
Abstract
Background
Subjective cognitive complaints are generally poorly associated with objective memory functioning in older persons. Subjective cognitive decline (SCD) is a key feature in SCD and amnestic mild cognitive impairment (aMCI) which both can represent early Alzheimer’s disease (AD). The aim of this study was to assess how memory clinic patients with SCD, MCI and mild AD dementia scored on 3 different complaint measures and if the format of assessment had an impact on the association with cognitive functioning, age, and depressive symptoms.
Methods
We included 17 SCD patients, 17 aMCI patients, 17 patients with mild AD, and 30 controls. Complaints were assessed with the Cognitive Change Index (CCI), the Subjective Memory Complaints (SMC) scale, and the Memory Complaint Questionnaire (MAC-Q).
Results
There were no significant differences between the total scores in the patient groups on the questionnaires. However, significant differences were found in the number of patients classified with impairment when using the CCI, the SMC, and the MAC-Q. Scores on all questionnaires were significantly associated with depressive symptoms, and significant associations with age, gender, and Addenbrookes Cognitive Examination score were found for the SMC. In patients with cognitive dysfunction, lower memory awareness significantly predicted fewer cognitive complaints.
Conclusions
SCD patients in a memory clinic setting report the same degree of cognitive impairment as patients with aMCI and mild dementia, and in a hospital-based cohort we extend previous findings from healthy controls, that definition of SCD may depend on the format of assessment.
Keywords
Introduction
An increasing number of individuals seek medical attention due to concerns about cognitive dysfunction, but subjective cognitive complaints are not necessarily associated with poor objective test performances. 1 Subjective complaints are related to several factors such as affective symptoms, personality traits, age, medical disorders, and medication use.2,3 Subjective cognitive complaints are often referred to as subjective cognitive decline (SCD) which is a complex, multidimensional construct influenced by several factors and it may be a preclinical marker of later Alzheimer’s disease (AD). 1 The severity of cognitive complaints in SCD patients with help-seeking behavior is linked to a higher risk of preclinical AD.1,2
Cognitive complaints can be assessed using various methods including open-ended questions, 4 semi-structured interviews, 5 or questionnaires, which can be self-report 6 or informant based. 7 Important differences in assessment may also be found depending on whether a person compares memory functioning to a previous level or to age matched peers. 8 Some questionnaires only include items about memory, while other scales also investigate other cognitive functions. Previous studies on SCD have predominantly assessed complaints in samples with healthy older adults.8–11 However, as some people have help-seeking behavior and are referred to memory clinics there is unmet need to investigate the degree and frequency of complaints in SCD patients diagnosed in a memory clinic setting. Further, it is unknown if the degree of complaints is different in SCD, MCI and AD, but a previous study suggest that self-report becomes less accurate as AD progresses. 12
Results from a mixed memory clinic cohort has previously shown that different measures of cognitive complaints are not interchangeable since some have associations with variables as age whereas others do not. 13 However, it has not yet been investigated whether a selection of self-report scales designed to assess cognitive complaints would lead to different associations with variables as depression, age or cognitive status in a group of patients on the AD continuum (including both MCI and mild AD dementia patients). Thus, the convergent validity of different types of subjective measures for cognitive dysfunction is not sufficiently studied in memory clinic patients.
The aim of this study was to investigate whether scores on scales assessing subjective cognitive complaints differed in memory clinic patients with SCD, aMCI, and mild dementia due to AD when 3 different quantitative scales were applied. Further, we aimed to investigate the association between these scales and study to which degree results from these scales were associated with age, depressive symptoms, gender, and cognitive impairment in patients with SCD, aMCI and mild dementia due to AD.
