
Abstract
Objective:
The efficacy of antidepressants in post-stroke depressive symptoms (PSD) varies. We aimed to examine whether the effect of escitalopram on PSD differs according to individual depressive symptoms and stroke lesion location.
Methods:
This is a post hoc analysis of EMOTION (ClinicalTrials.gov, NCT01278498), a randomized, placebo-controlled, double-blind trial that examined the efficacy of escitalopram on depression in acute stroke patients (237 with placebo, 241 with escitalopram). Depressive symptoms were evaluated with the 10-item Montgomery-Åsberg Depression Rating Scale (MADRS). Changes in MADRS and individual item scores at 12 weeks were compared between the treatment groups and among the stroke lesion location groups. Stroke lesion locations were grouped according to the anatomical distribution of serotonin fibers that originate from the midbrain/pons and spread to the forebrain via subcortical structures: “Midbrain-Pons,” “Frontal-Subcortical,” and “Others.” Least-squares means were calculated to demonstrate the independent effect of lesion location.
Results:
Total MADRS scores decreased more significantly in the escitalopram than in the placebo group, while a significant effect of escitalopram was observed in only 3 items: apparent sadness, reported sadness, pessimistic thoughts. In the lesion location analyses, escitalopram users in the Frontal-Subcortical group showed significant improvement in total MADRS scores (placebo [n = 130] vs. escitalopram [n = 148], least-square mean [95% CI]: -2.3 [-3.5 to -0.2] vs. -4.5 [-5.5 to -3.4], p = .005), while those in the Midbrain-Pons and Others groups did not.
Conclusions:
The effect of escitalopram on PSD may be more prominent in patients with particular depressive symptoms and stroke lesion locations, suggesting the need for tailored treatment strategies.
Keywords
Introduction
Post-stroke depressive symptoms (PSD) are common, and worsens the clinical outcome. 1 However, the effect of pharmacological treatment is often unsatisfactory or heterogeneous.2-6 This may be ascribed to heterogeneous mechanisms of PSD. 2 PSD may in part due to damages on neurotransmitter fibers that project from the brainstem to the frontal cortex, so-called the “frontal subcortical circuits.”7-9 Thus, the pharmacological therapy such as selective serotonin reuptake inhibitors (SSRIs) may vary according to the lesion location.
In addition, the varying therapeutic responses may be attributed to inappropriateness of diagnostic tools used in stroke patients. Most tools assessing PSD are for psychiatric patients without structural brain damage, and include symptoms such as fatigue, sleep disturbances or concentration difficulty. In acute stroke patients, such symptoms may be secondary to neurological disturbances, changes in environment or medications. Thus, patients with predominant symptoms on these dimensions may be less responsive to antidepressants.
In this study, we hypothesized that the effect of SSRIs varies according to neurobehavioral symptom dimensions and stroke lesion locations. To examine this hypothesis, we performed a post-hoc analysis of our recent clinical trial with escitalopram, which investigated stroke lesion locations and multiple dimensions of depressive symptoms in acute stroke patients.
Methods
Study Design
This is a post hoc analysis of our randomized, double-blind, placebo-controlled, multicenter (17 university hospitals) clinical trial, EMOTION (ClinicalTrials.gov, NCT01278498), 10 conducted between 2011 and 2014. Patients received either an escitalopram (10 mg/day per os) or a placebo for 12 weeks and were followed up for additional 12 weeks without study medications.
We included patients who were older than 20 years, had experienced an acute stroke within 21 days (confirmed by MRI or CT), had a neurologic deficit with modified Rankin score ≥2, and provided an informed consent. Meanwhile, we excluded patients who had a history of diagnosed depression or other psychiatric disorders prior to the index stroke; those who had altered mental status, severe dementia, 11 and/or aphasia resulting in communication difficulties. Patients with the presence of depression symptoms during screening were not excluded, but those who exhibited strong suicidal thoughts were excluded. The initial assessment was conducted when the neurological condition became stabilized after the onset of stroke (typically ≥3 days after onset). Patients with aphasia were included if the symptoms improved so that they could communicate. Further detailed study criteria are provided in the Table S1. 10
All participants were directed to take 5 mg escitalopram or placebo daily as a starting dose, which was subsequently increased to 10 mg daily from the second week in case of no adverse events. The placebo was identical in shape and color to escitalopram over the trial. Compliance to the study medications was closely monitored. At each study visit, participants were instructed to return all remaining drugs.
The study was conducted according to Good Clinical Practice guidelines and the Declaration of Helsinki and was approved by the institutional review boards of the respective hospitals. Informed consent was obtained from all participants.
Assessments
PSD was evaluated using the Montgomery-Åsberg Depression Rating Scale (MADRS), comprised of 10 symptom items (apparent sadness, reported sadness, inner tension, reduced sleep, reduced appetite, concentration difficulties, lassitude, inability to feel, pessimistic thoughts, and suicidal thoughts). We used MADRS because its score mostly reflects mood but not physical disturbances in patients with neurological deficits 12 and it is considered a sensitive tool for assessing pharmacological effects on depressive symptoms. 13 Each item yields a score of 0–6 with higher scores indicating more severe depression. 12 In the current analysis, we evaluated baseline and 12-week MADRS scores to differentiate the effect of escitalopram during the actual treatment. Neurological deficits were evaluated with the National Institute of Health Stroke Scale (NIHSS). 14 For patients who did not complete the study or had missing data, we used the latest available records for analysis.
Lesion Location
Stroke lesion locations were confirmed by MRI or CT. 10 The imaging studies were performed in accordance with the protocols of each local participating center. The presence and location (frontal, parietal, temporal, occipital, subcortex [corona radiata/internal capsule/basal ganglia], thalamus, midbrain, pons, medulla and cerebellum) of a stroke lesion was determined by consensus between the attending stroke neurologist and neuroradiologist at each center.
Serotonin neurons in the brainstem can be grouped as follows. 15 The rostral group contains most serotonergic neurons (∼85%) densely packed in the midbrain (dorsal raphe nucleus) and pons (median raphe nucleus). Ascending axons widely spread to the forebrain via subcortical structures. 15 The caudal group (∼15%), located in the caudal pons and medulla oblongata, sprouts descending axons to the spinal cord. 15 Functionally, the rostral group is mainly related to mood regulation, 16 while the caudal group is mostly involved in pain control. 16 We therefore re-classified the lesion locations into 3 mutually exclusive groups: “Midbrain-Pons” (lesions in the midbrain or pons), “Frontal-Subcortical” (lesions in the frontal cortex or subcortex [corona radiata/internal capsule/basal ganglia]), and “Others.” Patients who had multiple lesions in multiple locational categories (n = 5) were not included in lesion location analysis.
