
Abstract
Background:
Geriatric depression is a heterogeneous disorder that increases morbidity and mortality in a population that is already vulnerable. Predicting response and remission to antidepressants could help clinicians to optimize the management of antidepressants and reduce the consequences of depression.
Method:
The aim of this article is to present results of a systematic review of the literature on predictive factors related to antidepressant response and remission in older adults with depression.
Main Findings:
We identified sociodemographic, clinical, neuropsychological, neuroimaging, and genetic factors that could be potential predictors of outcomes. Inconsistent findings and methodological differences among studies, however, limit the generalizability and application of these predictors in clinical practice. The results of our review confirm that geriatric depression includes many subgroups of patients with particular endophenotypes that may influence the course of depression.
Conclusion:
Further studies are needed to characterize depression subgroups in order to better understand the pathophysiology of late life depression and to find specific predictors for each group of patients.
Introduction
Major depressive disorder (MDD) is a widespread psychiatric disorder that is associated with high rates of morbidity and mortality and a substantial loss of productivity and quality of life. 1,2 In older adults, the estimated prevalence of MDD ranges from 2% to 10%, with milder forms of depression affecting 20% to 30% of older adults. 3,4 Geriatric depression takes a staggering toll through personal suffering, family disruption, increased use of health-care services, and overall mortality. In addition, MDD worsens the prognosis for the comorbid medical illnesses prevalent in this population. In clinical practice, the large variety of psychotropic medications currently available offers a wide array of treatment strategies but raises questions regarding the selection of the most appropriate therapy. In most evidence-based guidelines, general principles for treating older adults are similar to those described for younger adults, and this may reflect the scarcity of research focused on older adult patients. Furthermore, special vigilance is needed in this population for adverse drug reactions, potential drug interactions, and exacerbation of preexisting somatic comorbidities. Moreover, the probability of response and remission in mood disorders drops considerably with each successive treatment failure, highlighting the need for planning short- and long-term individualized treatment.
Choosing an appropriate therapy for an older adult with MDD could be greatly facilitated by the identification of factors that reliably predict antidepressant response. Literature on the potential predictive factors of response or remission, mostly focused on young adults, has identified clinical, neurocognitive, neurobiological, and genetic parameters. Among the clinical parameters, comorbid anxiety was associated with lower rates of remission, independent of depression severity in large cohort studies. 5,6 Moreover, several studies suggest that psychomotor speed may provide prognostic information concerning antidepressant response. Among the neurocognitive parameters, Taylor et al compared performances on verbal fluency and the Stroop test between responders and nonresponders to 12 weeks of fluoxetine and found that nonresponders showed poorer word fluency and reduced processing speed with no differences in executive functioning. 7 Bruder et al replicated these data with patients receiving escitalopram or citalopram but found that nonresponders to bupropion alone tended to have a higher performance in verbal fluency test than responders. 8 Gorlyn et al extended these considerations to global cognitive functioning and found a significantly lower performance in all neuropsychological domains among nonresponders to selective serotonin reuptake inhibitor (SSRI). 9
From a neurobiological point of view, inflammatory biomarkers (ie, the levels of inflammatory markers such as C-reactive protein) and normalization during treatment of pretreatment frontal hypometabolism appeared to be significant prognostic markers for response. 10,11 Additionally, pharmacogenomic differences between individuals could also modulate the response to antidepressants. A large body of evidence showed an association between SSRI response and presence of long or short allele of the promoter of the serotonin transporter. The long allele is associated with an increased expression of this gene and appears to be a predictor of response and remission in caucasians. 12 In the GENDEP project, the authors found several associations between candidate gene variants and response to antidepressants. 13 Although promising, these markers have been explored in studies assessing young adult samples, and the applicability of these results to older adults is not clear.
In this article, we report the results of a systematic review of the literature assessing predictive factors of response or remission to antidepressant treatment in unipolar geriatric depression. A recent meta-analysis found that depression severity, comorbid anxiety, current episode duration, early improvement, and executive dysfunction were significant predictors of outcomes in geriatric depression. 14 We were interested in exploring these predictors and also investigating studies of factors such as inflammatory markers or neuroimaging abnormalities that might reflect neurobiological factors relevant to depression in later life.
Method
To identify studies reporting predictive factors of response or remission to antidepressant treatment in unipolar geriatric depression, 2 authors (CM and DB) searched PubMed, PsycInfo, and the Cochrane Library database following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline recommendations. 15 Publication year limits were not applied to the research. The identification of articles was based on the following key words: “predictors,” “geriatric depression,” “late-life depression,” “elderly depression,” “depression,” “aged,” and “antidepressant” using Boolean operators. Reviewing the references of each article identified additional studies.
The inclusion criteria for this study were (1) publication in English; (2) inclusion of unipolar depressed patients aged 60 years and older treated with antidepressant therapy; (3) open-label study, controlled or uncontrolled clinical trial, comparative study, or randomized controlled trial (RCT); and (4) assessment of potential predictors of response (ie, decrease in a depression score of 50%) or remission (ie, depression score on Hamilton Depression Rating Scale [HDRS] or HAM-D <7 or Montgomery-Asberg Depression Rating Scale [MADRS] <10) to antidepressants. Working independently and together, the 2 reviewers examined all titles and abstracts, obtained full texts of potentially relevant papers, and read the papers to determine whether they met the inclusion criteria. Discrepancies between reviewers were resolved through discussion until consensus was reached. We updated our review in August 2018 with updated data. Of the 201 full-text articles that were reviewed, we excluded a total of 149 articles that did not meet eligibility criteria. Thus, we obtained data from 58 articles that met our eligibility criteria (Figure 1).
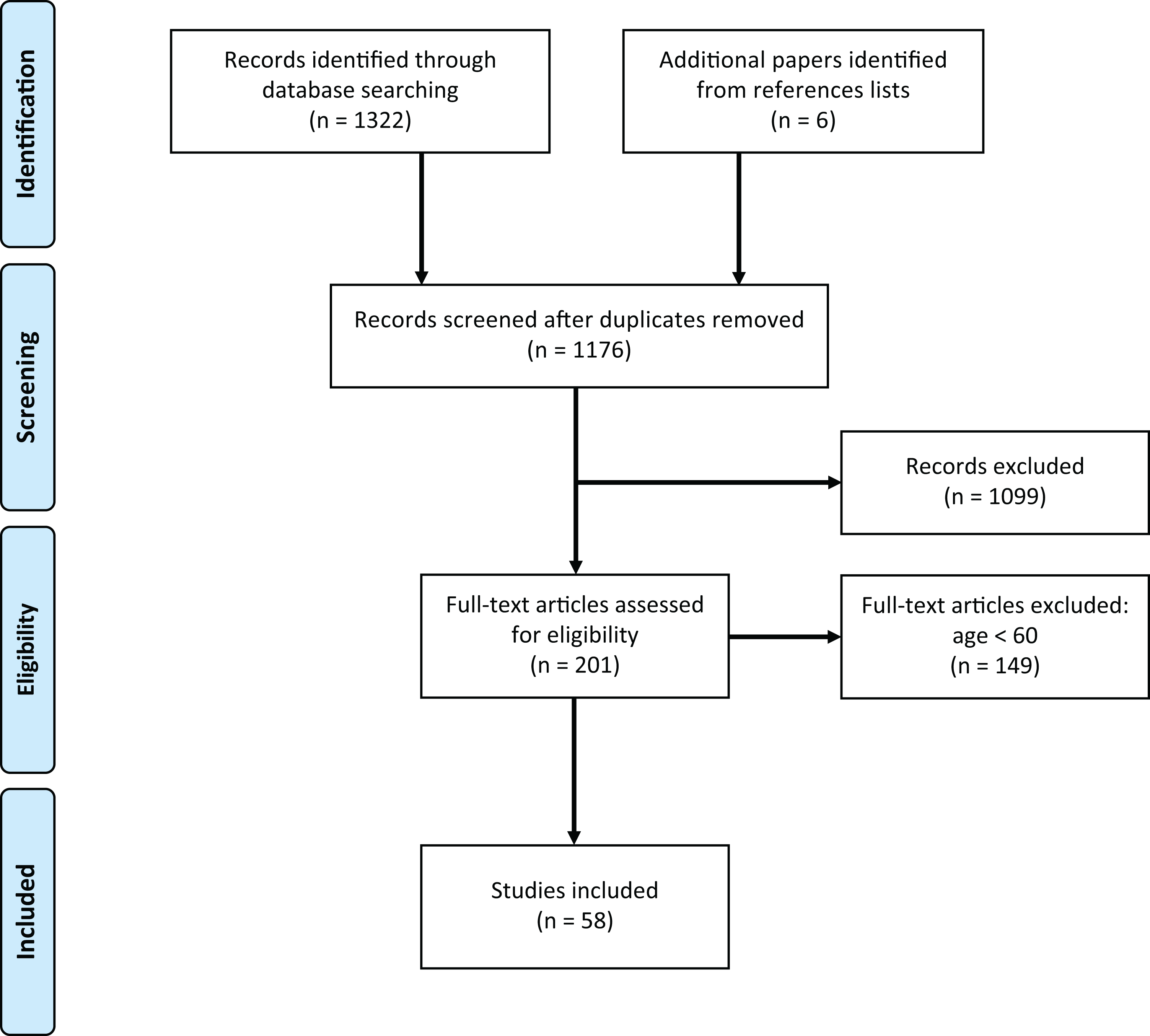
Flow diagram.
