
Abstract
The apolipoprotein (APOE) ε4 allele, a well-described genetic risk factor for late-onset Alzheimer disease (AD), is associated with sleep disturbances even in cognitively normal older adults, although it is not clear whether this association is independent of sleep apnea. We sought to extend previous studies by examining whether cognitively normal older adults without self-reported sleep apnea who carry the APOE ε4 allele have altered sleep characteristics compared to noncarriers. Data from N = 36 (APOE ε4 carriers [n = 9], noncarriers [n = 27]) cognitively normal older adults (Clinical Dementia Rating [CDR] scale = 0) without self-reported sleep apnea were used for these analyses. Participants wore an actigraph for 7 days to determine sleep characteristics. The Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS) were used to assess sleep quality and daytime sleepiness, respectively. The APOE ε4 carriers had a higher number of awakenings compared to the noncarriers (P = .02). There was no significant difference in the PSQI global score and the ESS; however, the PSQI subcomponent of daily disturbances was significantly higher in APOE ε4 carriers (P = .03), indicating increased daytime dysfunction is related to disrupted sleep. This study provides evidence that individuals who are cognitively normal and genetically at risk of AD may have disrupted sleep. These findings are consistent with prior studies and suggest that sleep disruption may be present in the presymptomatic stages of AD.
Keywords
Introduction
Disrupted sleep has been shown to be a risk factor for the development of Alzheimer disease (AD) and often begins in the preclinical stage prior to the onset of observable cognitive symptoms. 1 –3 A large population-based study demonstrated that reduced sleep duration doubled the risk of developing AD 6 to 9 years later. 4 In addition, individuals with high sleep fragmentation had a 1.5-fold increased risk of developing AD compared to individuals with low sleep fragmentation. 5 These studies indicate that disrupted sleep may be an early manifestation of AD and may also contribute to the development of AD.
The apolipoprotein (APOE) gene, located on chromosome 19, has 3 alleles (ε2, ε3, and ε4). The APOE ε4 allele is a well-established risk factor for developing AD, 6 –8 and the carriers of the ε4 allele have a 3- to 4-fold higher risk of developing AD compared to noncarriers. 9
Several studies have linked APOE ε4 with sleep characteristics in individuals with AD, although results have been mixed. 10 –12 Additionally, only 2 studies have examined the association between APOE ε4 and sleep characteristics in cognitively normal older adults. 13,14 Cognitively normal individuals who were APOE ε4 homozygotes had an almost 12-fold increased risk of having sleep problems and ε4 heterozygotes had an almost 5-fold increased risk compared to noncarriers. 13 However, a significant limitation of this study is the use of the Neuropsychiatric Inventory Questionnaire 15 to measure sleep problems, which is limited to only 1 sleep-related item. A recent study 14 compared sleep characteristics and sleep stages between cognitively normal APOE ε4 carriers and noncarriers by using in-home polysomnography, actigraphy, and the Pittsburgh Sleep Quality Index (PSQI). They found that individuals with APOE ε4 had significantly impaired objectively measured sleep quality compared to noncarriers. However, 51.9% of noncarriers and 37.5% of APOE ε4 carriers were diagnosed with sleep apnea (apnea hypopnea index >15) by using in-home polysomnography. Therefore, it was not clear whether the sleep apnea or the APOE ε4 carrier status led to the impairments of sleep characteristics and sleep stages.
Understanding the relationship between APOE ε4 carrier status and sleep characteristics in cognitively normal adults would help to provide groundwork for future studies to develop effective sleep interventions for individuals who are genetically at risk of AD. The purpose of the present study was to extend prior studies examining the relationship between APOE ε4 carrier status and sleep characteristics measured objectively using actigraphy in cognitively normal older adults without self-reported sleep apnea. The secondary aim was to understand the difference between sleep quality and daytime sleepiness using valid and reliable questionnaires in APOE ε4 carriers versus noncarriers. We hypothesized that individuals with APOE ε4 would have disrupted sleep and increased daytime sleepiness compared to noncarriers.
