
Abstract
Objective:
The aim of this study was to identify factors that are associated with cognitive decline in the long-term follow-up after hip fractures in previously nondemented patients.
Methods:
A consecutive series of 402 patients with hip fractures admitted to our university hospital were analyzed. After exclusion of all patients with preexisting dementia, 266 patients were included, of which 188 could be examined 6 months after surgery. Additional to several demographic data, cognitive ability was assessed using the Mini-Mental State Examination (MMSE). Patients with 19 or less points on the MMSE were considered demented. Furthermore, geriatric scores were recorded, as well as perioperative medical complications. Mini-Mental State Examination was performed again 6 months after surgery.
Results:
Of 188 previously nondemented patients, 12 (6.4%) patients showed a cognitive decline during the 6 months of follow-up. Multivariate regression analysis showed that age (P = .040) and medical complications (P = .048) were the only significant independent influencing factors for cognitive decline.
Conclusions:
In our patient population, the incidence of dementia exceeded the average age-appropriate cognitive decline. Significant independent influencing factors for cognitive decline were age and medical complications.
Introduction
With an incidence of >150/100 000 persons per year in the population aged 50 years and older in industrialized countries, 1,2 hip fractures are one of the major health problems in the elderly population. Hip fractures are still associated with high rates of mortality, with 1-year mortality rates reported between 18% and 31%. 2 –7 There is also a high morbidity following hip fractures, with estimated 1.75 million disability-adjusted life years (DALYs) lost due to hip fractures in 1990, 8 and 0.82 million DALYs lost in men and 1.53 million DALYs lost in women due to hip fractures in 2000. 9 Furthermore, 35% to 64% of previously noninstitutionalized patients need to be admitted to nursing homes after hip fracture, 6,10 and 29% to 90% of the patients retain permanent functional limitations. 6,10 –13
In this context, an important aim after hip fracture is avoiding institutionalization and regaining the independence and status in activities of daily living that a patient had before the fracture. Whether this can be achieved depends not only on the physical status and functional outcome after surgery but also on the patient’s cognitive status. The cognitive status is influencing the outcome after hip fracture in at least 2 ways: On one hand, only nondemented patients can handle daily life autonomously in their home environment. On the other hand, cognitive status also influences the functional outcome after hip fracture in several ways, for example, in terms of a higher rate of postoperative complications, 14 worse functional outcome with lower scores in the Barthel and Tinetti Index, 15,16 poorer rehabilitation outcome, 17 –19 and higher fall risk 20 in demented patients. However, specific orthogeriatric rehabilitation programs can improve the outcome of demented hip fracture patients. 21,22 Concerning the adverse effects of dementia on the outcome after hip fracture and the special needs of demented patients regarding rehabilitation programs, it seems to be crucial to detect and, if possible, prevent the onset of dementia in hip fracture patients. In this context, it is necessary to identify risk factors for the development of dementia after hip fracture.
Only a limited number of studies have evaluated the development of dementia after hip fracture so far. Some studies could show that the risk of cognitive impairment is increased after hip fractures in the short-term 23,24 and long-term follow-up. 19,25 However, little is known about factors influencing the development of dementia after hip fractures in previously nondemented patients. The aim of this study was to analyze which factors are associated with cognitive decline in previously nondemented patients 6 months after hip fracture.
Methods
Study Design and Patients
The current investigation is a secondary analysis of a prospective observational study including a total of 402 patients with hip fractures aged 60 years and older who were admitted to our university hospital for surgical fracture treatment. 26 The recruitment period was from 1 April, 2009, to 30 September, 2011. Institutional review board approval was obtained from the ethics committee (AZ 175/08). All of the patients provided written informed consent for participation in the study. Apart from the exclusion criteria of malignancy-related fractures and polytrauma (injury severity score ≥ 16), 27 we excluded 133 demented patients due to prior dementia (Mini-Mental State Examination [MMSE] of ≤19 points at the time of admission to the hospital) for this subgroup analysis. Additionally, 3 patients were excluded due to incomplete MMSE on admission, leaving 266 patients who met the inclusion criteria.
