hippocampal volume (left: t = 0.6, P = .563, right: t = 0.7, P = .492).
Association between hippocampal volumes and learning and memory
Table 4 shows that for the entire patient group, smaller hippocampal volumes bilaterally were associated with poorer encoding (RAVLT1-5) and memory retention (RAVLT7/5). For the MCI subgroup, smaller hippocampal volumes bilaterally were associated with poorer memory retention while the left hippocampus (and not the right) was associated with poorer encoding. For the cognitively intact patient subgroup, smaller right hippocampal volume was associated with poorer memory retention. However, there were no significant correlations between the left hippocampus and memory retention, nor between either hippocampi and encoding for the cognitively intact patient subgroup.
Correlations Between Hippocampal Volume and Memory for the Patient Group Subset With Neuroimaging Data.a ,b
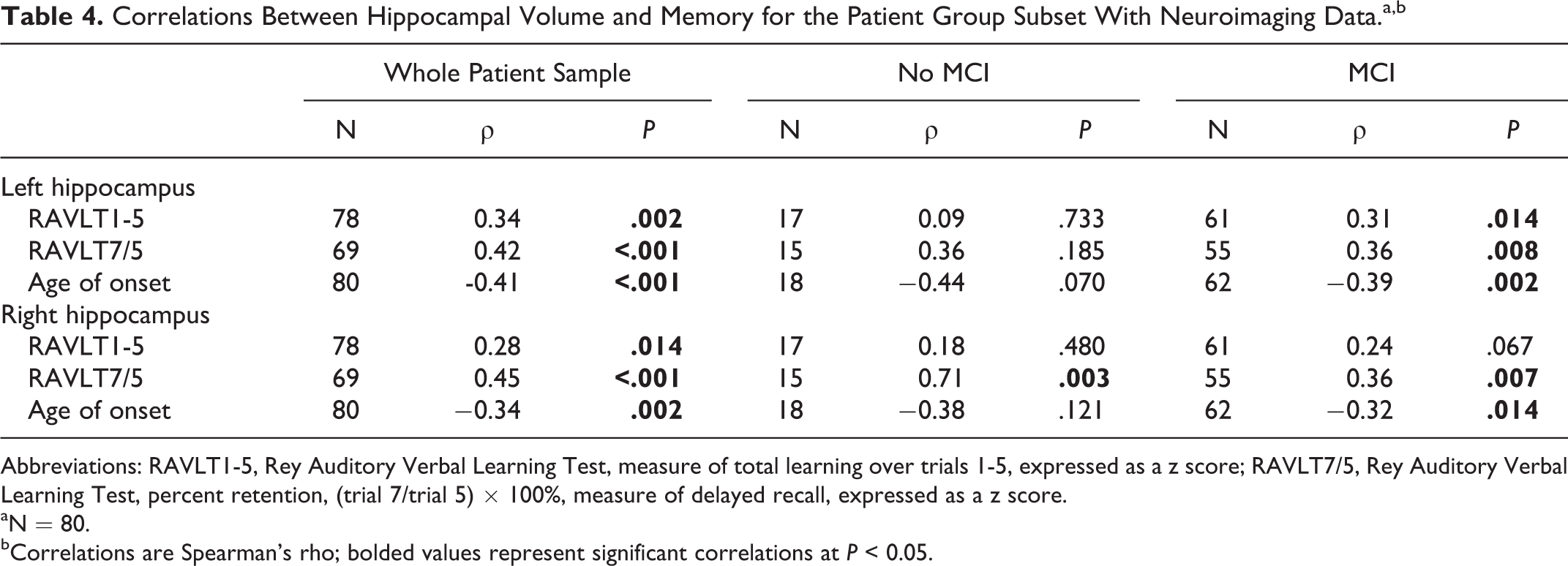
Abbreviations: RAVLT1-5, Rey Auditory Verbal Learning Test, measure of total learning over trials 1-5, expressed as a z score; RAVLT7/5, Rey Auditory Verbal Learning Test, percent retention, (trial 7/trial 5) × 100%, measure of delayed recall, expressed as a z score.
aN = 80.
bCorrelations are Spearman’s rho; bolded values represent significant correlations at P < 0.05.