Statistical Analyses
Analyses were performed on an intention-to-treat basis. Changes in total MADRS scores 17 and in each symptom item score from baseline to 12 weeks were evaluated as outcome variables. Baseline characteristics and clinical variables were compared between the treatment groups and among the 3 location groups using Chi-square tests (or Fisher’s exact tests) for categorical variables and Student’s t-tests (or Mann-Whitney U tests) or 1-way analysis of variance for continuous variables. The effect of escitalopram on the main outcome (changes in total MADRS scores at 12 weeks) were examined with multiple variable linear regression, along with other potential contributors such as age, sex, side of brain lesions, and the size of lesions (≥ 2 cm in diameter). Outcome variables examining differences in the effect of escitalopram among the location groups were evaluated using analysis of covariance. Because the location groups were defined in a post hoc manner, we further adjusted changes in outcome variables for 1) age and baseline neurologic deficits (NIHSS), important contributors to the neurologic functional outcome 18 and 2) variables that showed significant imbalances (p < 0.05) in baseline characteristics. Least-squares means for each location group were calculated to show the magnitude of the independent effect of lesion location on changes in depressive symptoms. Two-tailed p-values < 0.05 were considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., USA).
Data Availability
The authors are willing to provide the anonymized data related to this work upon reasonable request.
Results