Methods
Assessment of cognitive status
Cognitive ability was assessed using the MMSE. 28 The MMSE is a well-established, reliable, valid, and brief cognitive screening instrument, which has a high interrater reliability and is easy to administer. The instrument has standardized instructions, takes a mean of 15 minutes to administer, and examines attention, memory (orientation, recall of words, recognition of sentences, and drawings), and initiation and maintenance of verbal and motor responses. Individual points are assigned to the subscales, with a total score of 30 points representing optimal performance. In accordance with the German guidelines for dementia, 29 we have considered patients with 19 or fewer points demented. Mini-Mental State Examination was assessed at the day of admission to the hospital and again 6 months after the surgery. Both times, the examination was performed by a member of our study group (physician or specially trained medical student). For the 6-month follow-up examination, the patients either came to the hospital or were visited at their place of residence.
Patient data
Apart from sociodemographic patient data (age, sex), the type of fracture, preoperative American Society of Anesthesiologists (ASA) score, 30 prefracture Charlson comorbidity index (CCI), 31 and prefracture Barthel index (BI) 32 were recorded. Barthel index was assessed at the day of admission to the hospital retrospectively, regarding the last week before the fracture occurred. In addition, length of hospital stay and perioperative medical complications were documented. Medical complications therefore were defined as any unanticipated event or additional pathology that occurred during the in-patient stay before, during, or after the surgery and was documented in the patient’s report or discharge letter.
Outcome parameter
The primary outcome measurement was cognitive ability 6 months after hip fracture. The end point was dichotomized as follows: patients with a MMSE score of 19 or less were considered as cognitively declined; patients with a score of 20 or more were considered as not cognitively declined.
Data management and analysis
Data were collected in a FileMaker database (FileMaker Inc, Santa Clara, California). We performed double entry with a plausibility check to monitor for data quality. IBM SPSS Statistics 22 (Statistical Package for the Social Sciences; IBM Corporation, Armonk, New York) was used for statistical analysis. The data were presented as frequencies and percentages for dichotomous variables and as means and 95% confidence intervals (CIs) for numerous parameters. For bivariate analysis, an unpaired Student t test or Wilcoxon rank sum test and χ2 test or Fisher exact test were calculated as appropriate depending on normal distribution. The Kolmogorov-Smirnov test was used to test for normal distribution. For all tests, statistical significance was assumed at P < .05.
Finally, multivariate logistic regression analysis with backward selection was performed to detect independent influencing factors (inclusion at P < .05, exclusion at P > .10). This analysis included the following covariables: age, gender, ASA, CCI, BI, initial MMSE, and medical complications during acute care.
Results
Of the 266 patients included in this subgroup analysis, a total of 12 patients died during acute care. By the follow-up investigation 6 months after fracture, another 26 patients had died. Additionally, 36 patients were lost to follow-up or declined further participation in the study, and 4 patients had to be excluded due to incomplete MMSE at the 6-month follow-up examination. Figure 1 shows the flowchart of the study with the number of patients excluded because of death, loss to follow-up, or incomplete data. Ultimately, 188 patients could be analyzed 6 months after surgery. The mean age of those patients was 79 years (95% CI: 78-80); 75% were female. Detailed patients’ characteristics are shown in Table 1.
