
Abstract
Background
One of the non-motor features of idiopathic Parkinson’s disease (IPD) is sexual dysfunction (SD) which is under-recognized and, consequently, undertreated. This study aimed to evaluate SD in patients with IPD.
Patients and methods
The study was conducted on 67 IPD patients; 30 healthy subjects with age and gender matching with the patients served as the control group. All participants were subjected to sexual function assessment using the Arabic version of Arizona Sexual Experience Scale (ASEX), Mini-Mental State Examination (MMSE), and Beck Depression Inventory (BDI), while the severity of IPD was assessed using the modified Hoehn and Yahr scoring scale and MDS-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS).
Results
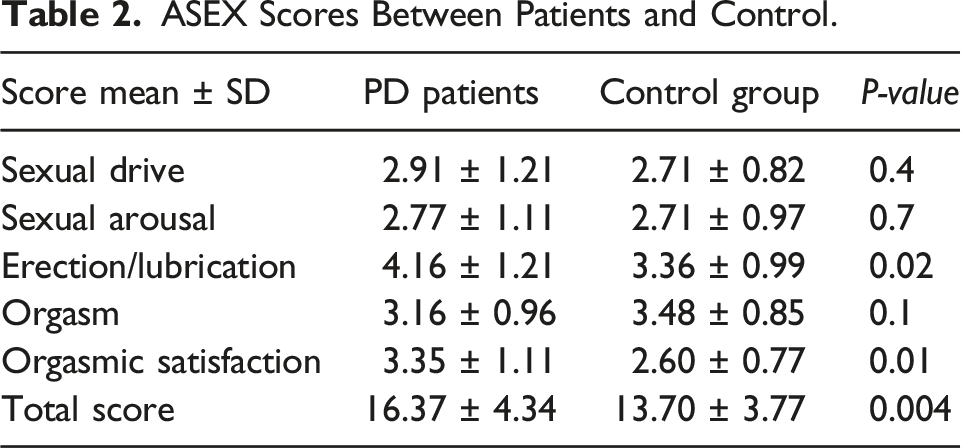
There were no statistically significant differences between patients with IPD and the control group regarding MMSE, hypertension, diabetes mellitus, or dyslipidemia. However, BDI scores were significantly higher in patients with IPD. The rate of SD among our patients was 64% compared to 30% in the control group. The total score and subscales of ASEX were significantly higher in IPD patients than in controls. SD showed a significant correlation with the severity of the IPD irrespective of other variables, including patient age, sex, disease duration, hypertension, diabetes, dyslipidemia, smoking, and dose of L-dopa.
Conclusion
SD is a commonly underrated feature in patients with IPD; it should be investigated carefully as it is an important non-motor symptom that correlates with disease severity.
Keywords
Introduction
Although the motor symptoms of Parkinson’s disease are well known, the non-motor symptoms are under-recognized and, consequently, undertreated. One of these neglected non-motor symptoms is sexual dysfunction (SD) 1 which has not been extensively studied since the early recognition of IPD by James Parkinson.
Previous studies have shown a high prevalence of SD in IPD which includes decreased libido, erectile dysfunction, orgasmic dysfunction, and hypersexuality, which are associated with dopaminergic drugs.2-5 Others reported incomplete and contradictory results regarding the prevalence rates of SD in male and female IPD patients.6,7 SD as a non-motor symptom (NMS) adds more disabilities to IPD patients and interferes with their daily lives. As most IPD patients are older than 60 years, they have a low possibility of receiving adequate sexual counseling. However, the need for intimacy and an affectionate relationship does not subside with age, and it affects the quality of life. 8 More studies are needed to cover the subject of SD in IPD with the purpose of improving the quality of life of such patients and their partners.
Patients and Methods
In the current study, 67 IPD patients (46 men and 21 women) diagnosed according to the UK Parkinson’s Disease Society Brain Bank criteria 9 were recruited from the Neuropsychiatry Department, Neurology outpatient clinic database. Thirty healthy subjects (21 males and 9 females) with age- and sex-matched with the IPD patients were enrolled in the study as a control group.
