
Abstract
Background
The current comparative efficacy, safety, and acceptability of atypical antipsychotics (AAPs) in treating Parkinson's Disease Psychosis (PDP) are not entirely understood.
Objective
To evaluate comparative efficacy, safety, and acceptability of AAPs in patients with PDP.
Methods
We conducted a systematic review and a network meta-analysis to compare the efficacy, safety, and acceptability of pimavanserin, quetiapine, olanzapine, clozapine, ziprasidone, and risperidone. We estimated relative standardized mean differences (SMDs) for continuous outcomes and odds ratios (OR) for binary outcomes, with their respective 95% confidence intervals (CIs).
Results
We included 19 unique studies evaluating AAPs in a total of 1,242 persons with PDP. Based on Clinical Global Impression Scale for Severity, pimavanserin (SMD, −4.81; 95% CI, −5.39, −4.24) and clozapine (SMD, −4.25; 95% CI, −5.24, −3.26) significantly improved symptoms compared with placebo. Also, compared to placebo, pimavanserin (OR, 1.16; 95% CI, 1.07, 1.24) significantly improved psychotic symptoms based on Scale for Assessment of Positive Symptoms for Parkinson's Disease Psychosis/Hallucinations and Delusions scores. In comparison to placebo, clozapine (SMD, −0.69; 95% CI, −1.35, −0.02), pimavanserin (SMD, −0.01; 95% CI, −0.56, 0.53), and quetiapine (SMD, 0.00; 95% CI, −0.68, 0.69) did not impair motor function per Unified Parkinson's Disease Rating scale. Based on Mini-Mental State Examination scale, quetiapine (SMD, 0.60; 95% CI, 0.07, 1.14) significantly impaired cognition compared to placebo.
Conclusions
In patients with PDP, pimavanserin and clozapine demonstrated significant improvement in psychosis without affecting motor function. With quetiapine being associated with a significant decline in cognition and despite not impairing motor function, our findings suggest that it should be avoided in patients with PDP and reduced cognitive abilities.
Introduction
Parkinson's disease (PD) affects nearly 1 million individuals in the US and more than 10 million globally.1,2 Over and above PD's typical motor symptoms, many patients develop cognitive changes and neuropsychiatric symptoms such as psychosis (i.e., hallucinations and delusions), which can be greater sources of morbidity than motor dysfunction.3-5 Up to 60% of patients with PD alone and about 75% of patients with co-morbid dementia may present persistent psychotic symptoms requiring antipsychotic (AP) medications.6,7 PD-associated psychosis (PDP) may develop due to PD itself or as a consequence of drugs targeting PD-associated motor dysfunction. 8 PDP increases healthcare resource utilization and the likelihood of disability, hospitalization, institutionalization, new-onset dementia, and death.5,8-12
Therefore, optimal treatment with APs in patients with PDP is critical to avoiding detrimental health outcomes and reducing unnecessary healthcare costs.
In 2016, pimavanserin became the first drug approved by the US Food and Drug Administration (FDA) for hallucinations and delusions associated with PDP. 13 Before the FDA approval of pimavanserin, clinicians prescribed other atypical antipsychotic (AAP) medications to treat PDP. 11 These off-label AAPs can result in worsened motor symptoms, cognitive decline, metabolic disturbance, and in the case of clozapine, need for specialized monitoring of absolute neutrophil counts (ANC).6,11 Multiple randomized controlled trials (RCTs) have provided strong evidence of both pimavanserin's efficacy in treating PDP and its lack of known effects on motor function, blood dyscrasias, or metabolic markers. 14 Moreover, in an observational retrospective analysis of Medicare patients with PD, the associated risk of mortality was lower in pimavanserin patients than with other AAPs for first 180-days of the treatment, while the risk of mortality was similar thereafter. These findings were limited to patients in the community setting only. 15
However, despite the FDA approval of pimavanserin for PDP, its effectiveness, and more favorable adverse-effect profile, treatment guidelines continue to recommend quetiapine and clozapine as well as pimavanserin, and quetiapine and clozapine continue to be commonly prescribed to treat PDP.11,16 Quetiapine, the most frequently used AAP for treating PDP that is prescribed off label, has shown mixed efficacy in RCTs and is associated with increased somnolence and orthostatic hypotension.17,18 There is some evidence supporting the effectiveness of clozapine,14,19 but its use is associated with an increased risk of pneumonia-related hospitalization, myocarditis, hematologic malignancies, orthostatic hypotension, syncope, neutropenia, and life-threatening agranulocytosis.11,20-23 Thus, treatment with clozapine requires intensive ANC monitoring. 24
While previous studies of patients with PDP evaluated pimavanserin's relative efficacy and safety compared with other AAPs, no studies have assessed the comparative acceptability of AAPs, including pimavanserin, on a broad range of acceptability outcomes defined as discontinuations due to lack of efficacy, adverse events (AEs), and all causes.14,19,25 Therefore, this study evaluated the comparative efficacy, safety, and acceptability of pimavanserin and other AAPs used to treat PDP. Determining the comparative acceptability, in addition to the relative efficacy and safety of AAPs for patients with PDP, provides more comprehensive evidence to clinicians to better inform treatment decisions.
Methods
We conducted a systematic literature review (SLR) based on the Cochrane Handbook for Systematic Reviews of Interventions. 26 Following the SLR, we conducted a network meta-analysis (NMA) and matching-adjusted indirect comparison (MAIC). The reporting of this study follows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guideline. 27
Eligibility Criteria
We utilized the Population, Intervention, Comparator, Outcomes, and Study design (PICOS) framework as an eligibility criterion to search, select and review relevant studies. We included study participants of patients diagnosed with nondrug PDP and drug-induced psychosis (DIP) with or without dementia. Articles were excluded if they did not use operationalized criteria for diagnosing PDP, such as the International Classification of Disease 9th or 10th Revision (ICD-9/10) or the Diagnostic and Statistical Manual of Mental Disorders. 28 The interventions included were typical and atypical APs with or without multiple comparator groups, placebo controls, and outcomes related to efficacy, safety, and acceptability (i.e., discontinuations due to any AEs, lack of efficacy, and all causes). In addition, we included RCTs, open-label (OL) trials, post hoc analyses, and observational studies of AAP monotherapy in treating patients with PDP.
