
Abstract
Introduction:
Electroconvulsive therapy (ECT) is commonly used in the elderly due to its proven efficacy and safety profile. However, presence of cardiovascular comorbidities such as cerebral aneurysms may complicate the course of treatment. Our knowledge about the possible risk factors and precautionary measures remains limited.
Methods:
We performed a systematic review of published case reports of elderly patients with cerebral aneurysms treated with ECT.
Results:
A total of 11 cases were included for the review. One patient died because of subarachnoid hemorrhage (SAH) secondary to ictal hypertensive surge during treatment with ECT.
Discussion:
Risk factors such as history of hypertension, age of the patient, extent of the ictal surge in blood pressure, efficacy of prophylactic treatment to control surge in blood pressure and characteristics of cerebral aneurysm each elevated the risk of complication in these cases. We reviewed safety measures based on the evidence from the current literature available.
Conclusion:
ECT is safe in elderly patients with cerebral aneurysms provided appropriate safety measures are employed. Screening for cerebral aneurysms in high risk patients, effective prevention and management of blood pressure elevation acutely during ECT is the best practice to avoid adverse outcomes.
Introduction
ECT is an effective treatment modality for severe and treatment-resistant affective disorders. 1 ECT has been increasingly utilized in the elderly population. As per the National Institute of Mental Health survey data, a third of patients receiving ECT were 65 years old or older. 1 ECT is a good alternative treatment for elderly patients with major depression who do not improve with antidepressant medications or cannot tolerate the medication-related side effects.1-4 There is growing evidence that ECT is safe and tolerable in elderly patients.2,4 A systematic review estimated an ECT-related mortality rate of 2.1 per 100,000 treatments. 5 However, this does not imply the universal safety of ECT in the elderly. The presence of cardiovascular comorbidities, such as cerebral aneurysms, presents a challenge due to concerns of a possible aneurysm rupture during ECT. 3 Rupture of an aneurysm is a catastrophic outcome. It is estimated that about 10% to 30% of patients with aneurysm rupture die before reaching the hospital. 6 Among those who survive the risk of another bleed remains significantly elevated. 6 The prevalence of cerebral aneurysm increases with age, 7 yet the literature on performing ECT in the presence of cerebral aneurysms remains sparse. It is suggested that older patients with cerebral aneurysms might have higher rates of adverse outcomes. 8 Several questions arise in this context:
How safe is it to perform ECT in elderly patients with a cerebral aneurysm?
Should elderly patients be routinely screened for cerebral aneurysms as part of medical clearance work up before ECT?
How can the risk of adverse outcomes during treatment be minimized?
In this article, we will review the relevant literature and address the above-mentioned concerns. We will also summarize the previously reported cases of ECT performed in elderly patients with a cerebral aneurysm to help increase our understanding of the topic.
Methods
We performed a literature search on PubMed, Google Scholar, and the Columbia University library search engine using the terms: “Electroconvulsive Therapy, ECT, cerebral aneurysm, brain aneurysm, vascular malformations and intracranial aneurysms.” Reference lists of the articles were also screened for any missed article. We included all articles with case reports of ECT performed in patients greater than 60 years old with a cerebral aneurysm. (Figure 1).