Materials and Methods
Participants
In this study, patients with SCD (n = 17), aMCI (n = 17), and mild dementia due to AD (n = 17) were recruited from the Memory Clinic at the Danish Dementia Research Centre. All patients had undergone clinical assessment including a physical and neurological examination, routine laboratory tests, structural brain imaging, testing with the Mini-Mental State Examination (MMSE) and Addenbrooke’s Cognitive Examination (ACE), 14 and a neuropsychological evaluation. The inclusion process and the neuropsychological battery was previously described. 15 Three memory tests were applied – of which one was the Rey Auditory Verbal Learning Task (RAVLT). All patients were examined for one or more AD biomarkers (CSF Aβ42, CSF p-tau, PiB-PET standardized uptake value ratio, FDG-PET glucose metabolism pattern, and/or medial temporal atrophy). A syndromic and etiological diagnosis was established on a multidisciplinary consensus conference in accordance with international diagnostic guidelines (specified below). A control group with 30 volunteering, healthy participants was also recruited. Controls were not examined for AD biomarkers.
Ethical Approval
The project was evaluated by the local Ethic committee of the Capitol Region of Denmark and the inclusion of patients (and examinations as described) was approved (journal number H-18048977).
Inclusion and Exclusion Criteria
Participants had to be at least 45 years and have Danish as their native language. Exclusion criteria for all groups were: (1) presence of (other) neurological, somatic, or psychiatric disorders that could significantly affect cognition; (2) ongoing alcohol or substance abuse (according to national health recommendations); and (3) use of medication known to affect cognition. The Geriatric Depression Scale with 15 items (GDS-15) and a cut-off score of ≥ 5 was applied to screen for depression.
Group Specific Criteria
Patients with MCI were diagnosed in accordance with the guidelines by The National Institute of Aging and the Alzheimer’s Association (NIA-AA). 16 MCI was operationalized as: (1) significant impairment in one or more cognitive domains; (2) concerns about change in cognitive functioning expressed by the patient or an informant; and (3) no impairment of activities of daily living (as measured by the Functional Activities Questionnaire). 17 All MCI patients were required to have amnestic cognitive profiles (aMCI), with impairments on at least one memory test.
Patients with mild dementia due to AD were also diagnosed based on NIA-AA criteria 18 and had: (1) significant impairments representing a change from an earlier level of functioning in at least 2 cognitive domains; and (2) impaired activities of daily living. The patients with mild dementia had MMSE scores ≥ 24 and at least one abnormal AD biomarker.
The SCD patients fulfilled the criteria presented by the SCD Initiative working group: 1 They had (1) SCD unrelated to an acute event; and (2) normal age-, gender-, and education-adjusted performances on standardized cognitive tests. The patients had all been referred to the Memory Clinic for a diagnostic evaluation and had therefore expressed subjective concerns of memory impairment as well as help-seeking behavior. Since the patients had worries associated with SCD, help-seeking behavior, and specific memory complaints, they had at least 3 of the SCD-plus features listed in Jessen et al. 1 The controls were excluded if they expressed: (1) concerns associated with SCD; or (2) feelings of impaired memory compared to others of the same age (as reflected on the 12th item on the CCI-S). Controls had neuropsychological test performances on expected level based on age-, gender-, and education-adjusted norms.
Assessment of Cognitive Complaints
In a visit separate from the neurological and the neuropsychological evaluation, Danish adaptations of 3 questionnaires inquiring about subjective cognitive symptoms were applied. These scales were all developed to assess feelings of memory decline. The scales were administered in an interview format and in a fixed order. No neuropsychological testing of memory was performed prior to the interviews.
The Subjective Memory Complaints Scale. 19
The SMC contains 10 questions where 5 concern memory difficulties, while the last 5 items assess problems with word finding, orientation, thinking, and concentration. The questionnaire focuses on current difficulties and does not require respondents to compare their current state to a previous level of functioning. Each item is given a score of 0-1, 0-2 or 0-3, and the highest possible total score is 21.