We assessed efficacy as improvement in the severity of psychotic symptoms using the Clinical Global Impression Scale for Severity (CGI-S) and improvement in psychosis using the Brief Psychiatric Rating Scale (BPRS) and the Scale for Assessment of Positive Symptoms for Parkinson's Disease Psychosis/ Hallucinations and Delusions (SAPS-PD/H+D). The CGI-S scale measures the patient's severity of symptoms relative to the severity of other patients experiencing the same mental ailment. 29 The BPRS scale characterizes psychotic symptoms in PD and measures ratings based solely on clinician-observed symptom severity. 30 The SAPS-PD assesses and provides qualitative information about specific features of hallucinations, delusions, and behavioral changes associated with psychosis. 30 Additionally, we assessed safety as impairment in motor functions using the Unified Parkinson's Disease Rating Scale Parts II/III (UPDRS II/III), a decline in cognition using Mini-Mental State Examination (MMSE) scale, and AEs such as somnolence. The UPDRS II (Activities of daily living [ADL]) allows a physician to assess patients' perceptions of their ability to carry out ADL, including dressing, walking and eating, whereas UPDRS III (motor section) covers the motor evaluation of disability and includes ratings for tremor, slowness (bradykinesia), stiffness (rigidity), and balance. 31 The MMSE assesses cognitive functioning, with a decrease in MMSE level from baseline indicating impairment in cognition. Further, acceptability outcomes were summarized as all-cause discontinuations, discontinuations due to lack of efficacy, and discontinuations due to any AEs.
Data Source & Search Strategy
We searched MEDLINE via PubMed, EMBASE, Cochrane Library, Health Technology Assessment (HTA) databases, NHS Economic Evaluation Database (NHS EED), Database of Abstracts of Reviews of Effects (DARE), ClinicalTrials.gov, and conference proceedings using pre-specified criteria until October 2021 for inclusion in the SLR. We included articles published in the English language only. The search strategy did not have any restrictions on the publication date, age, living setting, gender, race, ethnicity, or geographical region of the patient population. We developed search strategies using MeSH terms in PubMed and Cochrane Library, Emtree terms in EMBASE, and text words related to AP treatment for PDP. Details of the search strategy are presented in supplementary table 1.
Search, Study Selection, & Data Extraction
Two researchers independently searched the electronic databases through the Anlitiks SLR platform, a proprietary internal search engine within Anlitiks that allows integrated searches of selected index databases such as Medline/PubMed and Cochrane Library separately. Articles were also independently screened against predefined eligibility criteria in two phases, title/abstract screening (Phase 1) and full-text screening (Phase 2). Subsequently, data were extracted from eligible articles that passed Phase 2 screening using an a priori standardized data extraction form in Microsoft Excel. The two independent abstractors resolved any disagreement between them by consulting a third reviewer. To ensure the same study was not included as two different studies, we extracted data from both primary and secondary articles as one study. Preference was given to the publication of a study reporting the most recent data on the outcomes of interest. We extracted the following information from the included studies: mean change from baseline scores, standard deviation, and sample size in each study arm, whereas, for categorical outcomes, the number of events and sample size in every study arm were reported.
Risk of Bias and Study Quality Assessment
We used the Cochrane Risk of Bias tool and Risk of Bias In Non-randomized Studies of Interventions' to assess the risk of bias for randomized 32 and non-randomized studies, 33 respectively. The risk of bias in randomized studies was evaluated in seven domains; sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome data, selective outcome reporting, and other sources of bias. 32 We categorized the risk of bias as “Low risk,” “High risk,” and “Unclear risk.”
Data Analysis
Network Meta-Analysis
We performed an NMA according to the PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions. 34 Before conducting the NMA, we ensured that necessary assumptions of homogeneity, transitivity, and consistency were met. To assess transitivity assumption, we examined the distribution of clinical variables such as age and sex that could potentially modify treatment effect across AAP comparisons. 35 We used the loop-specific and node-splitting approaches to determine inconsistency, which is a disagreement between direct and indirect sources of evidence.36-38 The node splitting method separates evidence on a particular comparison into direct and indirect evidence and uses it to examine inconsistency in a model.39,40 We used a frequentist approach 36 to compare all outcomes using a random-effects model with the 'network' package in Stata Statistical Software, version 16 (StataCorp, College Station, Texas). In cases where there is no evidence to suggest consistency, we used a design-by-treatment interaction model to estimate treatment effects. 41
We compared continuous outcomes of AAPs by estimating effect sizes (Cohen's d) as standard mean differences (SMDs) and their 95% confidence intervals (CIs) based on changes from baseline to the final endpoint. Using Cohen's rule of thumb, the clinical importance of these SMDs can be interpreted as small, medium, or large (e.g., SMD = 0.2, low; SMD = 0.5, medium; and SMD = 0.8, large). 42 Since higher scores on the MMSE scale meant a lower level of cognitive impairment, the algebraic signs for individual scores were reversed before analysis. 43 Therefore, SMDs with negative values suggested improvements, and positive values indicate impairment across all comparisons of continuous outcomes. For binary outcomes, we compared AAPs by estimating odds ratios (ORs) and their respective 95% CIs. In the case of binary outcomes with zero counts in observed treatment, we implemented the standard procedure of continuity correction by adding 0.5 to all cells for any trial with a zero count.44,45 We used the surface under the cumulative ranking curve (SUCRA) to rank the treatments. SUCRA is a single number associated with each treatment ranging from 0 to 100% that represents the predicted probability that an AAP will rank favorable (in terms of efficacy, safety, or acceptability) compared to a hypothetical treatment option that will certainly rank the best.46,47 The closer a treatment's SUCRA value was to 100%, the more likely it was to be the most efficacious, acceptable, or safe treatment. Finally, we created cluster ranking plots using the SUCRA values to simultaneously compare AAPs based on efficacy, safety, and acceptability outcomes. 48 A cluster ranking analysis is a technique used for categorizing groups based on their characteristics in such a way that the degree of association is high between members of the same group and low between members of different groups. 48
Matching-Adjusted Indirect Comparison
An NMA for the SAPS-PD was not feasible due to the lack of a common comparator to compare all AAPs with available data on the outcome. To indirectly compare the AAPs in the absence of a common comparator, we conducted a MAIC. MAIC requires access to individual patient data (IPD) from trials of at least one treatment which are further matched on baseline summary characteristics reported from trials of another treatment. 49 We defined treatment response as a ≥30% decrease from baseline SAPS-PD/H+D score consistent with the methodology used by Citrome et al. 50 We dichotomized the outcome using ≥30% as a threshold to indicate clinically relevant symptom improvement. 51 We reweighted patients' baseline age and sex in the IPD of Cummings et al. 52 to match those of the aggregate data from included studies with available data on SAPS-PD/H+D. The reweighted data was used to estimate ORs across AAPs. Additionally, to examine the robustness of our findings, a sensitivity analysis was conducted using the same approach for threshold points of ≥20% and ≥40%, respectively.