The reviewed studies are listed in Tables 1 to 4 according to sample, design, treatment, and outcome assessed. Our main findings are summarized in Table 5.
Sociodemographic and Clinical Predictors of Response or Remission to Antidepressants.
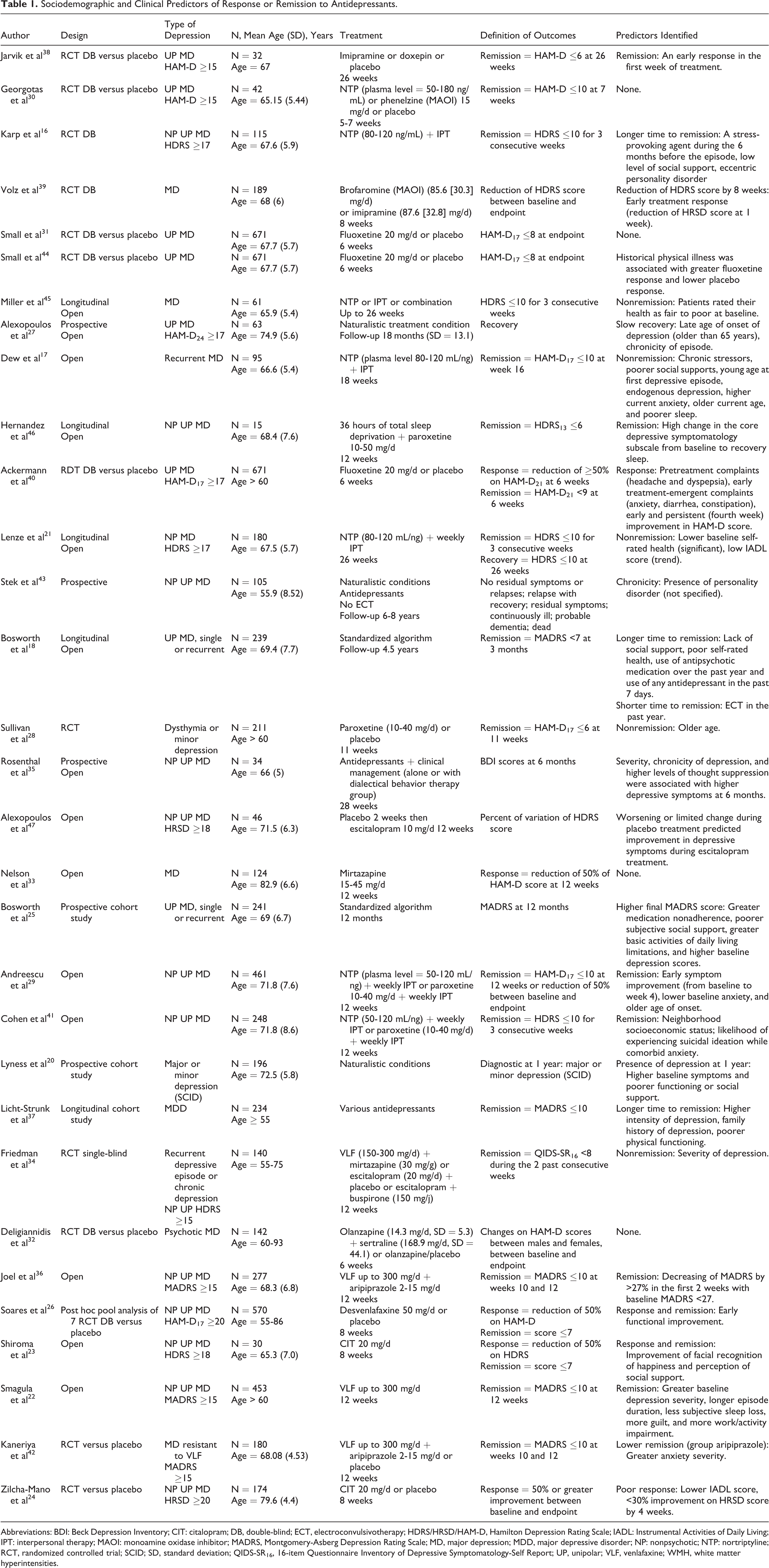
Abbreviations: BDI: Beck Depression Inventory; CIT: citalopram; DB, double-blind; ECT, electroconvulsivotherapy; HDRS/HRSD/HAM-D, Hamilton Depression Rating Scale; IADL: Instrumental Activities of Daily Living; IPT: interpersonal therapy; MAOI: monoamine oxidase inhibitor; MADRS, Montgomery-Asberg Depression Rating Scale; MD, major depression; MDD, major depressive disorder; NP: nonpsychotic; NTP: nortriptyline; RCT, randomized controlled trial; SCID; SD, standard deviation; QIDS-SR16, 16-item Questionnaire Inventory of Depressive Symptomatology-Self Report; UP, unipolar; VLF, venlafaxine; WMH, white matter hyperintensities.
Cognitive Predictors of Response or Remission to Antidepressants.
