
Abstract
Aim:
Associations between cerebrospinal fluid (CSF) biomarkers of Alzheimer’s disease (AD) with the severity of cognitive impairment are unclear. We examined the correlations between CSF biomarkers and cognitive performance in the AD continuum.
Methods:
We studied 143 elderly patients: cognitively unimpaired (n = 51), mild cognitive impairment (MCI) amnestic (n = 55) and nonamnestic (n = 20), and mild AD (n = 17) assessed with the Cambridge Cognitive Test (CAMCOG). We correlated total CAMCOG and its subdomains with CSF Aβ42, T-tau, p-tau levels, and Aβ42/p-tau.
Results:
In the total sample, T-tau and Aβ42/p-tau correlated with the total CAMCOG (P < .01); all biomarkers correlated with memory (P < .001); T-tau correlated with language (P < .01).
Conclusion:
Memory and T-tau levels may be the most suitable parameters to reflect cognitive/CSF biomarker correlations. At present, such correlations are of little use in routine clinical practice.
Introduction
Alzheimer disease (AD) accounts for 60% to 70% of dementia cases, and by 2018, AD already affected 50 million people worldwide. 1 The neuropathological signature of AD includes the presence of cerebral extracellular neuritic plaques and the accumulation of intracellular neurofibrillary tangles (NFT), which are composed of fibrillar forms of amyloid-beta peptide and hyperphosphorylated tau protein, respectively. These pathological processes are indirectly reflected by biochemical changes in cerebrospinal fluid (CSF) consisting of a reduction in the amyloid peptide (Aβ42 soluble monomer) and an increase in 181Thr-phosphorylated tau protein (p-tau). 2
Mild cognitive impairment (MCI) refers to a condition where the subject has complaints and objective signs of decline from a previous cognitive status but not fulfilling the criteria for a dementia diagnosis. Mild cognitive impairment may be subdivided into amnestic (aMCI) and nonamnestic (naMCI). In aMCI, the mainly affected cognitive domain is memory; in naMCI, the decline occurs in domains other than memory, such as language, executive functions, visuospatial skills, and cognitive processing speed. Both aMCI and naMCI can be further classified as single (aMCI-SD; naMCI-SD) and multiple domains (aMCI-MD; naMCI-MD), depending on the number of functions affected. 3
A hypothetical model to explain the alterations in AD CSF biomarkers over time suggests that pathological levels occur in an orderly manner. These alterations are hypothesized to follow a sigmoidal-shaped and nonlinear temporal course. According to this model, CSF Aβ42 becomes abnormal years before the onset of clinical symptoms and has already reached a plateau by the time cognitive symptoms appear. It is followed by elevations in CSF T-tau and p-tau, which reflects neurodegeneration and deposition of pathologic tau that continues after the symptomatic threshold has been crossed. 4
A new research framework from the National Institute on Aging–Alzheimer’s Association (NIA-AA) proposes a novel AD definition based on biomarkers of neuropathologic change, and the diagnosis moves from syndromic to a biological construct. In this new proposition, individuals are classified according to the presence or absence of the AT(N) biomarkers, where A represents amyloid aggregation, T represents pathologic tau aggregation (NFT), and (N) represents neurodegeneration. In this context, CSF Aβ42 lowering (A+) is considered the best biomarker of early amyloid plaque formation, which associated with normal CSF tau levels composes the “Alzheimer’s pathologic change” in cognitively unimpaired or impaired subjects. 5 The elevation in CSF p-tau (T+) is associated with the paired helical filament tau formation and is considered a more specific biomarker for AD, as it appears normal or mildly elevated in other forms of dementia. 6 The elevation in CSF T-tau (N+) primarily reflects the intensity of neurodegeneration and therefore can be increased in various neurological diseases. 5 Neuropathologic criteria for AD require alterations in both Aβ42 and p-tau, that is, the individual must exhibit an A+ T+ (associated to N+ or N−) biomarker profile; when combined with the clinical stage, they define a person as having preclinical AD (when cognitively unimpaired), AD with MCI, or AD with dementia.
Many clinical studies report that CSF biomarkers provide good accuracy in discriminating cognitively healthy individuals from patients with AD dementia, especially CSF Aβ42 and T-Tau levels combined. 7 In the dementia stage, CSF biomarkers are useful in identifying or excluding AD as the etiology of dementia and in the differential diagnosis in atypical presentations. 8 Other relevant issues regard CSF biomarkers’ predictive value in conversion from cognitively unimpaired to MCI and subsequent dementia,9,10 their usefulness as proxies of cognitive decline progression, and whether they might reliably reflect therapeutic response in clinical trials.