Results
We identified 1,540 unique articles by searching the bibliographic databases, and their titles and abstracts were screened for eligibility against predefined inclusion/exclusion criteria. A total of 160 studies were eligible for full-text screening. We selected 32 eligible articles for the SLR (n = 1,860) and 19 studies for the NMA after the full-text review. The PRISMA flow diagram (Figure 1) illustrates the search yield and study attrition to select eligible studies. PRISMA study selection flowchart.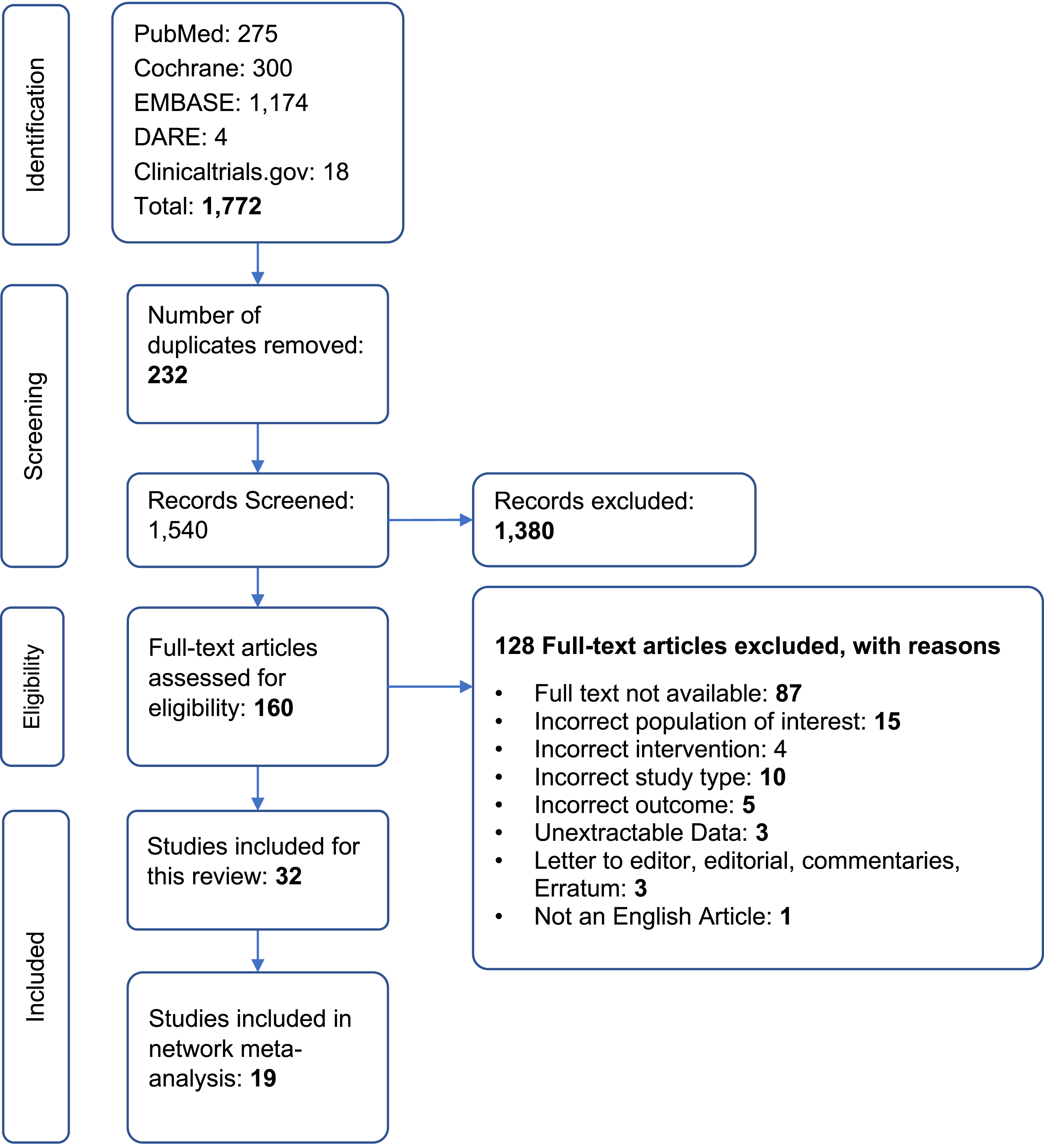
Patient Characteristics
The 19 studies52-70 included in the NMA had a total of 1,242 patients with a median follow-up of 12 weeks (range, 4 to 104 weeks). The median of the average age of patients in the included trials was 72 years (range, 68 to 75 years), and most were male (63.8%)
Risk of Bias & Study Quality Assessment
There was a low risk of selective outcome reporting in the studies included in this SLR and NMA. The most common limitations of the included studies were limited information on random sequence generation and the lack of blinding of outcome accessors (supplementary figure 1a and figure 1b).
Efficacy Outcomes
The Clinical Global Impression-Severity Scale
A total of 5 eligible studies52,53,55,70 (n = 413 patients) were included in the NMA of CGI-S outcome. Supplementary figure 2 (a) depicts the network diagram for CGI-S scale. Compared with placebo, pimavanserin (SMD, −4.81; 95% CI, −5.39, −4.24), clozapine (SMD, −4.25; 95% CI, −5.24, −3.26), and quetiapine (SMD, −1.15; 95% CI, −2.23, −0.07) significantly improved severity of psychotic symptoms on the CGI-S scale (Figure 2a). Pimavanserin significantly improved psychosis compared to olanzapine (SMD, −4.91; 95% CI, −5.56, −4.25), and quetiapine (SMD, −3.67; 95% CI, −4.89, −2.44,) (supplementary table 3a). SUCRA ranking suggested that pimavanserin (95.7%) had the highest probability of improving psychosis followed by clozapine (79.3%) (supplementary figure 6a). Forest plots for efficacy outcomes of atypical antipsychotics in comparison with drug comparators. (A) Forest plot for Clinical Global Impression Scale for Severity (CGI-S) scale, representing pooled standard mean differences comparing each treatment option with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 0 (null value); the results imply statistical significance (B) Forest plot for Brief Psychiatric Rating Scale (BPRS) scale, representing pooled standard mean differences comparing each treatment option with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 0 (null value); the results imply statistical significance (C) Forest plot for Scale for Assessment of Positive Symptoms for Parkinson's Disease Psychosis/ Hallucinations and Delusions (SAPS-PD/H+D) scale (dichotomized at 30% cut-off), representing pooled odds ratio comparing pimavanserin with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 1 (null value); the results imply statistical significance.