The Memory Complaint Questionnaire. 20
This scale has 6 items in which respondents are asked to compare their current memory abilities with their memory abilities when they were young (in this adaptation, subjects are asked to compare to when they were 20 years old). 13 The first 5 questions inquire about changes in the ability to remember specific details from daily-life situations. The last question asks for an overall evaluation of change in memory function. Each item is rated on a 5-point scale from “Much better now” to “Much worse now”. The total score range is 7 to 35. Internal consistency (Cronbach’s alpha) was 0.57 in the original validation. 20
The Cognitive Change Index – Self Report Version. 21
The CCI-S has 20 items of which 12 concern experiences of memory decline. The remaining 6 items investigate decline in executive functions, language, and attention. Respondents are asked to compare their current abilities with their abilities 5 years ago and to rate the change on a 5-point scale from “No change” to “Much worse”. The total score range is 20 to 100. Internal consistency (Cronbach’s alpha) was 0.96 in the original validation.
Estimation of Awareness of Memory Function
An estimation of awareness of memory deficits was applied in accordance with the method presented in Vannini et al. 22 We used the score from the SMC and a combined RAVLT score (a total of the A1-A5, A6, and A7 performance). For each subject, the raw objective and subjective memory scores were converted into z-scores. Since higher scores on the RAVLT indicate a good performance, while higher SMC scores indicate a negative outcome (many complaints), the subjective memory z-scores had to be reversed. The reversed subjective memory z-score was then subtracted from the non-reversed objective memory z-score to create a delta score (the memory awareness score).
Statistical Analysis