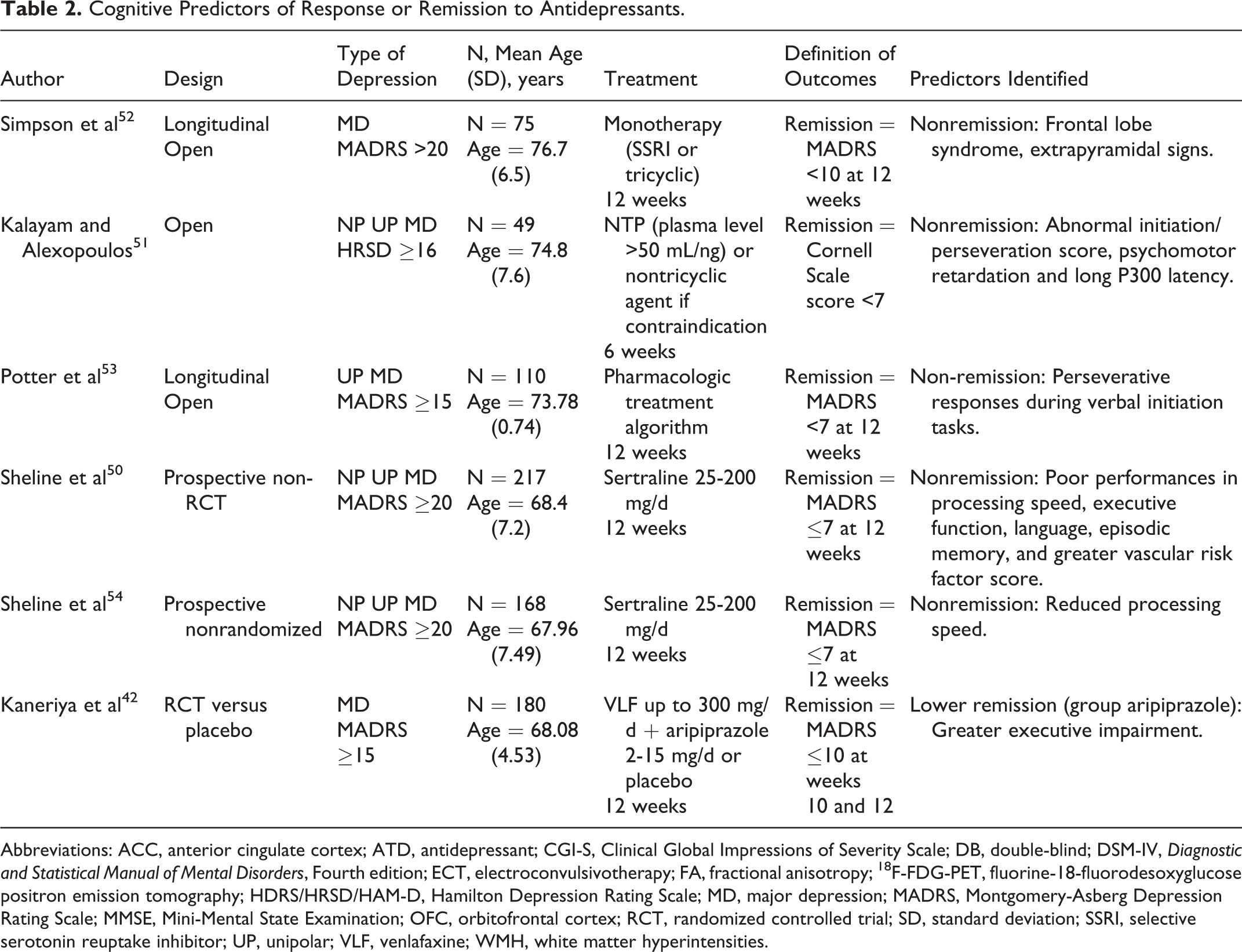
Abbreviations: ACC, anterior cingulate cortex; ATD, antidepressant; CGI-S, Clinical Global Impressions of Severity Scale; DB, double-blind; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth edition; ECT, electroconvulsivotherapy; FA, fractional anisotropy; 18F-FDG-PET, fluorine-18-fluorodesoxyglucose positron emission tomography; HDRS/HRSD/HAM-D, Hamilton Depression Rating Scale; MD, major depression; MADRS, Montgomery-Asberg Depression Rating Scale; MMSE, Mini-Mental State Examination; OFC, orbitofrontal cortex; RCT, randomized controlled trial; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor; UP, unipolar; VLF, venlafaxine; WMH, white matter hyperintensities.
Morphological and Functional Neuroimaging Predictors of Response or Remission to Antidepressants.
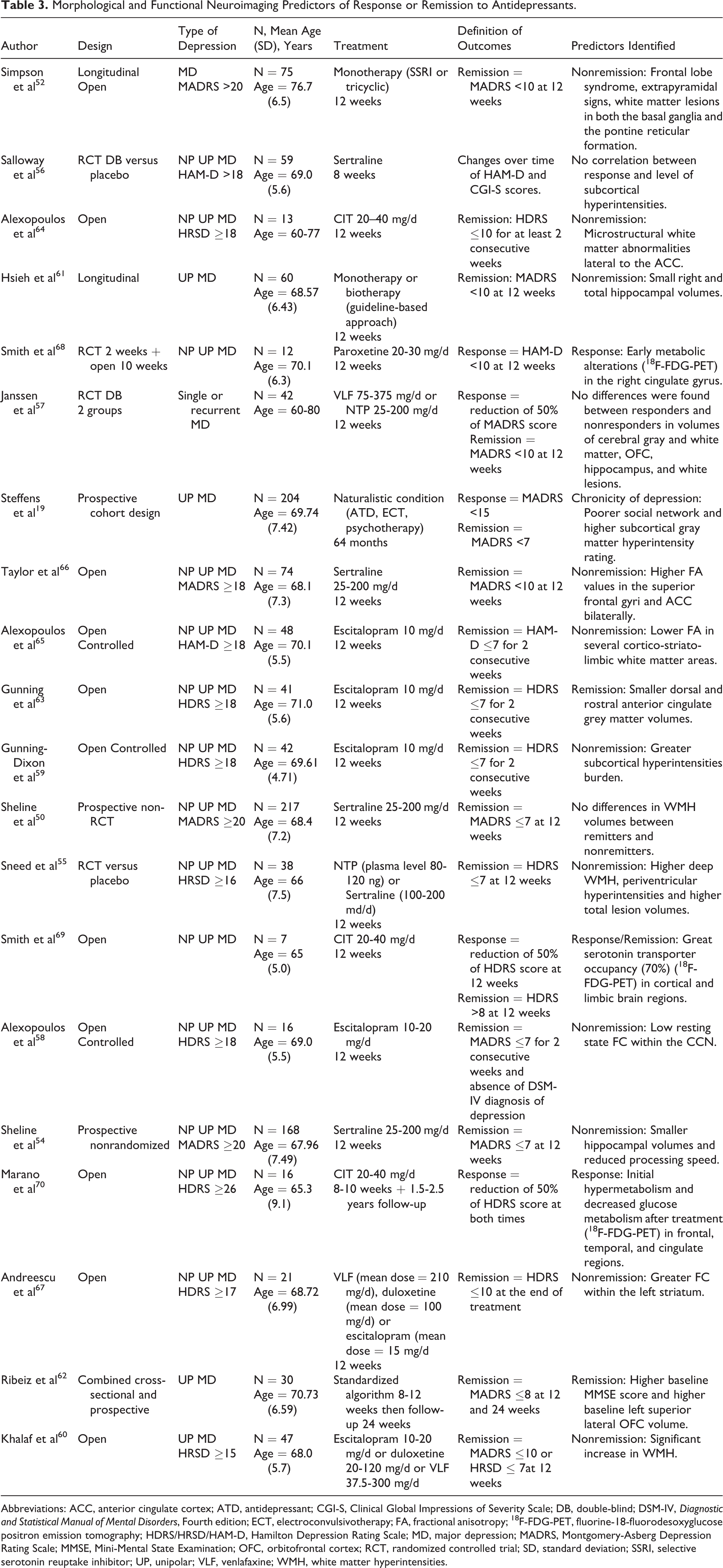
Abbreviations: ACC, anterior cingulate cortex; ATD, antidepressant; CGI-S, Clinical Global Impressions of Severity Scale; DB, double-blind; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth edition; ECT, electroconvulsivotherapy; FA, fractional anisotropy; 18F-FDG-PET, fluorine-18-fluorodesoxyglucose positron emission tomography; HDRS/HRSD/HAM-D, Hamilton Depression Rating Scale; MD, major depression; MADRS, Montgomery-Asberg Depression Rating Scale; MMSE, Mini-Mental State Examination; OFC, orbitofrontal cortex; RCT, randomized controlled trial; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor; UP, unipolar; VLF, venlafaxine; WMH, white matter hyperintensities.