Relative contributions of MCI status and hippocampal volume to memory
Given that the left hippocampus correlated with memory performance only for those with MCI and not for the cognitively intact patient subgroup, we were interested in determining the relative contributions of MCI status and hippocampal volume to memory encoding. In order to analyze this, we conducted mediation analysis using multiple linear regression. 43 In our mediation model, the independent variable was MCI status (MCI vs. no MCI), mediator was left hippocampal volume and the outcome variable was encoding (see Figure 1).
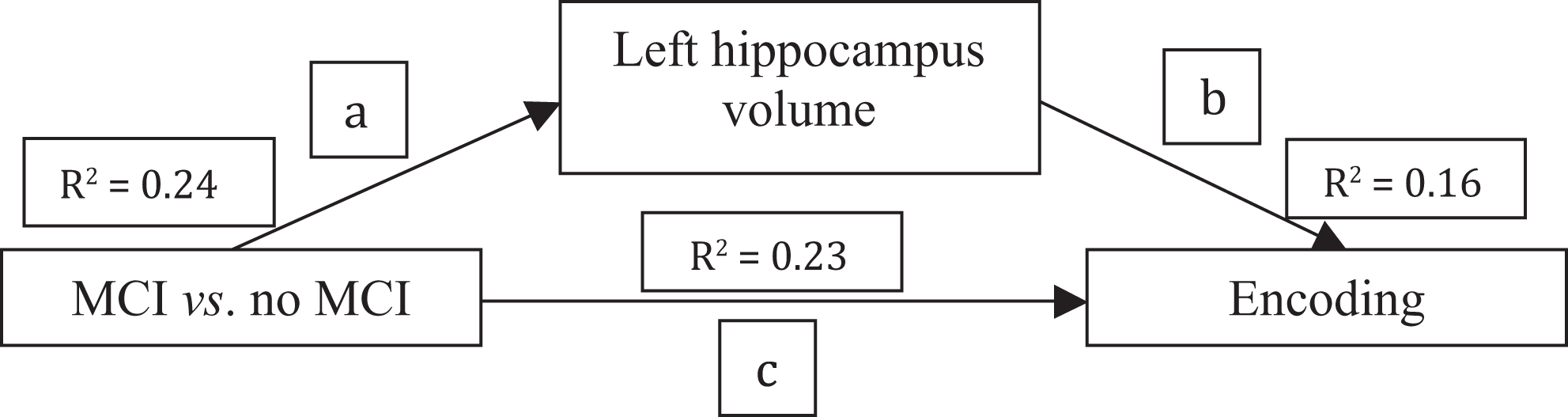
Pictorial representation of the mediation effect of left hippocampal volume on the relationship between MCI status and encoding. The MCI status significantly accounted for variance s in encoding (23%, t = −4.70, df = 76, P < .001), path c; MCI status significantly accounted for variance in left hippocampal volume (24%, t = −2.17, df = 79, P = .033), path a; left hippocampal volume significantly accounted for variance in encoding (16.0%, t = 3.81, df = 76, P < .001), path b.
It was found that left hippocampal volume mediated the relationship between MCI status and memory encoding according to the guidelines suggested by Baron and Kenny 43 (Figure 1). When the mediator (left hippocampal volume) and the independent variable (MCI status) were entered into the regression model together, the entire model accounted for 32% of the variance in encoding (R 2 = 0.32, F(2,75) = 17.26, P < .001). The MCI status uniquely accounted for 15% of the variance in encoding (t = −4.12, P < .001) while hippocampal volume uniquely accounted for 9% of the variance in encoding (t = 3.09, P = .003), with the remaining 8% being shared predictor variance. The mediation effect of hippocampal volume on the relationship between MCI status and encoding was seen by less variance being accounted for by MCI status than when MCI status was the sole predictor (15% compared to 23% respectively). Hence, left hippocampal volume mediated the relationship between MCI status and verbal encoding.