Most cross-sectional studies failed to find a correlation between global cognition and CSF biomarkers at different clinical stages,11-13 although a meta-analysis by Duke et al 14 involving cognitively healthy elderly patients showed that “amyloid positive” (A+; ie, with signs of amyloid deposition) presented poorer cognitive performance than those of “amyloid negative” (A−; ie, no signs of amyloid deposition). Longitudinal studies involving cognitively healthy elderly population have demonstrated that A+ subjects had a more significant cognitive decline over time than those A−.15,16 However, Vemuri et al 17 did not find a correlation between CSF Aβ42 and T-tau levels and the concurrent annual decline in general cognition in patients with aMCI and AD. Regarding neurodegeneration, higher CSF T-tau levels were associated with a subsequent decline in the Mini-Mental State Examination (MMSE) 18 and memory tests in healthy controls. 19
A 2014 Cochrane review 20 reported measurement of CSF Aβ42 levels to be of very little diagnostic utility and concluded for its low accuracy in the detection of AD or in predicting conversion in patients with MCI. Moreover, a 2017 Cochrane review on CSF biomarkers 21 concluded for a “state of uncertainty” regarding the value of CSF testing of T-tau, p-tau, and p-tau/Aβ42 ratio for the diagnosis of AD, including a warning on the risks of mis- and overdiagnosis.
Considering that discrepancies are expected to occur between different approaches in the diagnosis of MCI and AD at different geriatric and memory centers, it is of interest to verify which parameters might be useful to add large-scale diagnostic and prognostic value for practical daily management of patients with cognitive decline. This study’s general objective was to investigate whether CSF biomarkers would be useful to reflect the AD continuum cognitive trajectory in the setting of primary or secondary levels of health care where extensive neuropsychological examination for specific cognitive domains may not be readily available. Previous studies on this subject employed mostly the MMSE as the outcome variable for global cognition. Few studies used the Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog), 17 the Cambridge Cognitive Test (CAMCOG), 12 and the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) battery,22,23 which are brief but more comprehensive batteries than the MMSE and allow a more in-depth analysis of cognitive subdomains. Hence, we used the CAMCOG test, a brief neuropsychological battery, which measures memory (recent, remote, and learning), orientation, language (comprehension and expression), attention/calculation, praxis, abstract thinking, and perception. The original version of the CAMCOG was reported as having a sensitivity of 92% and a specificity of 96% in discriminating cognitively healthy elderly population from patients with dementia. 24 In a previous study, our group found that the CAMCOG was able to discriminate patients with dementia from MCI or cognitively healthy elderly population (sensitivities: 81% and 100%; specificities: 88% and 95%, respectively) and MCI from controls (sensitivity: 64%; specificity: 88%), 25 and different cutoffs according to age and schooling have been described. 26 The specific objective of this study was to verify whether CAMCOG scores (and its subdomains) correlated with AD classic CSF biomarker (Aβ42, T-tau, and p-tau) levels in cognitively healthy elderly population (controls) and patients with aMCI, naMCI, and AD.
Methods
Study Design
We conducted a cross-sectional study to evaluate the correlation between performance in the CAMCOG battery (raw, unadjusted scores) and classic AD CSF biomarkers levels.
Study Sample
The total sample consisted of 143 individuals aged 60 and over, including 51 cognitively healthy subjects (controls), 55 patients with aMCI, 20 patients with naMCI, and 17 patients with mild AD dementia. Patients were evaluated at the psychogeriatric clinic linked to a university tertiary hospital. Recruitment was made through call notes within the hospital, media, and referrals from other outpatient clinics, and those patients who had memory complaints or some concern for cognitive decline were enrolled. Subjects enrolled in the control group were either acquaintance from patients regularly followed in our institution or had a relative with sporadic AD but did not present any subjective cognitive complaints by the time of assessment, and all patients or proxy signed their consent to participate in the study.
Clinical and Neuropsychological Assessment
Patients and controls had their global cognition assessed through the Brazilian version of the CAMCOG, 27 which is embedded in the CAMDEX, a standardized instrument for the examination of mental disorders in the elderly population.
A team of neuropsychologists conducted full neuropsychological assessment through the Fuld Object Memory Evaluation, 28 the Rivermead Behavioural Memory Test, 29 the Trail Making Test parts A and B, 30 and the Revised Wechsler Adult Intelligence Scale Vocabulary and Block Design subtests using reference scores validated for the Brazilian population according to age and schooling. 31
Functional status was assessed using the Informant Questionnaire on Cognitive Decline in the Elderly. 32 All participants were evaluated through the 21-item Hamilton Depression Rating Scale (HDRS-21), 33 and euthymia was considered for scores <8. All patients clinically diagnosed as MCI and AD had their blood counts, biochemical and lipid profile, vitamin B12, folic acid, syphilis serology, and thyroid function tested and performed magnetic resonance imaging studies to rule out metabolic, infectious, and vascular etiologies for cognitive decline. Exclusion criteria were: being illiterate or having a health condition that could limit the administration of neuropsychological tests (such as noncorrectable vision or hearing impairment) or influence cognition (such as noncontrolled hypothyroidism, autoimmune diseases, heart conditions). Patients presenting conditions of high prevalence in the elderly, such as hypertension, diabetes, hypercholesterolemia, osteoarthrosis, and so on, were not excluded as long as they were well controlled and could perform the tasks. We also excluded individuals with a history or evidence of cerebrovascular injury, non-AD dementias, and other neurologic/psychiatric conditions that might impair cognition (such as severe traumatic brain injury, epilepsy, depression, bipolar disorder, and psychosis).