A total of 478 patients (456 with ischemic stroke, 22 with hemorrhagic stroke) were included. Baseline variables were balanced between the escitalopram and placebo groups (Table 1). Of them, 353 (73.8%) underwent 12-week evaluations with MADRS scores (Figure 1); the numbers of patients lost during this period were comparable between the treatment groups (65 with placebo and 60 with escitalopram). The study medication was generally well tolerated 10 ; adherence to study medications during the trial was comparable between the 2 groups (placebo vs. escitalopram, 86.3% vs. 89.3%, p = 0.176).
Baseline Characteristics of the Participants (Intention-to-Treat).
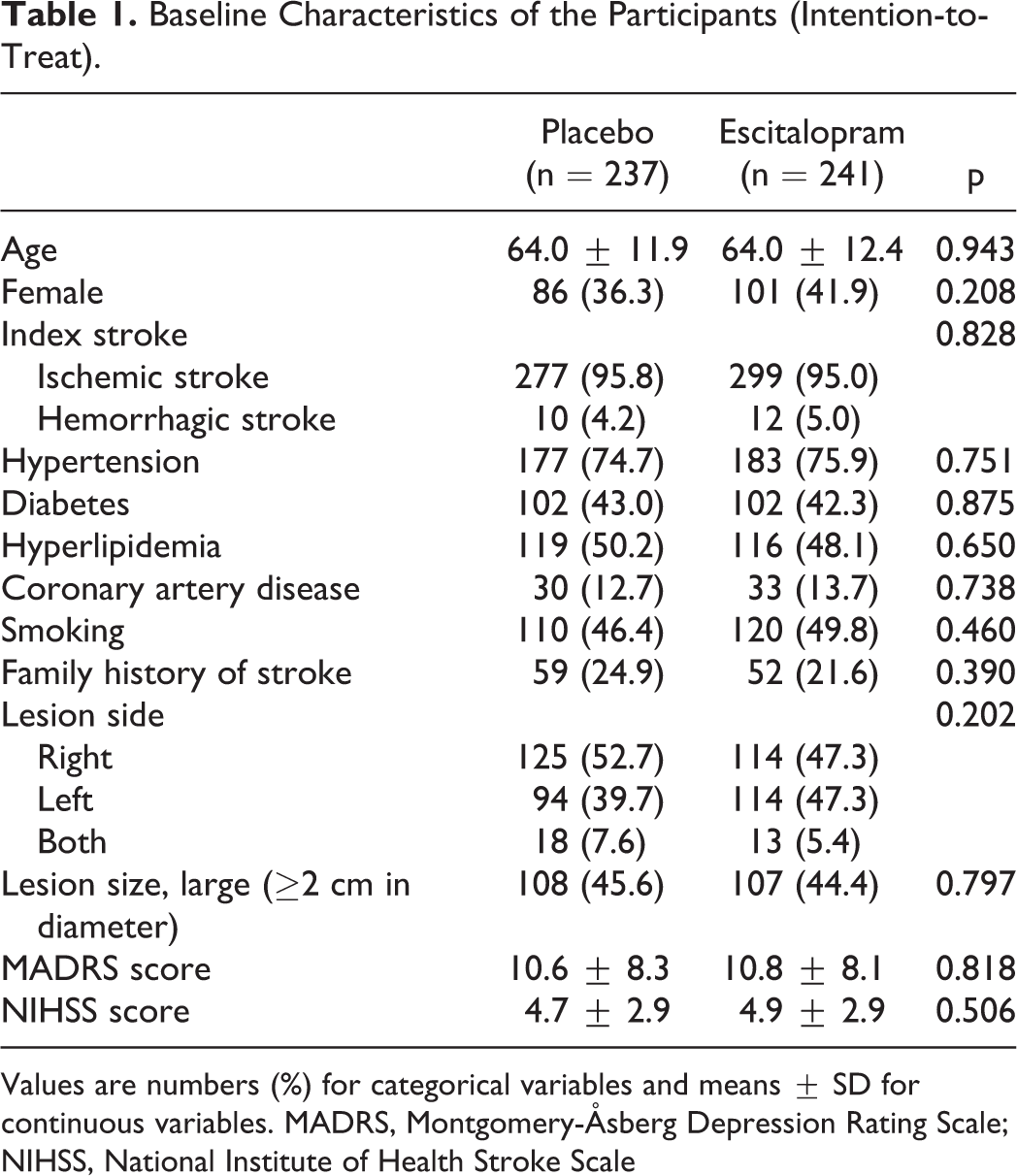
Values are numbers (%) for categorical variables and means ± SD for continuous variables. MADRS, Montgomery-Åsberg Depression Rating Scale; NIHSS, National Institute of Health Stroke Scale
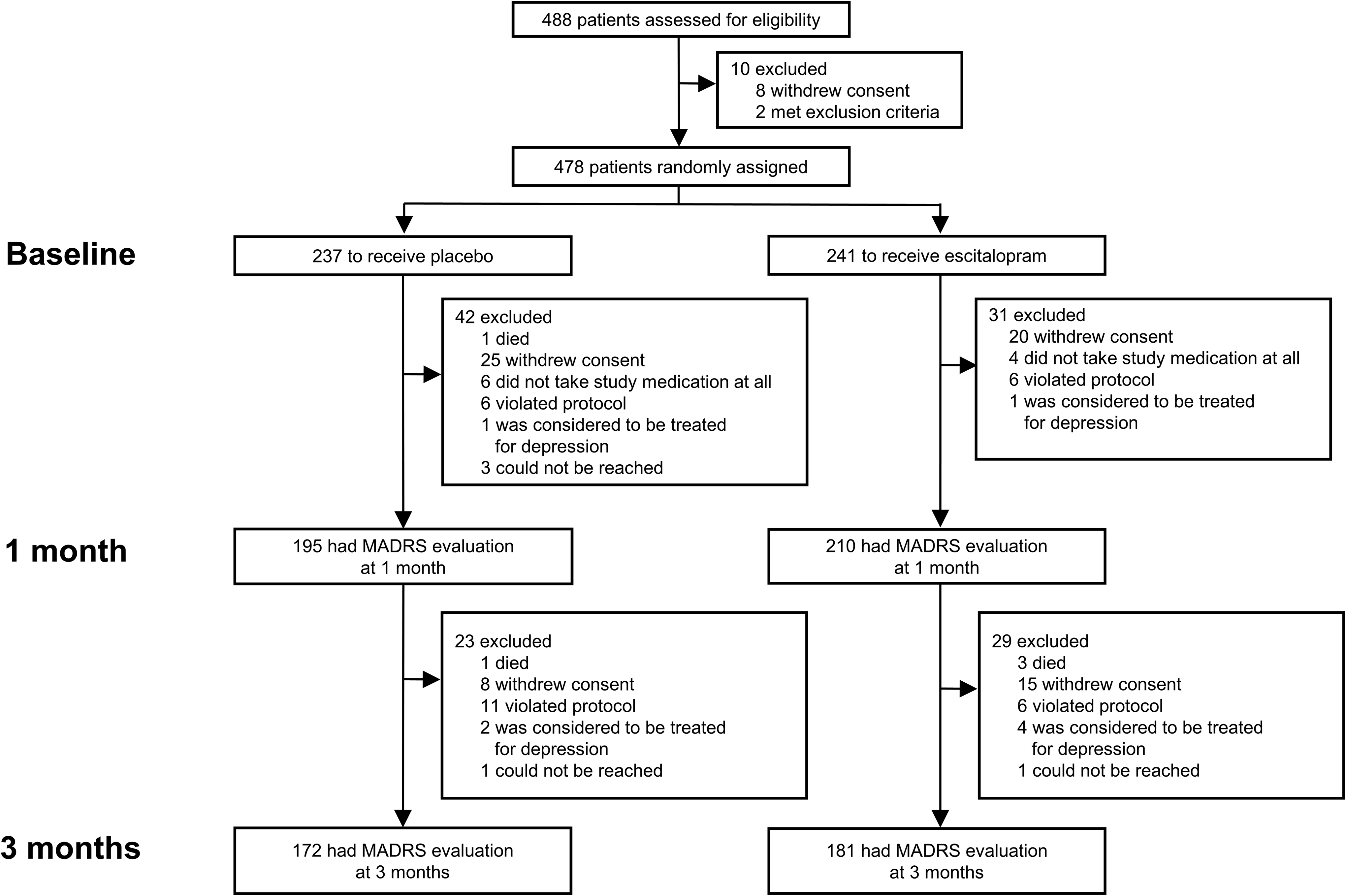
Study profile.
Baseline severity of depressive symptoms (MADRS, placebo vs. escitalopram, 10.6 ± 8.3 vs. 10.8 ± 8.1, p = 0.818) and neurological deficits (NIHSS, 4.7 ± 2.9 vs. 4.9 ± 2.9, p = 0.506) were similar between the 2 groups. As neurologic deficits lessened over time, depressive symptoms became alleviated; this change in total MADRS score was significantly greater in the escitalopram group (Table 2 and Figure 2). The effect of escitalopram on changes in total MADRS score was significant (β = -1.194, p = 0.044), even after the adjustment of several other potential contributors such as age, sex, the side and size of brain lesions (Table S2). Among the individual symptom items, 3 item scores (apparent sadness, reported sadness, and pessimistic thoughts) significantly improved in the escitalopram group, while other symptoms did not (Figure 3).
Changes in Total MADRS Score and Individual Symptom Item Score at 12 Weeks.