All patients and controls were assessed for sexual function using the Arabic version of the Arizona Sexual Experience Scale (ASEX). 10 A face-to-face interview was conducted by two of the authors with each patient individually and with his/her partner in two separate sessions two weeks apart. The Arizona Sexual Experiences Scale (ASEX) Arabic version consists of five subscales or items (ie, five individual questions assessing sexual desire, arousal, erection/lubrication, ability to reach orgasm, and satisfaction from orgasm). For each item, the lowest possible score is 1 and highest is 6 points. 11 A score of 19 points was applied as a cutoff value to determine whether the subject had SD. Those who scored 19 or higher were considered to have SD. In addition, those who scored less than 19 but scored 4 points in three or more items or who scored specifically 5–6 points in any one item were considered to have SD. 11
All participants were evaluated using the Mini-Mental State Examination (MMSE) and Beck Depression Inventory (BDI). The severity of IPD was assessed using the modified Hoehn and Yahr scoring scale 12 and MDS-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). 13 Exclusion criteria included a score lower than 21 in Mini-Mental State Examination (MMSE), 14 presence of urological medical disorders known to affect sexual functions, drug abuse, thyroid dysfunction, and psychosis.
The study proposal was approved by the Research Ethics Committee and Quality Assurance Unit of the Faculty of Medicine, Tanta University. Participation was voluntary, and informed written consent was obtained from all participants to clarify any possible risks. Statistical analyses were conducted using SPSS Prism version 20, 2013 (created by IBM, Armonk, NY, USA). Statistical differences between the studied groups were tested using the Chi-square test for categorical variables and ANOVA/Post-ANOVA tests for numerical variables. Statistical significance was set at P <.05. Correlation analysis was performed using Pearson’s correlation test.
Results
Demographic Data of the Patients and Control Group.

Abbreviations: MMSE Mini-Mental State Examination; BDI: Beck Depression Inventory; ASEX: Arizona Sexual Experiences Scale.
ASEX Scores Between Patients and Control.
Demographic Characteristics IPD Patients According to Gender.
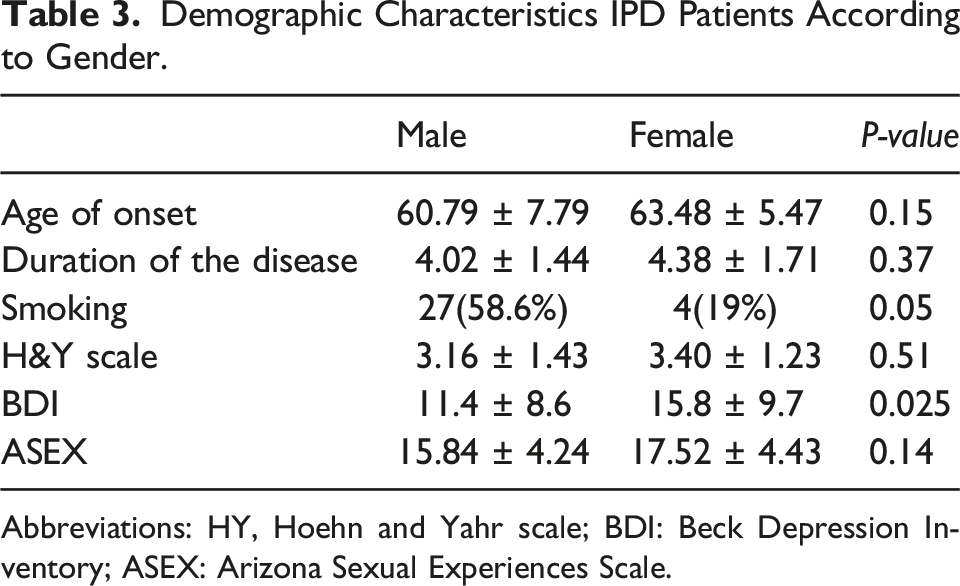
Abbreviations: HY, Hoehn and Yahr scale; BDI: Beck Depression Inventory; ASEX: Arizona Sexual Experiences Scale.