Discussion
This study represents the first to examine the occurrence of MCI in older adults with a history of depression with concurrent and quantitative measurements of key subcortical nuclei volumes and neuropsychological functioning. We found that despite being a remitted or only mildly depressed sample, the large majority (75.7%) of patients met criteria for MCI. Our findings are thus aligned with previous studies 13 –15 reporting the common concomitance of mood and cognitive disturbance in older adults. Our data also support studies showing that deficits persist even when symptomatology has largely resolved, 11 likely reflecting underlying structural brain changes. 1 Importantly, these findings are unlikely to merely reflect the “state” effects of depressed mood, since there were no differences in MCI rates according to DSM-IV-TR defined Major Depression, nor did the subtypes differ in the severity of depressive symptoms.
In comparison to prior work, our study found higher rates of MCI in older adults with a history of depression than that obtained by Lee et al. 13 and Yeh et al. 15 who reported that 55% and 52% met MCI criteria respectively. In interpreting these differences, it is important to note that all patients in our study were assessed by a clinical neuropsychologist and we rated our MCI diagnoses according to decline relative to premorbid IQ levels (as well as endorsing subjective cognitive complaints), rather than simply using a generic 1.5 SD cut-off relative to normative data. Thus, in our reasonably educated sample, our method is likely to have yielded higher rates of MCI when compared to studies including patients with “average” intellect. It is not entirely clear whether previous studies have placed similar emphasis on premorbid functioning or whether they rated MCI using similar consensus methods to ours (i.e, taking into account clinical history as well as neuropsychological performance). Also, another factor contributing to the difference between our study and that of Bhalla et al. 14 may be the fact that Bhalla et al. 14 used criteria specified by the University of Pittsburgh’s Alzheimer’s Disease Research Centre, which does not specify the use of a 1.5 SD reduction in objective neuropsychological testing compared to normative data as stipulated by the Winblad et al. 36 criteria used in our study. Further, Bhalla et al. 14 used an objective in-home instrumental activities of daily living assessment in their diagnoses, whereas we used informant reports and information gathering during the clinical interview to obtain the information about activities of daily living that formed part of the MCI diagnosis. 14 Indeed, quite varied methodologies have been employed in the few studies that have examined MCI in depression, a factor that requires consideration when comparing MCI prevalence rates.
In terms of MCI subtype, our data show that multi-domain MCI was the predominant profile, evident in 52% of patients and also associated with advancing age. Non-amnestic forms were also more common in our sample, with rates being around 55% and 21% for naMCI and aMCI, respectively. This finding differs from that of Bhalla et al. 14 where aMCI was found in 63% and naMCI was found in 37%. Yeh et al. 15 found roughly equal rates of 28.5% for aMCI and 23.8% for naMCI. Although we did not find naMCI to be associated with any particular clinical feature, the amnestic subtype was associated with advancing age, poor global cognition and greater medical comorbidity. Given that aMCI was associated with advancing age, it is possible that these differences in prevalence rates partly reflect the inclusion of a lower age limit in our study (i.e, 50 years compared to 60 years or greater in prior studies 14,15 ). Our lower age limit is predicated on work from the MCI and neurodegenerative disease literature, which increasingly shows that subtle cognitive decline and/or subjective memory complaints are evident 10 to 20 years prior to MCI or dementia diagnosis (i.e, the preclinical period) 7 and should be investigated. This view is also consistent with that proposed in a US National Institute of Mental Health workgroup (1986). 44
In interpreting our findings, it is also important to note that we were particularly stringent regarding aMCI classification. That is, unlike Yeh et al. 15 who used deficits in learning or delayed recall to classify patients as having memory deficits and Bhalla et al. 14 who have not specified whether their memory measure includes encoding and/or delayed recall deficits, patients in our study were required to demonstrate clear evidence of deficits in delayed recall, such that deficits on the encoding aspect of a task were insufficient for a diagnosis of aMCI. 45 This method, in turn, is likely to yield lower rates of aMCI than those classifying aMCI on the basis of any decrement on memory testing. Given that deficits in delayed recall are one of the strongest predictors of AD, 7 our stringent method of classifying aMCI is likely to have reduced subgroup heterogeneity and affords greater confidence that those diagnosed with aMCI have an increased likelihood of progressing to AD. Furthermore, while the higher proportion of naMCI in our study is not typical of traditional memory clinics, it is similar to other large-scale studies of aging that have used the MMSE for screening purposes. 46 The higher proportion of naMCI in our study may also reflect the fact that our clinic is a specialist early-intervention clinic targeting older adults with a range of cognitive difficulties rather than focusing on memory complaints. This is hence likely to result in a diverse range of participants rather than focusing solely on those with underlying AD pathologies. Another factor contributing to the difference between our study and that of Yeh et al. 15 may be the lower cut-off on the HDRS (score of 7 or less) used by Yeh et al. 15 as well as only including patients who are in remission compared to the HDRS cut-off of 20 or less used in our study (which included patients who are currently mildly depressed).