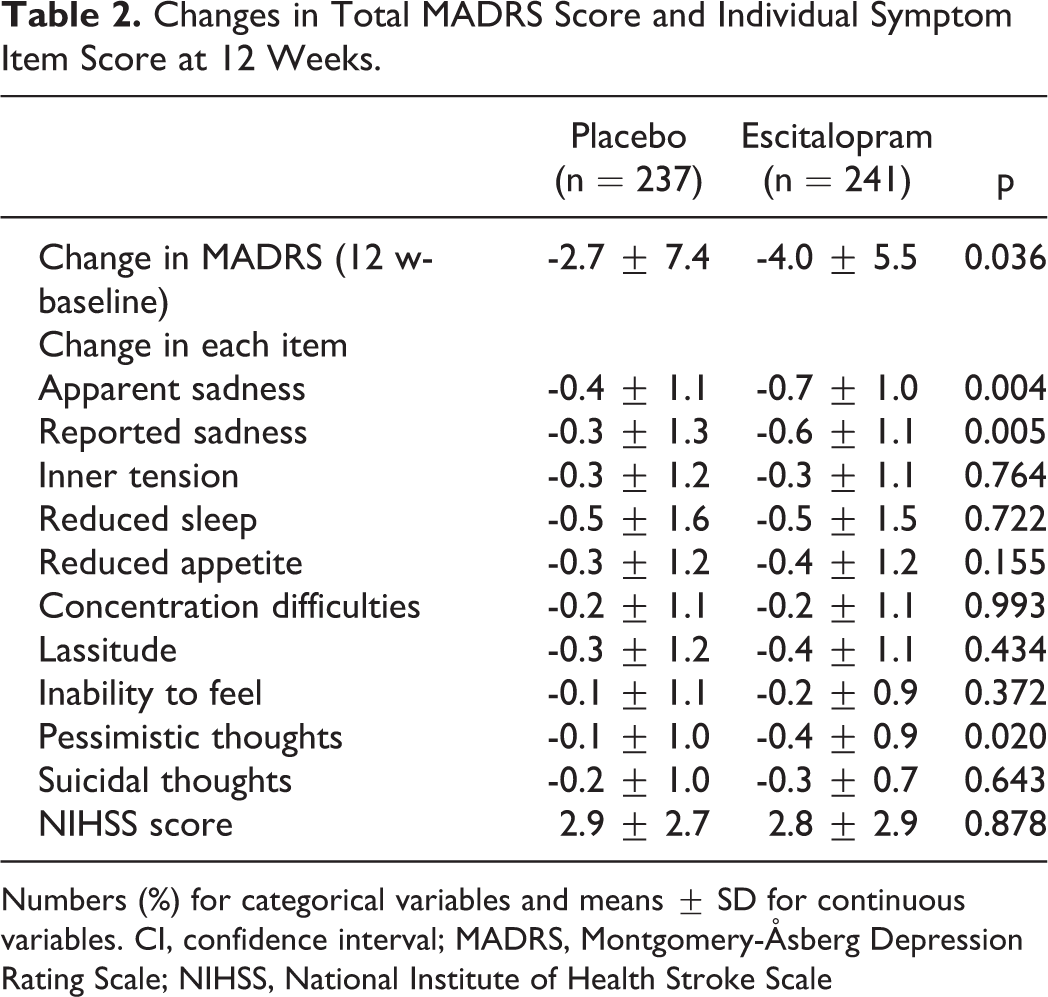
Numbers (%) for categorical variables and means ± SD for continuous variables. CI, confidence interval; MADRS, Montgomery-Åsberg Depression Rating Scale; NIHSS, National Institute of Health Stroke Scale
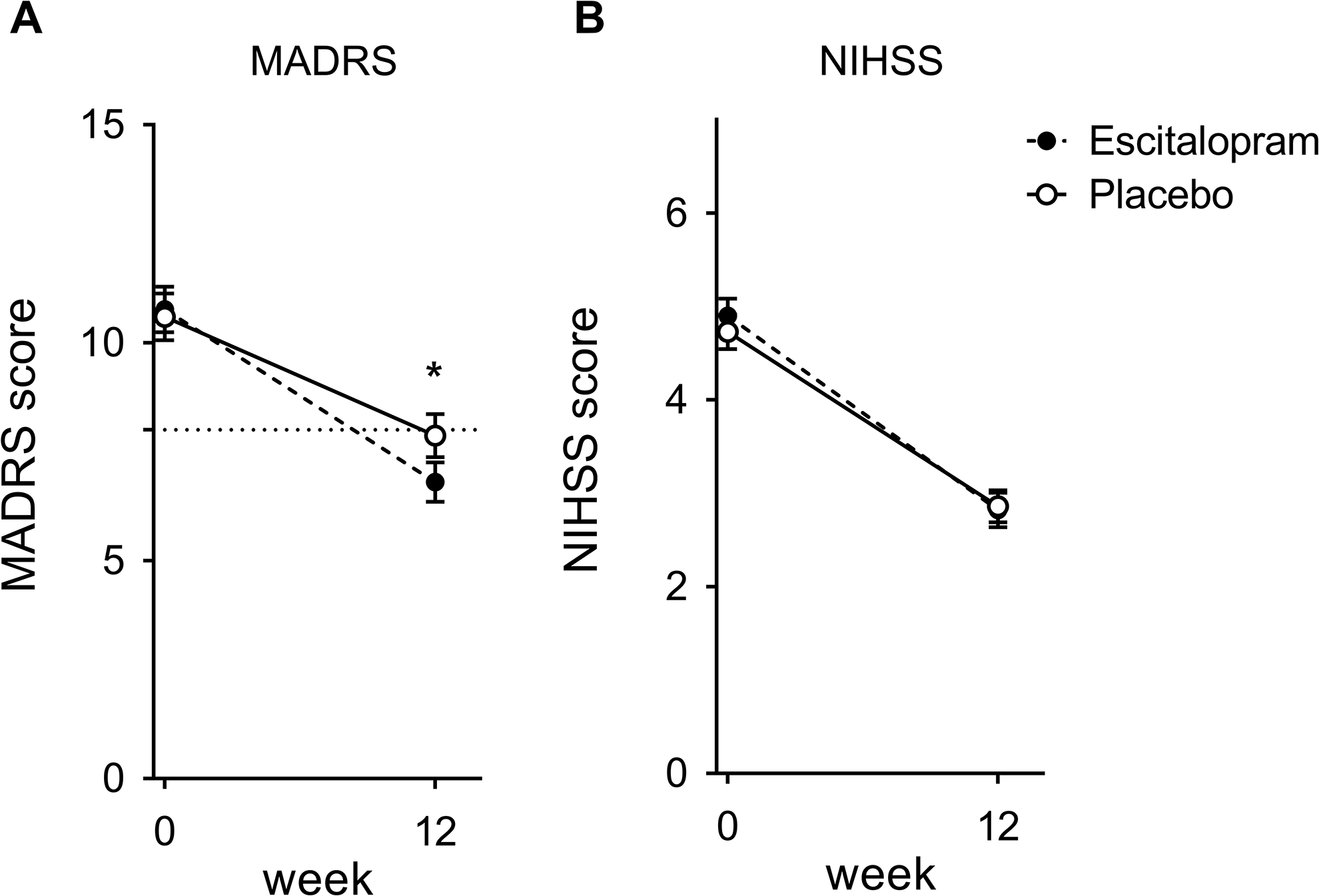
Depressive symptoms and neurologic deficit over time. (A) Total MADRS score and (B) NIHSS score (mean with bars indicating standard error). NIHSS, National Institute of Health Stroke Scale; MADRS, Montgomery-Åsberg Depression Rating Scale. * P < 0.05 by comparison of score changes from baseline between the treatments.