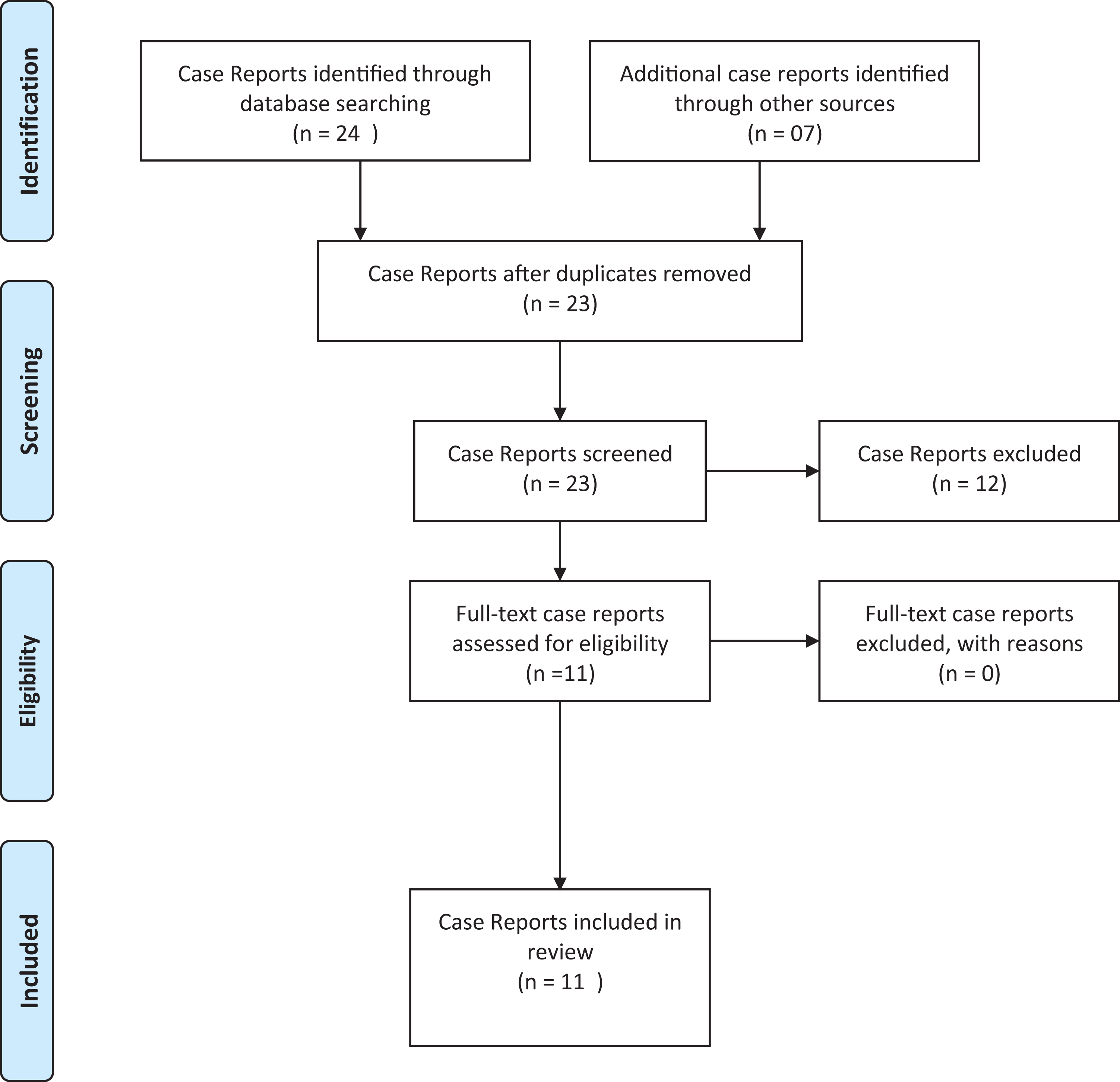
Prisma chart diagram. 9
Results
We identified a total of 31 case reports through database searching. After duplicate case reports were removed, we excluded case reports of patients less than 60 years old. Only case reports with full-text availability were included. Eleven case reports met the eligibility criteria and were included in the review (Table 1).