Materials and Methods
Participants
Individuals participating in a longitudinal observational study with annual evaluations at the University of Kansas Alzheimer Disease Center (ADC) 16 were recruited to participate in the current study. Participants were without evidence of cognitive decline (Clinical Dementia Rating [CDR] = 0 17 ) and were without a self-reported diagnosis of sleep apnea. A trained clinician (advanced nurse practitioner or neurologist) completed the CDR 17 to carefully screen out individuals with cognitive impairments and AD, and a trained psychometrician performed the standard cognitive battery tests. Standard cognitive battery tests included measures of memory (Logical Memory IA and IIA 18 ), attention (Digit Span 18 ), executive function (Trail Making B 19 ), processing speed (Trail Making A, 19 Digit Symbol 20 ), and language (Semantic Fluency, 21 Boston Naming Test 22 ). The clinical and cognitive results for each participant were reviewed at a consensus diagnostic conference, which include all the ADC neurologists, nurse practitioners, and psychometricians who see participants in the observational study. Normal cognitive status is defined as a CDR 17 = 0 and no clinically significant deficits on the cognitive battery tests. Diagnosis of sleep apnea was ascertained through self-reported answer to the question “Do you have a diagnosis of sleep apnea?”
The study was performed in accordance with the institutional review board of University of Kansas Medical Center. Informed consent was obtained in writing from each individual prior to participation in the study. Information regarding age, sex, race, body mass index, years of education, sleep aid (such as melatonin, zolpidem, benzodiazepines, zaleplon, eszopiclone, ramelteon) and stimulant (such as amphetamine, methylphenidate, methamphetamine) usage, and APOE status was obtained as part of the longitudinal study. Apolipoprotein genotype status was determined by restriction enzyme isotyping. 23 One individual with an ε2ε4 profile was not included in the sample because the ε2 allele has been shown to have a protective effect on developing AD 24 and is, therefore, thought to neutralize the effect of the ε4 allele. 25
Sleep Measurements
Participants wore an actigraph (ActiGraph GT9X; Actigraph LLC, Pensacola, Florida) on their nondominant wrist for 7 days and returned the actigraph using a postage paid envelope. An actigraph is a portable device that records movement over extended periods of time and has been used extensively in the study of sleep and circadian rhythms. 26 ActiGraph has been validated to use in sleep research with an adult population. 27 The outcome variables of interest include total sleep time, sleep latency, sleep efficiency, wake after sleep onset (WASO), and number of awakenings. Actigraph data were analyzed using the ActiLife software version 6.11.8. The Choi algorithm was used to analyze wear time validation. 28 This algorithm was verified in an adult population by comparing the data from the actigraph with the actual wear time by 24-hour monitoring in a whole room with an indirect calorimeter. 28 Actigraph data were included in the analysis if wear time validation indicated the device was worn for a minimum 600 minutes for at least 4 days of wear time out of the 7 days. 29 None of the participants wore the actigraph less than this criterion. The sleep algorithm that was used in the analysis was Cole Kripke, 30 which has been validated for use in adult populations by comparing the nighttime sleep characteristic results from actigraphy with polysomnography. 30 This algorithm differentiated sleep from wakefulness with at least 88% accuracy in a variety of groups including adult populations. 30 Participants also completed a sleep log during the time they wore the actigraph. Participants were asked to provide napping time, time in bed, time in bed with lights out to sleep, time between light out to being asleep (latency), time woke up in morning, and time got out of bed. The sleep log was used to verify the actigraph data. If the difference in time in bed and time out of bed was ≤30 minutes between reported in the sleep log and the actigraph, the actigraph data were used for scoring. If the difference in time in bed and time of out of bed was >30 minutes between reported in the sleep log and the actigraph, the sleep graphs generated from the ActiLife software were visually inspected for activity spikes. Time in bed typically is reflected by a sharp decrease in the activity spikes, and time out bed is typically reflected by an immediate increase in the activity spikes in the software. 31 After visually inspecting the activity spikes and comparing the data between the sleep log and the ActiLife software, 2 trained research personnel determined whether to manually enter the sleep periods from the sleep log or to maintain the sleep periods based on the software. Interrater reliability was determined by an a priori decision to randomly compare 10% of the available files. Blackwell et al 32 investigated the actigraph scoring reliability between 2 scorers for each actigraph variables and found a high level of agreement (range: 0.84-0.99). The interclass correlation coefficient and 95% confidence interval were calculated for time in bed, time out of bed, and WASO. Results for each outcomes are as follows: time in bed: 0.93 (0.88-0.96), time out of bed: 0.99 (0.99-0.99), and WASO: 0.96 (0.93-0.98). These findings demonstrated that there was a high level of agreement in scoring between the research personnel.