Diagnosis
The clinical diagnosis was defined by consensus among a multidisciplinary team (comprising psychiatrists, a neurologist, a geriatrician, neuropsychologists, occupational therapists, and a speech therapist), taking into account the results of clinical, neuropsychological, laboratory, and neuroimaging studies. Controls were defined as those individuals who had a neuropsychological and functional performance within the normal range for their age and schooling levels. The diagnosis of MCI and subtypes was based on Petersen criteria, 34 and AD diagnosis of AD followed the NIA-AA criteria. 35 The CAMCOG scores were not taken into account for diagnosis definition.
The CSF Biomarker Analysis
The samples of CSF were collected in the morning by lumbar puncture in the intervertebral space L3-L4 or L4-L5, with a 23-gauge needle making use of polypropylene tubes. A total of 12 to 15 mL of each sample were centrifuged at 3200g for 10 minutes at 4 °C. The following procedure was to separate the samples in 0.5 mL aliquots, and immediately, they were frozen at −80 °C until analysis. The Aβ42, p-tau181, and T-tau CSF biomarkers were analyzed in duplicate with the INNo-Bia AlzBio3 assay (Innogenetics), a multiplex microsphere-based Luminex MAP platform that allows simultaneous analysis of these biomarkers. Following the pre-wetting of the filter plate with a wash buffer, a suspension of microspheres containing the corresponding capturing antibodies (4D7A3, AT270, AT120 to Aβ42, p-tau e T-tau, respectively) was incorporated into the plate. A mixture of biotinylated detection monoclonal antibodies made for the specific detection of capturing antibodies (3D6 to Aβ1-42 and HT7 for T-tau and p-tau) and 75 µL of CSF or standards were added to the plate and incubated during night in the dark. The plate was washed, and a detection conjugate (phycoerythrin-labeled streptavidin) was incubated for 1 hour at room temperature. The plate was washed, and after the addition of a reading solution (phosphate-buffered saline), the assay was analyzed on a Luminex 100 IS platform (Luminex). Standard curves were drawn for each biomarker employing a sigmoidal curve fitting method, and the mean fluorescence values for duplicate CSF samples were used to establish the concentration of Aβ42, p-tau, and T-tau.
Statistical Analysis
Our sample showed a non-normal distribution across all variables as defined by the Kolmogorov-Smirnov test, and nonparametric tests were employed for all analyses with post hoc tests for multiple comparisons. Mean differences in sociodemographic characteristics, CAMCOG scores, and levels of biomarkers in the CSF by clinical diagnostic group (controls, aMCI, naMCI, AD) were evaluated through analysis of variance (Kruskal-Wallis test) followed by Dunn test for pairwise comparison. After logarithmic transformation of data, age and schooling were used as covariates when comparing means by analyses of variance. Spearman partial correlation coefficients using age as a covariate were used to evaluate the association between CSF biomarkers levels (Aβ42, T-tau, p-Tau, and Aβ42/p-Tau ratio) and cognitive performance in the total sample and by clinical diagnostic group. Sex distribution was analyzed through the χ2 test. A P value <.05 was considered significant for mean comparisons among groups, and a P value <.01 was considered significant for all correlation analyses (after Bonferroni correction). Analyses were performed using the software IBM SPPS Statistics version 25.
Results
Patients with AD and MCI were older (P = .037) and less educated than controls (P = .044), but there were no significant differences in age and schooling among the cognitively impaired groups (aMCI, naMCI, and AD). There were no differences among groups in sex distribution (P = .748). As expected, patients with AD had the lowest scores in the CAMCOG (total) (P < .001), as well as in the subdomains language (P < .001), memory (P < .001), perception (P = .005), and praxis (P < .001). Patients with aMCI performed poorer than controls in memory (P < .001; Table 1). There were no intergroup differences in the HDRS-21 items scores, and controls performed better than AD in the IQ-CODE. Regarding CSF biomarkers, patients with AD showed the lowest Aβ42 (P < .001), the highest T-tau (P < .001), and the lowest Aβ42/p-tau ratio (P < .001). P-tau levels were higher in aMCI and AD when compared to controls (Table 1).