Group comparisons were performed using one-way analysis of variance and Dunnett’s post hoc test if assumptions of homogeneity of variance and normality were met. When the assumption of homogeneity of variance was not met, the Welch t-test or the Welch F test followed by Dunnett’s T3 post hoc test were applied. The Kruskal-Wallis test and Dunn’s post hoc test were applied if the assumption of normality or both assumptions were violated. All nonparametric post hoc analyses were corrected for multiple comparisons using the Bonferroni-Holm procedure (adjusted P values are noted as Padj). Pearson’s Chi-Square test was used to investigate the significance of differences in gender distribution and in the frequency of patients in each group with abnormal complaint scores. Correlation analyses were performed using Spearman’s Correlation Coefficient. The Cochran Q test and Dunn’s post hoc test were used to assess whether frequencies of impairment on the SMC, MAC-Q, and CCI-S scales were significantly different. Differences were considered significant at an alpha level below .05.
Results
Background Data, Cognitive Status, and Mood
Background Data and Results of the Cognitive and Neuropsychiatric Screening Tests for the Patient and Control Groups. Age is Presented as Mean (SD), While the Results from GDS-15, MMSE, and ACE are Presented as Median [Range].
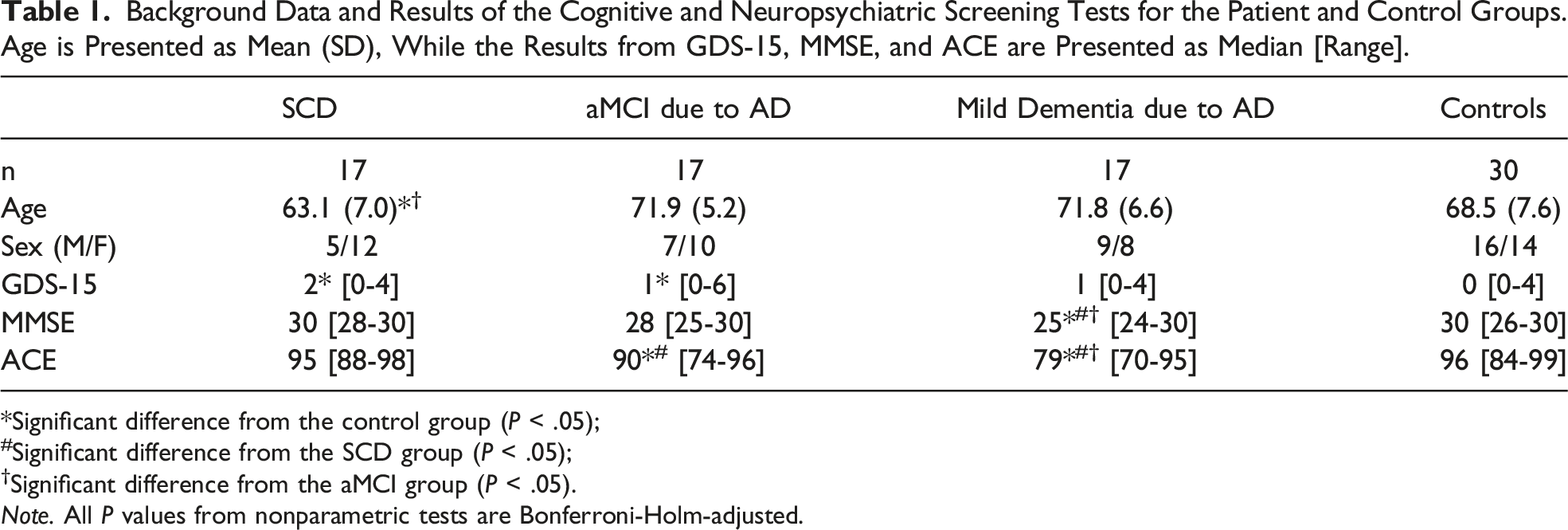
*Significant difference from the control group (P < .05);
#Significant difference from the SCD group (P < .05);
†Significant difference from the aMCI group (P < .05).
Note. All P values from nonparametric tests are Bonferroni-Holm-adjusted.
Subjective Cognitive Complaints Score in Patients and Controls
Scores on SMC, MAC-Q, and CCI-S for the Patient and Control Groups. The Results from SMC and CCI-S are Presented as Mean (SD), While Results from MAC-Q are Presented as Median [Range].
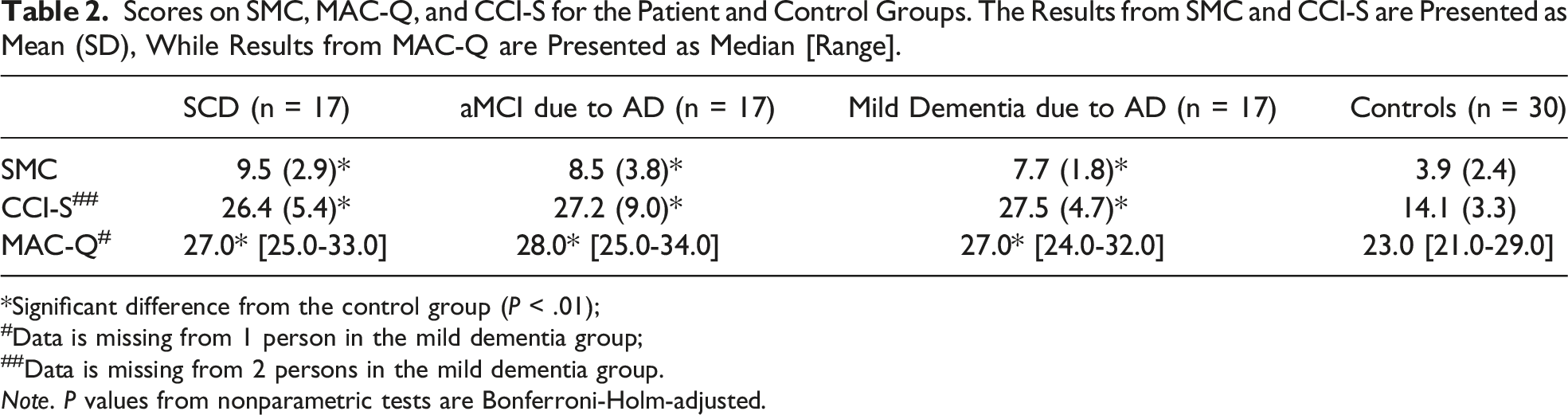
*Significant difference from the control group (P < .01);
#Data is missing from 1 person in the mild dementia group;
##Data is missing from 2 persons in the mild dementia group.
Note. P values from nonparametric tests are Bonferroni-Holm-adjusted.
