
Abstract
Background
Being diagnosed with a neurodegenerative disease is a life-changing event and a critical time to help patients cope and move forward in a proactive way. Historically, the main focus of Parkinson’s disease (PD) treatment has been on the motor features with limited attention given to non-motor and mental health sequelae, which have the most impact on quality of life. Although depression and anxiety have been described at the time of PD diagnosis, demoralization, intolerance of uncertainty, decreased self-efficacy, stigma and loneliness can also present and have negative effects on the trajectory of the disease. Hence, understanding the psychological impact of the diagnosis and how to provide better counselling at this critical time point may be the key to a better long-term trajectory and quality of life.
Focus
There has been a paradigm shift in the treatment of chronic illness moving beyond the medical model, which focuses on fighting illness with the physician being in charge of the treatment process and the patient being the passive recipient, toward a more holistic (i.e., physical, psychological, social, and spiritual health) biopsychosocial approach that emphasizes behavioral factors with the patient being an active collaborator in their treatment. Hence, we propose that fostering resilience, social support, and psychological flexibility offer promise toward attenuating negative reactions and improving overall well-being.
Conclusion
Through a proactive wellness approach incorporating lifestyle choices, people with PD (PwP) can not only achieve improved states of health, well-being, and quality of life, but actually thrive.
Key Points
1. Clinicians should have regular discussions about the psychosocial and mental health reactions their patients may be experiencing, especially at the time of diagnosis and at other transition points during the disease trajectory and collaborate with and make appropriate referrals to a multidisciplinary team. 2. Social prescribing and appropriate referrals can be used to mitigate the effects of these reactions. Engaging psychologists, social workers and psychiatrists early in disease can be invaluable. 3. A proactive approach including regular counselling on lifestyle choices should be part of a prescription for wellness that becomes part of the care of PwP from diagnosis throughout the disease course.
Being diagnosed with a chronic, neurodegenerative illness like Parkinson’s disease results in several physical and psychological changes that contribute to how one experiences the life-changing and often traumatic news. 1 Among these potential new challenges are stress, crisis, loss and grief, body image, self-concept, stigma, uncertainty and unpredictability, and decreased quality of life. 2 The onset of a chronic medical condition represents a unique set of stressors resulting from the need to cope with newly encountered daily threats (e.g., independence and autonomy, fulfillment of defined roles, concerns about the future, economic stability). 3 The ability to manage psychological stress has implications for both mental health and physical symptom management. 4 Because the diagnosis of a chronic condition results in the potential loss of valued functions and societal and familial roles, it can result in psychological distress that worsens overall well-being. 5 Among the emotional consequences commonly encountered following diagnosis are loss and grief for what is now at risk as a result of the permanency of the condition. 6 These losses can include a change in physical appearance, functional ability, and social roles, which may distort body image and self-concept. 7 Judgments are made about people who have chronic medical conditions (i.e., stigma), particularly those with visible symptoms such as tremor or stooped posture, may lead to negative stereotypes and devaluation of people by society. 8 This, along with perceived uncertainty about treatment, prognosis, and relationships, may ultimately lead to decreased quality of life. 9
The Psychological Impact of Parkinson’s Disease
Currently, the diagnostic gold standard of PD is made by a movement disorders specialist based on the presence of the cardinal motor feature of bradykinesia, in addition to tremor or rigidity. 10 Initial treatment focuses on the motor symptoms with dopamine replacement, but heterogeneous psychosocial and mental health issues (e.g., anxiety, depression, adjustment challenges) related to PD are often undervalued and unrecognized despite often being present at the time of diagnosis. 11 Evidence suggests that actively addressing these comorbidities may improve both overall quality of life and functioning. 12 Patients are typically reevaluated at six month intervals following diagnosis and pharmacologic adjustments are made as necessary, but mental health challenges are frequently not addressed. 13 There is a lack of awareness of the impact of mental health issues among clinicians, which is evidenced by reports of patients with PD (PwP) feeling that doctors were not sensitive enough about their mental health needs. 14 Specifically, literature reports that neurologists have neglected to recognize depression and anxiety more than 50% of the time, 15 and a significant number of patients with depressive symptoms were neither treated nor referred for a psychiatric evaluation. 16
While recognition and treatment initiation are first steps, empowering patients with the knowledge of the importance of mental health and support to take an active role in their wellness is critical. Despite the increasing awareness of mental health issues that accompany a PD diagnosis, there remains a potentially even more troubling and underrecognized reaction. See Figure 1. Demoralization has not yet been well addressed in the PD literature but is an emotional reaction to stress that is worthy of attention. Demoralization is described as a syndrome that, as a result of living with chronic symptoms, is characterized by existential distress, hopelessness, loss of meaning and purpose in life, pessimism, helplessness, sense of being trapped, absence of motivation to cope differently, and is associated with features of social alienation and lack of social support.17,18 There is limited research on demoralization in the medical literature aside from in people with cancer, but there are clearly implications for addressing demoralization in PwP and their caregivers.