Demographic, Clinical, and Cognitive Characteristics of the Sample According to Baseline Diagnosis.a
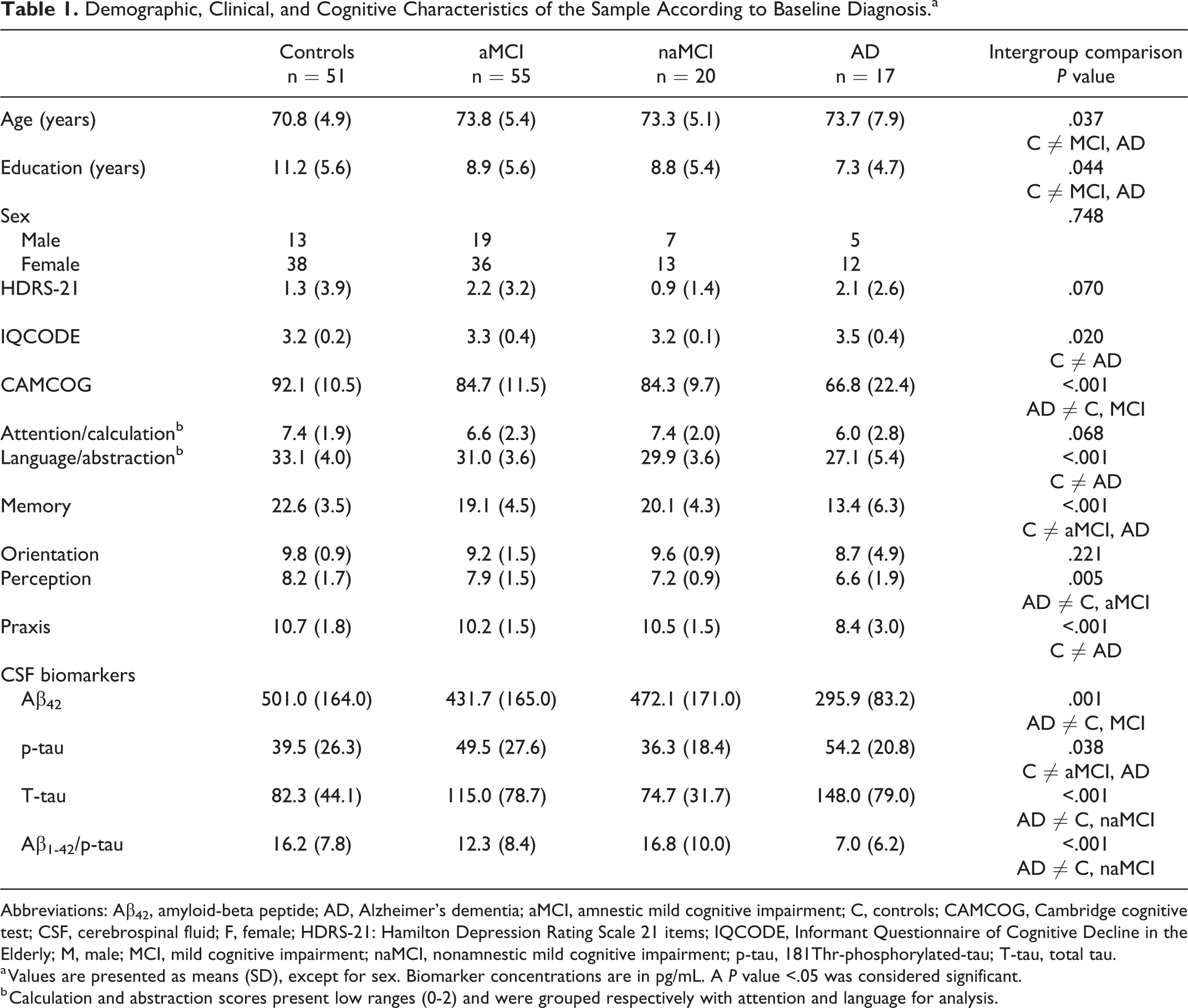
Abbreviations: Aβ42, amyloid-beta peptide; AD, Alzheimer’s dementia; aMCI, amnestic mild cognitive impairment; C, controls; CAMCOG, Cambridge cognitive test; CSF, cerebrospinal fluid; F, female; HDRS-21: Hamilton Depression Rating Scale 21 items; IQCODE, Informant Questionnaire of Cognitive Decline in the Elderly; M, male; MCI, mild cognitive impairment; naMCI, nonamnestic mild cognitive impairment; p-tau, 181Thr-phosphorylated-tau; T-tau, total tau.
a Values are presented as means (SD), except for sex. Biomarker concentrations are in pg/mL. A P value <.05 was considered significant.
b Calculation and abstraction scores present low ranges (0-2) and were grouped respectively with attention and language for analysis.
In the total sample, CAMCOG scores and language correlated with T-tau levels. All biomarker levels correlated with the memory subdomain. There were no correlations between the attention, perception, and praxis domains with any biomarker level (Table 2).