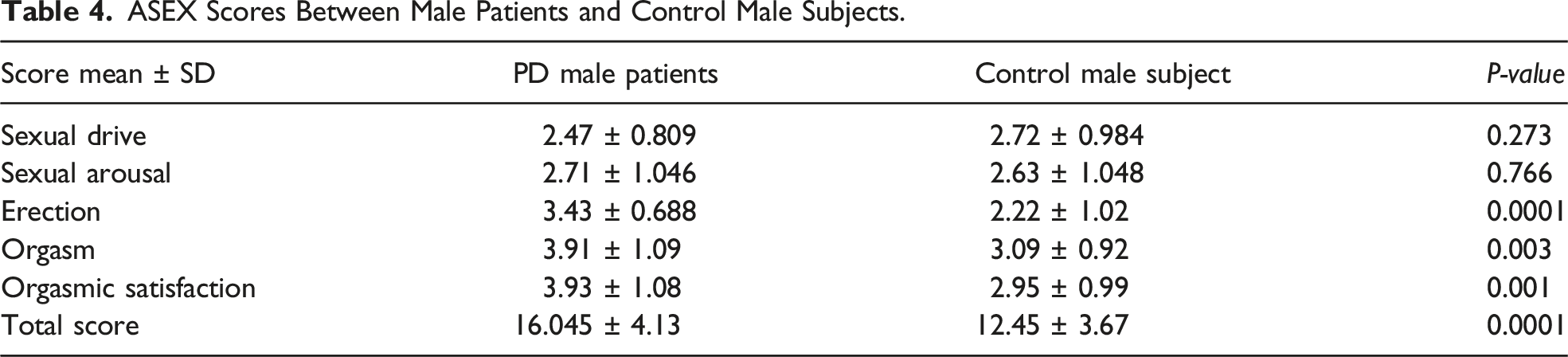
ASEX Scores Between Male Patients and Control Male Subjects.
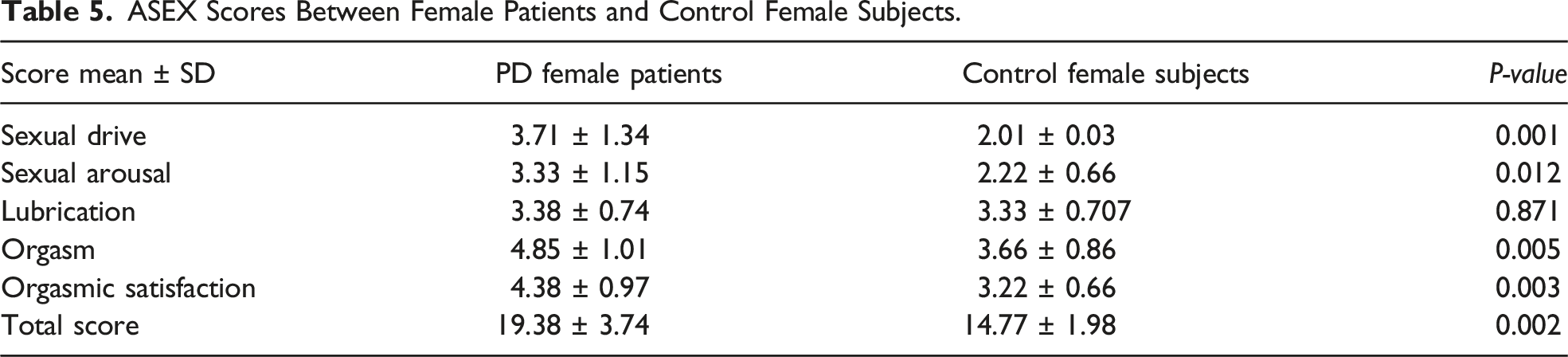
ASEX Scores Between Female Patients and Control Female Subjects.