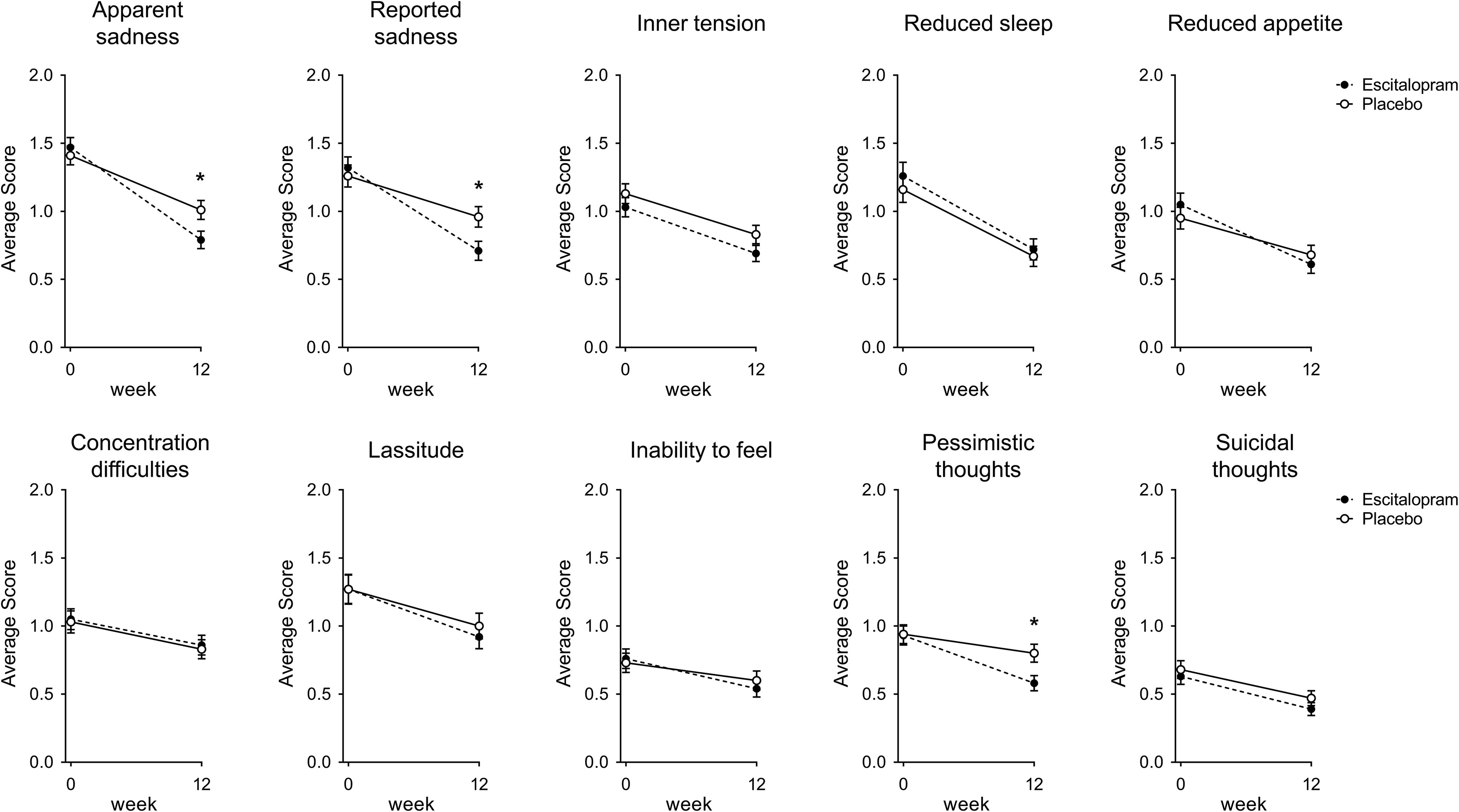
Each depressive symptom item over time (mean with bars indicating standard error). MADRS, Montgomery-Åsberg Depression Rating Scale, * p < 0.05, by comparison of score changes from baseline between the treatments.
Among the patients included in the lesion location analysis (n = 473), 101 had lesions in the midbrain/pons (Midbrain-Pons group), and 278 had lesions in the frontal cortex or internal capsule/corona radiata/basal ganglia (Frontal-Subcortical group) (Table 3). The Midbrain-Pons and Frontal-Subcortical group patients had more severe neurologic deficits (NIHSS) than the Others group patients both at baseline and at 12 weeks.
Clinical Characteristics According to Lesion Location.
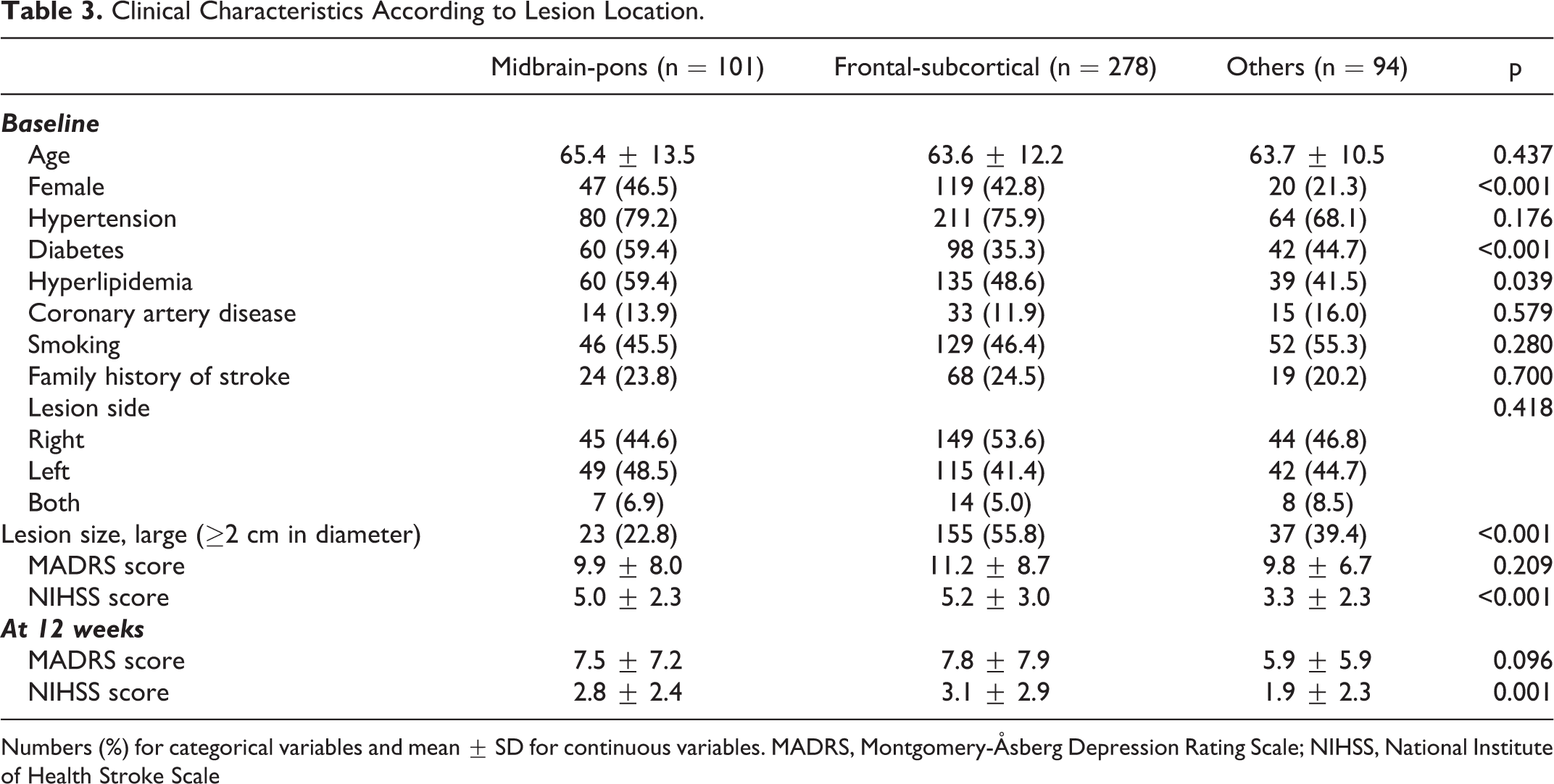
Numbers (%) for categorical variables and mean ± SD for continuous variables. MADRS, Montgomery-Åsberg Depression Rating Scale; NIHSS, National Institute of Health Stroke Scale