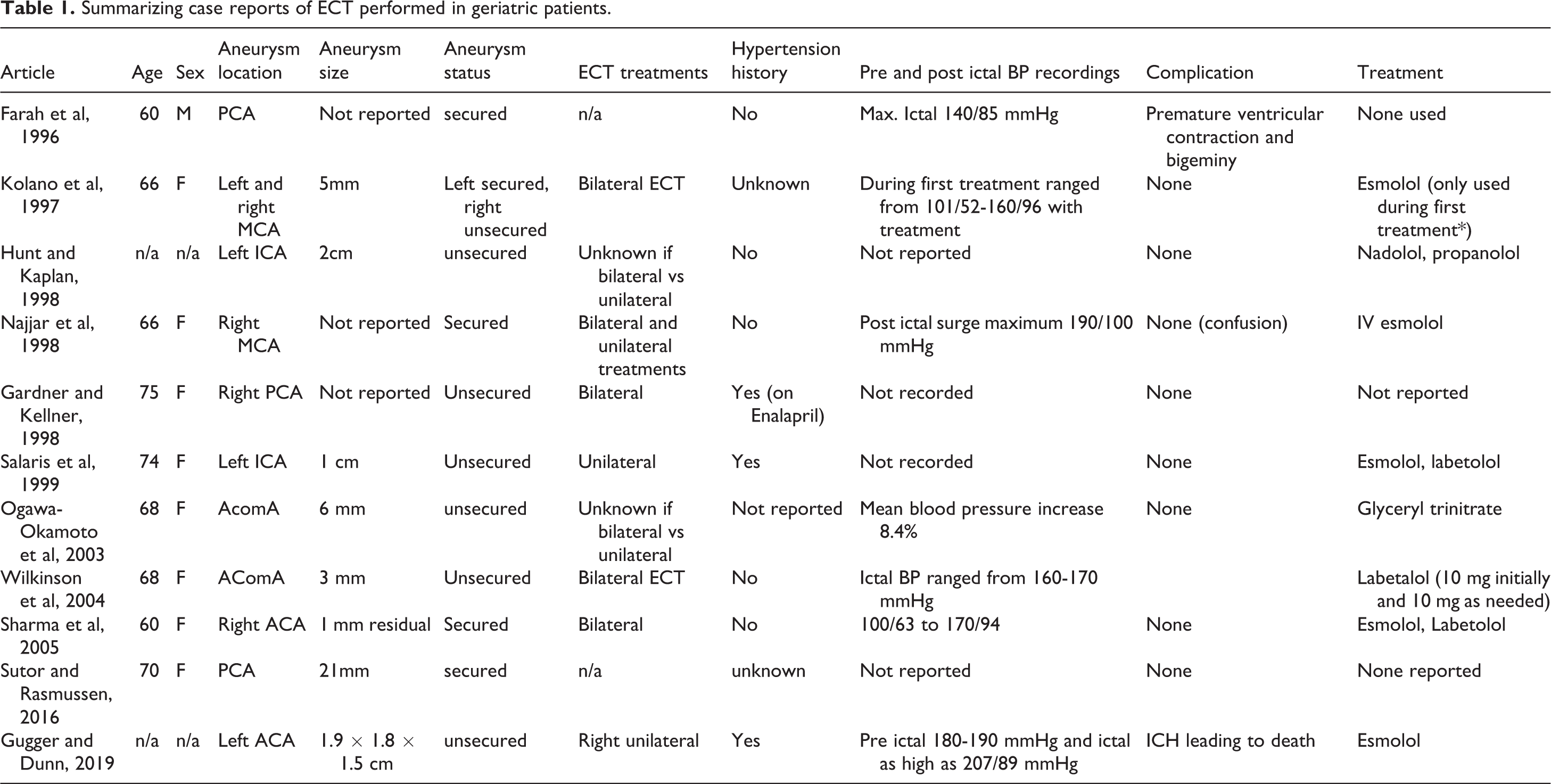
Summarizing case reports of ECT performed in geriatric patients.
Patient Characteristics
The mean age for our sample was 67.4 years. Two reports did not mention the age; however, each report categorized the patient as “geriatric.”10,11 The majority of the patients were female (8 out of 9 cases). Gender was not reported in 2 cases. Three patients had a prior history of hypertension, while others did not mention if there was a previous history of hypertension. Among patients who had a prior history of hypertension, only one was reported to be on antihypertensive medication (i.e., enalapril). 12
Intracranial Aneurysm Characteristics
The posterior cerebral artery (PCA) was the most common site of an aneurysm in the cases we reviewed (3 cases). Other location sites included the Middle Cerebral Artery (MCA), internal carotid artery (ICA), anterior communicating artery (AcomA), and anterior cerebral artery (ACA), (2 cases each). Four out of 11 cases had secured aneurysms.13-16 One patient had both a secured and an unsecured aneurysm. 17 Among those which were secured, 3 were secured via clipping and 2 were secured via coiling. The aneurysms ranged in size from 1 to 21 mm. Three cases did not report the size of the aneurysm.12-14
Treatment
Esmolol was the most used antihypertensive agent to control the ictal surge in blood pressure. Esmolol was used in combination with other agents in 4 cases and as an isolated agent in 2 cases. Other agents used included labetalol (in one case as isolated and in one as a combination with esmolol), glyceryl trinitrate (in one case) and nadolol along with propranolol in one case. No treatment was used in 3 cases.12,13,16
Anesthesia
Five out of 11 cases did not report the type of anesthetic agent used. Propofol and methohexital were used in 3 cases each.