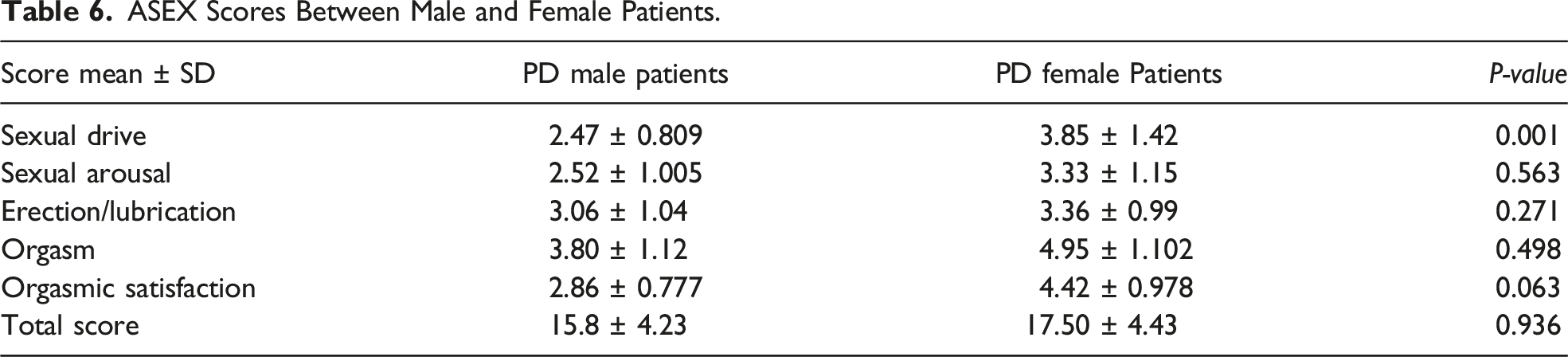
ASEX Scores Between Male and Female Patients.
Hoehn and Yahr Staging and ASEX.
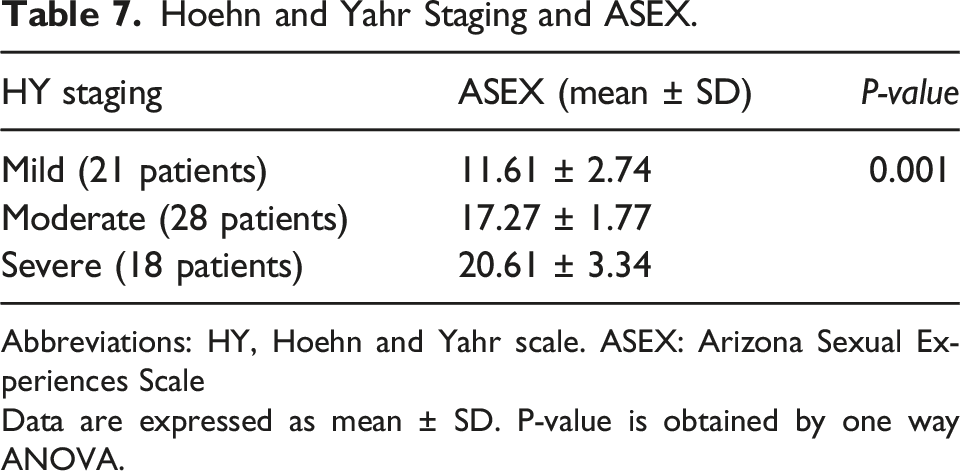
Abbreviations: HY, Hoehn and Yahr scale. ASEX: Arizona Sexual Experiences Scale
Data are expressed as mean ± SD. P-value is obtained by one way ANOVA.
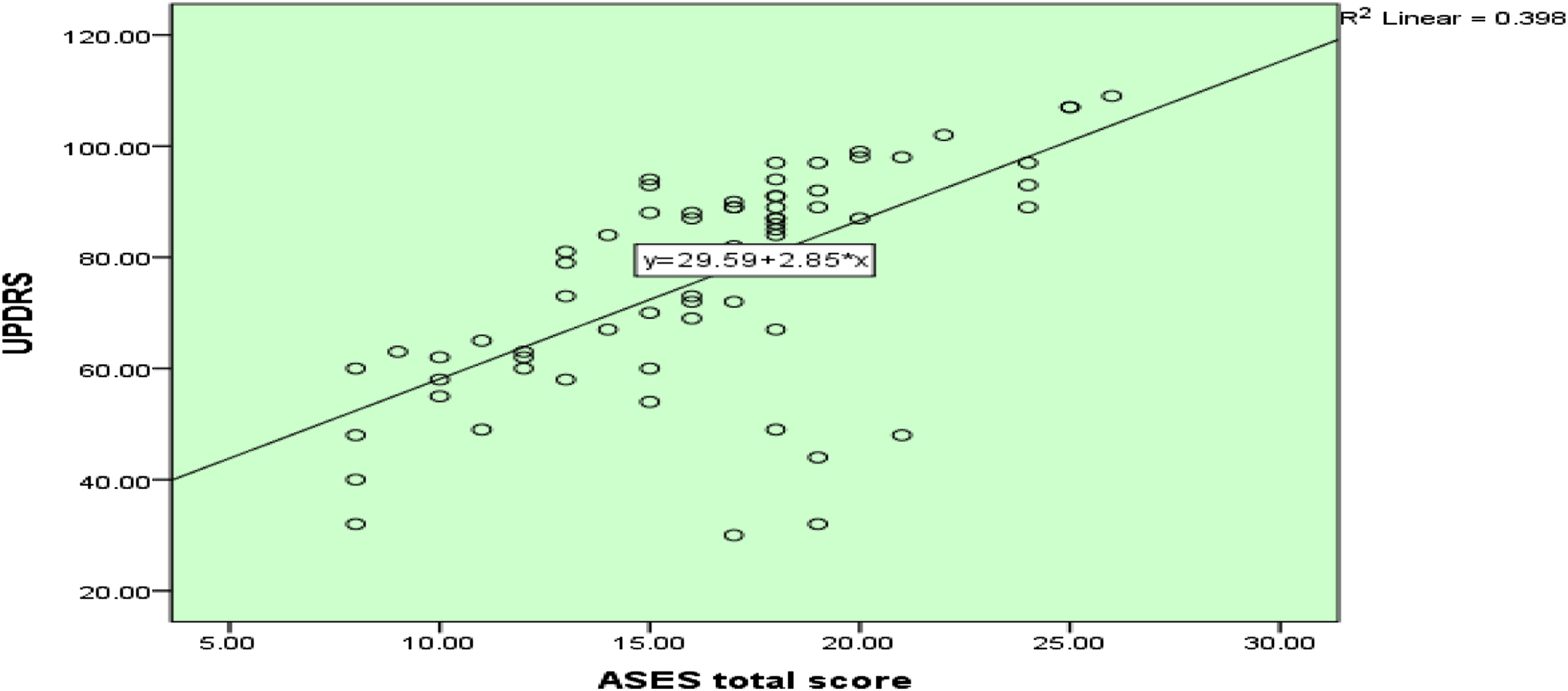
Positive significant correlation between Arizona Sexual Experiences Scale (ASES) and Unified Parkinson’s Disease Rating Scale (UPDRS) as (P≤0.001).
Finally, a regression analysis revealed that ASEX scores were affected by most variables in the studied patients (age, disease duration, total score of UPDRS, BDI scores, and the presence of DM) with a P value ≤0.05. Meanwhile, the presence of either HTN or dyslipidemia had no effect on the total ASEX score (Appendix 1).
Discussion
The reported rates of SD in IPD have varied in published literature from different countries. It was reported in 30%, 66.6%, and 81.6% of patients with IPD in Mexico, 16 Egypt, 17 and Thailand, 18 respectively. The varying results of these studies could be due to two reasons: (1) most patients probably felt uncomfortable and ashamed to discuss sexual issues with their neurologists during regular consultation and (2) the studies used diverse methodologies (face-to-face, phone, or email interviews). 19 Another issue that can hinder the extensive and accurate evaluation of SD is religion. Discussing sexual topics goes against the religious beliefs of Muslim patients. Evaluation is especially difficult in the case of Muslim women as them discussing their sexual experiences could be considered immoral and embarrassing by their husbands and families.20.21 Also women do not prefer disclosing their sexual life in front of strangers as it can negatively affect their self-image. 22
It is equally true that neurologists also seem to be somewhat insensitive and less attentive toward NMS. 23 Most sexual health services in Egypt are directed toward reproductive medicine and family planning, and it is one of the factors behind the underestimation of SD prevalence among elderly people. 24
To the best of our knowledge, this is the first study to focus on SD among IPD patients in Egypt. Sexual dysfunction is not gender-specific or age-related. This is in contrast to the study of Ferrucci et al, 25 who reported no difference in sexual function between mild and moderate IPD patients and the normal population. The discrepancies between these two studies may result from the different methodologies, cultures, and sample sizes. In our study, patients with severe IPD, as assessed by the Hoehn and Yahr scale, were enrolled. Our results are consistent with a study by Bronner and Vodusek, 26 who reported that sexual dysfunction is common in PD patients even if they are young. In addition, a study by Brown et al, 27 conducted on young IPD patients, found that the prevalence of SD was higher in male patients (65%) and much lower in female patients (36%). Young age can explain the severe effect of the disease itself on sexual function, although aging is the most significant risk factor for hypoactive sexual desire. 28 Solla et al 29 reported that non-motor functional impairment was more common in females, and there was no statistically significant difference on the level of gender concerning SD.
