
Abstract
Objective:
To examine the effect of employment status on sleep, care burden, and negative affect among family caregivers (FCs) at home.
Methods:
An intensive longitudinal design was applied in which 25 FCs underwent in-home assessments for up to 56 days. At baseline, demographic data and employment status were collected. FCs wore a wrist-worn device with an accelerometer to assess objective total sleep time (TST) for consecutive 24-hour periods. FCs answered the Zarit Burden Interview (ZBI) and Positive and Negative Affect Schedule (PANAS) every night before sleep. Linear mixed model analysis was used to examine the effect of objective sleep status on ZBI and PANAS scores the following day.
Results:
Mean participant age was 66.3 ± 10.8 years (72.0% female), and mean survey period was 29.1 ± 9.6 days (866 observations). Mean TST of FCs was 5.7 ± 1.4 hours. In total, 32.0% of FCs were employed either full- or part-time. TST of employed FCs was significantly associated with care burden and negative affect (B = −0.4 and −1.3, respectively); however, positive affect was not associated with TST. FCs who were unemployed experienced less care burden and negative affect (rate of change: −7.7 and −8.0, respectively). Additionally, TST of unemployed FCs was associated with negative affect; thus, when they slept 1 hour longer than their mean TST, they experienced less negative affect the following day.
Conclusion:
A reduction in TST could lead to increased care burden and more severe negative affect the following day, which may be moderated by employment status.
Introduction
Providing informal care to a family member often compromises caregivers’ mental and physical health, including sleep status.1-8 Previous studies have reported that poor sleep is linked to many other health problems for family caregivers (FCs), such as depression, care burden, poor subjective well-being, and cardiovascular disease.6,8,9 However, there is limited research about the intensive longitudinal effects of objective sleep status on care burden and negative and positive affect the following day, or the moderating factors of these associations.2,8 One previous study that analyzed the relation between sleep status and positive affect suggested that elevated levels of positive affect were longitudinally associated with better subjective sleep status but not objective sleep status, as measured by a wrist-worn device with an accelerometer for consecutive 3-day periods. 8 Although other studies have measured sleep status of FCs for 1 night or over a few days to examine the relationship between objective sleep status and care burden, it has been a challenge to calculate representative values of objective sleep status under home care conditions that cause variations in the sleep status of FCs.2,6 If daily sleep variabilities could be objectively measured for a longer period than in previous studies, the relationship between objective sleep status, care burden, and positive and negative affect might be clarified, helping to fill a gap left by previous studies.
FCs play many roles in addition to caring for those requiring care. The employment rate of middle-aged FCs is increasing in Japan, 10 therefore, it is an urgent task for FCs to provide support that allows nursing care to continue at home while working. Recent studies have evaluated associations among employment status and objective sleep status, and findings suggest some nonlinear effects of employment status on the associations between sleep and fatigue, such as negative affect in FCs.11,12 One study was guided by the Work, Nonwork, and Sleep framework. 12 This framework characterizes longer sleep duration and better sleep quality as factors that regenerate physical energy and that are related to the capacity to work and provide care. 11 However, few studies have examined the naturally occurring association between sleep and care burden in the context of FCs’ employment status in Japan. Based on the Work, Nonwork, and Sleep framework and the presented empirical evidence, we set a hypothesized model of factors influencing care burden and negative affect among FCs as the conceptual framework for this study (Figure 1), comprising the following 2 hypotheses:
H1: total sleep time (TST) the previous day negatively predicts care burden and negative affect the following day;
H2: employment status of FCs is a moderator and boosts the negative association between sleep, care burden, and negative affect the following day.