Spearman Correlation Coefficients (rho) Between Cognitive Performance and CSF Biomarkers Levels for the Total Sample, Using Age and Schooling as Covariates.a
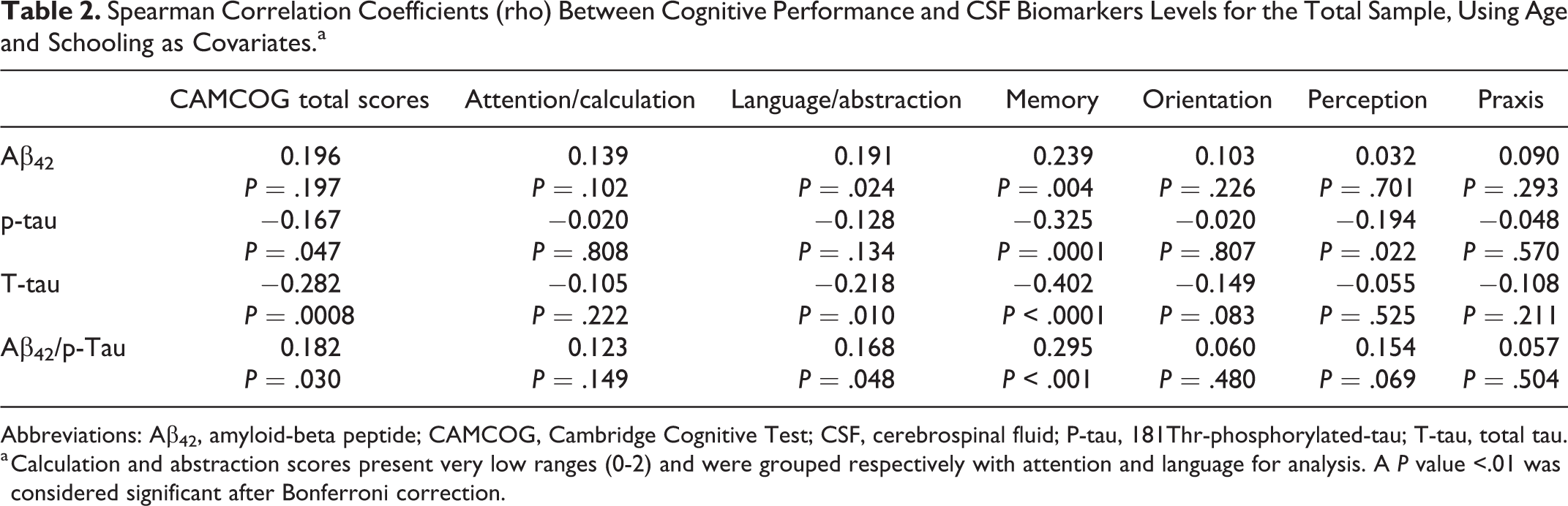
Abbreviations: Aβ42, amyloid-beta peptide; CAMCOG, Cambridge Cognitive Test; CSF, cerebrospinal fluid; P-tau, 181Thr-phosphorylated-tau; T-tau, total tau.
a Calculation and abstraction scores present very low ranges (0-2) and were grouped respectively with attention and language for analysis. A P value <.01 was considered significant after Bonferroni correction.
We did not find any significant correlations between CSF biomarkers levels and diagnosis after correction for multiple comparisons when analyzing each diagnostic group separately (Table 3, Figure 1).
Spearman Correlation Coefficients (rho) Between Cognitive Performance and CSF Biomarkers Levels by Diagnostic Subgroup, Using Age and Schooling as Covariates.a
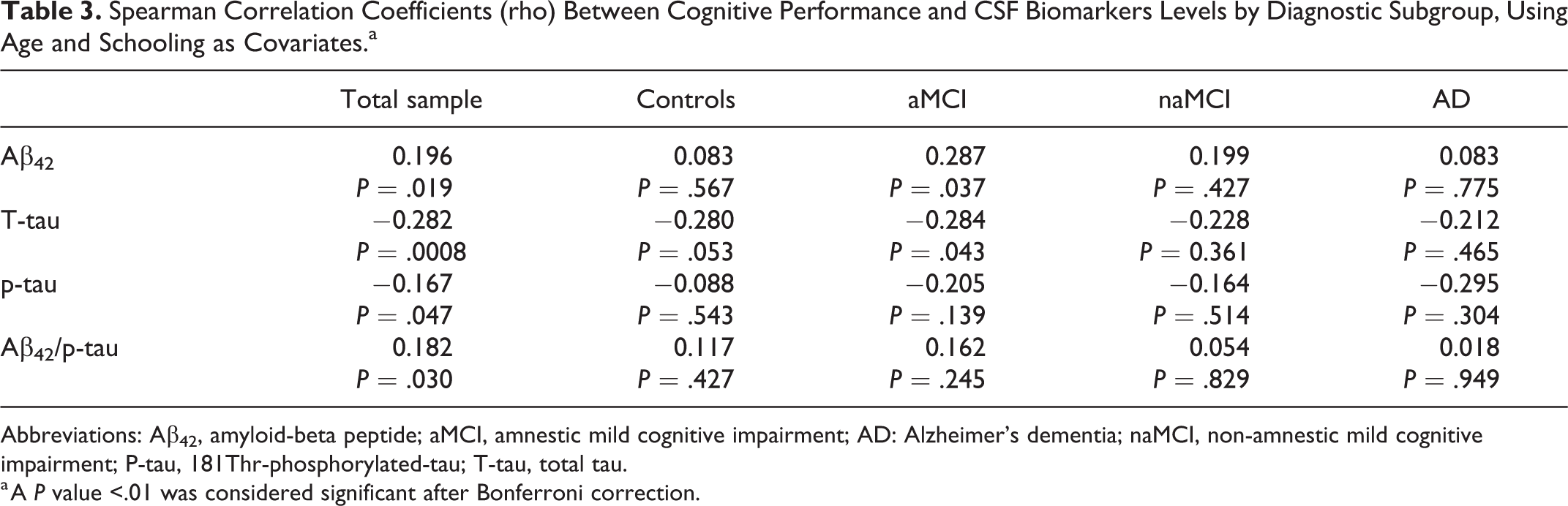
Abbreviations: Aβ42, amyloid-beta peptide; aMCI, amnestic mild cognitive impairment; AD: Alzheimer’s dementia; naMCI, non-amnestic mild cognitive impairment; P-tau, 181Thr-phosphorylated-tau; T-tau, total tau.