Research staff administrated the PSQI 33 to participants to assess self-perception of sleep quality and the Epworth Sleepiness Scale (ESS) 34 to assess self-perception of daytime sleepiness. The PSQI is a valid and reliable measure to assess self-perception of sleep quality and consists of 19 questions. These 19 questions are rated on a scale of 0 to 3, with 0 representing no sleep difficulty and 3 representing severe sleep difficulties. The 3 subcomponents of the PSQI (sleep efficiency, perceived sleep quality, and daily disturbances) were calculated based on the study by Cole et al. 35 Epworth Sleepiness Scale is a self-reported measure of daytime sleepiness which assesses the rate of dozing in 8 different scenarios of daily activities. Each question has a 4-point Likert scale to rate how likely the participants would be to doze. A higher score indicates higher daytime sleepiness.
Statistical Analysis
Data analysis was performed by using SPSS 22 software (SPSS Inc, Chicago, Illinois), and the significance level was set at .05. Data were tested for normality using the Kolmogorov-Smirnov test and found to be normally distributed. However, for a rigorous analysis, nonparametric tests were selected to analyze the data. Demographic differences between APOE ε4 carriers and noncarriers were tested by using χ2 and Mann-Whitney U tests. The value of the sleep characteristics was obtained from the actigraph for each night and then averaged across the 7 nights. Mann-Whitney U tests were used to determine differences in sleep characteristics, PSQI global score and 3 subcomponents, and ESS between APOE ε4 carriers and noncarriers. Effect size (Cohen d) was used to examine the magnitude of difference between the groups and interpreted as small d = 0.2, medium d = 0.5, and large d = 0.8. 36
Results
Baseline Characteristics
Thirty-six individuals participated in the study: n = 9 APOE ε4 carriers (ε3ε4 [n = 8], ε4ε4 [n = 1]) and n = 27 noncarriers (ε2ε3 [n = 4], ε3ε3 [n = 23]). Demographic characteristics did not significantly differ between the 2 groups (Table 1).
Demographic Characteristics.a
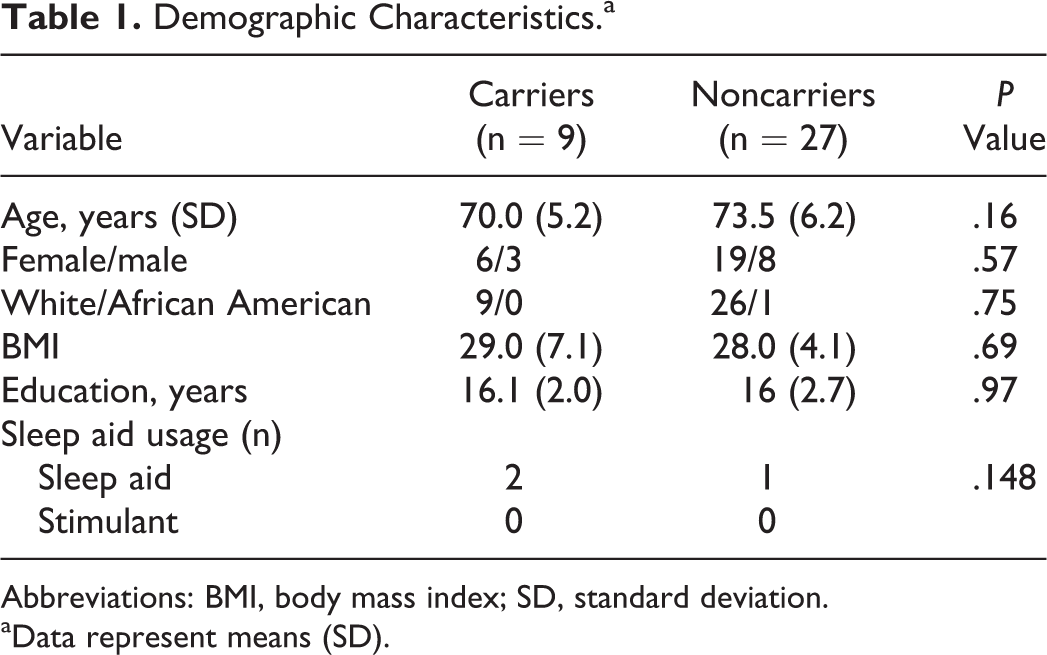
Abbreviations: BMI, body mass index; SD, standard deviation.