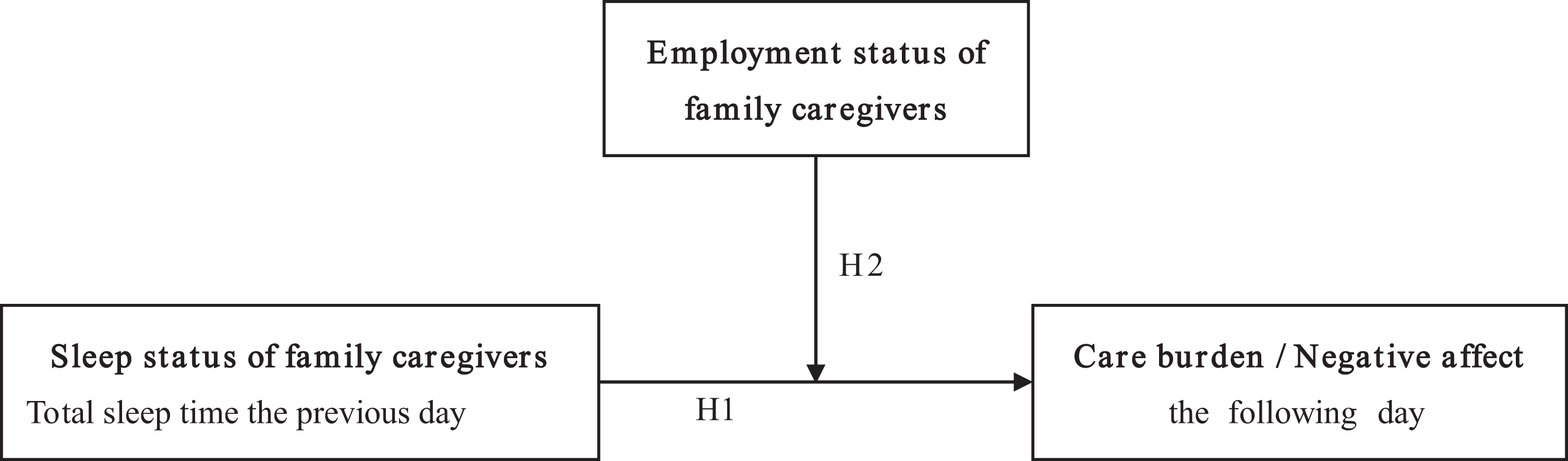
Hypothesized model of factors influencing care burden and negative affect the following day among family caregivers who are employed or unemployed. H1, hypothesis 1; H2, hypothesis 2.
As the number of people requiring care rapidly increases in Japan and other super-aged nations, more FCs continue to take care of their relatives while remaining employed. Additionally, the number of FCs who provide home care in Japan has consistently been increasing, reaching about 7 million in 2016, and the number of middle-aged FCs and the time required for caregiving have also increased. 10 At the same time, more than 40% of FCs are engaged in work other than taking care of relatives. 10 Thus, it is an urgent task to examine how employment status plays a role in the associations between sleep, care burden, and negative affect. Therefore, the purpose of this study was to examine the effect of employment status on objective sleep status, care burden, and negative affect among FCs in their homes.
Methods
Study Design and Participants
The current study was part of an intensive longitudinal survey conducted from February 2017 to March 2019 that investigated the health and objective sleep status of FCs in a home care setting. 9 Participants constituted 25 dyads of primary FCs and care receivers (CRs) living together, recruited from 3 day-service providers and 1 nursing home respite service in a general residential area in Osaka, Japan. CRs were aged 65 years and older and under the long-term care insurance system in Japan. We conducted the survey while CRs were not using the respite service to ensure that data were collected while FCs and CRs spent time at home together. At the baseline survey, the 25 dyads participated for 14 consecutive days. At 3 months, 6 months, and 1 year after the baseline survey, this study followed the same protocol. The objective sleep measures were collected at these intervals for 14 consecutive days each time; however, 1 CR died and 3 CRs were hospitalized after the baseline survey. Thus, after the baseline survey, 21 dyads participated until their CRs died, were hospitalized, or it became too difficult for FCs to continue participation. Of those, 11 dyads participated for 28-29 days, 4 dyads participated for 42-44 days, and 6 dyads participated for 54-56 days; therefore, the data collection period was between 14 and 56 days for all dyads.
Measurements
In the baseline survey, age; sex; level of care required (national standard for care needs was determined by assessing applicants’ severity of physical disability and dementia: care levels 1-5, ranging from the lowest to the highest care needs level); CRs’ assistance requirement regarding moving, bathing, eating, and toileting; CRs’ age at care service use onset; duration of care service use; and clinical history were collected.13,14 Both FCs and CRs were asked if they had ever been told by a physician that they had dementia, with answers coded as yes or no. Current employment information of FCs was collected regarding work status (full-time, part-time, or non-worker, including retirement). FCs’ working hours per day, working days per week, and duration of current work were also collected at baseline.
Sleep measurement
After the baseline survey, objective sleep status was measured using an ActiGraph GT9X (ActiGraph, Florida, USA), which was worn for consecutive 24-hour periods for between 14 and 56 consecutive days on FCs’ non-dominant wrist. Actigraphy has been validated and recommended for use among elderly populations and has been compared favorably with polysomnography, which is considered the “gold standard” for sleep assessment.15-18 Recorded actigraphy data were analyzed using ActiLife software (version 6, by ActiGraph, Florida, USA). The following sleep parameters were calculated across time periods: (1) TST; amount of time spent sleeping in minutes); (2) total time in bed (amount of time spent in bed between in-bed and final out-of-bed times of nocturnal sleep period in minutes); (3) sleep efficiency (ratio of total sleep time to total time in bed); and (4) wake after sleep onset at night between initial sleep onset and final awakening.