19
It is important to note that demoralization can present independently from depression, anxiety and apathy and is, therefore, something that warrants specific attention and surveillance. Wellness strategies to combat the challenges of PD.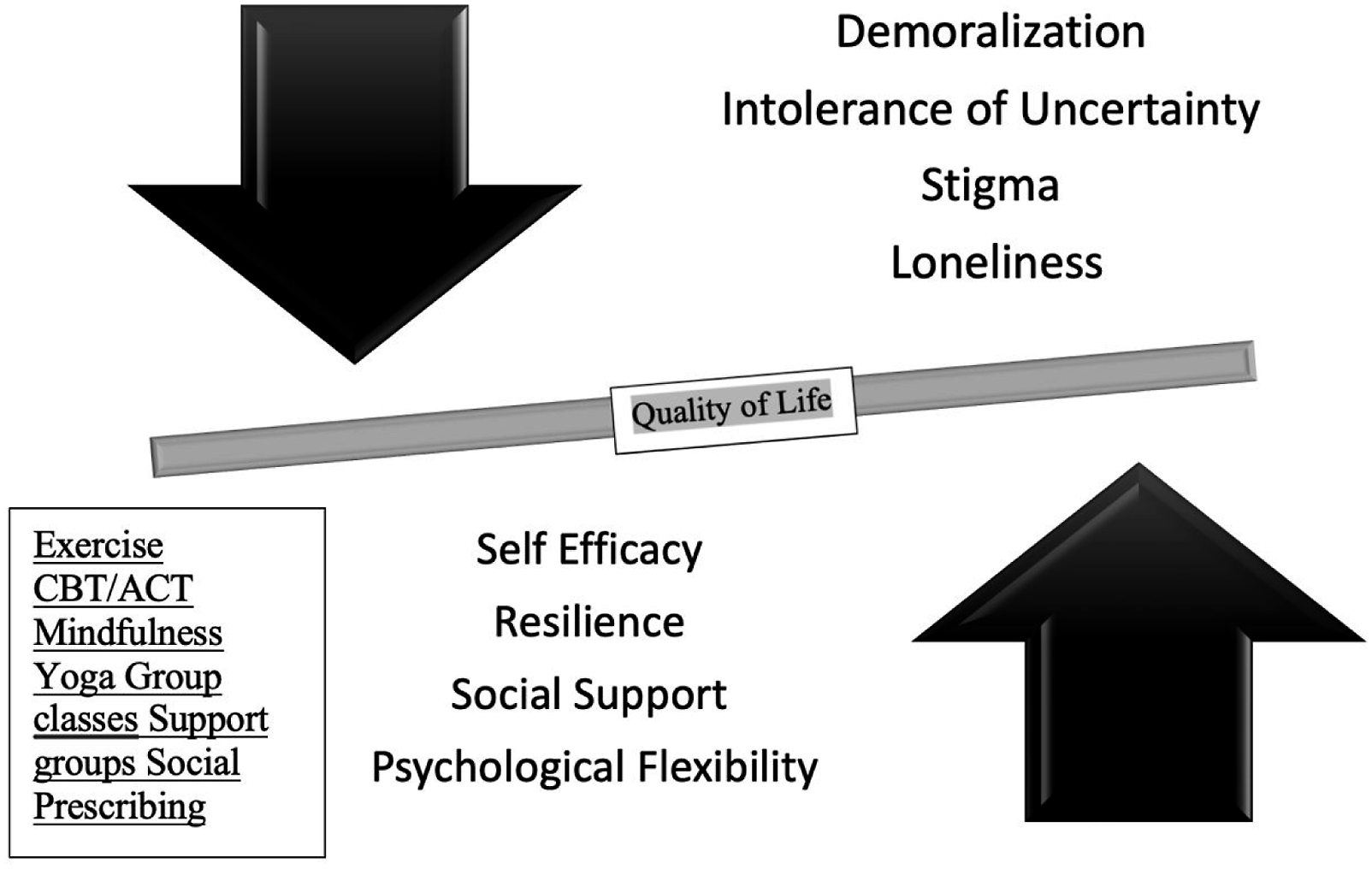
A challenge encountered early in the disease process (e.g., the first 5 years) is the concern that visible signs of illness, e.g., tremor or abnormal gait, may lead to negative assumptions and devaluation by others. This process is referred to as ‘felt stigma’ and can be conceptualized as one’s belief that they may encounter negative reactions if their condition is revealed and is associated with low self-esteem, depression, anxiety, and decreased help-seeking behaviors (e.g., mental health counseling). 20 The distress that frequently accompanies chronic illness if untreated can be detrimental in and of itself as it may contribute to the development of additional stress-related conditions (e.g., depression, anxiety, apathy).