Blood Pressure Measurements
Reports varied in the pattern of recording pre-ictal, ictal, and post-ictal blood pressures. The highest ictal surge was recorded as 207/89. 11
Complications
Nine out of 11 cases reported no complications in the setting of treatment with ECT. In one case, premature ventricular contraction and bigeminy developed post ECT. The abnormal rhythm was successfully treated with lidocaine. 13 In another case, the patient died because of subarachnoid hemorrhage (SAH) occurring due to an ictal hypertensive surge. 11
Discussion
We performed a systematic literature search to enhance our knowledge about the safety profile of ECT in elderly patients with cerebral aneurysms. We identified 11 cases where ECT was performed in elderly patients with identified Cerebral Aneurysm.10-20 The report of a death due to aneurysmal rupture in one case undergoing ECT is alarming given the low reported mortality risk associated with ECT in general (only one death reported in the 9 studies published after 2001 with a total of 414,747 treatments). 6 This implies that the risk of death might be higher among elderly patients with cerebral aneurysms compared to other groups. This finding necessitates that we prudently evaluate the underlying risk factors that elevate the risk of aneurysmal rupture in this population.
Cerebral aneurysms are classified into saccular, fusiform and mycotic aneuryms.6,21 Saccular aneuryms also known as “berry aneurysms” are the most common type of cerebral aneurysms and are usually found on the arteries at the base of the brain.6,21 Fusiform aneurysms are less common in the brain area and occur more frequently in the aorta.6,21 Mycotic aneuryms occur as a result of an infection and hence their discussion is beyond the scope of this article. We have limited the scope of this article to common saccular aneurysms as they constitute up to 90 percent of the brain aneurysms and are clinically more relevant.
Factors that usually predict the risk of aneurysmal rupture include characteristics of an aneurysm such as its size, location and growth, history of hypertension, age, history of smoking, family history and previous history of rupture.
Hypertension alone is considered an independent risk factor for aneurysmal rupture, even in small-sized aneurysms.22,23 Identification and proper management of baseline hypertension are crucial and should be a part of regular medical clearance for ECT, especially in the elderly. It is also known that electrical stimulation given during the ECT transiently increases cerebral vascular pressure.11,14,24 Two experimental trials conducted in rats demonstrated an abrupt elevation in systematic blood pressure and cerebral vascular dilation during the electrical stimulation.25,26 The likely mechanism for the elevation of blood pressure during ECT is the increase in sympathetic discharge. 24 The elevation in vascular pressure increases the risk of rupture by increasing vascular wall tension.11,14,24 Though these physiologic changes are benign and transient in most cases,24,27 the risk is considered to be elevated in vulnerable cases, such as those with aneurysms. Elderly patients further add to the risk. In a study of 52 geriatric patients treated with ECT, 6% of patients reported hypertension (diastolic blood pressure greater than 100 mmHg) 28 as an adverse effect that persisted for longer than 3 days, suggesting that geriatric patients are at higher risk of a hypertensive surge during ECT. In our review the highest ictal surge of 207/89 mmHg is relatively modest compared to those commonly seen during ECT. 29
Due to the suspected risks associated with the increase in blood pressure, it is recommended to control the blood pressure before ECT. 30 Previous studies have also highlighted the need for pre-treatment identification and optimization of cardiovascular risk factors during ECT to minimize complications. 27 We emphasize that such precautionary measures are not limited to patients with known hypertension. However, in cases without a prior history of hypertension, caution should be exercised as pre-treatment with antihypertensive agents might cause unwanted side effects such as bradycardia or asystole with beta blockers. In such cases, we suggest using antihypertensive medications immediately post-seizure instead of pre-seizure treatment.
The following classes of medications have been commonly used to prevent hypertensive surge during ECT:
A- Beta-Blockers:
Both short and long-acting beta-blockers have been used to prevent an increase in blood pressure. However, it has been estimated that short-acting beta-blockers are better because they have minimal impact on the efficacy of seizure activity. 31 Data, however, remains limited, and most studies have not considered case dependent risk factors, such as age and the presence of cardiovascular abnormalities, such as aneurysms.