The Japanese version of the Pittsburgh Sleep Quality Index (PSQI) was used as a baseline assessment to quantify subjective sleep disturbance in FCs and CRs.19,20 PSQI scores range from 0 to 21, with PSQI scores of 5 or greater indicating clinically significant sleep disturbance. The Cronbach’s alpha of the PSQI has been calculated as 0.83, and its construct validity has also been verified. 19
Other factor measurements
The following factors were measured at baseline and 3 months, 6 months, and 1 year after baseline. The mean scores of the following measurements were calculated in this study.
The well-being of FCs and CRs was measured using the Japanese version of the WHO-Five Well-being Index (WHO-5), at baseline and 3 months, 6 months, and 1 year after baseline. 21 The scale consists of 5 items. Scores range from 0 to 25, and higher scores indicate better well-being. The Cronbach’s alpha of the WHO-5 has been calculated as 0.87, and its construct validity has also been verified. 21
Depressive mood was assessed for both FCs and CRs using the 15-item Geriatric Depression Scale (GDS-15). 22 The GDS-15 is a questionnaire specifically developed to screen for and assess depression in the elderly.22,23 The Cronbach’s alpha of the GDS-15 has been calculated as 0.87, and its construct validity has also been verified. 22
Assessment of Care Burden and Positive and Negative Affect
Caregiver burden was assessed using the short version of the Zarit Caregiver Burden Interview (ZBI_8).24,25 It is a commonly used measure of care burden and has been utilized with older adults. 9 Total scores range from 0 to 32, and higher scores indicate a more severe care burden. The Cronbach’s alpha of the ZBI_8 has been calculated as 0.93, and its construct validity has also been verified. 24
FCs’ positive affect, such as the feeling of happiness, cheerfulness, and enjoyment, and negative affect, such as the feeling of distress, hostility, and fear, they felt at the moment the survey was given were assessed using the Positive and Negative Affect Schedule (PANAS).26,27 The Cronbach’s alpha of positive and negative affect has been calculated as 0.90 and 0.91, respectively, and the PANAS has shown good validity in older adults.8,26,28 FCs rated 10 items each for both negative and positive affect on a 5-point scale ranging from 1 (very slightly or not at all) to 5 (extremely). The total score was calculated from 10 to 50 for either scale. FCs answered the ZBI_8 and PANAS every night before going to bed during the study period.
Statistical Analyses
Sociodemographic and clinical characteristics were expressed as means, standard deviations, and percentages. They were calculated after excluding those with missing data. Spearman’s rank correlation analysis was performed between objective and subjective sleep parameters, care burden, and positive and negative affect. The current employment status of FCs was used to stratify their employment status as groups: those who were employed (full-time or part-time) and those who were unemployed (non-worker, including retirement). Differences between employed and unemployed FCs were obtained using Mann-Whitney U-tests for continuous variables and Fisher’s exact tests for dichotomous variables. A mixed model using data across the entire study period was run for caregiving burden and positive and negative affect using ZBI_8 and PANAS scores as dependent variables. The model estimated an intercept and slope for each FC based on all available data for that individual, augmented by data from the entire sample. TST was centered by overall mean. Slopes indicated the rate of change for 1 hour of TST. Employment status indicated FCs who worked a full- or part-time job during the day. A dummy variable was based on employment status and showed the rate of change for FCs who were unemployed. Slope estimates indicated non-standardized coefficients in the models. Statistical analysis was performed using SPSS 25 (IBM Japan). A probability value of P < 0.05 was considered statistically significant.
This study was approved by the internal review board of the Graduate School of Health Sciences, Kobe University (approval numbers 544 and 720), conforming to the provisions of the Declaration of Helsinki. After receiving a complete description of all procedures for this study, all CRs and FCs provided written informed consent.