As a way of attempting to mitigate potential felt stigma, PwP may try to hide or minimize visible motor symptoms so that they are less noticeable or to avoid being in public. This attempt to cope with the unpredictable nature of PD can be conceptualized as intolerance of uncertainty (IU), which is defined as “a dispositional characteristic that results from a set of negative beliefs about uncertainty and its implications. Individuals who are intolerant to uncertainty find uncertainty stressful and upsetting, believe that uncertainty is negative and should be avoided and experience difficulties functioning in uncertainty-inducing situations.” 21 The concept of IU was developed around general anxiety disorder but is also a transdiagnostic risk factor for social anxiety disorder, panic disorder, agoraphobia, and health anxiety. 22 Because IU is fundamentally a fear of the unknown that is associated with significant anxiety, the emotional disturbances are largely driven by a desire to increase or regain control and certainty. 23
The association between stigma, IU, and emotional and mental health issues will undoubtedly contribute to worse quality of life for PwP. The additional social determinants of health such as race, ethnicity and sexual orientation or identification further compound the negative impact of felt stigma, which is known as double stigma. Because of the felt stigma associated with IU, PwP who experience uncontrolled motor symptoms may choose to withdraw and socially isolate leading to increased loneliness, which is a well-established risk factor contributing to negative health outcomes for people with chronic health conditions and is the most suggestive predictor of psychological distress. 24 Loneliness may be a bidirectional process as people around the PwP may withdraw because of stigma and discomfort while the PwP simultaneously avoids social engagements for similar reasons.
Loneliness is a risk factor for depression and depression often causes social withdrawal, which in turn increases the risk of loneliness leading to a cascade of negative mental health events. However, for some PwP, a negative trajectory is set at the time of diagnosis, as receiving the diagnosis is often experienced as a traumatic event. At the time of initial diagnosis of PD, denial is a common reaction. 2 PD is particularly vulnerable to maladaptive coping by denial as most initial symptoms are subtle and the diagnosis is made clinically with no tangible biomarkers of disease presence, e.g., no blood test, genetic markers, or observable structural changes on imaging. While denial may appropriately lead to a second opinion, it may instead result in delayed time to treatment or pursuing additional unnecessary work up or inappropriate alternative therapies. 25
Catastrophizing, or believing the worst about a situation despite having only limited information, is another common reaction to a PD diagnosis. An extreme example of catastrophizing occurs in neurodegenerative disorders with dementia and can often be associated with an increased risk of depression and suicide.26-28 Depression and demoralization around the time of PD diagnosis is common, although the risk of suicide in idiopathic PD without dementia is less clear, these parallel findings of increased risk in related neurodegenerative diseases suggest increased monitoring is warranted. 29 Education with the goal of managing expectations and allaying fears about the disease course may help mitigate the risk of suicide and improve mental health and quality of life outcomes.