In an unadjusted analysis, the effect of escitalopram appears to be most pronounced in the Frontal-Subcortical group, especially for apparent sadness, reported sadness, and pessimistic thoughts (Figure 4, Table S3). After adjustment for the variables showing significant group differences at baseline (sex, diabetes, hyperlipidemia, and the size of lesion) (Table 3) as well as other essential variables (age and baseline NIHSS), we found that escitalopram improved depressive symptoms only in the Frontal-Subcortical group ( Table 4 ). However, the effect of escitalopram did not show significant interactions with the location groups.
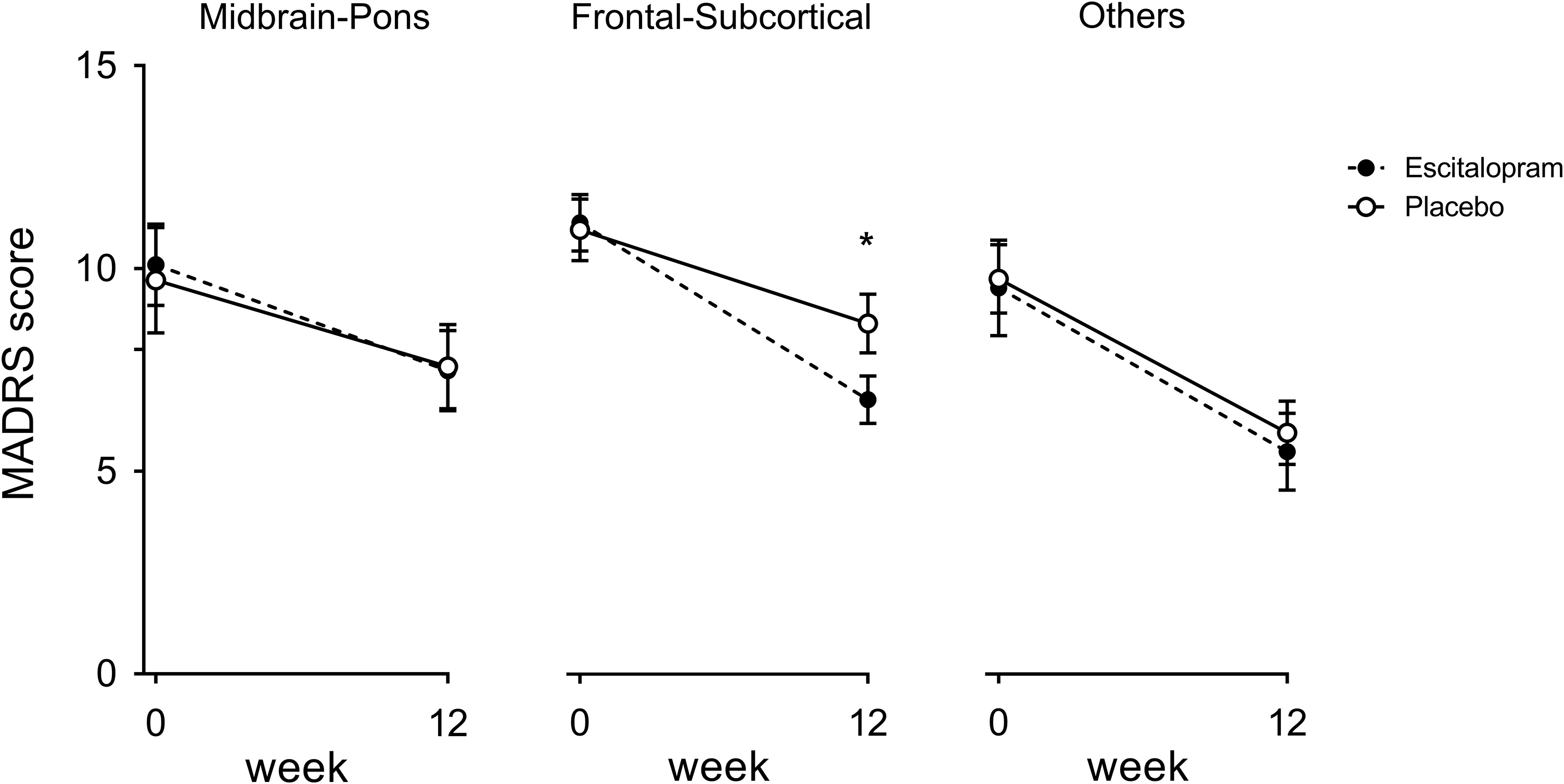
Depressive symptoms according to lesion location group over time (mean with bars indicating standard error). MADRS, Montgomery-Åsberg Depression Rating Scale, * p < 0.05 by comparison of score changes from baseline between the treatments.