Among beta-blockers, the most commonly used medications include:
Esmolol is a short-acting beta-blocker. With around 18 reported clinical trials, it is one of the most widely used treatment options and for the same reason is also recommended as the most favorable first choice. 31 It is known to blunt hemodynamic response in the first 3 min of ECT stimulus.30,32 Many suggest that since Esmolol is associated with shortening of the seizure duration, it might impact the efficacy of ECT however the claim remains unsubstantiated. 31
Propranolol has been used to treat hypertensive surge during ECT; however, there is a concern that it was involved in inducing cardiac asystole in one of the cases.30,33
Labetalol is a combined alpha- and beta-adrenoceptor blocker and has been used effectively as both mono and combined therapy.30,31,34 McCall et al found labetalol to be more effective in controlling heart rate than blood pressure. 34 There are also conflicting reviews about the potential to alter the seizure threshold.27,28 When compared with esmolol, labetalol is usually effective after 5 min until about 10 min.31,32
Landiolol is another short-acting beta-blocker. Data remains inconclusive about its ability to control blood pressure during an ictal surge.
B- Calcium channel blockers:
Current trials have shown some efficacy of calcium channel blockers. 35 However, the hypotensive effect is usually accompanied by reflex tachycardia. Hence it has been recommended to use it in combination with the beta-blockers. 35
The following agents among calcium channel blockers have been used:
Nicardipine in a randomized trial worked effectively when combined with labetalol without altering the seizure threshold. However, when used alone, nicardipine might be associated with reflex tachycardia. 35
Diltiazem in a controlled study effectively controlled heart rate and mean arterial pressure compared to placebo; however, it shortened seizure duration which according to some may impact efficacy of ECT. 36
Verapamil use in a controlled trial resulted in a significant decrease in blood pressure and heart rate compared to placebo without altering the seizure threshold. 37
C- Vasodilators:
Among medications that reduce systemic blood pressure via vasodilation, the following agents have been used to control ictal hypertensive surge during ECT.
Nitroglycerin is classified as nitrate and has been employed in hypertensive emergencies. 38 Nitroglycerin is used both as a topical agent and as a patch and in both cases, and has been reported to effectively control arterial pressures during ECT30,39,40
Nitroprusside is also primarily used to treat hypertensive emergencies. 41 It is known to effectively control blood pressure during ECT. 42 Devanand et al reported successful management of blood pressure with nitroprusside and esmolol during ECT in a 74-year-old patient with a history of corrected dissecting aortic aneurysm and current aortic dissection. 43
D- Analgesics:
Remifentanil is an ultra-short acting synthetic opioid analgesic that, in a double-blind crossover study in adjuvant with methohexital anesthetic, was found to attenuate hemodynamic response from ECT in a dose-dependent fashion without impacting seizure activity. 44
E- Miscellaneous:
Some other medications that have also been used include hydralazine 45 and nifedipine 46 ; however, limited literature exists about their utility and efficacy.
Our literature review suggested that short-acting antihypertensives such as esmolol, when used alone, may not be sufficient in controlling ictal hypertension. 11 However, the inefficacy in managing ictal surge could be due to changing pharmacodynamics related to aging. The concern about the decrease in response by beta-blockers, such as labetalol in older patients, has also been raised previously. 34 The same might be true for other antihypertensives that have been studied so far. Thus, we recommend using combination therapy to control blood pressure episodes if monotherapy is unsuccessful.24,30,46 More importantly, in resistant-cases, we recommend using nitroprusside, as it is known to effectively control blood pressure, especially in cases undergoing ECT with arterial aneurysms 43 (Figure 2).