a A P value <.01 was considered significant after Bonferroni correction.
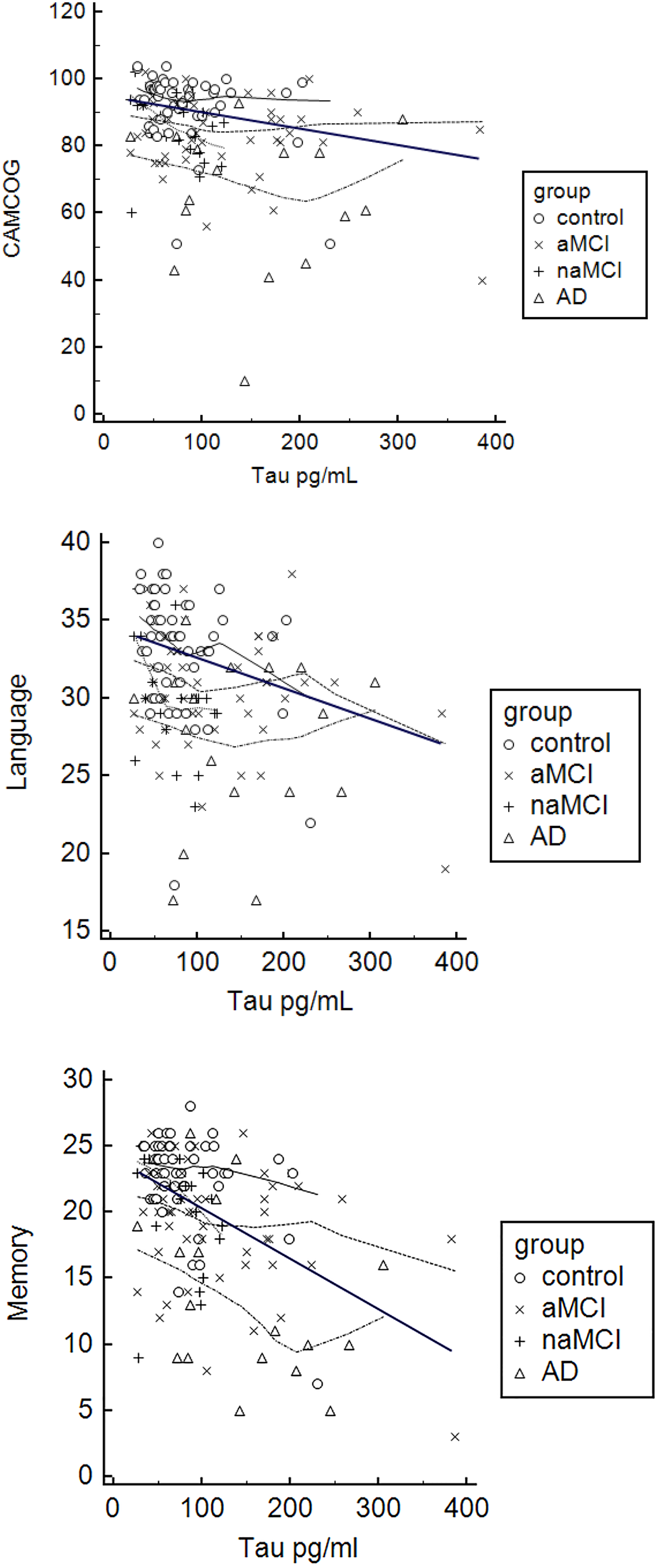
Correlations between cerebrospinal fluid (CSF) levels of T-tau and performance in the Cambridge Cognitive Test (CAMCOG), language subtest, and memory subtest by diagnostic group. The thicker line represents the overall correlation in each task.