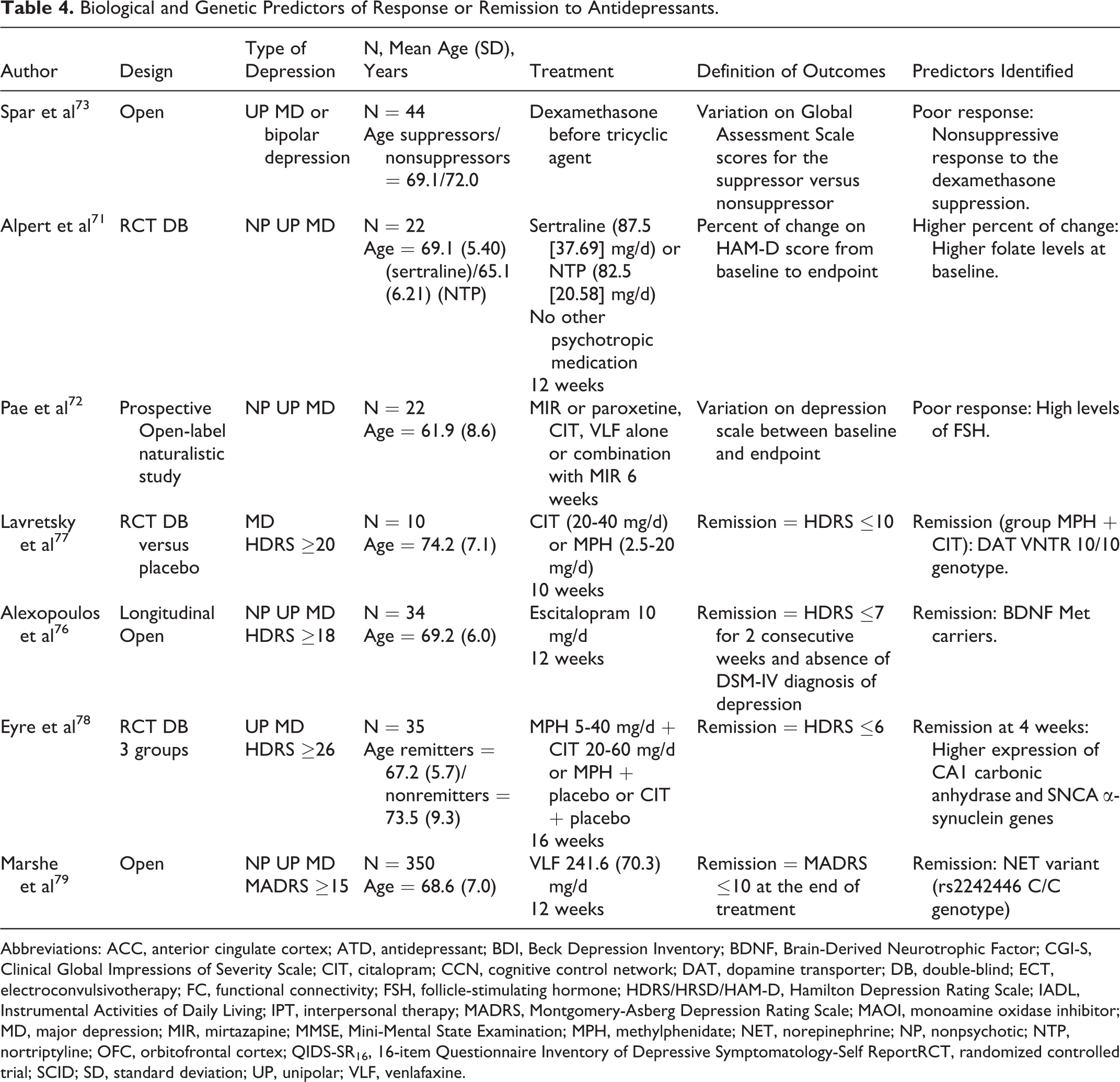
Biological and Genetic Predictors of Response or Remission to Antidepressants.
Abbreviations: ACC, anterior cingulate cortex; ATD, antidepressant; BDI, Beck Depression Inventory; BDNF, Brain-Derived Neurotrophic Factor; CGI-S, Clinical Global Impressions of Severity Scale; CIT, citalopram; CCN, cognitive control network; DAT, dopamine transporter; DB, double-blind; ECT, electroconvulsivotherapy; FC, functional connectivity; FSH, follicle-stimulating hormone; HDRS/HRSD/HAM-D, Hamilton Depression Rating Scale; IADL, Instrumental Activities of Daily Living; IPT, interpersonal therapy; MADRS, Montgomery-Asberg Depression Rating Scale; MAOI, monoamine oxidase inhibitor; MD, major depression; MIR, mirtazapine; MMSE, Mini-Mental State Examination; MPH, methylphenidate; NET, norepinephrine; NP, nonpsychotic; NTP, nortriptyline; OFC, orbitofrontal cortex; QIDS-SR16, 16-item Questionnaire Inventory of Depressive Symptomatology-Self ReportRCT, randomized controlled trial; SCID; SD, standard deviation; UP, unipolar; VLF, venlafaxine.
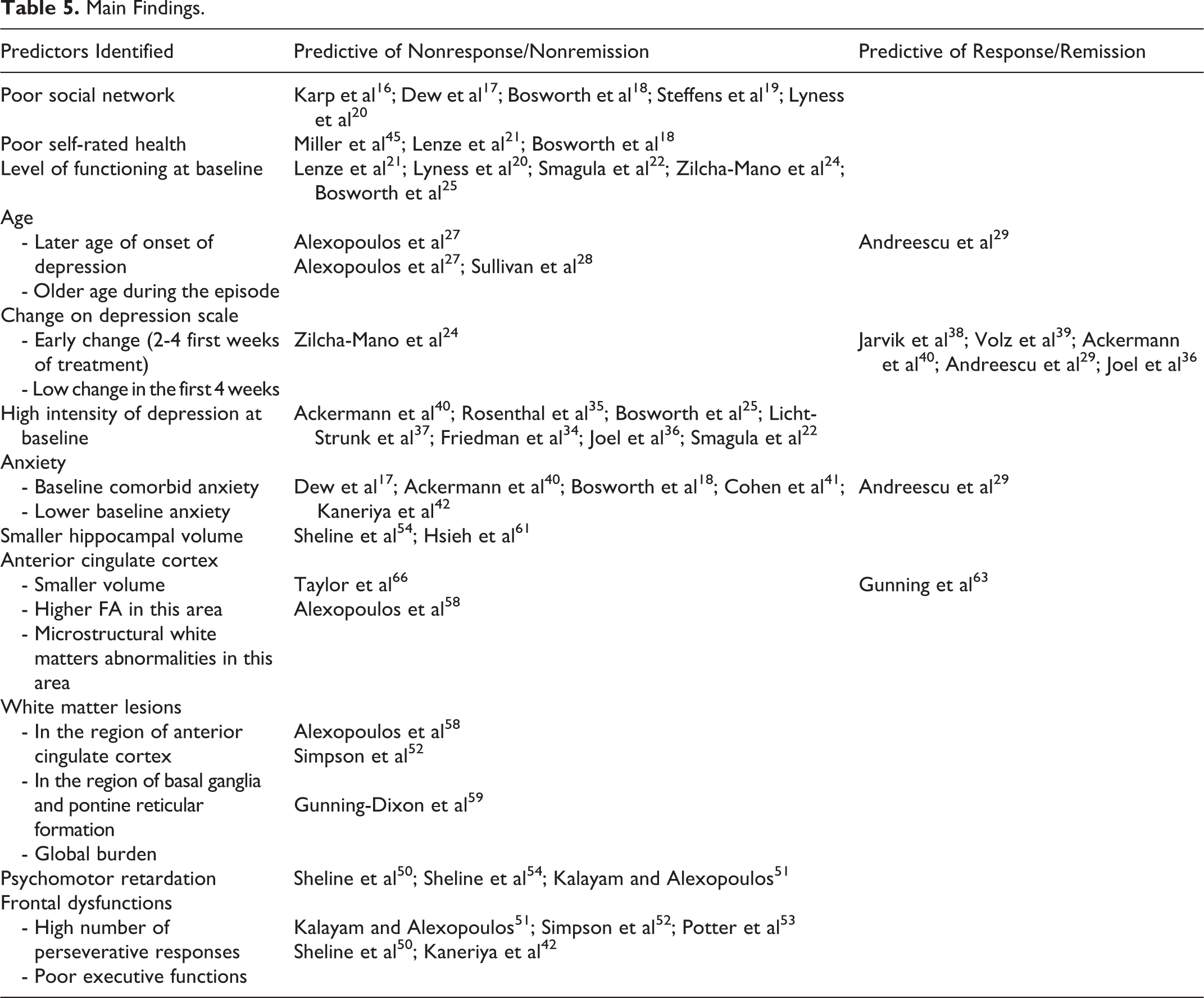
Main Findings.