Results
Participant Characteristics
The mean survey period was 29.1 ± 9.6 days (866 observations). The mean age was 66.3 ± 10.8 years for FCs and 82.8 ± 8.2 years for CRs, and 72.0% of FCs and CRs were female (Table 1). Mean ZBI_8, positive affect, and negative affect scores during the survey were 7.3 ± 6.8, 19.8 ± 8.4, and 16.1 ± 6.4, respectively. Of those, 41.6% of FCs and 55.6% of CRs scored above the GDS-15 threshold of 5, indicating depressive mood. Mean TST of FCs was 5.7 ± 1.4 hours per day. Regarding CRs who required moving assistance, 24.0%, 36.0%, and 40.0% needed assistance because they were bedridden, used a wheel chair, or were ambulatory, respectively. Further, 76.0%, 60.0%, and 80.0% of CRs needed bathing, eating, or toileting assistance, respectively. FCs who worked full- or part-time totaled 32.0%. Of those, working hours per day, working days per week, and duration of current work were 5.2 ± 1.9 hours, 3.6 ± 1.0 days, and 9.3 ± 5.9 years, respectively. Age, ZBI_8 scores, TST, and total time in bed showed significant differences between FCs who were employed and those who were unemployed. FCs who were employed were significantly younger, felt a severe care burden, slept for shorter periods of time, and spent less time in bed than unemployed FCs, but there were no significant differences between employed and unemployed FCs regarding FCs’ positive and negative affect; FCs’ and CRs’ GDS-15, WHO-5 Well-Being, and PSQI scores; and CRs’ assistance required for moving, bathing, eating, and toileting. Finally, there was a significant correlation between FCs’ PSQI and ZBI_8 scores (Supplemental Table 1), whereas no significant correlation was found between PSQI and positive and negative affect.
Participant Characteristics According to Caregiver’s Employment Status.
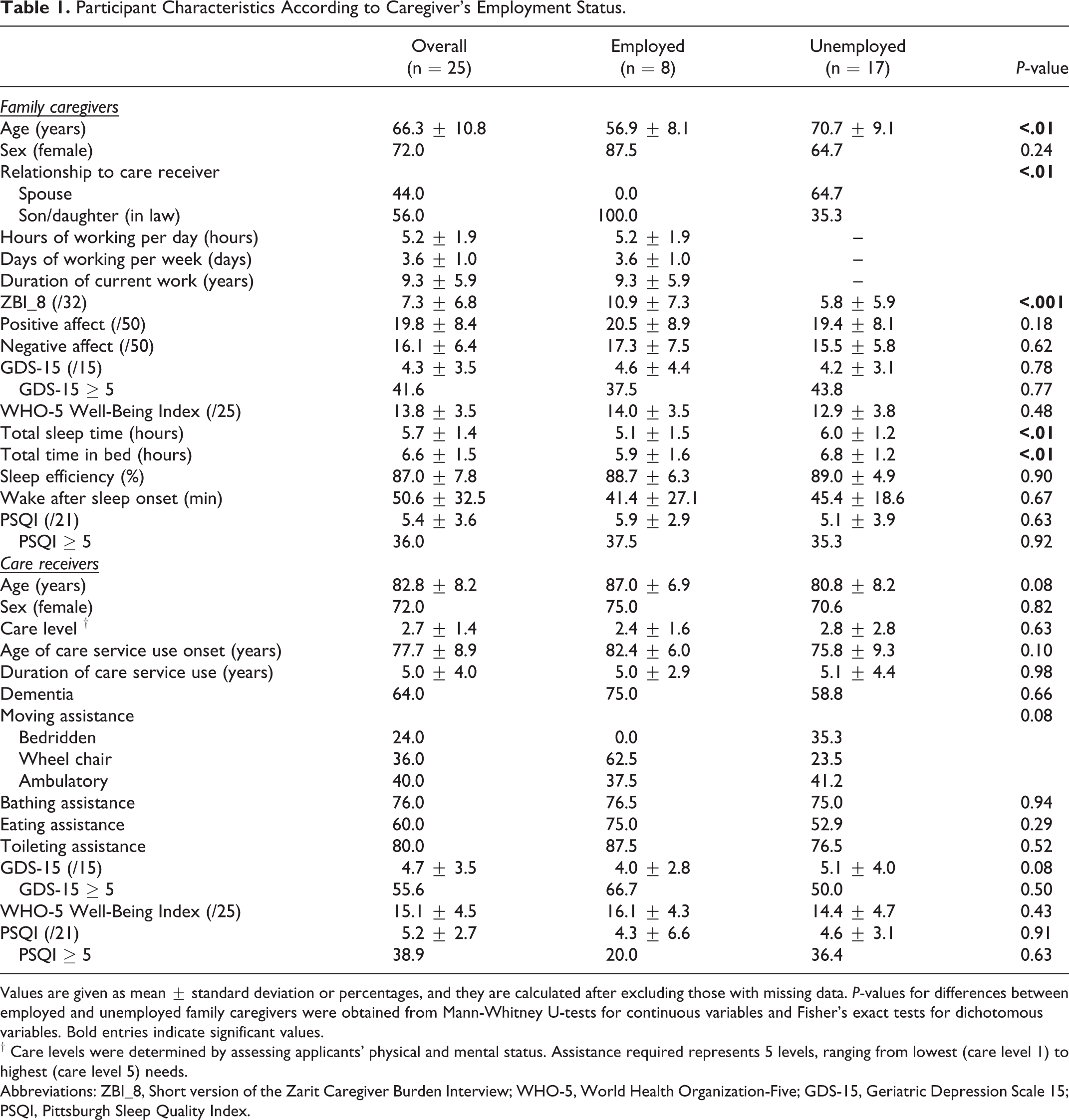
Values are given as mean ± standard deviation or percentages, and they are calculated after excluding those with missing data. P-values for differences between employed and unemployed family caregivers were obtained from Mann-Whitney U-tests for continuous variables and Fisher’s exact tests for dichotomous variables. Bold entries indicate significant values.