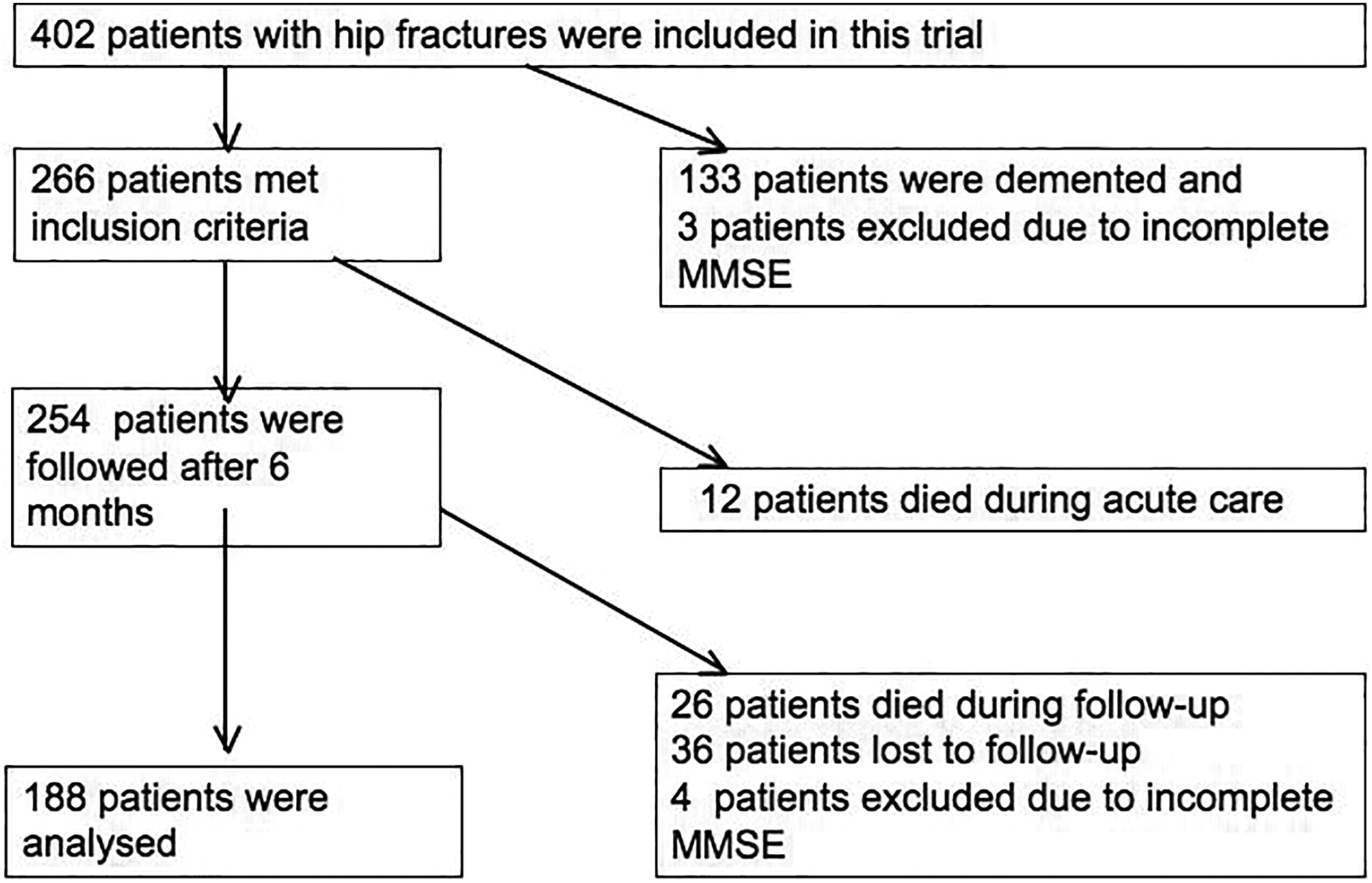
Flowchart of the study.
Baseline Data of Patients.
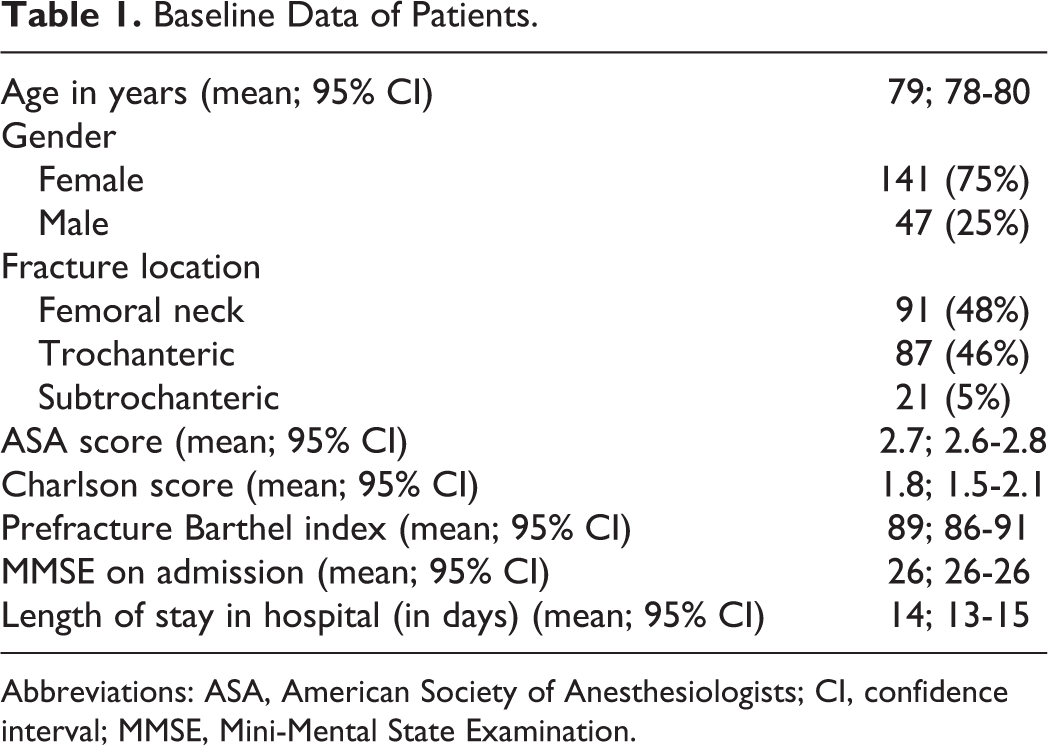
Abbreviations: ASA, American Society of Anesthesiologists; CI, confidence interval; MMSE, Mini-Mental State Examination.