Results
Sociodemographic, Clinical, and Cognitive Predictors of Response or Remission to Antidepressants
Sociodemographic predictors
Sixteen studies investigated the role of sociodemographic parameters on antidepressant response in unipolar geriatric depression. Having a poor social network was found to be a predictor of nonremission or slow recovery in 5 studies. 16 –20 Karp et al showed that the perception of diminished social support prolonged the time to remission. 16 Dew et al and Bosworth et al confirmed these findings in longitudinal open trials. 17,18 Bosworth and colleagues followed 239 old patients treated according to a standardized algorithm for 4.5 years. They found that poor subjective social and instrumental support measured by the 35-item Duke Social Support Index were significant predictors of longer time to remission. 18 In a naturalistic study, Lyness et al found that patients with poor functioning or social support were more likely to have depressive symptoms 1 year after diagnosis. 20 Similar results have been reported in 2 longitudinal studies with patients receiving nortriptyline and interpersonal therapy (IPT) for 26 weeks or venlafaxine for 12 weeks. 21,22 Dew et al followed 95 patients aged 60 years or older treated openly with nortriptyline and IPT for 18 weeks. The authors clustered the patients into 4 groups according to the pattern of response (nonresponse, partial or mixed response, delayed sustained response, or rapid sustained response). Variables related to psychosocial status (social support, perceived chronic stress, and occurrence of major life stressor prior to episode onset) predicted a greater likelihood of a partial or mixed response than any other response profile. 17 In an open-label trial, Shiroma et al assessed emotion recognition processing as a predictor of response to 8 weeks of citalopram in 30 patients with MDD. 23 A facial emotion recognition task was administrated prior to the onset of citalopram treatment and 7 days later. The authors showed that antidepressants increased recognition of facial expression of happiness prior to the improvement in mood symptoms. Moreover, recognition of positive emotions and higher perceived social support at baseline were predictors of subsequent response and remission to citalopram (Tables 1 and 2).
Five studies have found that a pretreatment low level of independent living skill, as assessed by the Instrumental and Activities of Daily Living scores were predictive of poor antidepressant response. 20 –22,24,25 Soares et al assessed the predictive value of early functional improvement for treatment success after 8 weeks on desvenlafaxine. They pooled data from 7 double-blind RCTs; functional improvement was assessed using the Sheehan Disability Scale (SDS). They found that early improvement (week 2) in SDS was highly predictive of all levels of treatment success at 8 weeks in patients aged 55 years or older. 26
Among demographic parameters, age could be a predictive factor for resistance to antidepressants. Alexopoulos et al followed up 63 older adult and 23 young patients with major depressive episodes treated under naturalistic conditions for an average of 18.2 months. They found similar recovery rates in both groups but reported that the older patients had a significantly longer time to recovery than younger individuals. Moreover, a later age of onset of depression was the strongest predictor of slow recovery. 27 Sullivan et al compared 2 groups (≤59 years and >60 years) of patients with dysthymia or minor depression treated with paroxetine in a 11-week RCT. They showed that patients younger than 59 years were more likely to respond to paroxetine than the older patients. 28 Similarly, Andreescu et al correlated older age of onset with a 54% chance of responding to a 12-week treatment with paroxetine or nortriptyline associated with IPT, whereas a younger age of onset correlated with a 67% chance of response. 29 No effect of gender, level of education, or marital status was observed in these studies.
Three double-blind RCTs and 1 open study assessed several demographic and clinical variables as predictors of response but failed to reach a level of significance. 30 –33 Georgotas et al 30 tested 21 variables as potential predictors of remission to antidepressants: 12 clinical variables (anhedonia, mood autonomy, anxiety, agitation, retardation, low energy, hypochondriasis, diurnal variation in the morning and in the afternoon, initial, middle and late insomnia, weight gain during episode), 4 demographic variables (age, sex, mental status, family history of depression), and 4 variables characterizing the depressive illness (presence of a precipitant, number of prior episodes of depression, duration of current episode, age of onset of first episode). In all, 25 older adult patients with MDD were taking nortriptyline, 22 patients were taking phenelzine (monoamine oxidase inhibitor), and 28 patients were taking a placebo. The outcome measure was the week 7 Hamilton score, and none of these variables were found to be significantly correlated with remission. Small et al 31 conducted a 6-week, double-blind RCT with 671 older adults taking fluoxetine or placebo. Nine categories of potential clinical response predictors were defined: agitation/anxiety, retardation, somatic complaints, medical illness, mood complaints, guilt expression, psychosocial stress, cognition, and miscellaneous characteristics. According to the authors, the results did not reach significance because of methodological considerations and because geriatric depression is a heterogeneous condition. In a double-blind RCT, Deligiannidis et al assessed the predictive value of age and gender on depression outcomes (change in HAM-D score between baseline and 6 weeks with olanzapine plus sertraline or olanzapine plus placebo). 32 They included 142 patients with MDD aged 60 to 83 years. The authors found no significant interactions between treatment and age, or gender,and the treatment effect on depression score was consistent across age-groups and for both genders. In a 12-week, open-label study, 124 nursing home residents with MDD were taking mirtazapine. 33 The association of response with different predictors (age, medical burden, cognitive impairment, sex, history of prior depression, and depression severity) was examined. These hypothesized predictors were not associated with response or with discontinuation of antidepressant treatment.
Clinical predictors
Several clinical predictive factors have been related to a poor response to antidepressant treatment, including depression severity at baseline, family history of depression, lack of early change in depression severity scales, or comorbid anxiety (Table 2).
Depression severity at baseline appears to be a strong clinical predictor of nonremission. In a published RCT, 140 older adult patients (aged from 55 to 75) received venlafaxine + mirtazapine or escitalopram + placebo or escitalopram + buspirone for 12 weeks. The authors identified greater baseline severity, assessed using the 16-item Questionnaire Inventory of Depressive Symptomatology-Self Report, as a predictor of nonresponse to antidepressant therapy. 34 Two naturalistic trials and 2 longitudinal studies also replicated these findings in patients treated with venlafaxine alone or combined with aripiprazole. 22,25,35,36 Licht-Strunk et al conducted a 3-follow-up study involving 234 patients. The outcome was the time to recovery at 1, 2, or 3 years, and the symptom severity was rated using the MADRS score every 6 months. These authors found that patients with a longer time to remission were those with a higher severity of depression at baseline and a family history of depression. 37
Early changes to scores in the depression scale have also emerged as potential clinical predictors. Three RCTs found that a reduction in depressive symptoms (ie, a reduction of 4 points on HDRS) at 1 week in patients treated with tricyclic agents 38 or monoamine oxidase inhibitors 39 or in the first 4 weeks of fluoxetine treatment were predictive of response or remission at 6 weeks. 40 Similarly, Joel et al found that a decrease in MADRS scores >27% in the first 2 weeks of treatment with venlafaxine plus aripiprazole predicted remission. 36 Andreescu et al proposed 2 models to help clinicians with decision-making: one minimizing false predictions of future response and the second minimizing false predictions of future nonresponse. In the first model, depressive symptom improvement in the first 4 weeks of treatment and lower baseline anxiety predicted response after 12 weeks of nortriptyline or paroxetine plus IPT. In the second model, early symptom changes were also a strong predictor of response at the end point. 29 One RCT study found that patients demonstrating a lower change (<30%) of symptom intensity during the first weeks of antidepressant treatment were less likely to achieve remission at 8 weeks. 24
Several authors pointed out that baseline comorbid anxiety predicted poor response or nonremission in patients treated in naturalistic conditions 18 with a tricyclic agent 17,41 or SSRI alone 40,41 or SSRI combined with an atypical antipsychotic. 42 Andreescu et al found that patients with a lower level of anxiety at baseline were more likely to respond to 12 weeks of nortriptyline or paroxetine combined with IPT. 29
Two studies correlated the presence of a personality disorder with chronicity of depression. 16,43 Karp et al found that depressed older adult patients with a paranoid, schizoid, or schizotypal personality were more likely to be antidepressant nonresponders. 16 Stek et al reported that a personality disorder was a predictor of chronicity but did not specifically talk about the type of personality concerned. 43
Somatic comorbidities are often present in older age, and a few authors have investigated the impact of physical illness on depression treatment outcome. Small et al and Miller et al found that the number of chronic illnesses was not correlated with antidepressant response. 44,45 Miller et al compared the perception of health status in responders and nonresponders to nortriptyline or IPT or the combination of both treatments. They used the Perception of Illness Scale Score and showed that pretreatment self-rated health was significantly poorer among the nonresponders than among the responders. 45 Lenze et al, Bosworth et al, and Sullivan et al also showed that lower baseline self-rated health was a significant predictor of nonremission. 18,21,28