As PD progresses and symptoms increase, maintaining well-being can become increasingly challenging. Beyond the motor features lie the emotional and motivational sequelae that are commonly associated with a loss of self-efficacy. Self-efficacy is best defined as one’s perceived ability to achieve desired goals. 30 Self-efficacy is considered a critical mediator of self-management (i.e., one’s active engagement in their disease) leading to improved health and quality of life. 31 There is a strong relationship between self-efficacy and PD motor functioning and caregiver burden.32,33 There have been a variety of studies linking self-efficacy to quality of life in other chronic conditions, such as chronic pain, 34 arthritis, 35 multiple sclerosis, 36 and traumatic brain injury. 37 The role of self-efficacy in achieving positive health outcomes appears clear, and helping PwP improve their self-efficacy is a key step towards wellness.
There has been a paradigm shift in the treatment of chronic illness moving beyond the physician centered medical model. This traditional model focuses on fighting illness with the physician being the controller of the treatment process while the patient is the passive recipient. A more holistic, biopsychosocial approach in which the patient proactively pursues health, rather than just reacting to disease seems to be the future. 38 Salutogenesis (i.e., what causes positive health) 39 is largely absent from the PD literature as pathology (i.e., reasons for disease) and complaints, symptoms and limitations remain the focal point. Antonovosky further describes the disequilibrium that accompanies disease and illness, which merits efforts to identify and provide solutions to improve overall health. 40 Many other medical models appreciate the body’s innate ability to ‘heal itself’ or at least mitigate disease risk through positive lifestyle choices (e.g., ayurveda, traditional Chinese medicine) rather than seeking purely external pharmaceutical or surgical remedies.
For decades, chronic illness has been characterized based on pathology with often little attention given to social and environmental factors that make up a holistic treatment paradigm, 41 and PD is no exception. In the PD literature, the recent adoption of wellness may provide clinicians additional tools with which to help patients reach their health outcome goals. Despite definitional ambiguity, wellness can be defined as “the active pursuit of activities, choices, and lifestyles that lead to a state of holistic health.” 42 According to Halbert Dunn, 43 widely considered the founder of the contemporary wellness movement, wellness is best characterized as a component of health and may be best conceptualized as a continuum rather than an end state.
Health is largely viewed as dichotomous (e.g., good, poor) based on the presence of absence of disease; however, the World Health Organization posits that health is “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.”
44
Included in this definition is “well-being,” which is helpful in further conceptualizing health: Through the International Classification of Functioning, Disease, and Health,
45
an interactive classification system designed to evaluate health and functioning in a holistic manner, the WHO defines well-being as “encompassing the total universe of human life domains, including physical, mental, and social aspects (p. 211). In other words, the WHO defines health in terms of well-being. Lastly, quality of life, often the ultimate measure of one’s satisfaction with life, is defined as “the subjective and personally derived assessment of overall well-being that results from evaluation of satisfaction across an aggregate of personally and clinically important domains.”
9