The number of reported medical complications was 50, though 4 patients had more than 1 complication. The most frequently observed complications were urinary tract infections, which occurred in 43 patients. All medical complications are listed in Table 2.
Medical Complications.
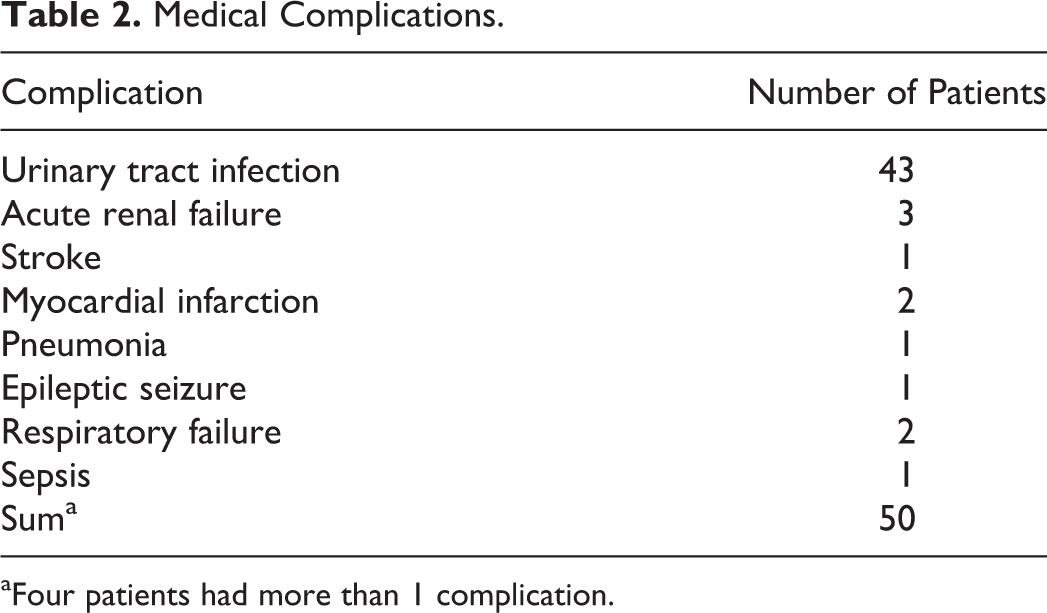
aFour patients had more than 1 complication.
Twelve (6.4%) patients had cognitive decline 6 months after surgery, as measured with the MMSE. Patients who had a cognitive decline were significantly older than patients without cognitive decline (84 vs 79 years, P = .020) and had a significantly lower prefracture BI (81 vs 89 points, P = .024), a significantly lower MMSE score at admission to hospital (23 vs 26 points, P = .001), and a significantly higher number of medical complications (58.3% vs 24.4%, P = .017; Table 3). Multivariate regression analysis for cognitive decline after 6 months showed that age (odds ratio [OR] = 1.104; 95% CI = 1.005-1.214; P = .040) and medical complications (OR = 4.016; 95% CI = 1.012-15.942; P = .048) both were significant independent influencing factors for cognitive decline (Table 4). Preexisting comorbidities, measured by ASA score (OR = 1.699; 95% CI = 0.449-6.422; P = .435) and CCI (OR = 0.735; 95% CI = 0.451-1.198; P = .217), were not significant in multivariate regression analysis.