Brief Psychiatric Rating Scale
Ten eligible studies53-55,57,60,66,68-70 (n = 387 patients) were included in the NMA of BPRS outcome. Supplementary figure 2b depicts the network diagram for the BPRS scale. Clozapine (SMD, −4.23; 95% CI, −6.53, −1.93), and ziprasidone (SMD, −4.70; 95% CI, −8.90, −0.50) significantly improved psychosis in comparison with placebo (Figure 2b). On the other hand, quetiapine (SMD, 1.12; 95% CI, −0.71, 2.96) did not improve psychotic symptoms. Also, in comparison with olanzapine (SMD, 3.27; 95% CI, 0.75, 5.80) and quetiapine (SMD, 5.35; 95% CI, 2.82, 7.89), clozapine significantly improved psychosis (supplementary table 3a). SUCRA suggested that ziprasidone (81.3%) had the highest probability of improving psychosis, followed by clozapine (76.7%) and risperidone (71.9%)
Scale for the Assessment of Positive Symptoms- Parkinson's Disease
Six eligible studies57,58,61,62,66 (n = 505 patients) and IPD data from Cummings et al, 52 (n = 157 patients) were included in the MAIC analysis of the SAPS-PD outcome. Pimavanserin (OR, 1.16; 95% CI, 1.07, 1.24) was associated with significantly greater odds of improving psychosis than placebo (Figure 2c). Similarly, although not statistically significant, pimavanserin had higher odds of improving psychotic symptoms compared to clozapine (OR, 1.14; 95% CI, 0.98, 1.31), olanzapine (OR, 1.23; 95% CI, 0.91, 1.37), and ziprasidone (OR, 1.13; 95% CI, 0.91-1.37). Results from sensitivity analysis were consistent with the primary analysis suggesting that pimavanserin was associated with higher odds of improving psychosis compared with placebo at both cut-offs, i.e., 20% cut-off (OR, 1.12; 95% CI, 1.02, 1.21) and 40% cut-off (OR, 1.05; 95% CI, 0.98, 1.15), respectively (supplementary figure 5).
Safety Outcomes
Unified Parkinson's Disease Rating Scale
Fifteen eligible studies52-55,57,58,60,66-70 (n = 1,035 patients) were included in the NMA of UPDRS outcome. Supplementary figure 3 (a) depicts the network diagram for the UPDRS scale. Compared with placebo, clozapine (SMD, −0.69; 95% CI, −1.35, −0.02), pimavanserin (SMD, −0.01; 95% CI, −0.56, 0.53), and quetiapine (SMD, 0.00; 95% CI, −0.68, 069) did not worsen motor symptoms (Figure 3a). Results for all AAPs compared to each other were not statistically significantly different (supplementary table 3b). SUCRA suggested that clozapine (78.0%) had the highest probability of being safe in avoiding impairment of motor function (supplementary figure 7a). Forest plots for safety outcomes of atypical antipsychotics in comparison with drug comparators. (A) Forest plot for Unified Parkinson's Disease Rating Scale Parts II/III (UPDRS II/III) motor scale, representing pooled standard mean differences comparing each treatment option with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 0 (null value); the results imply statistical significance.(B) Forest plot for Mini-Mental State Examination (MMSE), representing pooled standard mean differences comparing each treatment option with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 0 (null value); the results imply statistical significance. Note that since higher scores on the MMSE scale meant a lower level of cognitive impairment, the algebraic signs for individual scores were reversed before analysis. Therefore, SMDs with negative values in this study suggested improvements, and positive values indicate impairment across all comparisons of continuous outcomes. (C) Forest plot for somnolence, representing pooled odds ratio comparing each treatment option with placebo or dug. The blue boxes denote the point estimate for each treatment , while the horizontal line denoted the 95% CI. If the 95% CI does not cross 1 (null value); the results imply statistical significance.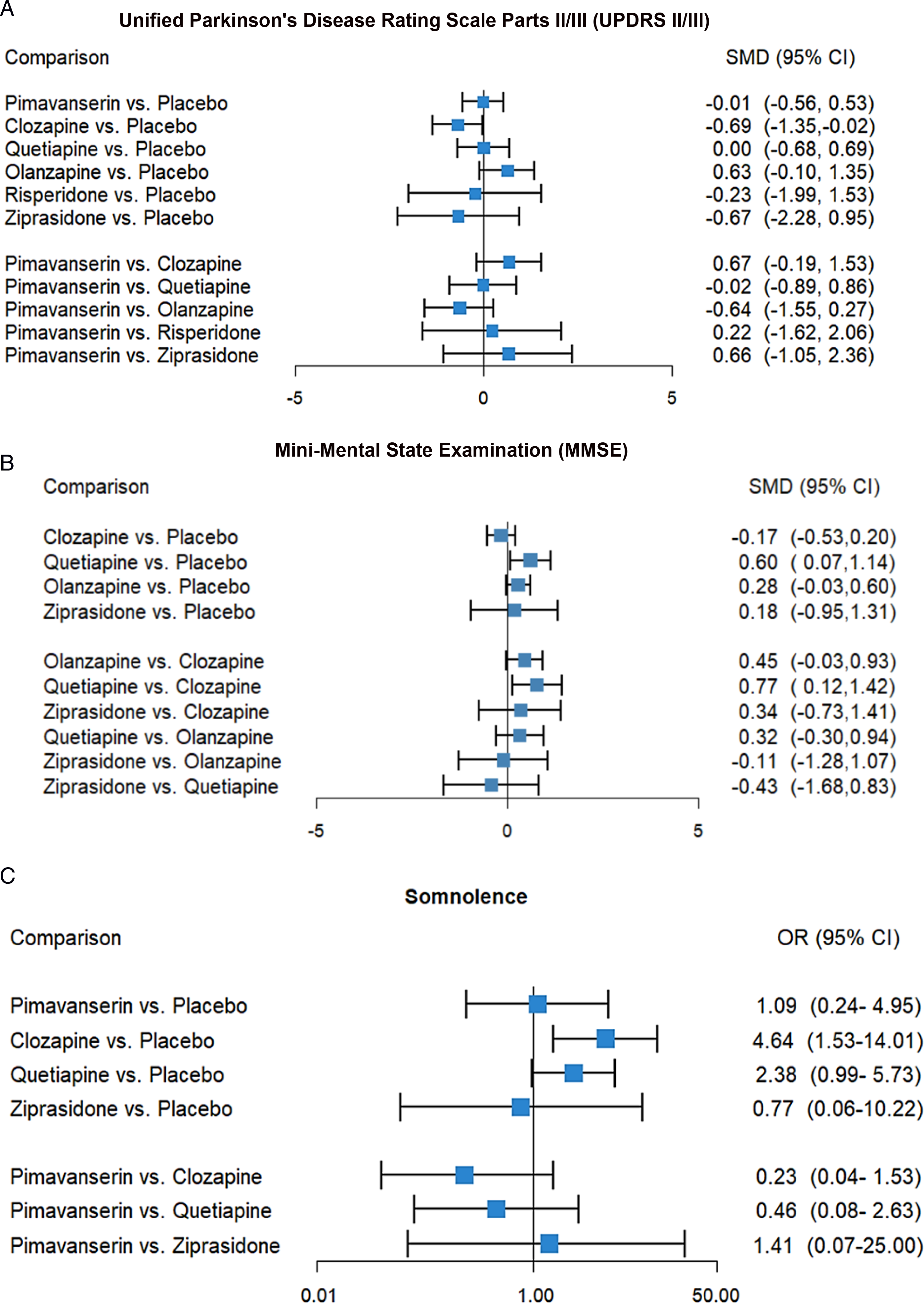
Mini-Mental State Examination
Seven eligible studies53,64,66-68,70 (n = 349) were included in the NMA of MMSE outcome. Supplementary figure 3 (b) depicts the network diagram for the MMSE outcome
Somnolence
Ten eligible studies55,58,60,62,66,69 (n = 442 patients) were included in the NMA of somnolence outcome. Supplementary figure 3(c) depicts the network diagram for somnolence. Compared with placebo, clozapine (OR, 4.64; 95% CI, 1.53, 14.01), and quetiapine (OR, 2.38; 95% CI, 0.99, 5.73) had higher odds of somnolence (Figure 3c). When compared with each other, pimavanserin had numerically lower odds of somnolence than clozapine (OR, 0.23; 95% CI, 0.04, 1.53) and quetiapine (OR, 0.46; 95% CI, 0.08, 2.63) (supplementary table 3b). SUCRA showed that olanzapine (91.8%) had the highest probability of being safe in avoiding somnolence (supplementary figure 7c).