Frequencies of Abnormal Cognitive Complaint Scores (as Measured on the SMC, MAC-Q, or CCI-S) in the 3 Patient Groups.
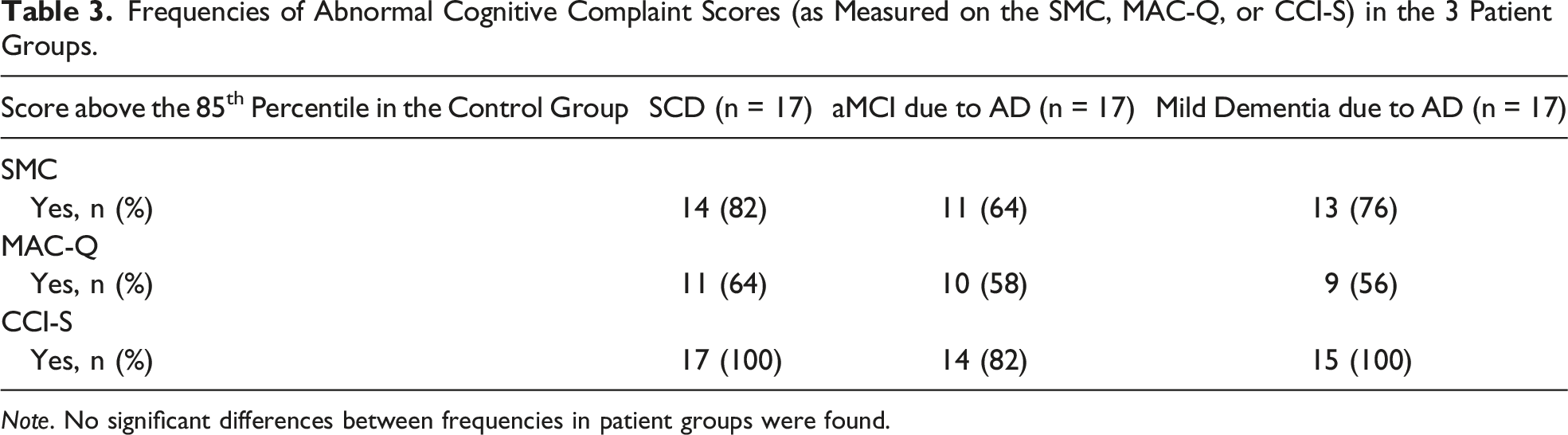
Note. No significant differences between frequencies in patient groups were found.
Association between Subjective Cognitive Measures and Mood, Cognitive Status, and Gender
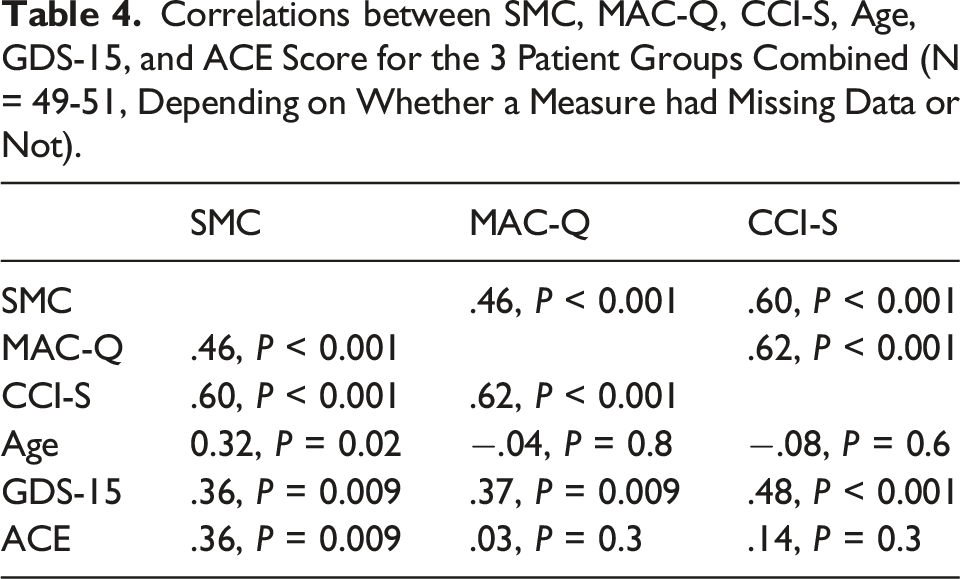
Correlations between SMC, MAC-Q, CCI-S, Age, GDS-15, and ACE Score for the 3 Patient Groups Combined (N = 49-51, Depending on Whether a Measure had Missing Data or Not).