aData represent means (SD).
Actigraph and Self-Reported Sleep Outcomes
For the actigraph variables, APOE ε4 carriers had a significantly higher number of awakenings compared to noncarriers (P = .02, d = 1.03; Figure 1). There were no statistically significant group differences in sleep latency, sleep efficiency, total sleep time, and WASO (Table 2).
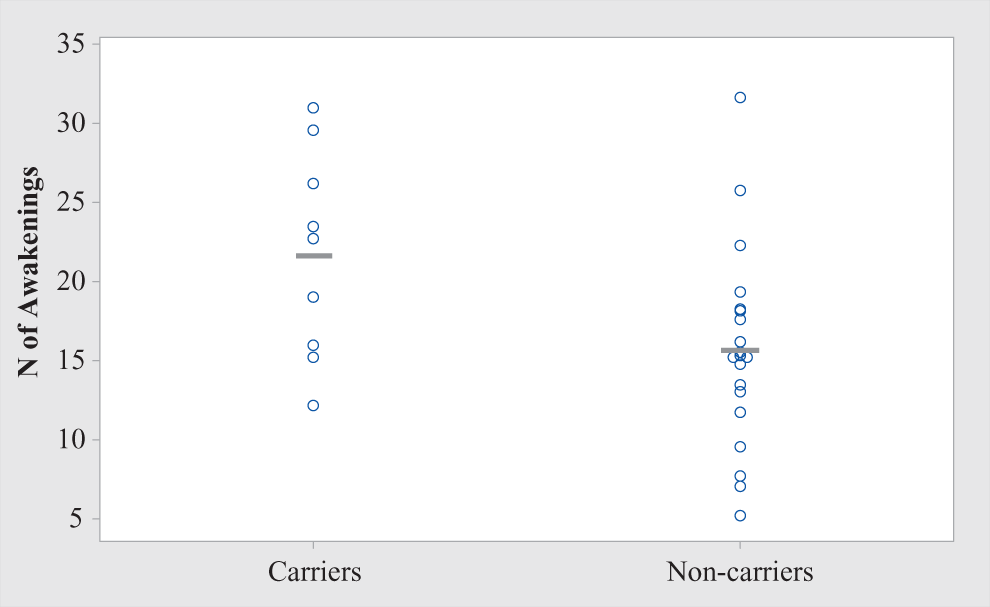
Number of awakenings data plot among apolipoprotein (APOE) ε4 carriers and noncarriers.