Changes in MADRS Score and Its Components at 12 Weeks (Adjusted Analysis).
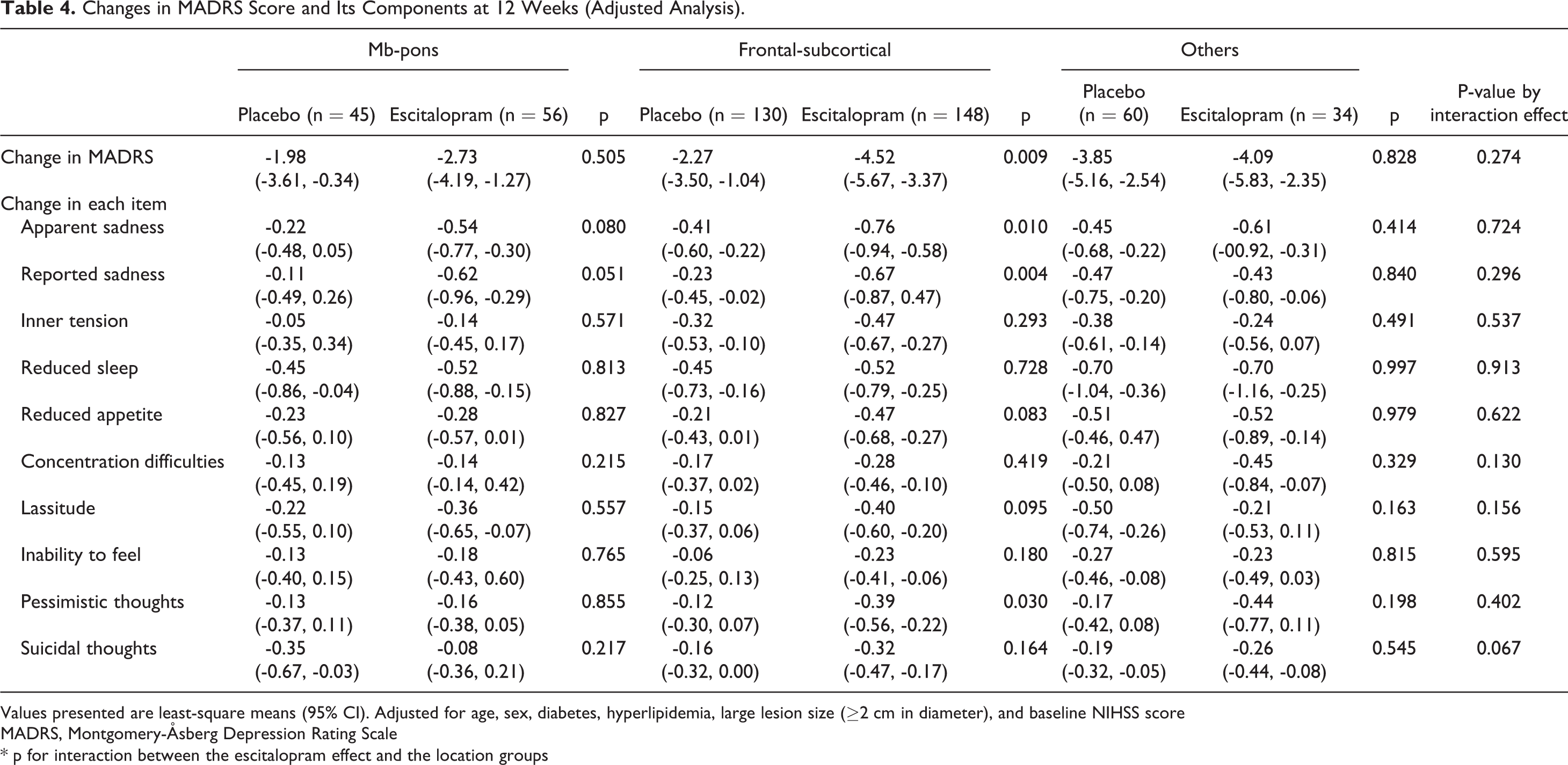
Values presented are least-square means (95% CI). Adjusted for age, sex, diabetes, hyperlipidemia, large lesion size (≥2 cm in diameter), and baseline NIHSS score
MADRS, Montgomery-Åsberg Depression Rating Scale
* p for interaction between the escitalopram effect and the location groups
Discussion
In this study, we demonstrated that pharmacological effect for PSD differed based on individual depression symptoms and lesion locations, which have not been considered previously in determining pharmacological efficacy for PSD. We found that escitalopram significantly improved apparent sadness, reported sadness, and pessimistic thoughts, which have been categorized as “depression dimension” symptoms. 19 In contrast, symptoms on other dimensions 19 including cognitive (concentration difficulties) and neurovegetative (reduced sleep, reduced appetite, and lassitude) symptom dimensions did not improve. This may be because participants in this study had acute stroke; symptoms of cognitive or neurovegetative dimensions may be partly caused by stroke and its related factors (e.g., changes in environment, medications), thus may have been less responsive to escitalopram. Considering a higher frequency of vegetative symptoms in early-onset than late-onset PSD, 20 our findings suggest that using tools that include vegetative symptoms in the assessment of PSD may underestimate treatment responses of antidepressants in patients with acute stroke.
Alternatively, SSRIs may inherently be more effective on symptoms of certain dimensions. A study showed that escitalopram more effectively reduced depression dimension symptoms, whereas nortriptyline improved neurovegetative symptoms in patients with major depression. 21 Meanwhile, another study demonstrated that although duloxetine more effectively improved core emotional symptoms (sad mood, feelings of worthlessness, and loss of interest) than other symptoms, escitalopram did not. 22 Because we used only escitalopram, further researches with other antidepressants are needed to elucidate inherent differences in pharmacological effects on each depression symptom.