† Care levels were determined by assessing applicants’ physical and mental status. Assistance required represents 5 levels, ranging from lowest (care level 1) to highest (care level 5) needs.
Abbreviations: ZBI_8, Short version of the Zarit Caregiver Burden Interview; WHO-5, World Health Organization-Five; GDS-15, Geriatric Depression Scale 15; PSQI, Pittsburgh Sleep Quality Index.
Changes in Main Outcomes
Figure 2 shows the model-predicted change of care burden (top) and negative affect (bottom) in terms of TST and the between-person differences according to FCs’ employment status. As indicated by the solid line, employed FCs’ care burden and negative affect were higher than those of unemployed FCs on average. Additionally, TST had a negative effect on care burden; thus, a longer TST of FCs who worked full- or part-time was associated with lower ZBI_8 scores.
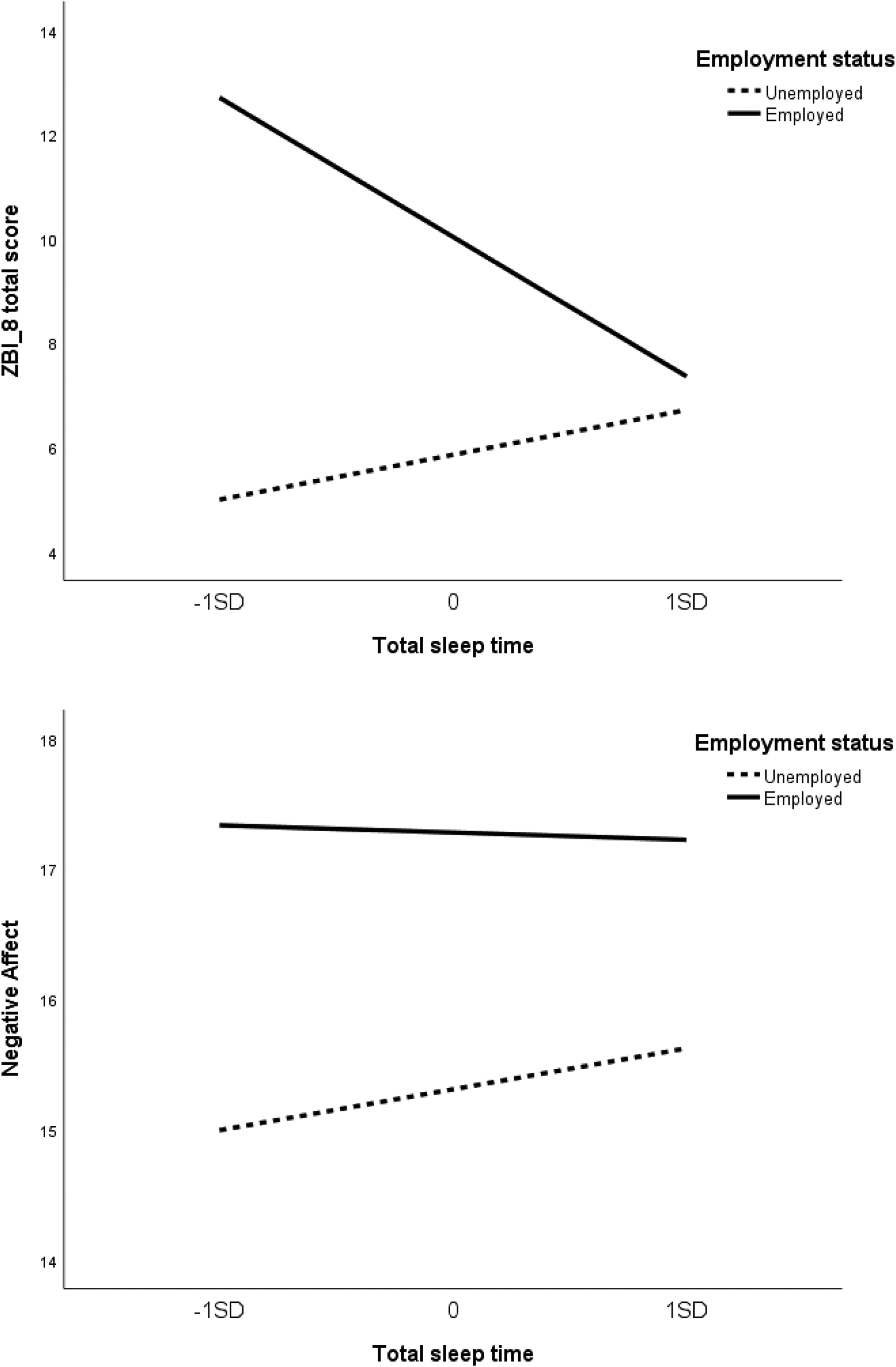
Model-predicted change of care burden (top) and negative affect (bottom) in terms of total sleep time. Average regression lines for employed (solid line) and unemployed (dotted line) groups. Total sleep time was centered by the mean of each group before being standardized. Slopes indicate the rate of change for 1 SD of total sleep time. Abbreviations: SD, standard deviation; ZBI_8, Short version of the Zarit Caregiver Burden Interview.
Moderation Effect of Employment Status
The results of a fitted multilevel model for changes in scores for the ZBI_8, positive affect, and negative affect were as follows: TST of FCs who were employed was significantly associated with ZBI_8 and negative affect scores (B = −0.41 and −1.30, respectively); positive affect scores were not associated with TST. FCs who were unemployed and with average TST experienced significantly less care burden (rate of change: −5.7; Table 2). Additionally, TST of unemployed FCs was associated with negative affect: on days when they slept 1 hour longer than their mean TST, they experienced less negative affect the next day (rate of B change: 1.45). As seen in Table 1, mean age was significantly different between employed and unemployed FCs; therefore, the