Actigraph Results.a
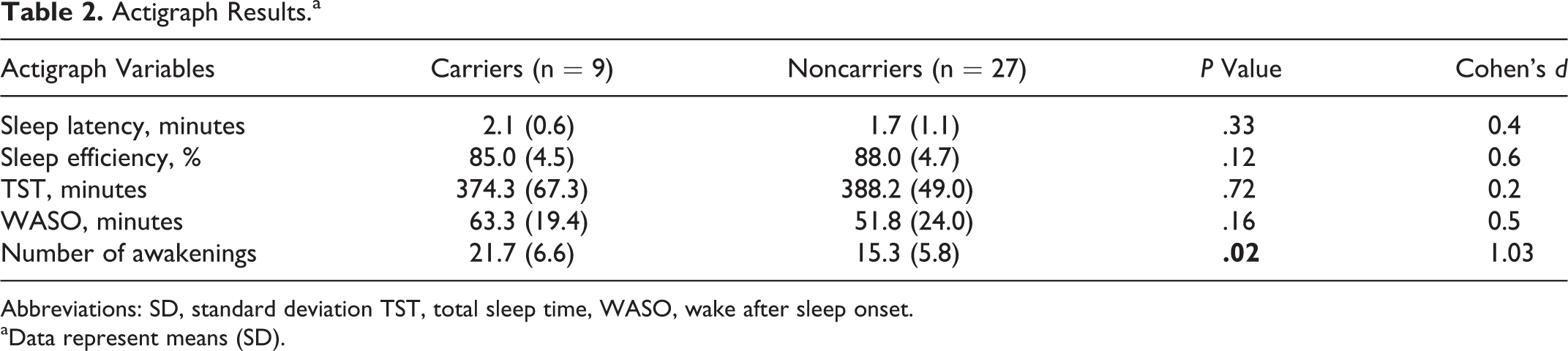
Abbreviations: SD, standard deviation TST, total sleep time, WASO, wake after sleep onset.
aData represent means (SD).
The self-report sleep outcomes (PSQI, ESS) were completed by 21 of the 36 participants. There was no significant difference between groups for sleep quality measured by global PSQI score (P = .47, d = 0.3) and daytime sleepiness measured by ESS (P = .97, d = 0.08; Table 3). However, the daily disturbances (items of sleep disturbances and daytime dysfunction) subcomponent of the PSQI was significantly higher in APOE ε4 carriers compared to noncarriers (P = .03, d = 1.13; Figure 2).
Self-Reported Sleep Results.a
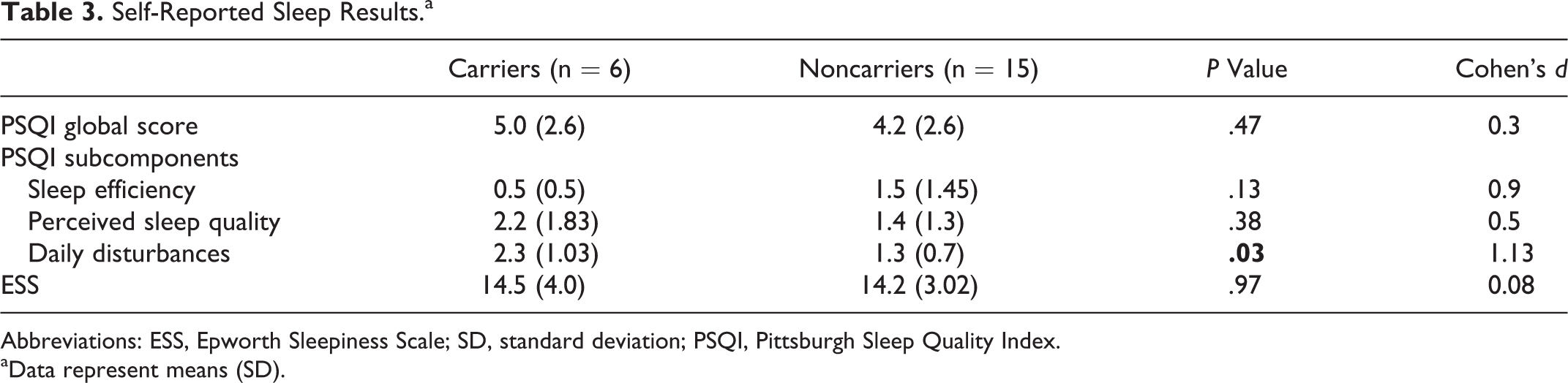
Abbreviations: ESS, Epworth Sleepiness Scale; SD, standard deviation; PSQI, Pittsburgh Sleep Quality Index.
aData represent means (SD).