Acceptability Outcomes
Discontinuations due to Adverse Events
Seventeen eligible studies53-56,58-63,65,67-71 (n = 1,205 patients) were included in the NMA of discontinuation due to AE outcome. Supplementary figure 4 (a) depicts the network diagram for discontinuation due to AEs. Compared with placebo, clozapine (OR, 1.60; 95% CI, 0.53, 4.85), olanzapine (OR, 8.48; 95% CI, 2.56, 28.03), pimavanserin (OR, 1.44; 95% CI, 0.68, 3.04), and quetiapine (OR, 1.25; 95% CI, 0.47, 3.36) had higher odds of discontinuation due to AEs, while risperidone (OR, 0.60; 95% CI, 0.03, 12.80) had lower odds of discontinuation due to AEs (Figure 4a). Olanzapine was associated with significantly higher odds of discontinuation due to AEs than clozapine (OR, 5.30; 95% CI, 1.16, 24.25) Forest Plots for Acceptability Outcomes of Atypical Antipsychotics in Comparison with Drug Comparators. (A) Forest plot for Discontinuations due to adverse events, representing pooled odds ratio comparing each treatment option with placebo or drug. The blue boxes denote the point estimate for each treatment, while the horizontal line denoted the 95% CI. If the 95% CI does not cross 1 (null value); the results imply statistical significance (B) Forest plot for Discontinuations due to lack of efficacy, representing pooled odds ratio comparing each treatment option with placebo. The blue boxes denote the point estimate for each treatment , while the horizontal line denoted the 95% CI. If the 95% CI does not cross 1 (null value); the results imply statistical significance (C) Forest plot for All-cause discontinuations representing pooled odds ratio comparing each treatment option with placebo. The blue boxes denote the point estimate for each treatment , while the horizontal line denoted the 95% CI. If the 95% CI does not cross 1 (null value); the results imply statistical significance.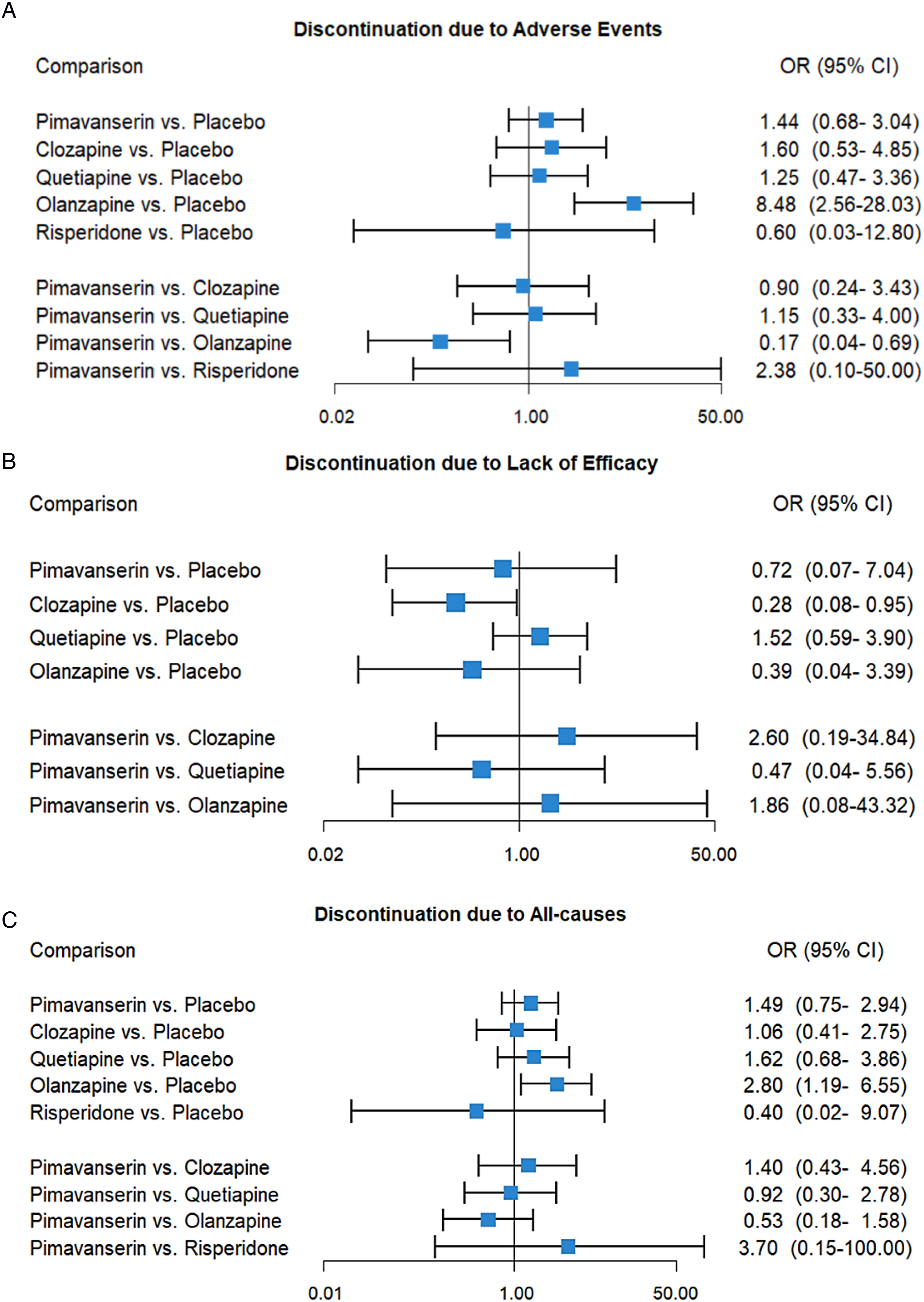
Discontinuation due to Lack of Efficacy
Ten eligible 10 studies55,58,59,61,63-65,67,68,70 (n = 657 patients) were included in the NMA of discontinuation due to lack of efficacy outcome. Supplementary figure 4 (b) depicts the network diagram for discontinuation due to lack of efficacy outcome. Compared with placebo, clozapine (OR, 0.28; 95% CI, 0.08, 0.95), olanzapine (OR, 0.39; 95% CI, 0.04, 3.39), and pimavanserin (OR, 0.72; 95% CI, 0.07, 7.04) had lower odds of discontinuation due to lack of efficacy (Figure 4b). SUCRA showed that clozapine (83.9%) was the most acceptable
Discontinuation due to All Causes
Eighteen eligible studies52-56,58-65,67-70 (n = 1236) were included in the NMA of discontinuation due to all causes. Supplementary figure 4 (c) depicts the network diagram for discontinuation due to lack of efficacy. Olanzapine (OR, 2.80; 95% CI, 1.19, 6.55) had significantly higher odds of discontinuation due to all causes than placebo (Figure 4c). Clozapine (OR, 1.06; 95% CI, 0.41, 2.75), pimavanserin (OR, 1.49; 95% CI, 0.75, 2.94), and quetiapine (OR, 1.62; 95% CI: 0.68, 3.86) were not associated with a significant increase in the odds of discontinuation due to all causes. SUCRA ranking suggested that risperidone (78.3%) was the most acceptable based on discontinuation due to all causes, followed by placebo (65.8%) (supplementary figure 8c).