same multilevel model was used to determine changes in ZBI_8, positive affect, and negative affect scores according to age (Supplemental Table 2). Results showed the TST of FCs 65 years old or younger was not significantly associated with ZBI_8 or positive or negative affect scores; however, on days when elderly FCs slept 1 hour longer than their mean TST, they experienced less care burden the next day (rate of change: −0.72).
Mixed Models on Caregiver Burden, Positive Affect, and Negative Affect.
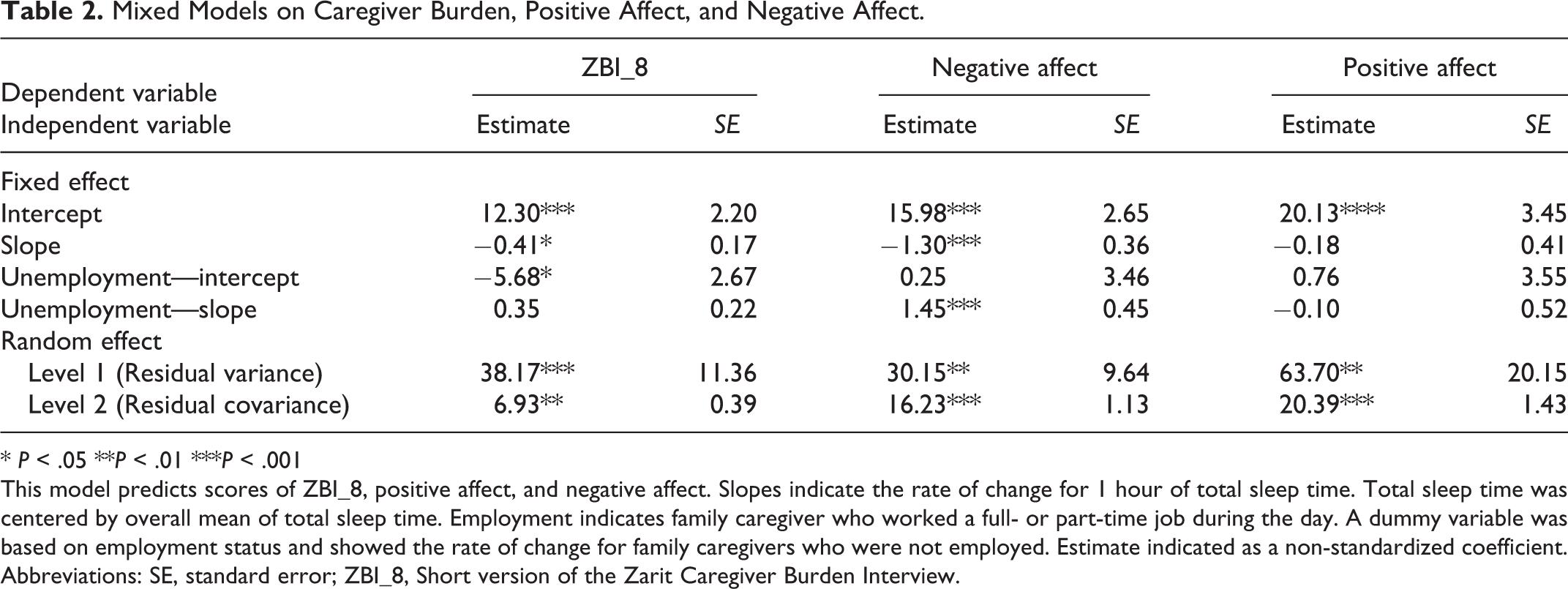
* P < .05 **P < .01 ***P < .001
This model predicts scores of ZBI_8, positive affect, and negative affect. Slopes indicate the rate of change for 1 hour of total sleep time. Total sleep time was centered by overall mean of total sleep time. Employment indicates family caregiver who worked a full- or part-time job during the day. A dummy variable was based on employment status and showed the rate of change for family caregivers who were not employed. Estimate indicated as a non-standardized coefficient.
Abbreviations: SE, standard error; ZBI_8, Short version of the Zarit Caregiver Burden Interview.
Discussion
The purpose of this study was to examine the effect of employment status on objective sleep, care burden, and negative affect among FCs at home. This study showed the intensive longitudinal effect of objective sleep status from the previous day measured at multiple points, between 14 and 56 days, on care burden and negative affect, as moderated by FCs’ employment status. It found that a more severe care burden was significantly associated with poorer TST, as objectively measured. This is consistent with our cross-sectional results at baseline. 9 Additionally, to the best of our knowledge, this study was the first to demonstrate that a reduction in TST could lead to more severe negative affect for FCs the following day, which might be moderated by employment status. The use of the intensive longitudinal method allowed novel associations to be determined; the findings imply it would be important for FCs who work to sleep and get enough rest at night.