Discussion
In the past few years, CSF biomarkers have been incorporated in the diagnostic algorithm for AD. Consequently, there has been a growing interest in verifying these biomarkers’ performance in predicting cognitive trajectories along the cognitively healthy–MCI–dementia continuum. Our study aimed to determine the association between CSF levels of Aβ42, T-tau, p-tau, and Aβ42/p-tau ratio with cognitive performance in a sample of elderly ranging from cognitively healthy to clinical AD through a brief neuropsychological battery (the CAMCOG). Various studies have described correlations between specific cognitive domains (such as memory or executive functions) and specific CSF biomarkers; therefore, we tried to further investigate this issue by pursuing correlations between CAMCOG subdomains and CSF biomarkers. We tried to interpret our results based on the hypothetical model of the dynamic of AD biomarkers proposed by Sperling et al, 36 in which the progression of biomarkers over time obeys a sigmoid-shaped curve.
Findings in the Total Sample
In the sample as a whole, CAMCOG total scores and language subscores correlated with T-tau levels, and memory subscores correlated with all CSF biomarkers. The association between T-tau concentrations and cognitive measures (in the absence of association with the other biomarkers) might be because T-tau reflects a broader spectrum of mechanisms to neuronal injury, therefore being more suitable to represent the loss of cognitive reserve even in patients where the AT(N) criteria for AD diagnosis are not followed. 37
Correlations between CSF biomarkers and global scores in cognitive tests in the continuum normal cognition to AD were reported by Solé-Padullés et al 38 (Aβ42), Jack et al 39 (Aβ42 and T-tau), and Vemuri et al 11 (Aβ42, T-tau, and p-tau). Conversely, Spies et al 12 and Tsolaki et al 13 did not find correlations between CAMCOG total scores and levels of any CSF biomarkers. Our results agree with those by Jack et al 39 and Vemuri et al 11 regarding T-tau levels, but we could not find correlations between global cognition and Aβ42 or p-Tau levels.
In our study, all CSF biomarkers correlated with the memory subdomain. This finding suggests that memory might be the cognitive subdomain that reflects more closely the burden of amyloid and Tau-proteins that finally lead to neuronal damage. Similar results were reported in tests of visual and verbal memory 22 and word delayed recall in women 23 in cohorts involving the spectrum controls to AD. Associations between low CSF Aβ42 and T-tau levels with episodic memory (visual and verbal) performance have also been described by Reijs et al 40 in a sample of elderly population ranging from cognitively normal to AD.
We found only one study exploring the association between cognition and Aβ42/p-tau ratio, a measure conceived to enhance the discrimination and predictive power of CSF biomarkers.41,42 Racine et al 43 reported p-tau/Aβ42 ratios to negatively correlate with a working memory task in both cognitively healthy and impaired elderly population. In our sample, the Aβ42/p-tau ratio correlated with the memory subdomain.
Our results showed that performance in the language subdomain correlated with T-tau levels. This finding was surprising given that we did not include patients with presenile AD (in which language impairment often occurs earlier and more intensively in the course of the disease). We found only 2 previous reports associating CSF biomarkers and language tasks. Both correlate increased CSF T-tau levels with lower performance in animal fluency in patients with MCI (a cross-sectional study) 44 and the cognitively healthy AD continuum (a longitudinal study). 40
Findings by Diagnostic Subgroup
We did not find any significant correlations between CSF biomarkers levels and CAMCOG total scores when analyzed by diagnostic subgroup (controls, aMCI, naMCI, AD), which is in line with some previous reports,12,45 but in disagreement with a number of studies which reported associations between CSF biomarkers and cognitive measures in specific diagnostic groups.
Focusing on each biomarker separately, we found some studies highlighting associations between CSF Aβ42 levels and cognition in cognitively normal elderly population, 46 in patients with subjective memory complaints,22,47 and in patients with aMCI. 48 Higher baseline values of CSF T-tau might predict cognitive decline in cognitively healthy subjects,19,49 the transition from cognitively healthy to MCI, 18 and from MCI to dementia. 50 Association between memory performance and CSF p-tau levels was described in patients with MCI. 51 Elevation in CSF p-tau represents the hallmark of tau pathology 5 that has been documented as a good predictor of progression to dementia, 52 but its role as a proxy for cognitive status remains to be defined in AD dementia clinical phenotype. 53
The hypothetical model proposed by Sperling et al 36 describes CSF Aβ42 levels to decrease several years before the onset of cognitive symptoms to reach a plateau by the time the symptomatic threshold is reached (transition from cognitively normal to MCI). Therefore, CSF Aβ42 is expected to correlate with cognitive performance mostly in the preclinical stage or MCI45,48,54 and may be regarded as a marker for AD development but not a proxy for disease severity. The CSF evidence of neurodegeneration (elevation in T-tau levels) and pathological Tau deposition (elevation in p-tau levels) start later than that of cerebral amyloidopathy and will reach a plateau only in overt dementia stage, thus better reflecting cognitive decline over time.5,6 This dynamic was not replicated in our results when we analyzed CSF biomarkers/CAMCOG associations by diagnostic subgroup, which is likely due to the small number of patients that limited statistical power for subgroup analyses. Moreover, this nonlinear relationship is more prone to be documented in longitudinal studies.