Simultaneous Treatment Ranking
Figure 5a presents the ranking of the 5 AAPs according to SUCRA values for efficacy and safety outcomes. Cluster ranking for CGI-S (efficacy) vs. UPDRS (safety) demonstrated pimavanserin and clozapine were most efficacious and most safe (upper right quadrant; most efficacious/most safe), with pimavanserin having the greatest probability of being efficacious. Olanzapine was the least efficacious, with placebo falling into the same cluster (lower left quadrant; less efficacious/less safe). (A) Clustered Ranking Plots of Networks Based on SUCRA Values for Two Outcomes: Efficacy vs. Safety. Each color represents a group of treatments that belong to the same cluster Treatments that fall in the upper right corner are more efficacious and safer than the other treatments. (B) Clustered Ranking Plots of Networks Based on SUCRA Values for Two Outcomes: Efficacy vs. Acceptability, CGI-S vs. Discontinuation due to AE. Each color represents a group of treatments that belong to the same cluster. Treatments that fall in the upper right corner are more efficacious and more acceptable than the other treatments. (C) Clustered Ranking Plots of Networks Based on SUCRA Values for Two Outcomes: Efficacy vs. Acceptability, CGI-S vs. Discontinuation due to Lack of Efficacy. Each color represents a group of treatments that belong to the same cluster. Treatments that fall in the upper right corner are more efficacious and more acceptable than the other treatments. (D) Clustered Ranking Plots of Networks Based on SUCRA Values for Two Outcomes: Efficacy vs. Acceptability, CGI-S vs. Discontinuation Due to All-Causes. Each color represents a group of treatments that belong to the same cluster. Treatments that fall in the upper right corner are more efficacious and more acceptable than the other treatments.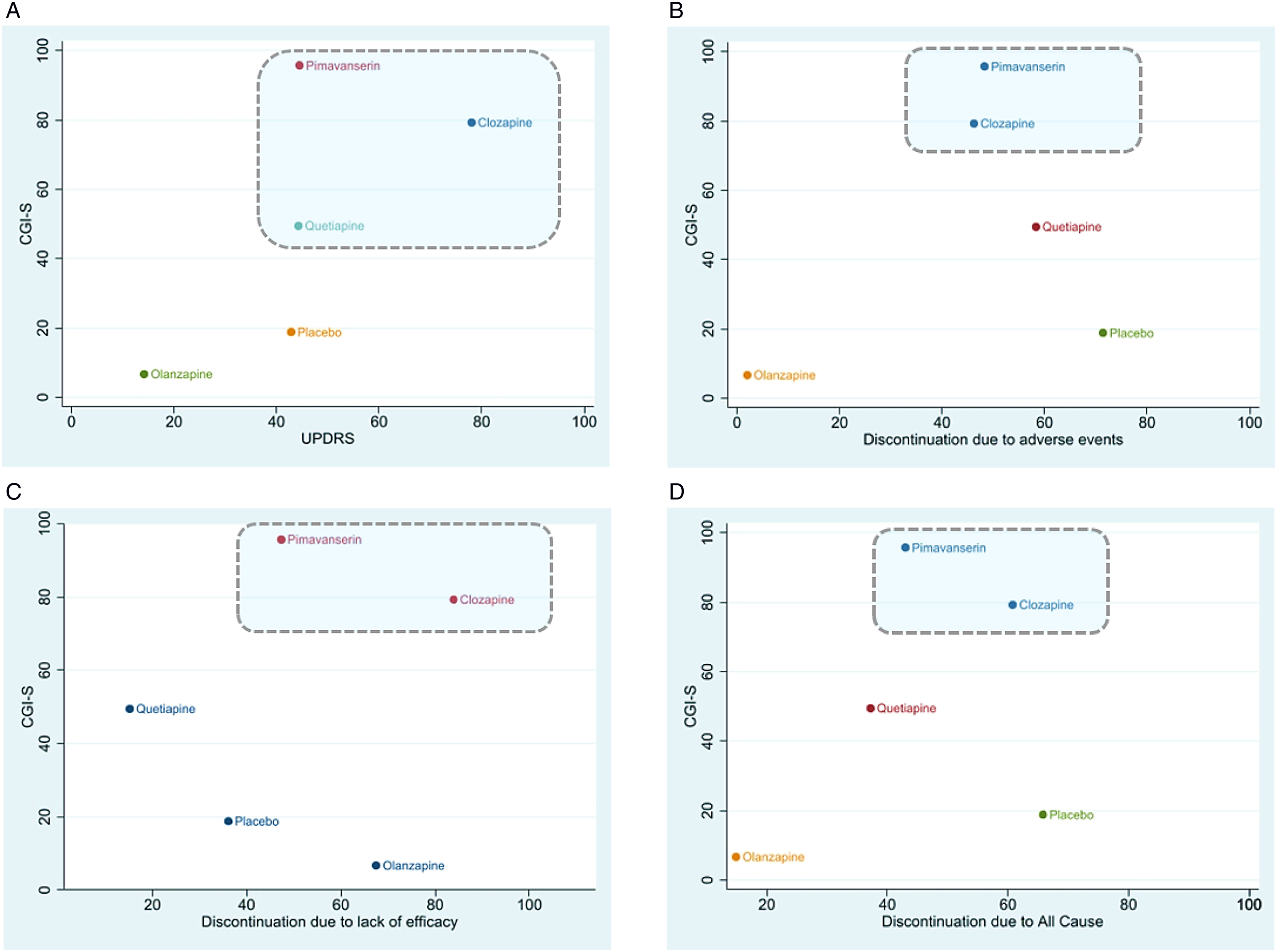
Simultaneous ranking of 5 AAPs for efficacy (CGI-S) vs. acceptability based on discontinuation due to AEs demonstrated that pimavanserin and clozapine were the most efficacious and acceptable (upper right quadrant; most efficacious/most acceptable) (Figure 5b). Placebo was the most acceptable (lower right quadrant; less efficacious/most acceptable). Similarly, for CGI-S vs. discontinuation due to lack of efficacy (Figure 5c) demonstrated that pimavanserin and clozapine were the most efficacious and acceptable. Finally, simultaneous ranking for CGI-S vs. discontinuation due to all causes (Figure 5d) showed that placebo was the most acceptable but less efficacious. Olanzapine was the least acceptable and least efficacious, with quetiapine falling in the same (lower left quadrant; less effective/less efficacious) cluster.