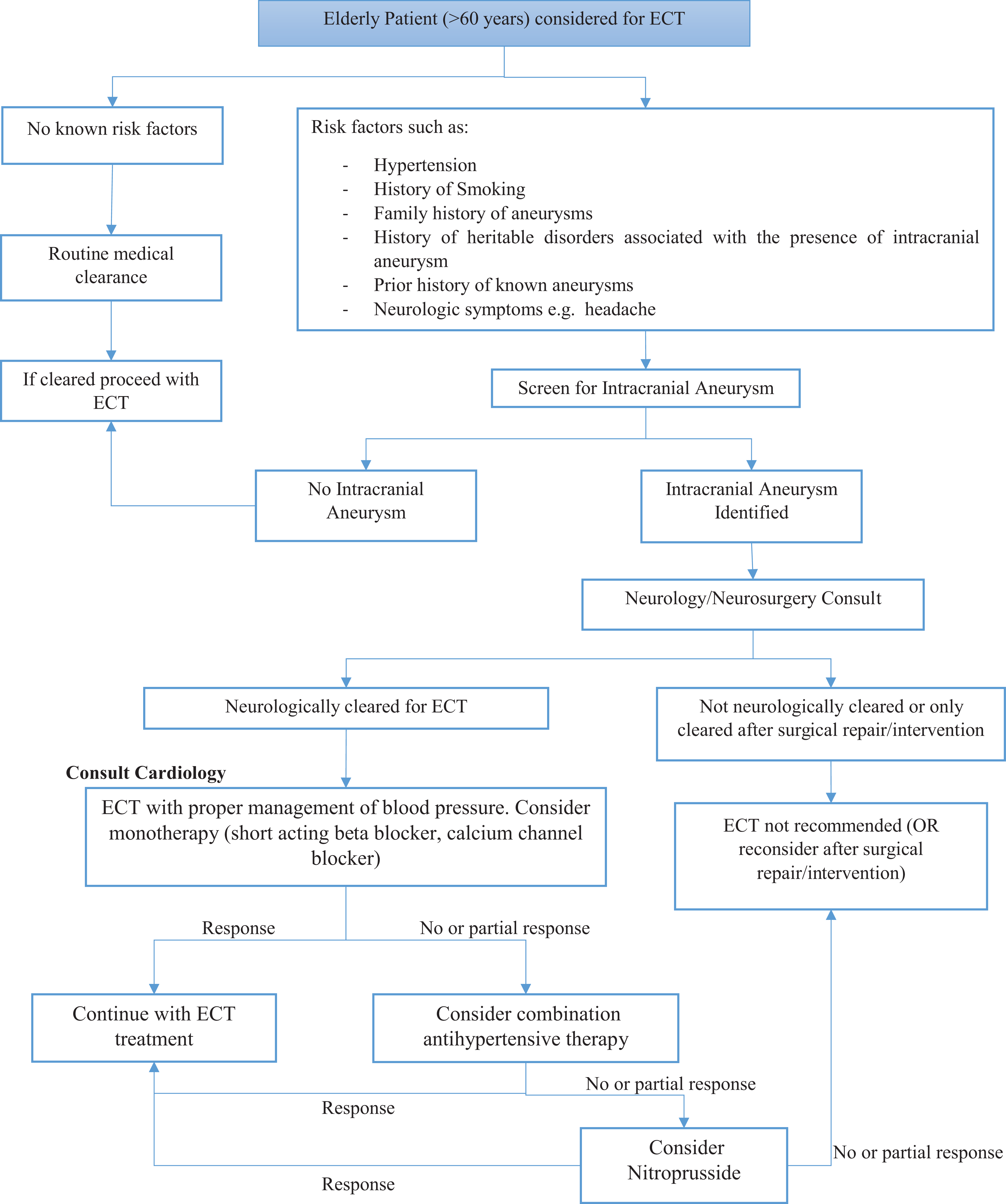
Clinical recommendations for screening and blood pressure management for elderly patients with cerebral aneurysm undergoing ECT.
Aging itself is not only considered a risk factor for aneurysmal growth and rupture, 7 but studies have shown that the elderly have a higher risk of poor outcomes in the setting of SAH due to aneurysmal rupture.47,48 The mean age for our sample was 67.4 years which is relatively younger for an elderly sample. However as per a meta-analysis, older age (>60) was identified as one of the significant risk factors for aneurysmal rupture. 48 Several cases have been reported with ECT successfully performed in young patients (< 60 years old) with cerebral aneurysms. 11 This corroborates with the earlier identified notion that old age alone is a significant risk factor for aneurysmal rupture. However, we do not imply that younger people be considered absolutely safe as other risk factors, such as the history of smoking, characteristics of the aneurysm, medical comorbidities, and sex, also impact the outcomes. 48
Due to the high prevalence of cerebral aneurysms in the general public, it is assumed that many patients undergoing ECT treatments without complications have an underlying undiagnosed cerebral aneurysm. 14 It should be highlighted that in most cases, it is unknown if there is an aneurysm present unless CT or MRI is done, so the actual rate of aneurysms is likely to be much higher than what is reported in the literature. Knowing however that the incidence of rupture in the ECT suite in general is quite a rare event, it is also possible that the risk proposed is over estimated.