A few nights of actigraphy may not be representative of habitual sleep status for FCs. Notably, this study used data covering 14 to 56 days of actigraphy to objectively measure sleep, while previous studies that reported no significant correlations between sleep and physical/psychological conditions often based their sleep measurements on a few nights of actigraphy or self-report.1,3,4,6,8,29 Sleep parameters in this study also considered sleep variability, as sleep for FCs might be affected by not only unexpected nighttime care involving, for example, tending to CRs’ behavioral and psychological symptoms of dementia, but also various daytime incidents such as FCs’ overtime work and CRs’ physical condition. This study thus considered the day-to-day variability of sleep, care burden, and negative affect, and inter-individual differences in intra-individual changes were taken into account.
However, in this study, no significant association was found between positive affect and objective and subjective sleep status. Positive affect of FCs in this study might have been influenced by factors other than home care. One previous longitudinal study has suggested that positive affect has stronger associations with subjective sleep measured by the PSQI than with objective sleep measured by actigraphy. 8 On the other hand, this study did not collect subjective sleep data longitudinally. Therefore, the current study clarifies that a longer sleep time does not necessarily increase positive affect, but whether positive feelings toward sleep quality enhance positive affect remains unclear.
A novel finding of the current study was that employment status of FCs moderated the association between TST, care burden, and negative affect, as few previous studies have considered FCs’ employment status. 6 The social background of FCs who take care of relatives at home is diverse, and it may be that many FCs worked more, thus shortening their sleep hours. Although we did not collect information on type of employment or when and how long FCs worked, this study suggests the importance of providing support for FCs who work while caring for a relative at home.