It is also plausible that MCI as a construct in our relatively younger sample with a mean age of 65 is different to some of the clinical characteristics of MCI with older participants. As mentioned earlier, this may account for the large number of patients with naMCI compared to patients with aMCI with diverse trajectories of illness progression. Furthermore, given that our sample included participants from 50 years to older than 80 years, there is likely to be heterogeneity in clinical characteristics within our sample. Hence further research with stratified age-groups is needed to explore these differences further. Indeed preliminary modelling conducted by Yesavage et al. 47 demonstrate the significance of baseline age in normal participants converting to MCI as well as participants with MCI converting to AD.
In accordance with a large corpus of research linking depression with vascular risk factors, 1 our data showed that the patient group had higher levels of medical burden and vascular risk factors, when compared to the control sample. Of further significance is the finding that around a quarter of the patient group were cognitively intact and this subsample had lower levels of vascular risk factors than those with MCI. These data are consistent with those linking cognitive impairment to “vascular depression” and/or cerebrovascular disease as well as progression to vascular dementia longitudinally. 12 These findings thus reinforce the need for early intervention strategies targeting physical health and cardiovascular well-being. 21
At this stage, it is unclear precisely which mechanistic pathways need to be targeted in order to reduce depression and concomitant cognitive decline due to cerebrovascular disease. Nonetheless, as extensively discussed by Taylor and colleagues, 48 it has been proposed that disconnection, inflammatory and hypoperfusion mechanisms are likely operative. It terms of disconnection mechanisms, it has been postulated that ischemia and white matter lesions may disrupt neural structural and functional connectivity which in turn impacts on the connected regions, resulting in both mood and cognitive syndromes. 48 Studies using diffusion tensor imaging have indeed supported this notion, showing altered white matter microstructure and/or myelin integrity as a result of cerebrovascular changes. 49 Further, both aging and disease-related processes relating to increased medical burden and compromised immune function may promote proinflammatory processes with a subsequent cascade of events, including disruption to neurotransmitters and their pathways, hippocampal damage and cell death. 48 Vascular disease may also impact cerebral metabolic activity via the reduction of cerebral blood flow, which not only increases risk for ischemia but also impacts upon protein synthesis critical for cognitive processing, particularly that subserved by subcortical and temporal structures including the hippocampus. 16
Interestingly, while the overall sample of patients in this study did not demonstrate reduced hippocampal volumes compared to controls, patients with MCI did have significantly smaller hippocampi compared to those who were cognitively intact. We also confirmed that within the patient group, hippocampal volume loss is associated with poorer memory. Importantly, this is the first study to show that (1) hippocampal volume reduction is more pronounced in those with MCI and particularly aMCI, in a group of older adults with mild/remitted depression; and (2) the relationship between hippocampal volume and memory is most pronounced in the MCI subsample, as compared to cognitively intact patients. Finally, this study demonstrates that hippocampal volume is an independent predictor and mediator of memory encoding, regardless of MCI status. These findings underscore the critical role of the hippocampus for memory change in depression occurring in older adults and highlight the additional utility of volumetric hippocampal measurement.