Erectile dysfunction in males and dry vagina in females were reported in our study, and orgasmic dissatisfaction was observed in both genders on the ASEX subscale. A previous study that focused on sexual function in young IPD patients reported that women were significantly more affected than men; reduced libido was reported by 40% of male patients and 70% of female patients. 30
Bronner et al investigated sexual function in 75 IPD patients. Women reported difficulties in getting aroused (87.5%), difficulties in reaching orgasm (75%), low sexual desire (47%), and sexual dissatisfaction (38%), while men reported having erectile dysfunction (68%), sexual dissatisfaction (65%), premature ejaculation (41%), and difficulties in reaching orgasm (40%). 31 The results of this early study correspond with our results despite the different sexual function scales used in the evaluation of the problem, the negative effect of the disease or effect on daily life activities including sexual life, and different drug regimens applied in the treatment of the patients. There was a significant association between the severity of IPD and sexual dysfunction; thus, another possible confounding factor for SD was motor symptoms which made sexual activities even more difficult. 32 Foreplay requires fine finger touch and secure hand movements. Kissing demands a stable head and the participation of the facial and postural muscles. 33
Psychiatric comorbidities may also contribute to the development of SD in patients with IPD. 34 Depression and anxiety are considered the most common NMS in IPD, with a prevalence of up to 70% and 66%, respectively, as shown in epidemiologic studies. Both depression and anxiety are associated with significant reductions in libido and orgasmic ability, and SD is often accompanied by depression and anxiety disorders in both men and women with IPD. Moreover, many patients with IPD receive psychotropic medications, such as antidepressants, which have been reported to impair sexual function. 35
Depression was more common in IPD patients than in the control group, and was more prevalent in female patients than in male patients. Depression is associated with hypoactive sexual desire and impaired erectile function. About 50–60% of untreated depressed patients in a previous study reported some degree of sexual dysfunction. Hypoactive sexual desire disorder, subjectively ascribed to fatigue, is also common among patients with chronic diseases. 36
Meanwhile, impaired sexual function can lead to depression which may have bidirectional action in patients with IPD. These findings suggest that depression can affect up to 45% of patients with IPD. 37 Jacobs et al 38 found that the frequency of depression was higher in sexually dissatisfied men with PD.
Conclusion
Sexual dysfunction associated with IPD patients should be investigated carefully, as it is a non-motor symptom that can affect patients’ quality of life. Motor symptoms have a distressing effect on sexual functions. Neurologists should pay more attention to the presence of SD and motor symptoms for better planning of effective therapeutic decisions.
Study Limitations
The sexual experience was not evaluated in our patients’ group before and after the diagnosis with PD.
The effect of anti-parkinsonian medications on sexual dysfunction was not addressed in our study whether these drugs have effect on our results or not.
The data were not collected anonymously. In contrary, two investigators were present during the interview to give patients the feeling that it was an academic professional work and a female resident attended the interview with female subjects to relieve their anxiety.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Multiple regression analysis revealed that; ASEX scores were affected by most variable in the studied patients (age, disease duration, total score of UPDRS, BDI scores, and the presence of DM) as (P ≤ 0.05) mean while the presence of HTN or dyslipidemia did not affect the ASEX total score. aDependent Variable: AESX.
Coefficientsa
Model
Unstandardized Coefficients
Standardized Coefficients
t
Sig.
B
Std. Error
Beta
1
(Constant)
2.047
3.055
.670
.506
DM
3.503
.841
.406
4.165
.000
UPDRS total
.116
.045
.043
2.160
.0293
AGE
.141
.042
.228
3.332
.001
HTN
.785
.810
.091
.969
.337
Dyslipidemia
.444
.638
.046
.695
.490
DURATION
1.263
.246
.444
5.131
.000
BDI
.126
.058
.182
2.168
.034