All cases that we reviewed carried pre-diagnosed cerebral aneurysms which were identified incidentally. Controversy exists about the screening for aneurysms especially as the risks associated with screening studies such as vascular contrast studies and surgical management are taken into consideration 49 but most agree that screening is beneficial in patients with risk factors such as family history and known genetic conditions associated with presence of aneurysms. 50 So far, to our knowledge, no guidelines exist about screening patients prior to ECT especially as its utility remains unclear. It is our understanding that centers across the country develop their own institutional guidelines and screening protocols. Aging individuals as mentioned above already present with a higher risk but it remains debatable in the light of current literature whether all elderly or only those with additional risk factors should be screened prior to ECT. Based on our review, we recommend that prior to ECT geriatric patients with known risk factors such as hypertension, family history of aneurysms, heritable disorders associated with the presence of intracranial aneurysm, prior history of known aneurysms and a history of smoking should be screened for intracranial aneurysms as a part of routine medical clearance work up. We also emphasize the necessity of neurology/neurosurgical referral 30 (Figure 2). All the cases we reviewed documented some sort of consultation and close communication between relevant specialties.
Lastly, we will discuss aneurysmal characteristics that predict the risk of rupture.
Generally larger aneurysms are at greater risk for rupture; however, it has now been identified that additional factors such as rate of growth, aneurysm angles, degree of atherosclerosis and collagen disposition also determine the risk of rupture.51,52 As a result smaller aneurysms are not considered immune from the risk of rupture. In a review article, it was reported that 13-75% of the ruptured aneurysms were small aneurysms. 53 Also, there is no consensus on the definition of small aneurysms. Usually, cutoff sizes of 5, 7, and 10 mm are used. 53 The patient in our review who developed subarachnoid hemorrhage (SAH) had a large aneurysm (1.9 × 1.8 × 1.5 cm) and thus already at greater risk for rupture.
The discrepancy also exists regarding the risk of rupture depending on location. 8 Some studies predict aneurysms located in the posterior communicating artery to be most at risk for rupture in the elderly. 7 However, others consider anatomical variables such as morphology, hemodynamics, age, sex, and nature of an aneurysm (such as bifurcation aneurysms) as predictors for aneurysmal rupture and disregard the prediction models dependent on location. 48 Also, as per our knowledge, no conclusive evidence exists predicting the risk of rupture between secured/treated vs. unsecured aneurysms. Thus, we suggest that the image-size and location-based rupture prediction models should not be universally used, and caution should be exercised in using ECT treatment in the elderly regardless of the characteristics of the aneurysm.
It is worth mentioning that other vascular aneurysms, such as aortic aneurysms and pulmonary aneurysms, might also present similar challenges. A number of case reports have documented ECT treatments in patients with aortic aneurysms without complications.54-56 Pascoe et al have also reported a case with ECT performed in a patient with a pulmonary aneurysm without any complication. 57 It is noteworthy that pulmonary aneurysms might represent low risk compared to a cerebral aneurysm due to low vascular pressure in the pulmonary vasculature. 57 For the sake of this review, we have limited our scope to brain aneurysms, as these are considered to be the most common and arguably the most dangerous aneurysms. 58 However, given the similarities in the anatomical characteristics of the various types of aneurysms and the mechanism associated with rupture, we assume that similar preventive measures, such as adequate control of ictal hypertension, will limit the risk of a catastrophic outcome in all sorts of aneurysms.
The major limitation of our review is the scarcity of literature. To the best of our knowledge, no controlled trials are available to determine the safety of ECT in the presence of cerebral aneurysms. The case reports we reviewed are the only available source of information. This adds a possibility of bias and errors. However, given the nature and the gravity of the topic under consideration, it is essential that such reviews are conducted to enhance our understanding.
Conclusion
Our review highlights that ECT may be safely performed in elderly patients with cerebral aneurysms, as long as there is careful assessment and management of relevant risk factors. It is recommend that screening for an intracranial aneurysm should be a part of routine medical clearance for ECT in elderly with known risk factors. In those undergoing ECT history of hypertension and the extent of an ictal surge in the blood pressure elevates the risk of aneurysmal rupture during ECT. Effective ongoing and acute management of blood pressure during ECT, with attention to avoiding adverse effects and limiting the impact on ECT efficacy, is the best strategy to optimize ECT outcomes in patients with cerebral aneurysm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.