Patients With Cognitive Decline Compared to Patients Without Cognitive Decline.
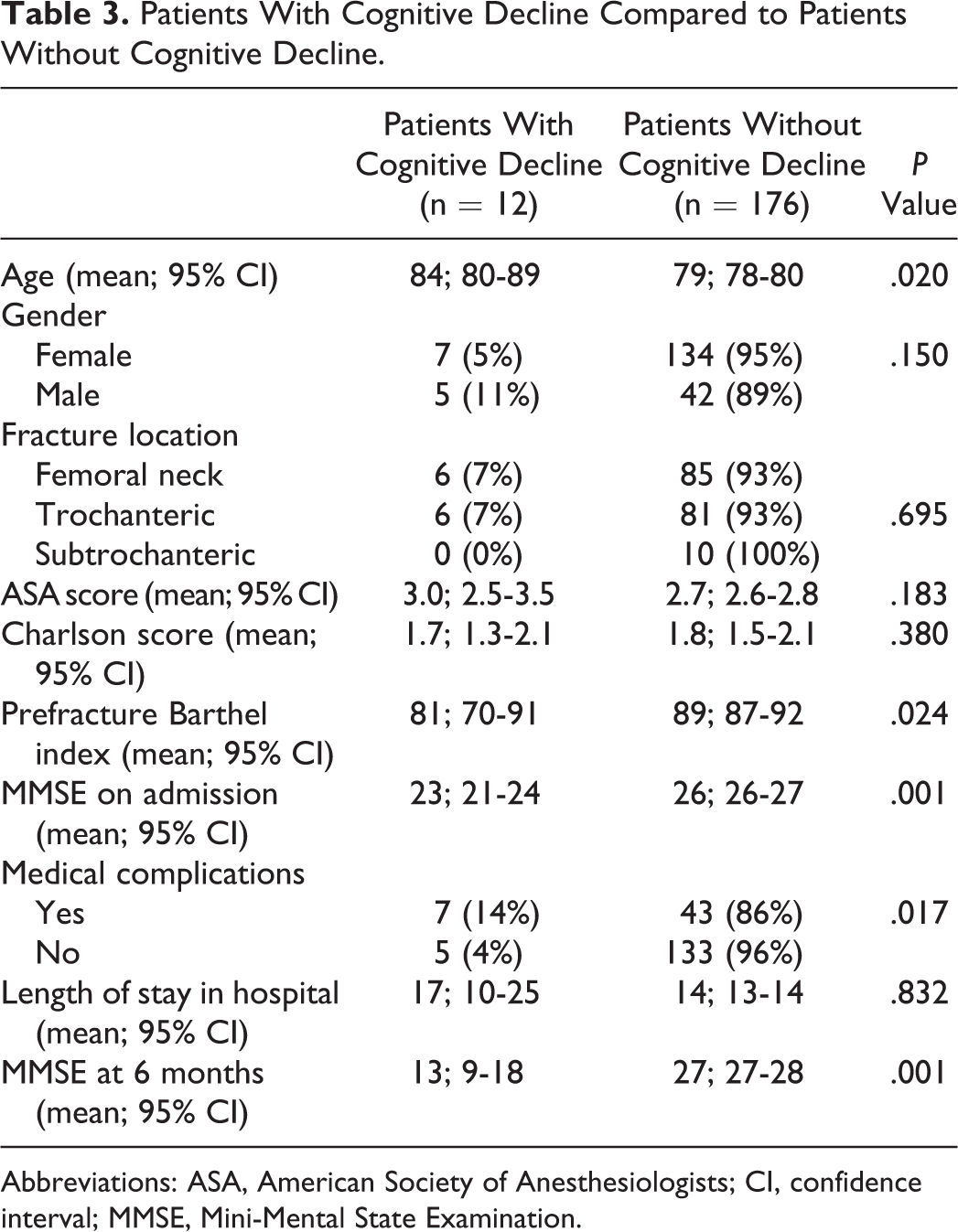
Abbreviations: ASA, American Society of Anesthesiologists; CI, confidence interval; MMSE, Mini-Mental State Examination.