Discussion
Principal Findings
Although clozapine has historically been considered the most efficacious drug in controlling the symptoms of PDP, this study found for the first time that pimavanserin had the most favorable effect size based on two efficacy outcomes (CGI-S and SAPS-PD). Even though the point estimate suggested that pimavanserin possibly reduce psychosis relative to clozapine, it is important to note that the confidence intervals included a benefit of clozapine. Pimavanserin significantly improved psychosis when compared with quetiapine and olanzapine. The study also found that clozapine, pimavanserin, and quetiapine were not associated with worsening motor symptoms of PD.
Clozapine and quetiapine were associated with the greatest odds of somnolence; clozapine had the highest odds of somnolence when compared with placebo, olanzapine, quetiapine, and ziprasidone. Our results suggest that pimavanserin had lower odds of somnolence than clozapine and quetiapine. Among AAPs, quetiapine was most likely to be discontinued due to lack of efficacy and significantly worsened cognition. Olanzapine was the least acceptable AAP with the greatest odds of being discontinued due to all causes and due to AEs. Overall, this study's results support and add critical data to existing studies and clinical practice guidelines for treating patients with PDP.
Comparison with Other Studies
Using an exhaustive search of relevant literature on the use of AAP in persons with PDP to date, this study included more studies than all previous pairwise or NMAs. As a result, it examined broader outcomes than previous studies. Consistent with an earlier NMA by Iketani et al., 19 the current study found clozapine, pimavanserin, and quetiapine are associated with significant improvement in symptoms based on CGI-S, without worsening of motor symptoms. The magnitude of the improvement in psychosis for clozapine was the largest of the drugs studied in Iketani; in the current study, the pimavanserin effect size was the largest. The difference in the magnitude of effects might be related to the fact that Iketani estimated non-standardized mean differences while this study estimated SMDs. Also, the current study included 4 more studies than Iketani, which used a Bayesian approach with priors that are not informative for patients with PDP.
Although previous studies examined discontinuations due to AEs, the current study is the first to also examine discontinuation due to all causes and lack of efficacy. Consistent with the previous studies, we found that olanzapine was associated with discontinuation due to AEs. In addition, we found that olanzapine was associated with significantly greater odds of discontinuation due to all causes.
Interestingly, the significant improvement found in psychosis symptoms when comparing pimavanserin vs. placebo based on SAPS-PD corroborates the recent pairwise meta-analysis by Mansuri et al. We used MAIC, however, to enable us to compare pimavanserin with other AAPs and found that pimavanserin numerically improves psychosis symptoms relative to clozapine and quetiapine. Similar to the current study, previous NMA and pairwise meta-analyses14,19 reported numerical improvements in psychotic symptoms (in terms of BPRS scores) for clozapine, olanzapine, risperidone, and ziprasidone, but quetiapine increased the BPRS scores, indicating a worsening effect on psychotic symptoms. The impact of pimavanserin on BPRS scores was not evaluated in the current study or in previous studies because trials of pimavanserin in patients with PDP did not report data on the BPRS outcome. Consistent with all previous studies, we did not find evidence that pimavanserin impairs PD's motor functions. Its lack of impact on motor function might be related to the fact that it does not induce clinically significant antagonism of adrenergic, dopaminergic, histaminergic, or muscarinic receptors. 72
Implications for Clinicians and Policymakers
Although clozapine is an efficacious treatment option, its use requires periodic intensive ANC monitoring, as mandated by the US FDA’s Risk Evaluation and Mitigation Strategy, because of the risk of life-threatening neutropenia. 73 This requirement has been found to pose a barrier to its use by clinicians and patients. In some treatment facilities, including all US Veteran Affairs medical centers, approval may be needed before clozapine can be prescribed, which may delay treatment initiation. 74
Despite the lack of strong evidence to support the efficacy of quetiapine and its significant risk of clinically meaningful AEs, it is the most used off-label AAP for treating PDP. Based on findings from the current study, quetiapine can induce excessive sleepiness and significantly impair cognition and may need to be avoided in PD patients with sleep problems and severely reduced cognitive ability. With risperidone being the most acceptable AAP in terms of discontinuation due to all causes, the lack of evidence to support its efficacy in improving psychosis and safety on motor function suggested that it is not an ideal option for patients with PDP.
Evidence from this study suggests that pimavanserin should be the first drug considered in patients with PDP because it showed improvement in psychosis without impairing motor function and demonstrated a more favorable safety profile. However, clinical practice guidelines and recommendations vary. The UK's National Institute for Health and Care Excellence (NICE) guideline recognized the possible detrimental effect of quetiapine on cognition, recommending that quetiapine be considered only in the treatment of psychosis in persons with PD who have no cognitive impairment.75,76 However, given that cognitive impairment is common among persons with PD, with a prevalence of 30-40%,77-79 both the NICE recommendation and the evidence from the current study suggest that before considering quetiapine treatment, clinicians should consider a drug that has more robust evidence of efficacy and does not impair cognition. 80
In its updated review of treatments for non-motor symptoms of PD, the Movement Disorder Society (MDS) determined that clozapine and pimavanserin are “clinically useful” in treating PDP and that, given insufficient evidence of its efficacy, quetiapine is “possibly useful”. 16 In contrast, the American Academy of Neurology review of PD's quality measurement set indicated that clozapine and quetiapine were effective without significantly worsening motor symptoms. 81 The Canadian guideline for PD suggested that pimavanserin could be considered in treating PDP and concurred with the MDS suggestion of the usefulness and possible usefulness of clozapine and quetiapine, respectively. 82 Evidence from the current study of pimavanserin's greater efficacy and favorable safety and acceptability profile, however, suggests that clozapine and quetiapine in patients with PDP should be considered only in situations where pimavanserin is contraindicated (such as in patients with a history of a hypersensitivity reaction to pimavanserin or any of its components). 83 It is also important to note that, as with other antipsychotics such as quetiapine, 84 pimavanserin is also associated with an increased risk of corrected QT interval (QT) prolongation and serious arrhythmia (abnormal heart rhythm). Therefore, we emphasize that, despite being efficacious, pimavanserin should be avoided in patients with risk factors for prolonged QT interval, and its concomitant use with drugs that prolong QT should also be avoided. 83
The MDS categorized other antipsychotics as having unacceptable risk due to risks of worsening parkinsonism. As evidenced by olanzapine's lesser effect size for UPDRS outcome, the present study's findings support the MDS categorization. Furthermore, in the study, olanzapine was associated with significantly greater odds of discontinuation due to AEs than placebo, and pimavanserin was associated with significantly lower odds than olanzapine. These findings suggest that olanzapine, with no evidence of efficacy, should be avoided in persons with PDP.