Although very few studies have examined the significance of hippocampal volume change in older adults with a history of depression, longitudinal data support the notion that hippocampal atrophy is associated with gross cognitive decline over a 2-year follow-up period. 50 Indeed, it remains a possibility that those with hippocampal atrophy are in the prodromal stages of AD, such that their depression symptomology is a manifestation of early AD. 51 Hence, it now remains to be determined whether patients with both hippocampal atrophy and an amnestic neuropsychological profile have a predominant trajectory longitudinally for AD, as opposed to cerebrovascular or other neurodegenerative pathologies. This would be consistent with the large body of research linking the aMCI subtype to higher rates of progression to AD compared to the naMCI subtype, which has been associated with diverse outcomes including dementias associated with cerebrovascular pathology, remaining stable as well as AD. 52
Alternatively, in older adults with a history of depression, hippocampal change may be attributed to illness-specific factors such as dysfunction of the hypothalamic–pituitary–adrenal axis, downregulation of neurotrophic factors, inflammatory changes and/or chronic effects of cortisol on hippocampal integrity, and thus may not be pathognomonic of neurodegenerative disease. 1,48 The current finding that greater hippocampal volume reduction was associated with later ages of depression onset, however, argues against hippocampal change being merely due to chronic illness-specific effects and alternatively suggests that aging-specific processes underlie both hippocampal volume change and depression onset.
Further, research indicates that hippocampal damage can occur due to mechanisms involved in vascular pathology 48 and that vascular risk factors not only increase risk of neurodegenerative processes typically associated with cerebrovascular disease, but that it also increases the risk of AD. Such findings highlight that the relationship between hippocampal damage, depression and cognitive decline is likely multi-faceted rather than exclusively relating to AD-type disease processes. Also, vascular factors may be contributing to cognitive decline seen in aMCI 53 as well as the traditional notion of it relating to naMCI.
Limitations
In interpreting these findings, it is worth noting the limitations of this study. First, only a subset of the patients had MRI volumetric data. Despite this subsample not differing from the rest of the patient group in terms of age, sex, depression severity or the rate of MCI, it would have been preferable to have volumetric data for the entire sample. The control sample in this study was particularly small and hence limits the comparisons that can be drawn with the patient group. Also, due to the high prevalence of MCI in this sample, the sample of cognitively intact participants with a history of depression was relatively small. Further research examining the pathophysiological mechanisms underpinning the changes in regional volume and their association with cognitive dysfunction in this cohort are now warranted.
It is also important to note that this is a cross-sectional study. As such, we were not able to report on whether the cognitive deficits found on testing would persist over time. Further, the time-course of memory deficits relative to depressive history cannot be determined from our data. Prospective studies elucidating the time-course of cognitive deficits in relation to depressive symptoms would be interesting, particularly for those with aMCI, to determine whether their depression symptoms are largely a reflection of underlying AD.
Furthermore, the differences that exist between studies examining cognitive decline in older adults with respect to factors such as sample characteristics and methodology for MCI diagnosis means that it is difficult to compare between studies and this is an inherent limitation in this area of study. Hence, collaboration between investigators is needed regarding the use of common assessment tools and diagnostic criteria, to enable cross-comparison between studies.
Implications
This is the first study to examine concurrently the MCI rates and hippocampal correlates of MCI in a remitted or mildly depressed older adult sample. It highlights not only the persistence of cognitive impairments in the majority of older patients with mild depression symptomatology, but also that these impairments may be underpinned by structural brain changes, which in turn relate to memory decline. It highlights the hippocampus as a structure that is particularly entwined with depression in older adults, particularly in those with later ages of depression onset, MCI status and memory change. Given work showing that the size of the hippocampus can change in association with depressive symptoms over short periods of time 39 and that cognitive training in older adults with depression is successful for improving memory, 31 the findings arising from this study suggest that pharmacological (e.g, antidepressants) or nonpharmacological (e.g, cognitive training and exercise) programs targeting memory and/or promotion of hippocampal neurogenesis are worth exploring in this group.
Footnotes
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the University of Sydney Human Ethical Research Committee (Sydney, Australia) and with the Helsinki Declaration of 1975, as revised in 2008.
Acknowledgments
We would like to acknowledge our volunteers for their kind participation in our research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Prof Naismith, Prof Hickie and A/Prof Lewis are funded by fellowships of the National Health and Medical Research Council (NHMRC) of Australia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.