Multivariate Regression Analysis for Cognitive Decline After 6 Months.a
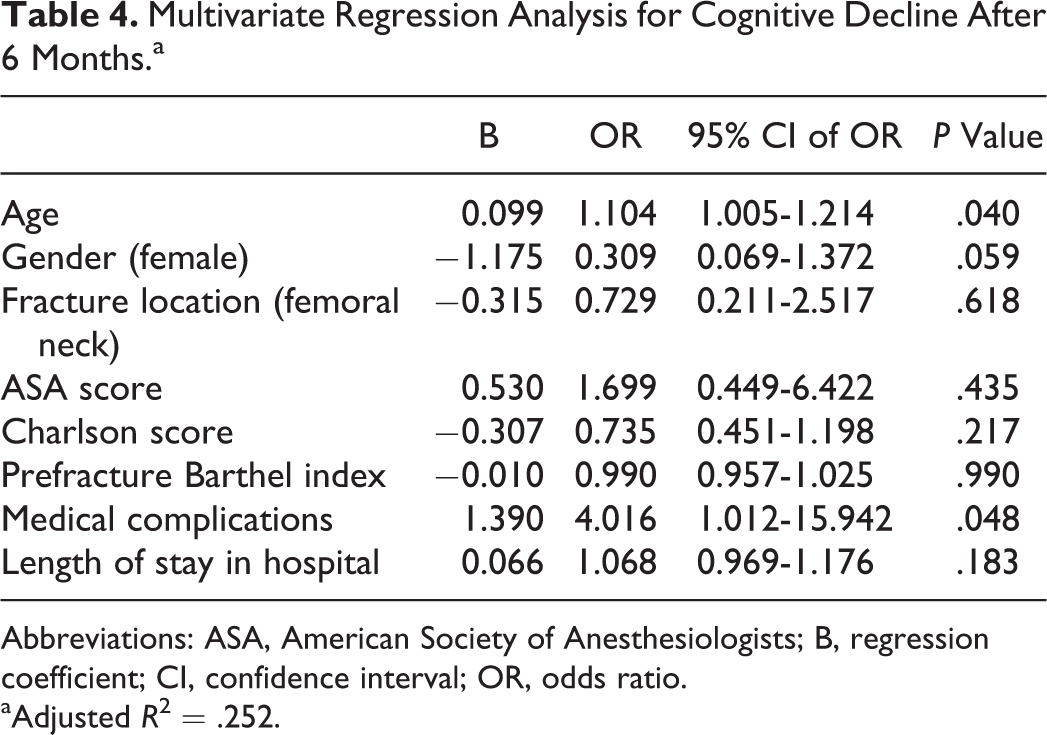
Abbreviations: ASA, American Society of Anesthesiologists; B, regression coefficient; CI, confidence interval; OR, odds ratio.
aAdjusted R 2 = .252.
Discussion
The outcome after hip fractures is dependent not only on a patient’s physical recovery after surgery but also on his or her mental status. However, not much is known about cognitive decline following hip fractures in previously nondemented patients. The aim of this study therefore was to identify factors that are associated with cognitive decline in a 6-month period after hip fractures.
We found an incidence of 6.4% for dementia 6 months after hip fracture in previously nondemented patients. On one hand, this could be seen as a normal, age-appropriate process. On the other hand, there is an estimated incidence of dementia in the German population aged 65 years and older between 1.4% and 3.2% per year. 33 –36 The estimated incidence of dementia in the age group of 75 to 79 years (corresponding to the mean age of 79 years in our population) is 1.33% per year in men and 3.01% in women, 33,34 which is considerably lower than the incidence of 6.4% observed in our study population during the follow-up period of only 6 months. The high incidence of dementia after hip fractures consequently seems to exceed the average age-appropriate cognitive decline.