The 2019 update of the American Geriatrics Society Beers Criteria for Potentially Inappropriate Medication Use in Older Adults recommended avoiding APs, except for quetiapine and pimavanserin, in older adults with PD, 85 due to potential worsening of movement disorders. Although the current study did not find evidence that quetiapine worsens motor function, it showed that it is significantly associated with other AEs and that, especially in patients without contraindications for pimavanserin, quetiapine may need to be avoided. In 2018, the most recent European guidelines (version 2) for prescribing medication to older adults, STOPP (Screening Tool of Older Person's Prescriptions) and START (Screening Tool to Alert to Right Treatment) recommended only quetiapine in older adults with movement disorders and did not recommend pimavanserin. Future updates to the STOPP and START criteria should reflect the current evidence of pimavanserin's lack of deleterious impact on motor function. 86
Strengths & Limitations
This study provides the most up-to-date, comprehensive synthesis of the evidence of efficacy, safety, and acceptability of AAPs in treating PDP. The NMA simultaneously compared AAPs across a wide range of outcomes that, to our knowledge, no previous clinical trial, observational study, pairwise meta-analysis, or NMA compared. Previous studies could not compare AAPs-based SAPS-PD/H+D due to the lack of a common comparator. To circumvent this limitation and provide a comprehensive evaluation of the efficacy and safety of AAPs, this study used the MAIC approach to compare the efficacy of pimavanserin vs. other AAPs with available data on SAPS-PD/H+D. This study estimates AEs with greater statistical power than individual trials that are powered primarily to detect differences in efficacy but not in safety outcomes. 87
Despite its strengths, this study has some limitations. Some of the included studies did not evaluate certain outcomes, and hence we could not provide evidence of efficacy, safety, or acceptability in all outcomes for some drugs. 88 For example, we did not examine pimavanserin using BPRS and MMSE because there was no relevant data on the outcomes. For the same reason, quetiapine and risperidone were not evaluated in clinical trials using the SAPS-PD/H+D scales, and risperidone and ziprasidone were not assessed using CGI-S.
Even though the NMA included 19 studies from an SLR that extensively reviewed all available potentially relevant studies, we believe that adding more studies, if available, would have improved the precision of some estimates that featured wide CIs. The wide CIs might be due to the small number of patients in individual studies and the absolute number of events. As demonstrated by Brozek (2008), we believe both factors contributed to wide CIs and that CIs become narrower when the number of events increases. 89 These wide CIs led to estimates that included values where there are no statistical differences (CI crossing 0 for continuous outcomes and crossing 1 for binary outcomes) between some drugs being compared, and either a benefit or lack of it was possible. Although ranking by SUCRA utilizes the point estimates and 95% CIs to estimate treatment ranks via bootstrapping, it does not take into account statistical significance and therefore should be interpreted cautiously.90,91 Due to the lack of consistency in the doses of AAPs used across the included studies and comparisons, we could not provide comparisons by dose. Instead, we reported estimates representing the average dose for each medication. Moreover, in real-life practice, some AAPs are initiated in low doses and then increased based on patient response; such granular information is unavailable in most of the included trials.
This study is amenable to the drawbacks of NMAs in that its conclusions depend on the validity of the evidence used and the underlying statistical assumptions it made. The strong and frequently challenging intrinsic statistical assumptions and the reliability of the evidence employed in the NMA make these assumptions difficult to satisfy. To get reliable and practical findings, certain conditions must be satisfied. Considering this, we took a comprehensive, cautious, and conservative approach when analyzing and assessing the NMA data. In this study, there are no closed/triangular loops for some comparisons because some drugs were not head-to-head in trials; as such, we were unable to assess consistency but accounted for possible inconsistency. We recommend future trials consider a head-to-head comparison of antipsychotics. This way, the reliability of assumptions, such as consistency, will be improved.
Conclusions
In this study, pimavanserin demonstrated improvement in symptoms of PDP and did not impair PD motor function. Although clozapine also improved symptoms of psychosis and did not worsen PD's motor functions, it was more likely than pimavanserin to be discontinued due to AEs, and it requires intensive ANC monitoring. In addition, the NMA did not find strong evidence to suggest that quetiapine was more efficacious, safe, and acceptable than clozapine and pimavanserin. Quetiapine was significantly associated with a decline in cognition. Therefore, the current evidence suggests that clinicians should avoid the use of quetiapine in patients with evidence of reduced cognitive abilities.
Supplemental Material
Supplemental Material - Comparative Efficacy, Safety, and Acceptability of Pimavanserin and Other Atypical Antipsychotics for Parkinson’s Disease Psychosis: Systematic Review and Network Meta-Analysis
Supplemental Material for Comparative Efficacy, Safety, and Acceptability of Pimavanserin and Other Atypical Antipsychotics for Parkinson’s Disease Psychosis: Systematic Review and Network Meta-Analysis by Ismaeel Yunusa, Nazia Rashid, Roxanna Seyedin, Deepika Paratane, and Krithika Rajagopalan in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
All authors made substantive contributions to the study and results interpretation for this work. Ismaeel Yunusa, Nazia Rashid, Roxanna Seyedin, Deepika Paratane, and Krithika Rajagopalan developed the concept and study design; Ismaeel Yunusa, Nazia Rashid, Roxanna Seyedin, Deepika Paratane, and Krithika Rajagopalan worked on study selection, and interpretation of data; Ismaeel Yunusa, Nazia Rashid, Roxanna Seyedin, Deepika Paratane, and Krithika Rajagopalan worked on preparation of manuscript; All authors critically reviewed and approved the final version of the paper.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Acadia Pharmaceuticals Inc. Employees of Acadia Pharmaceuticals Inc. were a part of the research team for development of concept, study design, study selection and interpretation of the results.
Disclosures
Nazia Rashid is an employee of Acadia Pharmaceuticals, Inc. which has funded the research. Roxanna Seyedin, Deepika Paratane, and Krithika Rajagopalan are employees of Anlitiks, Inc. The authors confirm that funding has in no way influenced the outcome. There are no other conflicts of interest associated with this publication.
Transparency Declaration
The guarantor affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained
Availability of Data and Material
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.