Subjective Memory Complaints and Memory Awareness
In combined group of the aMCI and the mild dementia patients, significant correlations between the memory awareness score and scores on the CCI-S, rho = 0.55, P < .01, and the MAC-Q, rho = 0.67, P < .001, were found. There was no significant difference in the memory awareness scores between the aMCI and mild dementia groups. The percentage of participants with impaired awareness of deficits (a memory awareness score below zero) was 23.5% in the aMCI group and 25% in the mild dementia group.
Discussion
Using 3 different cognitive complaint questionnaires in patients from a memory clinic cohort, we found that patients with SCD had as many subjective cognitive symptoms as patients with aMCI and mild dementia due to AD. Memory complaints are the key symptom in SCD, but few studies have investigated the magnitude of such complaints in memory clinic patients and the results from this study adds to existing knowledge on the characterization of cognitive complaints in SCD. Our results are consistent with findings recently described in Ryu et al. 7 There can be a lot of reasons why individuals report cognitive complaints other than actual symptoms and other variables (eg, personality factors, family history of dementia, mood symptoms) could have contributed to the finding that individuals with SCD reported equal level of/severity of complaints as patients with aMCI and AD. However, that SCD patients in a memory clinic setting have as many cognitive complaints as patients with aMCI and mild dementia due to AD is a clinically relevant finding, and some studies suggests that more severe complaints in SCD are associated with higher risk of amyloid pathology and clinical progression.23,24
Degree and type of complaints in SCD have been studied in some studies, but they have typically assessed healthy persons not referred to assessment in memory clinics. These studies show that the definition of SCD have an impact on the association between cognitive decline and atrophy patterns, 25 and that rates of SCD may vary as a function of the assessment format. 10 Different SCD phenotypes have been suggested, and these are characterized by different syndromic and biomarker profiles, and by comparing both data-driven and clinical approaches results indicate that clinical approach alone may lack specificity. 9 Prognostic value of SCD for later MCI diagnosis seem to improve if associated worry and consistency of SCD are assessed. 11
To investigate if different measures of SCD would yield different results in our patient groups, we applied 3 questionnaires that were all frequently used in previous studies of cognitive complaints.3,6,13,26–29 The observation that 1 patient can have an abnormal score on 1 cognitive complaint measure while scoring within the normal range on another, suggests that subjective complaints is not an easily defined or delineated phenomenon, and that different questionnaires developed to assess subjective cognitive impairment only to some degree capture the same phenomenon. Further, the correlations between the CCI-S, the SMC, and the MAC-Q were not very large. There is no gold standard definition of how to assess subjective cognitive impairment, but our results show that the convergent validity of these scales may be limited. Thus, these results may to some degree raise more questions than provide answers and combined with recent results from other studies on the assessment format of complaints in early AD and SCD there seem to be a need to try to find a consensus as to which format is most relevant for the assessment of subjective complaints since it may have important implications for the definition of SCD. Recently, findings from a longitudinal memory clinic based study have suggested that a semi-structured interview approach relying on a combination of open and fixed questions concerning different cognitive domains may be useful in the early identification of SCD due to preclinical AD, 5 while other studies have highlighted that significant differences may be found depending on whether a person compares memory functioning to a previous level or to age matched peers. 8
The scales applied in this study all ask questions about cognitive function in a retrospective perspective. The SMC and the MAC-Q have previously been applied in our clinic with a mixed memory clinic chohort, 13 whereas the CCI-S has not been used in a Danish context before. The nature of the scales is very different. The MAC-Q has few items, and the person compares their current memory functioning as to when they were young. The other scales have more items and measure a more recent change in cognitive functioning. Our results show the MAC-Q had the lowest frequency of impairment in this study and this (type of) scale may be more imprecise than scales assessing recent changes in cognition.