Hernandez et al investigated a sleep deprivation paradigm in which patients underwent a combined treatment with an initial 36-hour Total Sleep Deprivation (TSD) and a 12-week trial with paroxetine. The aim of this study was to evaluate whether the change in HDRS after 36 hours of TSD and after 1 night of recovery sleep predicted remission after 12 subsequent weeks of antidepressant treatment. The authors observed that the change in the core depressive symptomatology subscale from baseline to recovery sleep was robustly correlated with the 12-week HDRS score. These findings were consistent with a previous report in younger adults. 46
Only 1 study examined whether change in severity of depression in a 2-week placebo lead-in phase could predict the change in HDRS score during a 12-week phase of antidepressant treatment with escitalopram. The main finding of this study was that worsening or limited improvement in depressive symptoms during placebo treatment predicted an improvement in depressive symptoms during antidepressant treatment. 47
Cognitive predictors
Cognitive deficits are frequent in geriatric depression, and many anatomical and functional abnormalities observed in brain magnetic resonance imaging (MRI) have been correlated with alterations in cognition. 48,49 Sheline et al evaluated the relationship between neuropsychological performances, white matter hyperintensities (WMH), and clinical response in late-life depression. They found that cognitive performances and WMH burden were correlated and were both predictors of MADRS scores after 12 weeks of sertraline. Furthermore, those predictive variables were also correlated with cardiovascular risk (Table 2). 50
Several studies showed that older adult depressed patients were more likely to be nonremitters when they had lower executive functioning and frontal dysfunctions at baseline. Kalayam and Alexopoulos used initiation/perseveration (I/P) scores (word generation, manual sequencing, and graphomotor copying task) and psychomotor retardation as clinical measures of prefrontal dysfunction. They examined the correlations between I/P score, psychomotor retardation, P300 latency, and the depression score on the Cornell scale between baseline and 6 weeks of antidepressant treatment (paroxetine, sertraline, fluoxetine, or nortriptyline). The P300 evoked response was used as an electrophysiological index of prefrontal dysfunction, and long latency was associated with executive impairment. The authors found that abnormal I/P scores, psychomotor retardation, and long P300 latency were associated with a poor or delayed response to antidepressants. 51 Simpson et al also showed that patients with frontal and pyramidal neurological signs were less likely to respond to antidepressant monotherapy. 52 Potter et al also reported that an index of verbal perseveration among older patients with depression was correlated with a lower remission rate after 3 months of treatment using a standardized pharmacological algorithm. 53 In 2 consecutive studies, Sheline at al confirmed that lower processing speed was a predictor of low rates of remission. 50,54 They further constructed a model of prediction, where lower performances on processing speed and smaller hippocampal volume were combined and were strongly associated with lower remission. 54 More recently, Kaneriya et al included 180 patients with depression up to 68 years in an RCT comparing the 12-week treatment response to venlafaxine + aripiprazole and venlafaxine + placebo. Set-shifting ability, which is related to mental flexibility and executive functions, was assessed with the Trail Making Test part B (TMT B). Patients with poorer performances on TMT B at baseline were more likely to achieve remission and responded more favorably to aripiprazole augmentation. 42 These results underlined the important role of executive impairment in some subgroups of older patients with depression and could help clinicians to personalize their therapeutic strategy.
Neurobiological Predictors of Response or Remission to Antidepressants
Neuroimaging predictors
Morphological studies
A number of studies have examined how structural or functional MRI markers can predict antidepressant response in older adults with unipolar depression. These studies examined gray or white matter volumes and WMH burden. White matter integrity was assessed using Diffusion Tensor Imaging to calculate fractional anisotropy (FA), which is a marker of myelin integrity (Table 3).
Nine studies assessed the association between WMH burden and response to antidepressant treatment. These studies generally found that higher WHM burden predicted a poor response or nonremission. 19,50,52,55 –60 The largest study, involving 190 patients, did not find any significant differences in WHM volume between remitters and nonremitters. This lack of significance could be explained by the interaction of many other parameters relevant to treatment response; however, these study’s results highlighted the link between vascular risk factors and response to antidepressant treatment, as a higher vascular risk was predictive of lower remission after 12 weeks of sertraline. 50 In another RCT, Sneed et al found that older adult patients with a higher level of deep WMH, periventricular hyperintensities, and higher total lesion volumes were 4 to 7 times more likely to not remit following nortriptyline or sertraline treatment compared to those with fewer white matter lesions. 55 Khalaf et al found that nonremitters to escitalopram, duloxetine, or venlafaxine demonstrated a significant increase in WMH between baseline and the end of treatment. 60 In contrast, Salloway et al, Janssen et al, Sheline et al, and Steffens et al found no correlation between response and level of subcortical WMH. 19,50,56,57
However, Steffens et al conducted a prospective naturalistic cohort study and also evaluated the impact of level of subcortical gray matter hyperintensities on response or remission to antidepressant treatment. The rating of subcortical gray matter hyperintensities was strongly predictive of chronicity of depression. 19
Results concerning other neuroimaging markers have been mixed. Preliminary data associate a smaller hippocampal volume at baseline and a decreased volume of the dorsal and rostral anterior cingulate cortex with nonremission, while higher baseline left superior lateral orbitofrontal cortex volume predicted remission. 54,61 –63
Three studies assessed the predictive power of FA and showed mixed findings: 2 studies found that microstructural brain damage in cortico-striato-limbic areas was associated with nonremission in patients treated with SSRI for 12 weeks. 64,65 The third study reported a different finding, a correlation of higher FA in the white matter of the anterior cingulate and frontal cortices with nonremission. 66 The apparent inconsistencies between these results may reflect methodological differences.
Functional neuroimaging studies
Data from functional neuroimaging studies are very limited. We found 2 studies that evaluated brain connectivity 58,67 and 3 studies that assessed the use of fluorine-18-fluorodesoxyglucose positron emission tomography (18F-FDG-PET) to predict antidepressant treatment response in geriatric depression. 68 –70
Alexopoulos and colleagues focused on functional connectivity (FC) within the cognitive control network (CCN) that involves the dorsal anterior cingulate cortex (ACC) and dorsolateral prefrontal cortex (DLPFC) parts of the parietal lobe and the default mode network (DMN), including the posterior cingulate/precuneus, ventromedial prefrontal cortex, ventral ACC, inferior parietal lobes, and parts of the temporal lobe. The CCN supports several functions including attention, working memory, or emotional regulation. Anatomical and functional abnormalities in these networks have been shown in older depressed patients and some links have been made with response to antidepressants. The principal finding was that low resting FC within the CCN and high FC within the DMN characterized late-life depression, which is consistent with the available neuroimaging studies. Moreover, resting FC at the CCN during the depressive episode predicted poor remission and the persistence of executive dysfunction. The FC in the DMN was not associated with remission. 64 In an open-label trial with 21 older adult patients taking venlafaxine, duloxetine, or escitalopram for 12 weeks, the authors focused on resting-state FC within the DMN and highlighted that treatment-resistant patients had increased FC in the left striatum. Of interest, this result remained significant after adjustment for intensity of white matter lesions. 67
In an open-label trial, Smith et al included 12 older adult patients with depression who underwent 18F-FDG-PET before antidepressant treatment, after 8 to 10 weeks and 1.5 to 2.5 years after completion of 12 weeks of paroxetine. 68 They found a positive correlation between the change on depression score and cerebral glucose metabolism in the right cingulus gyrus after 12 weeks and at follow-up. Later, Smith et al conducted an open-label trial with 7 patients treated with citalopram. 69 They studied correlations between changes in cerebral glucose metabolism, serotonin transporter occupancy by citalopram, and variations in depression score. They found that changes in cerebral metabolism and serotonin transporter occupancy in cortical regions and corticolimbic pathways were associated with improvement in depressive symptoms. The third study using 18F-FDG-PET was conducted by Marano et al. 70 Between baseline and follow-up (2 years after 8-10 weeks of citalopram), remitted patients showed decreased metabolism in regions including the superior frontal, middle and inferior temporal, posterior cingulate, insula, putamen, and thalamus.