It is worth noting that even the significant correlations found in our study are low. All data reviewed for this study showed that correlation coefficients between cognitive parameters and any CSF biomarker revolve around 0.3 to 0.4 at best, implying that most of the variance defining cognitive impairment remains unclear and is multifactorial, such as the co-occurrence of vascular disease or Lewy body pathology, APOE status, lifestyle parameters, cognitive reserve, among others.46,53 Hence, in a cohort of patients clinically diagnosed as AD, different factors may collaborate and interact to produce cognitive impairment, which may influence the index of correlation between CSF biomarkers level and cognition.
Finally, it has been hypothesized that from the dementia stage, all CSF biomarkers will reach a plateau but that has not been empirically confirmed as patients with moderate to severe AD are not able to participate in research studies. 4 Thus, once the dementia is full-blown, correlations between CSF biomarkers and the severity of cognitive impairment will disappear. We did not find correlations between CSF biomarkers and cognitive performance in our AD group, as reported by Liguori et al. 55
Limitations of the Study
The main limitations of our study are: (1) the cross-sectional design that does not allow to discriminate between cognitive stable and potential converters in control and MCI groups, (2) we used a convenience sample, that is, certainly subgroup analyses were underpowered, (3) we intended to perform an analysis of cognition/CSF biomarkers following diagnostic procedures limited to those employed in primary and secondary levels of health care; therefore, we did not use the 2018 NIA-AA AT(N) diagnostic criteria, and (4) we have probably included patients with clinically defined Limbic-predominant age-related TDP-43 encephalopathy neuropathological change (LATE-NC) or any other condition that might be associated with CSF T-tau elevation. 52 Further studies starting from this new framework might be of interest considering that, albeit demonstrating a good sensitivity when applied to patients clinically diagnosed as AD, the AD continuum profile was found in a high proportion of patients diagnosed as non-AD dementias. 56
Conclusions
We aimed to verify whether cognitive performance correlated with CSF biomarkers levels in a sample of subjects in the cognitively healthy elderly–AD continuum as a means to understand the potential usefulness of such biomarker measures in primary and secondary levels of care. To accomplish that, we chose to diagnose our subjects primarily based on diagnostic procedures available at such levels of care and to assess cognition employing an instrument that is more accessible for nonspecialists, that is, the CAMCOG.
In general, we observed that performance in memory correlated with all biomarkers levels and the Aβ42/p-Tau ratio. T-tau levels correlated with global cognitive performance in the total sample, although several variables may interact to produce an increase in T-tau levels, such as cognitive status, presence of vascular-related factors, gait speed, history of cancer, and indeed the levels of Aβ42. 57 Finally, as proposed by Jack et al, 39 the correlation between classical CSF biomarkers and cognition may follow a nonlinear pattern yet to be demonstrated in more extensive longitudinal studies. We conclude that, currently, the inclusion of classical CSF biomarkers in clinical settings with limited resources (ie, nonspecialized clinics and hospitals) is not helpful as an indicator to estimate an individual’s cognitive trajectory more than the cognitive evaluation itself. However, our results also disclose that in the specific case of episodic memory and T-tau levels, correlations with CSF biomarkers might prove more robust and eventually become useful as supportive instruments in monitoring disease progression and response to therapeutic interventions.
Footnotes
Authors’ Note
The study was approved by the Hospital das Clinicas Research Ethics Committee (CAPPesq) and a National Research Ethics Committee (Plataforma Brazil). Rómel Ibarra contributed to literature search, interpretation of data, and writing of the manuscript. Marcia Radanovic contributed to study design, acquisition, and interpretation of data, statistical analysis, manuscript revision, and final approval of the manuscript. Leda L. Talib contributed to CSF analyses. Orestes V. Forlenza contributed to study concept, intellectual contributions to the study, manuscript revision, and final approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: The Laboratory of Neuroscience (LIM-27), University of Sao Paulo, receives financial support from the Alzira Denise Hertzog Silva Association (ABADHS), Instituto Nacional de Biomarcadores em Neuropsiquiatria (INBION), Sao Paulo Research Foundation (FAPESP; Projects 09/52825-8, 2014/14211-6, 2016/01302-9), and National Council for Scientific and Technological Development (CNPq; Projects 442795/2014-9 and 466625/2014-6).