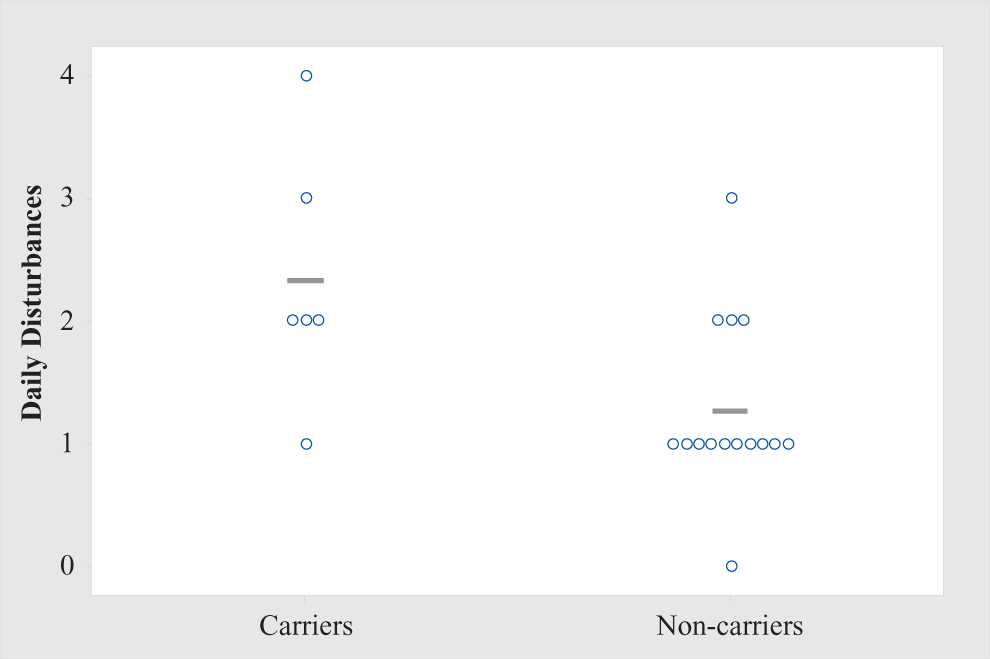
Daily disturbances data plot among apolipoprotein (APOE) ε4 carriers and noncarriers.
The significant results remained when the analyses were conducted without the individual with ε4ε4 alleles to examine the relationship between ε3ε4 carrying status in particular and sleep characteristics. Therefore, these results are not reported in the article.
Discussion
The present study provides evidence that cognitively normal APOE ε4 carriers without self-reported sleep apnea may experience disrupted sleep. Similar total sleep times but greater number of awakenings was observed in those with the APOE ε4 allele. In addition, although the self-perceived sleep quality was not significantly different between the groups, the daily disturbances subcomponent was significantly higher in APOE ε4 carriers, suggesting daytime dysfunction related to sleep disturbances. These results are consistent with prior studies 13,14 and extend these studies by removing the confound of sleep apnea based on self-report. Removing the confound of sleep apnea is important as sleep apnea is associated with decreased total sleep time and sleep efficiency. 37
The possible mechanisms of how APOE e4 contributes to impaired sleep characteristics are unclear. The mechanisms may be related to the role of APOE ε4 in contributing to brain structural and functional abnormalities. The APOE ε4 allele has been associated with alterations in brain structural integrity including increased cortical atrophy. 38,39 In addition, the APOE ε4 allele has been shown to regulate amyloid-beta (Aβ) aggregation and decrease Aβ clearance from the brain, which can lead to an increase of Aβ plaques in the interstitial fluid. 40 An animal study demonstrated that Aβ plaque aggregation disrupts sleep and sleep disruption exacerbates Aβ pathology in the brain. 41 Therefore, Aβ plaque accumulation and impaired sleep characteristics appear to be bidirectional. 1,2 Previous work has demonstrated that increased nocturnal number of awakenings was associated with Aβ deposition 42,43 and decreased brain gray matter volume. 44 Therefore, it is possible that the APOE ε4 allele decreases Aβ clearance from the brain, 40 which may then interrupt the sleep centers contributing to sleep disruptions. The sleep disruptions may further perpetuate the accumulation of Aβ, contributing to alterations in brain structural integrity and increasing the risk of developing AD. 45 Alternatively, it is possible that individuals with preexisting sleep issues who have APOE ε4 are more susceptible to Aβ deposition in the brain, which in turns aggravates the sleep issues. In addition, the APOE ε4 allele is thought to disrupt cerebral blood flow. 46 Disruption of cerebral blood flow can affect brain protein synthesis and contribute to neuronal dysfunction in the brain. 47 These detrimental events could eventually affect the sleep regions in the brain and may lead to the impairments of sleep characteristics. 48 The exact mechanism of how the APOE ε4 allele contributes to impaired sleep characteristics warrants further investigation.