The ICF model (see Figure 2) has been described as a valuable tool to assess quality of life and well-being for PwP and other neurological conditions46-48 but remains underutilized. We propose that through a focused wellness approach, PwP can not only achieve improved states of health, well-being, and quality of life, but actually thrive. Interactions between the components of the ICF Model. Adapted from The International Classification of Functioning, Disability, and Health, WHO (2001).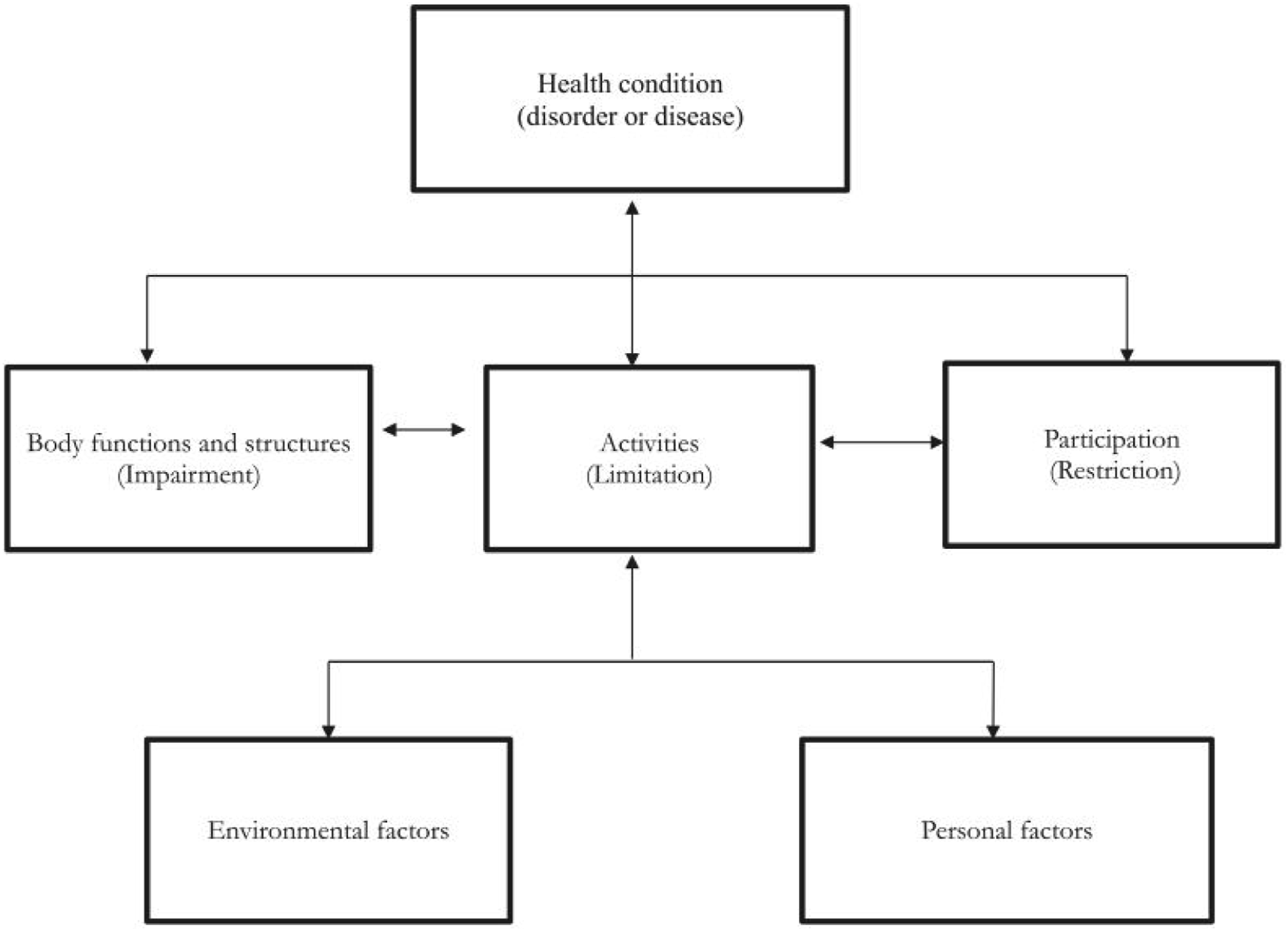
Wellness Tools
Coping with the challenges of a chronic illness is not a straightforward process and requires some effort on the part of the patient to develop strategies that facilitate positive psychological adjustment and reduce the effects of untoward mental health issues. There is a robust body of literature describing coping with chronic illness, and it is largely defined as the efforts, both biological and cognitive, used to mitigate the demands of stressful situations. 49 As self-efficacy refers to one’s appraisal of their ability to complete a task, coping self-efficacy denotes one’s belief in their capability to cope effectively with stressful life events 50 and is associated with lower levels of psychological distress. 51
Resilience
Mental health wellness is defined as a resource that allows people to think, feel, connect, and function at their best and is an active process that helps us build resilience. 42 Resilience is defined as the ability to bounce back following adversity and being able to flexibly adapt to the changing demands of stressful life situations. 52 People who are resilient are able to bolster positive emotions during times of stress to reduce the negative impact. Resilience is considered to be modifiable and is partially determined by a set of resilience factors. 53 Resilience factors include both internal factors: genetics, personality traits (e.g., optimism, hope, hardiness) and beliefs (self-efficacy) 54 and external factors such as social, material, and energy resources. 55 Practically, resilience can be fostered through the enhancement of well-being through positive, enjoyable activities (e.g., physical exercise), increase in social support, and the development of adaptive psychological coping strategies around insight, self-efficacy, hope, optimism, gratitude driven by the principles of cognitive behavioral therapy and acceptance and commitment therapy.56,57
Social Support
Resilience is important to help people manage the psychological distress associated with a PD diagnosis, and positive and supportive social relationships are no less essential. 58 Research supports the role of adequate social support in attenuating depression, anxiety, the negative effects of stigma, and improving emotional well-being, overall life satisfaction, and positive affect in PwP. 59 Social support can manifest in a variety of ways but is best understood as the resources available from others and from valued social networks. 60 Adaptation to stressful life events is partially dependent on social resources. Among the benefits of social support are emotional support, informational assistance, and instrumental assistance (e.g., material assistance with practical tasks), which are positively correlated with mental health. 61 Specifically, people with smaller social networks or interpersonal relationships consistently report elevated rates of depression and anxiety. 62
Social prescribing is one novel mechanism for clinicians to facilitate community connections to improve patient health and wellness. 63 Clinicians can direct patients toward community-based group classes including boxing, yoga, meditation, cycling, music, and dancing, which promote social engagement and support. 64 Additionally, PwP can also utilize family, spouses, online groups, community support groups, and health care and allied health care providers. Social support provides a way to buffer psychological distress by fostering healthy coping strategies through strengthening self-agency and coping self-efficacy resulting in the skills and confidence necessary to effectively negotiate stress. 65 These adaptive coping strategies are achieved through both behavioral and psychological processes. Behaviorally, most supportive relationships encourage healthy behaviors (e.g., exercise, adherence to medical regimens) and psychologically, social support aids with realistic appraisals of situations, positive affect, and feelings of control. 66