Despite its novel approaches, this study had several limitations. First, the sample size was small, so the findings may not be generalizable to larger populations even though 25 FCs were able to participate in at least 2 consecutive weeks of the survey. During the longitudinal study that the current study was a part of, some CRs in the study area were hospitalized after participating in the study and had subsequently died at follow-up of 3, 6 months later; therefore, it was difficult to increase the sample size. 9 Additionally, 32% of FCs (i.e., fewer than 10 participants) were employed; this might lead the results to seem more impactful than they actually are. Furthermore, it was difficult to adjust for other confounding factors in the mixed models, and we could not perform a stratified analysis based on the family relationships between the FCs and CRs and the FCs’ working hours. All FCs who were employed were children of the CRs; therefore, differences in family relationships might be related to our results of the influence of employment status on care burden and negative affect. In fact, the differences among FCs’ working hours per day, working days per week, and duration of current work could not be adjusted for in the mixed model because of the small sample size. Differences in the influence of employment status on care burden might depend on the amount of working hours per week and working days per month; therefore, taking these data into consideration would help determine whether the results can be generalized. Additionally, differences in the number of follow-up times per individual may have influenced the results. Second, the test for the level-1 residual variance suggested the existence of additional outcome variation at level-1, which may have been predictable. To explain some of this remaining within-person variation, we might add suitable time-varying predictors, such as working time, amount of nighttime care, or amount of FC-CR interaction, to the level-1 sub-model. Additionally, level-2 residual covariance indicated that the intercepts and slopes of individual true change trajectories were correlated; thus, we could not clarify several associations between true initial TST and true annual rate of change after controlling for the effect of employment status. Third, there were age differences between employed and unemployed FCs (unemployed FCs were older), although the TST of FCs 65 years old or younger was not significantly associated with ZBI_8 or positive or negative affect scores (Supplemental Table 2). An age difference could indicate differences in family relationships between FCs and CRs; therefore, it is necessary to adjust for this factor in this study model in the future. Fourth, our study investigated only TST and total time in bed, but FCs did not rest only during sleep. No other sleep parameters could be collected in this study because ActiGraph cannot measure sleep quality, as opposed to polysomnography; therefore, simply stating that FCs who work should sleep at night may not be enough for them to actually rest. Further study is needed to investigate not only objective sleep parameters but also how rest and use of care services can reduce care burden and negative affect. Finally, it is necessary to consider nighttime behavioral and psychological symptoms of dementia (BPSD) for CRs, because CRs’ BPSD would likely be the most distressing for FCs.4,30 Previous studies have taken dementia into consideration to analyze the association between care burden and sleep for FCs, whereas this study did not.3,5,6,8,13,14 Although approximately half of the CRs in the current study were diagnosed with dementia, and it collected data on care levels of CRs that considered the severity and symptoms of dementia according to the criteria of the public long-term care insurance policy, it is necessary to assess the severity of dementia and nighttime needs of CRs in future research.
In conclusion, a reduction in TST could lead to increased care burden and more severe negative affect the following day for FCs, which may be moderated by employment status. For FCs and CRs to continue living at home, it is important to provide formal and informal support that takes into account nighttime sleep status and employment status of FCs.
Supplemental Material
Supplemental Material, sj-pdf-1-jgp-10.1177_0891988720957099 - Effect of Employment Status on the Association Among Sleep, Care Burden, and Negative Affect in Family Caregivers
Supplemental Material, sj-pdf-1-jgp-10.1177_0891988720957099 for Effect of Employment Status on the Association Among Sleep, Care Burden, and Negative Affect in Family Caregivers by Hirochika Ryuno, Yuko Yamaguchi and Chieko Greiner in Journal of Geriatric Psychiatry and Neurology
Supplemental Material
Supplemental Material, sj-pdf-2-jgp-10.1177_0891988720957099 - Effect of Employment Status on the Association Among Sleep, Care Burden, and Negative Affect in Family Caregivers
Supplemental Material, sj-pdf-2-jgp-10.1177_0891988720957099 for Effect of Employment Status on the Association Among Sleep, Care Burden, and Negative Affect in Family Caregivers by Hirochika Ryuno, Yuko Yamaguchi and Chieko Greiner in Journal of Geriatric Psychiatry and Neurology
Footnotes
Authors’ Note
H. Ryuno designed the study, collected the data, analyzed the data, and wrote the paper. C. Greiner and Y. Yamaguchi helped design the study, supervised data analysis, and assisted with writing the article.
Acknowledgments
We gratefully thank all staff involved in the survey, especially vice manager Hitoshi Iguchi and head nurse Hisayo Uemura at the Social Welfare Corporation, and Ho-yu Fukushikai Syownkan for field management and sampling the participants. We also thank Prof. Kei Kamide and Dr. Mai Kabayama at the Osaka University Graduate School of Medicine for the analysis of data, Dr. Hirokazu Fujimoto at the Hyogo University of Health Sciences for designing this study and for assisting with data interpretation, Ms. Misato Hirota at the Kobe University Graduate School of Health Sciences for designing this study, and librarian Noriaki Akai at the Osaka University Life Sciences Library for the literature review. We sincerely appreciate all participants for their kind cooperation. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported, in part, by grants-in-aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan (RH: 18K17603 and 16H06975), and the Pfizer Health Care Research Foundation (to RH).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.