We hypothesized that the effect of SSRIs differs according to the presence of lesions affecting brainstem-subcortical-frontal regions, alleged areas of abundant serotonin fibers. Indeed, the Others group patients did not show responsiveness to escitalopram, although they demonstrated comparable alleviation in depressive symptoms regardless of escitalopram use, as neurologic deficits improved over time. Interestingly, significant pharmacological responsiveness was shown in the Frontal-Subcortical group patients, but not in the Midbrain-Pons group patients. One possible explanation for this discrepancy would be the different density of serotonergic fibers. Intact serotonergic axon terminals are indispensable for SSRI action. 23 The brainstem contains raphe nuclei and densely packed ascending serotonergic fibers, whereas the axonal fibers widely fan out in the frontal-subcortical areas. Therefore, the degree and number of damaged serotonin fibers may be different between these 2 groups, which may have resulted in varying therapeutic responses to SSRIs. Alternatively, this may be related to the receptor-medicated feedback system. 24 Glutaminergic projections from the medial prefrontal cortex to the brainstem raphe nuclei preferentially target gamma-aminobutyric acid neurons and inhibit serotonin neuronal firing in the raphe nuclei, which may explain the lack of early responses to SSRIs in patients with depression.25-27 Therefore, the damage to projection (i.e., cortex and basal ganglia) areas may dis-inhibit such a feedback system, thereby increasing the degree of SSRI effect. 28
Our study has several limitations. First, although we hypothesized that escitalopram effect varies according to lesion location affecting serotonergic fibers, the categorization of lesions was based on MRI findings, but not on the actual distribution of serotonergic fibers. Future studies using positron emission tomography (PET) or other advanced imaging tools that identify real serotonergic fibers may yield more definitive conclusions. However, our observation may still be of clinical relevance because physicians practically use MRI, but not PET in the assessment of stroke patients. Second, stroke lesions can affect neurotransmitters (e.g., dopamine and norepinephrine) other than serotonin, contributing to depressive symptoms. 29 However, our study focused on the effect of escitalopram, a pure serotonin reuptake inhibitor; therefore, we emphasized serotonin fiber disruption while discussing our results. Third, a number of potential predictors/moderators of PSD was not considered in this analysis, such as medication information other than escitalopram, quality of life scores, social habits (e.g., addiction and alcohol consumption) and concomitant psychological distress, neurotrophin (e.g., brain-derived neurotrophic factors) and neuroinflammatory cytokines (e.g., interleukin-6). 29 In addition, data for familial/social support that may be associated with PSD development had not been obtained. However, this familial/social support factor seems to be more important in the pathogenesis of depression in the chronic stage of stroke, 30 whereas we focused on patients with acute or subacute stroke. Fourth, we uniformly administered escitalopram 10 mg/day, thus different doses or types of antidepressants remain to be studied. Fifth, missing values of depressive symptoms (MADRS) at 12 weeks were replaced by the last-observation-carried-forward imputation method, which is commonly used in clinical trials with antidepressants. 31 However, this method is prone to bias, and may be conservative for evaluating the treatment efficacy.32,33 Although the numbers of patients lost during follow up were similar between the treatment groups, biases introduced by the imputation should be considered. Sixth, multiple-comparison issues should be addressed. Because we have included numerous outcome variables, alpha values may have increased. Our results should be cautiously interpreted, and regarded as an observational evidence. However, it should be noted that we did not employ depression scoring systems other than MADRS scores, or a newly generated composite score to promote statistically positive results. Previous studies in other groups have also performed an analysis of sub-dimensions or components of depressive symptom scores (e.g., MADRS score) to screen the differential efficacy of antidepressants.19,21 Finally, the lack of statistically significant interactions of locational analysis results should be noted, which might be due to the relatively small number of participants in each group.
Despite these limitations, we show that the pharmacological effect for PSD varies according to individual depressive symptoms and lesion locations. Future clinical trials should consider varying pharmacological efficacy according to different symptom dimensions and different lesion locations. For example, higher doses of SSRIs may be tested in patients with brainstem stroke. Such tailored treatment strategies may be helpful to maximize the therapeutic efficacy for PSD.
Supplemental Material
Supplemental Material, ms_change_tracking - Post-Stroke Depressive Symptoms: Varying Responses to Escitalopram by Individual Symptoms and Lesion Location
Supplemental Material, ms_change_tracking for Post-Stroke Depressive Symptoms: Varying Responses to Escitalopram by Individual Symptoms and Lesion Location by Eun-Jae Lee, Jong S. Kim, Dae-Il Chang, Jong-Ho Park, Seong Hwan Ahn, Jae-Kwan Cha, Ji Hoe Heo, Sung-Il Sohn, Byung-Chul Lee, Dong-Eog Kim, Hahn Young Kim, Seongheon Kim, Do-Young Kwon, Jei Kim, Woo-Keun Seo, Jun Lee, Sang-Won Park, Seong-Ho Koh, Jin Young Kim, Smi Choi-Kwon, Min-Sun Kim and Ji-Sung Lee in Journal of Geriatric Psychiatry and Neurology
Supplemental Material
Supplemental Material, supple_files - Post-Stroke Depressive Symptoms: Varying Responses to Escitalopram by Individual Symptoms and Lesion Location
Supplemental Material, supple_files for Post-Stroke Depressive Symptoms: Varying Responses to Escitalopram by Individual Symptoms and Lesion Location by Eun-Jae Lee, Jong S. Kim, Dae-Il Chang, Jong-Ho Park, Seong Hwan Ahn, Jae-Kwan Cha, Ji Hoe Heo, Sung-Il Sohn, Byung-Chul Lee, Dong-Eog Kim, Hahn Young Kim, Seongheon Kim, Do-Young Kwon, Jei Kim, Woo-Keun Seo, Jun Lee, Sang-Won Park, Seong-Ho Koh, Jin Young Kim, Smi Choi-Kwon, Min-Sun Kim and Ji-Sung Lee in Journal of Geriatric Psychiatry and Neurology
Footnotes
Authors’ Note
JSK contributed to study design, data collection and analysis, obtaining funding, manuscript preparation and study supervision. EJL contributed to manuscript preparation and statistical analysis. DIC, JHP, SHA, JKC, JHH, BCL, DEK, HYK, SK, JK, WKS, JL, SWP, SHK, and JYK participated in data collection, editing the manuscript, and interpretation of results. SC-K contributed to study design and interpretation of results. M-S Kim contributed to interpretation of results and manuscript preparation. J-S Lee participated in statistical analysis. All authors have read and approved the finalized manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jong S. Kim received grants from Dong-A Pharmaceutical, the Ministry for Health and Welfare, Korea (HI14C1985, HI18C2383), and Eun-Jae Lee received grants from the Ministry of Science and ICT (NRF-2018M3A9E8066249).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.