Biological predictors
Three reported studies investigated the predictive value of different biological variables for response to antidepressant treatment in older adults (Table 4). 71 –73
The first one assessed the interaction between SSRI or tricarboxylic antidepressant (TCA) and folate level. Folate is an essential nutriment that participates in a number of metabolic processes. In geriatric populations, depression has been found to be associated with lower folate levels. Some studies reported lower folate levels during severe depression, 74 while others found that supplementation with folate during depression could help to reduce symptoms. 75 These findings could be explained because folate is involved in serotonin metabolism. In their double-blind RCT study, Alpert et al randomized 22 patients into 2 groups (12-week treatment with sertraline or nortriptyline). They replicated previous data suggesting that a lower folate level at baseline is associated with reduced responsiveness to antidepressant treatment, but these correlations were only found in the sertraline group. In contrast to sertraline, nortriptyline effects are mainly mediated by noradrenergic and not serotoninergic mechanisms, which might explain these results. 71
The prevalence of depression is greatly increased in women, and hormonal status could be involved in depressive recurrence or symptom remission. To assess the effect of pre- or postmenopausal status on the effectiveness of a 6-week antidepressant treatment, Pae et al conducted a prospective open-label naturalistic study with 39 Korean women. Different classes of antidepressants were prescribed (SSRI, selective norepinephrine reuptake inhibitor [SNRI], and TCA); other psychotropic medications were not allowed. The authors found that postmenopausal women were less likely to remit compared to premenopausal women. Furthermore, a high basal level of follicle-stimulating hormone (FSH) significantly predicted the response to antidepressants in postmenopausal women. These findings suggested that FSH could interact with antidepressants via the modulation of neurotransmitters such as acetylcholine, dopamine, or serotonin, which has been shown to exert an important control on the release of FSH in the pituitary gland. 72
The third study of biological predictors used the dexamethasone suppression test (DST) to predict depression course. Several studies in older or young adults have suggested that an abnormal DST may identify a subgroup of patients with more “endogenous” depression. One milligram of dexamethasone was orally administrated at 11:30
Genetic Predictors
Only 4 studies, to our knowledge, have examined the relationship between genetic parameters and antidepressant response. In a longitudinal open study, Alexopoulos and colleagues investigated the influence of Brain Derived Neurotrophic Factor (BDNF) polymorphism on remission (ie, score on Hamilton Rating Scale <7 for 2 consecutive weeks). They recruited 34 older adult patients treated with escitalopram for 12 weeks and found that BDNF Val66Met or Met66Met carriers were more likely to achieve remission than Val66Val carriers (Table 4). 76
Two studies investigated the predictive factors of response to a combination of citalopram with methylphenidate (MPH), a dopamine reuptake inhibitor. 77,78 In a double-blind RCT, Lavretsky et al included 10 patients with depression older than 70 years who received 10 weeks of citalopram or MPH. They assessed the role of a specific dopamine transporter (DAT) polymorphism on remission. They found that DAT VNTR 10/10 carriers were more likely to go into remission with the combination of citalopram + MPH than with citalopram alone. 77 Eyre and colleagues used a genome-wide expression analysis to determine genomic predictors of remission to antidepressant treatment in 35 geriatric patients treated with MPH + citalopram, MPH + placebo, or citalopram + placebo for 16 weeks. They found 2 genes showing higher expression in early remitters at baseline compared with nonremitters. The first gene was the CA1 carbonic anhydrase gene, on chromosome 8, which could be involved in the modulation of excitatory neurotransmission. The second gene was the SNCA α-synuclein gene, which is associated with DAT functioning. 78
More recently, Marshe et al studied 350 patients with depression aged 60 years and older with MDD in order to investigate the link between functional variants of the norepinephrine transporter (SLC6A2, NET) and serotonin transporter (SLC6A4, SERT) genes and remission in patients treated with venlafaxine. 79 They found that NAT variant rs2242446 was significantly associated with remission. Patients with the rs2242446 C/C genotype were more likely to achieve remission, had a shorter time to remission, and had a greater percentage change in MADRS score from baseline to end of treatment than those with the C/T or T/T genotype. These findings underline the potential clinical utility of pharmacogenetic testing in older adults.
Discussion
This article aimed to review current data about predictive factors of response or remission to antidepressants in geriatric depression. Several predictors have been suggested among a large range of clinical, sociodemographic, cognitive, neurobiological, or genetic parameters.
A poor social network, a poor level of functioning, and poor self-rated health have been proposed as possible predictors of poor response 23,24 or poor remission. 16 –23 A number of studies have demonstrated that social support was a determinant of physical and mental health among older adults. A poor social network is associated with low levels of quality of life and with disability. 80,81 The perception of social network depends on the social and cultural context of living and could be modulated by emotional status. 82 For instance, loneliness reflects a subjective state in which the affection of friends or family members is lacking. Loneliness is a major risk factor for depression, impaired physical health, or functional limitations. The link between loneliness and health could involve neurobiological mechanisms including age-related changes in neuroendocrine, inflammatory stress response, or hypothalamic pituitary adrenocortical activity. 83 Cognitive processes have also been implicated because impaired executive functioning heightens sensitivity to negative social stimuli and alters personal trust. 84 Psychotherapy could be effective to reduce loneliness and social isolation in older adults. These interventions aimed to improve social skills, enhance social support, and address maladaptive social cognition. 85
Several clinical characteristics of depression could influence response or remission rates with antidepressants in older adults. The strongest results concerned a higher intensity of depression at baseline 22,25,34 –37,40 and a comorbid anxiety 17,18,40 –42 that were predictive of nonresponse or nonremission, and an early change in symptom severity during the first 4 weeks 29,36,38 –40 that was associated with higher rates of response or remission. Similar results were also found in a systematic review of risk factors for treatment resistance in younger adults with unipolar depression 86 and in a prospective European multicenter study combining clinical and sociodemographic predictors. 87 Currently, it remains difficult to generalize based on these results because of the many discrepancies between studies. However, the clinician should be aware that the presence of these risk factors might predict the patient’s course of treatment and allow earlier identification of patients less likely to respond to antidepressant treatment.
Among clinical parameters, apathy was not studied although it is often present during a depressive episode and could be associated with poor remission in geriatric depression. Some authors showed that apathy was correlated with lower cognitive control in older adult patients with depression and linked this symptom with poor remission. One study pointed out that apathy impacts the structural brain integrity and cognition in geriatric depression and could modulate the response to antidepressants.
88
Apathy screening may be beneficial for depressed older adult patients with cognitive dysfunction because conventional antidepressants may not be suited to treated apathy. Some studies have proposed memantine, a noncompetitive N-methyl-
Results regarding the timing of depression onset (early vs late onset) are conflicting. Alexopoulos et al found later age of onset to be a predictive factor of low recovery, whereas Andreescu et al showed the opposite result. 27,29 These discrepancies could be due to methodological differences (number of patients, design, type of medication). However, late-onset depression (LOD) is reported to have a particular pathophysiology and might show a different response profile. We diagnose LOD when the first depressive episode occurs after the age of 60, and multiple studies have shown an association between LOD, cerebrovascular disease, and low rates of antidepressant response in older adult populations. 92
Regarding biological parameters, we expected to find some data about inflammatory biomarkers of remission/nonremission, but no article has reported on these factors. However, recent studies suggest that antidepressants may exert effects on the immune system and during aging we can observe high levels of interleukin 6 (IL-6) so that levels are low in young people. This so-called “inflammaging” has been associated with functional changes in the aging central nervous system, including the development of depression. 93 In geriatric depression, it would be interesting to prescribe an antidepressant with greater anti-inflammatory effects to improve management of mood symptoms. A new antidepressant that combines SSRI activity and 5-HT 1A receptor partial agonist activity, vilazodone, showed similar effects than paroxetine on depressive symptoms in late-life depression. These effects may be attributed to downregulation of proinflammatory genes and arise predominantly from monocytes and dendritic cells. 94 A recent meta-analysis of 22 studies explored the effect of antidepressants on serum proinflammatory cytokines in 603 patients with depression. 95 They found that antidepressants with SSRI activity may reduce levels of IL-6 and tumor necrosis factor-α whether other types of antidepressants did not appear to reduce cytokine levels. This study suggests SSRI antidepressants exert the greatest inflammatory effects; however, these results are based on a small subsample of studies and must therefore be considered with caution. A limited number of studies explored the anti-inflammatory effect of SNRI antidepressants. 96 These antidepressants may have an anti-inflammatory effect, and this may depend on their dose range and on the status of patients (early responder or early nonresponder). Tricyclic agents appear to have anti-inflammatory effects, and IL-6 may assist in predicting responders versus nonresponders. However, the modulation of immune system by antidepressants is incompletely understood, and several factors may affect the anti-inflammatory response to antidepressants, such as the age range of the cohort or the higher burden of vascular-related pathology. 97 The presence of heart disease, obesity, or diabetes may also create a proinflammatory state and modulate the antidepressant response. In the field of geriatric depression and despite the heterogeneity of studies, SSRI antidepressants may be a suitable option to combined effectiveness on depressive symptoms, tolerability, and anti-inflammatory effects.