Using multivariate regression analysis for cognitive decline after 6 months, we found age, which cannot be influenced, and medical complications, which could be avoided at least in some cases, as significant independent influencing factors for cognitive decline. Consequently, an important issue should be to minimize the patients’ risk of suffering medical complications, as it seems that, in this situation, another hit additional to the fracture and surgery cannot be compensated by the mostly frail patients. In this context, early operation, short operation time, and less invasive operation techniques are important matters 37 in order to avoid medical complications. A possibility to reduce the risk of postoperative medical complications is collaboration with consulting geriatricians or special orthogeriatric wards. A study by Shyu et al showed that special interdisciplinary interventions could significantly lower the risk of cognitive impairment 6 months after hip fracture. 38 Furthermore, considering that the most frequently observed medical complications in our study were urinary tract infections, early mobilization is essential for avoiding urinary tract infections caused by urinary catheters needed because of immobility. On the other hand, medical complications probably rather occur in patients with a lower mobility level and stronger frailty before the fracture. Consequently, medical complications, although controlled for several variables in our analysis, might be a surrogate parameter and not be seen as the only reason for cognitive decline after hip fracture. Previous studies have indicated that frailty is associated with a higher incidence of postoperative complications after different kinds of surgeries. 39 –41 In this respect, this factor is only influenceable to some extent. The assumption that cognitive decline might be associated with a lower level of mobility before the fracture is supported by the fact that patients with cognitive decline at 6 months after the fracture had a significantly lower prefracture BI than patients without cognitive decline.
Another reason for the negative impact of medical complications on the cognitive outcome after hip fractures might be the fact that the occurrence of medical complications causes belated mobilization. However, early postoperative mobilization seems to be crucial to prevent cognitive decline, since immobilization could be identified as a main risk factor for cognitive decline in hospitalized older patients. 42 Moreover, several studies have demonstrated that few days and even hours of immobilization induce brain plasticity. 43,44
In contrast to immobility, comorbidities, however, do not seem to have a crucial influence on the cognitive status after hip fractures, as there was no significant difference concerning prefracture comorbidities measured by Charlson score between patients with and without cognitive decline. Another important point in this context is the fact that patients with cognitive decline at 6 months after the trauma had a significantly lower MMSE on admission, which leads to the assumption that preexisting mild cognitive impairment before the fracture is a strong risk factor for ending up demented in the long-term development. In this regard, it seems reasonable to develop some strategies, especially for patients with mild cognitive impairment, to prevent further cognitive decline. This might particularly concern the aspect of helping the patients to reorientate themselves after the surgery in the unfamiliar environment of the hospital and to familiarize them with the accompanying processes therein.
At last, general anesthesia with inhaled anesthetics might also contribute to cognitive decline after hip fractures, as there are hints that inhaled anesthetics increase the blood–brain barrier permeability and thus could cause postoperative cognitive decline. 45
Limitations
Our investigation is limited by some factors. First, for this subgroup analysis, 133 (33.1%) of 402 patients had to be excluded due to preexisting dementia. This appears to be a comparatively high rate of demented patients. However, demented patients have a multiply increased risk of falling and thereby suffering a hip fracture, 46 –48 which explains the higher prevalence of dementia in hip fracture patients than in the age-appropriate standard population. 49 Second, the number of patients with cognitive decline in this study is comparatively small (n = 12). Furthermore, some limitations concerning the data acquisition have to be stated. First, prefracture BI was evaluated retrospectively at the day of admission to the hospital, regarding the last week before the fracture occurred. Second, the initial MMSE score was recorded at the day of admission to the hospital. However, previous studies have indicated that a relevant share of hip fracture patients suffer from preoperative delirium or that the patients even fall because of a delirium. 50 For this reason, it cannot be ruled out that in some patients, the baseline MMSE score might have been impaired by an undetected preoperative delirium. Despite knowing of these limitations, the baseline data had to be recorded as described for reasons of practicability. Another limitation is the multifactorial genesis of dementia. Although we could identify some single influencing factors involved in the development of cognitive decline, the complex combination of several factors acting together in the genesis of dementia of course cannot be measured.
Conclusion
Our results show that advanced age and medical complications are significant independent influencing factors for cognitive decline after hip fractures. Consequently, special attention should be paid to avoiding medical complications.
Furthermore, a crucial step might be to identify patients with mild cognitive impairment as a risk group for major cognitive decline and to treat them in an interdisciplinary and interprofessional team to prevent further cognitive deterioration.
Footnotes
Authors’ Note
All works were completed at the Center for Orthopaedics and Trauma Surgery, University Hospital Giessen and Marburg, Marburg. This manuscript has not been presented at a meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.