Currently, the health-care cost of AD is approximately $236 billion USD, and the cost is expected to double by 2050. 49 Therefore, effective treatment strategies are needed to delay and prevent AD. Individuals with the APOE ε4 allele who had better sleep consolidation had a lower risk of developing AD and had lower density of neurofibrillary tangles than individuals with poor sleep consolidation. 50 A large population-based study demonstrated that among individuals with sleep disturbances, approximately 26% were APOE ε4 carriers. 13 While modifying the APOE ε4 genotype is not possible at this point in time, it is possible that providing an efficacious treatment for sleep disruptions may help to attenuate the increased risk of developing AD in APOE ε4 carriers. Future longitudinal studies are needed to assess the effect of sleep treatment strategies for delaying the onset of AD in individuals with an APOE ε4 allele. It has been estimated that delaying the onset of AD by 5 years would reduce the burden on AD by 43% by 2050. 51
This study has several limitations. The sample size for this study was small, but large observed effect sizes were detected for the difference in the number of awakenings and daily disturbances between carriers and noncarriers (Tables 2 and 3). Due to the cross-sectional design of the study, it is not possible to understand whether carrying the APOE ε4 allele may contribute to the development of sleep impairments or if experiencing sleep impairments amplifies the negative effects of the APOE ε4 allele. Longitudinal studies are needed to demonstrate such directions. Another limitation is that participants were not asked to refrain from taking medications, which might influence results. However, only 2 participants from the APOE ε4 group and 1 participant from the noncarriers reported taking sleep aid (Table 1). Lastly, individuals indicated the presence or absence of diagnosed sleep apnea through self-report, which may mean that individuals were included who have undiagnosed sleep apnea.
A strength of this study is that participants were carefully screened for cognitive impairment by using sensitive diagnostic method (CDR 17 and a standard cognitive battery), and only individuals without evidence of functional or cognitive decline were included in the study. Secondly, both objective (actigraphy) and self-report (PSQI, ESS) measurement tools were used to assess different aspects of the sleep. Benefits of using actigraphy compared to polysomnography are actigraphy is lower in cost, is ecologically valid, and is fairly unobtrusive to wear. 52 In addition, the PSQI and ESS are reliable and valid tools to assess self-report sleep quality and daytime sleepiness. 53
Conclusion
In conclusion, cognitively normal older APOE ε4 carriers without self-reported sleep apnea had disrupted sleep compared to noncarriers using objective and subjective measures. These findings are consistent with previous studies and may suggest that disrupted sleep could be an early manifestation of AD and may be present in its presymptomatic stages. Future studies are needed to verify whether disrupted sleep contributes to the increased risk of developing AD and whether sleep interventions would reduce the risk of developing of AD in individuals with the APOE ε4 allele.
Footnotes
Acknowledgments
The authors thank the Clinical and Data Management cores of the University of Kansas Alzheimer’s Disease Center as well as Chelsea Neumann, SPT, David Klauss, SPT, Emily Pahls, SPT, Erin Goodman, SPT, Garrett Brockmeyer, SPT, Christin Burgess, SPT, Madison Crocker, SPT, Brooke Katterhenry, SPT, Tad Parsons, SPT, and Elizabeth Shelly, SPT for their assistance with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a grant from the National Institute on Aging P30 AG035982 and by the Foundation for Physical Therapy through the Magistro Family Foundation Research Grant.