Morphological studies suggest an important predictive role of WMH in antidepressant response. Some researchers report that WMH in the ACC, 64 in the region of the basal ganglia and pontine reticular formation, 52 or a global burden of WMH predict of nonresponse or nonremission. 59 However, results are not yet regarded as definitive because other investigators have found no significant correlations between WMH burden and response to antidepressants. 50,56,57 The WMH are more prevalent in aged brains and could be a nonspecific predictor of antidepressant nonresponse in the geriatric population because it could be assumed that WMH are a consequence of microstructural lesions with a cumulative effect on life span. Thomas et al found that the causes of WMH were similar in depressed and healthy older adult patients and that WMH in the periventricular region were due to 1 of the 3 causes: ependymal loss, differing degrees of myelination in adjacent fiber tracts, and cerebral ischemia with associated demyelination. This variability in pathophysiology could explain the conflicting results regarding the association between cardiovascular risk factors and WMH burden. 98
It is assumed that WMH could impair connectivity between cortical and subcortical regions. The pathophysiology of depression implicates the functioning of different cerebral structures such as the prefrontal cortex, ACC, or basal ganglia, which are involved in emotion regulation and cognitive control. In depressed older adults, decreased metabolic activity at rest has been observed in dorsal ACC and in the DLPFC during episodes of depression. 99 Therefore, it could be of interest to explore the impact of frontosubcortical connectivity on response to antidepressants in the older adult population. Alexopoulos et al found specific characteristics when they studied cerebral connectivity in older depressed and healthy adults. In control patients, the activity in the DMN should be low during cognitive tasks, but they found an abnormally increased activity in this network in the same conditions during depressive episode. The DMN is important in self-referential activities, including evaluating salience of internal and external cues, remembering the past, and planning the future. In this study, this pattern of activation was correlated with pessimism but not with treatment response. 58 The other network studied was the CCN, which influences emotional response to stimuli or thought suppression; it is involved in decision making and conflict resolution. 100 The authors found that low FC within the CCN was associated with poor remission to sertraline, executive dysfunction, and apathy. This is the first study, to our knowledge, identifying an imbalance of resting FC in the DMN and CCN in LLD and a correlation between resting FC in the CCN and poor outcomes of depression. This pattern of activation could be a characteristic of brain functioning in LLD and could provide a novel target for therapeutic interventions. Andreescu et al confirmed the role of WMH in disrupting corticosubcortical circuits and showed that poor treatment response to SSRI or SNRI was associated with increased FC in the left striatum after 12 weeks of treatment. This result is interesting because the striatum is involved in motivation and voluntary movement mediation by the dopaminergic system. 67 This activation of the striatum in LLD could have therapeutic implications and can explain the lack of response to serotoninergic antidepressants in the geriatric population. This finding could lead to the identification of a subgroup of patients who are more likely to respond to dopaminergic agents, as suggested in genetic studies. 77,78
Frontostriatal circuits and the dopaminergic system support motivation, psychomotor speed, and executive function; the higher prevalence of executive dysfunction and impaired processing speed were assumed to be linked to frontostriatal abnormalities. 99 These neurocognitive factors seem to be particularly relevant in the course of depression in older adults. Indeed, many authors found that these 2 parameters were predictors of poor remission to antidepressants, and it has been suggested that patients presenting these symptoms were part of a subgroup that is less likely to respond to antidepressants and particularly to SSRI. Similar findings were exposed in cohorts of younger adults. 7,9 Taylor and colleagues showed that psychomotor slowing might identify a subgroup of depressed patients who have a dopaminergic deficit and were nonresponders to fluoxetine monotherapy. 7 Measures of verbal fluency such as the Controlled Oral Word Association-FAS is correlated with decreased dopaminergic activity within the striatum and was the strongest predictor of fluoxetine response. The particular interest in verbal fluency to predict response could be explained by the involvement of the left DLPFC and left ACC during this task; the activation of these brain structures may differ between responders and nonresponders to fluoxetine. In the geriatric population, some authors corroborated these results and found that a reduced processing speed was a predictor of nonremission after 12 weeks of sertraline. 50,54 Genetic factors implicating DAT could be combined with the verbal fluency test or neuropsychological test involving executive functions in order to predict remission or response to antidepressants. Although the number of genetic studies is limited, Eyre et al showed the increased expression of SNCA α-synuclein that is involved in DAT functioning, among remitters compared to nonremitters. 78 Moreover, Lavretsky et al found that a genetic polymorphism of DAT predicted the remission to citalopram alone or in association with MPH. 77 These preliminary data suggest the existence of many genotypes that are associated with specific endophenotypes in geriatric depression and that these genotypes could modulate the response to antidepressants.
Despite their interest to clinicians and researchers, some of these results showed a lack of consistency that makes them difficult to apply to clinical work. No variable seems to be specifically associated with remission or response to antidepressant, and complementary studies are needed to clarify this point. The discrepancies in findings could in part be explained by methodological considerations. The vast majority of studies used a longitudinal open design, and the treatment was not often controlled. Studies differed in antidepressants class and dose or duration of prescription. Plasma levels were not uniformly measured. Sometimes, the treatment was delivered according to a standardized algorithm without more precision, and the inclusion of adjunctive treatment such as psychotherapy or antipsychotics could affect results. The depression scales MADRS and HDRS are validated in the geriatric population and are appropriate tools for the assessment of variations in depression intensity over time. The heterogeneity of results could also be linked to the diversity of the clinical groups: Some authors included patients with a recurrent episode that could be a risk factor for nonresponse or nonremission, compared to those with a first episode of depression. The mean age was different between studies with groups of patients younger than others; therefore, the time to response or remission could be influenced by age. As a limitation of our own methodology, restricting our search to English-speaking articles would result in omission of potentially important studies.
The determination of several predictive factors of (non)response/(non)remission could help to better characterize a population of patients and better understand the pathophysiology of depression in older adults. Different domains such as neuroimaging, biology, cognition, clinical, panomics, environmental, and sociodemographic information are already pooled in large databanks in adult population but not yet in geriatric population, that is, a specific group of patients because of metabolic or pharmacogenetic changes due to aging. Finding a set of biomarkers of (non)response/(non)remission that can be applied to individuals and population might facilitate more individualized and more effective therapeutic strategies. “Precision psychiatry” holds the promise of more accurately predicting, and perhaps improving, prognosis. 101 There are currently more and more reported studies looking at pharmacogenetics in psychiatry research because this domain seems to be particularly relevant in diagnostic, prognostic, and symptoms management. Pharmacogenetic DSTs are also interesting for integration to “precision psychiatry,” and they have been evaluated in a psychiatric context in 3 studies. 102 Their potential utility in adult depression has been suggested, but no clinical trial evaluated a DST in geriatric depression. It would be important to conduct studies in geriatric population because age impacts both the pharmacodynamics and the pharmacokinetics of drugs, and recommendations provided for adult patients do not have the same clinical utility for older adults. If the utility and cost-effectiveness of DST can be established, these tools could be integrated to clinical practice guidelines to reduce the risk of initial treatment failure.
Conclusion
This systematic review of the literature found many potentially predictive factors of response or remission to antidepressants in the geriatric population. However, the lack of consistency between studies due to methodological discrepancies leads to difficulties in generalizing the results. Beyond methodological considerations, the differences observed could be explained by a variability of clinical subgroups in this population. The pathophysiology could be different between patients and lead to mixed results. Therefore, complementary studies are still needed to identify and characterize these subgroups so as to better understand the geriatric depression. Furthermore, this review highlights the importance of assessing processing speed and executive functioning to determine the best therapeutic strategy. Particularly, the verbal fluency test seemed to be very interesting to predict response or remission to antidepressant in older adults and the altered functioning of the dopaminergic system in some subgroups of depression could guide the clinician in the choice of antidepressant. Probably, a single neuropsychological measure would not be sufficient to provide a good predictive value, but it could be possible to combine many factors (clinical, cognitive, imaging, genetic, and so on) to determine the risk of nonremission to antidepressants.
Footnotes
Authors' Note
The main findings were presented at the French Congress of Psychiatry in December 2017 in Lyon.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.