The 3 patient groups were comparable regarding the severity of cognitive complaints even though SCD patients have no significant decline on neuropsychological tests, and that the dementia patients did not have more subjective complaints than the aMCI patients even though they had worse performances on the MMSE, ACE and other neuropsychological tests. This may be related to impaired awareness of memory problems, which is a common phenomenon in AD that tends to worsen with disease progression. 30 Studies suggest that self-report becomes less accurate as the disease progresses, 12 and our results support this (lower awareness in patients with objective cognitive deficits was significantly associated with fewer complaints). In a very recently published study, it was also found that the accuracy of an individual’s metamemory can influence to which degree SCD is associated with measures of semantic proactive interference. 31 The frequency of patients with impaired awareness was equivalent in the aMCI and the mild dementia groups and only approximately 25% of the patients had impaired awareness. This is a low number compared to the findings of a previous study in which more than 60% of MCI and mild dementia patients had impaired insight. 32 If the frequency of impaired awareness had been higher it could have led to significant group differences between SCD and dementia patients, where dementia patients may have underreported cognitive complaints even more than was found.
That different types of cognitive complaint questionnaires only to some degree measure the same thing is also supported by our finding that the questionnaires were differentially associated with factors such as age, gender, and cognitive status. The positive correlation with the GDS-15 score was not surprising, since depressive symptoms generally have a significant impact on the degree of subjective cognitive impairment.33,34 This association could possibly be explained by that fact that people with affective symptoms and stress do have problems with concentration/memory or that complaint questionnaires are affected by a negative mindset about a person’s belief of their current functioning.
Cognitive complaints are often poorly related to current objective cognitive impairment. 35 In accordance with this, we found no negative correlations between objective cognitive scores and scores on any of the cognitive complaint measures. Surprisingly, our results did show a significant positive correlation between scores on the ACE and the SMC (patients with better cognitive scores reported more complaints on the SMC). A similar tendency was previously found in another study, but the association was no longer significant when results were adjusted for depressive symptoms. 3 Since younger age and number of depressive symptoms were also positively correlated with the SMC score in our study, these variables (along with awareness of deficits) could be explanatory factors. Population-based studies often shown that cognitive complaints increase with age36,37 but the opposite was found in our study and in at least 2 previous studies in memory clinic cohorts.3,13 This could possibly explained by the less specific nature of the questions on the SMC that elicited fewer situation-specific complaints and made the SMC more sensitive to impaired awareness of deficits.
Female patients in general reported more cognitive symptoms on the SMC than male patients. Some previous studies have found that women report more complaints than men,38,39 one study observed an opposite tendency. 36 Other studies have found no association between complaints and gender.12,24
The nature of the present study was exploratory and had some important limitations including relatively small sample sizes. Thus, absolute conclusions are difficult to draw from this study alone and should be supported by other studies in the same field (eg on the nature of the complaints elicited by SCD patients in memory clinic cohorts). Further, it would have been relevant to have ratings of the patient’s memory functioning from informants on all patients. In conclusion, this study shows SCD patients referred to a memory clinic report the same level of subjective cognitive impairment as people with aMCI or mild dementia due to AD. Thus, we extend the knowledge in this field from previous findings from healthy controls, that measuring SCD may depend on the format of assessment. For both research and clinical purposes this means that the utility SCD as a marker of cognitive functioning may vary as a function of several factors including measurement factors, affective status, and memory awareness.
Footnotes
Acknowledgments
The authors thank the Danish Ministry of Health for their support to the Danish Dementia Research Centre.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Danish Alzheimer Association Research Fund for supporting this study.