Psychological Flexibility
Psychological flexibility is conceptualized as being fully in contact with the present, aware of emotions and thoughts, including uncomfortable ones, and welcoming them without judgment, and acting on long-term values rather than short-term impulses. 67 Evidence supports targeting psychological (in)flexibility is beneficial for a range of clinical disorders including depression, anxiety, and post-traumatic stress disorder 68 and, more specifically, for people with chronic illness. 65 Acceptance and Commitment Therapy (ACT) 69 is an evidence-based transdiagnostic cognitive-behavioral intervention that cultivates psychological flexibility as a means to adaptation and wellbeing 70 and has demonstrated improvements in quality of life, stress, self-management, coping, reduced distress, and perceived stigma.67,71 An important consideration for psychological flexibility is that executive functioning, which includes working memory and recall, information processing speed, and the ability to inhibit behavior is needed to effectively modulate responses adequate to a set of circumstances. 72 These challenges associated with executive dysfunction and psychological inflexibility may result in poorer coping and adapting to uncertain disease progression in PwP.
Formal Interventions
Besides ACT, which posits that psychological distress is largely caused by experiential avoidance and cognitive entanglement that, when combined, result in psychological inflexibility, there are several evidence-based interventions available to assist patients in navigating the mental health and psychological challenges associated with a PD diagnosis. Cognitive-behavioral therapy (CBT) is among the most widely used and evidence-based treatments designed to address negative automatic thoughts by challenging their empirical evidence. Hence, early referral to psychologists or social workers may be indicated. Additionally, mindfulness-based stress reduction 73 therapy has shown positive outcomes in clinical populations for people with co-occurring physical and psychological symptoms with marked reductions in depression and anxiety. 74 Several complementary and alternative treatment options have surfaced with initially compelling evidence. Music therapy has emerged as a potentially helpful option for improving social functioning, cognition, mental health and psychological functioning, and mobility for PwP. 75 Another possible option is mindfulness yoga, which has been shown to positively effect depression, anxiety, and quality of life in PwP. 76 Although these interventions do little to resolve the motor issues associated with PD, they all appear to effectively provide some relief form the negative psychological distress associated with a new diagnosis and potentially improve well-being. Engagement of a physical therapist or personal trainer may also provide a way to learn positive psychology techniques which should be explored in future studies. Although this paper focuses on those in the early stages of their PD (i.e., first 5 years), many of the recommendations can apply to those in later stages of disease; however, experience suggests that as people progress into later stages of their PD they become better equipped to navigate the negative aspects largely through education, established social support, and an increased understanding of how to have their needs met. Additionally, some issues in later stages (e.g., motor fluctuations) create different challenges and will be addressed in a subsequent paper.
Conclusion
Being diagnosed with PD sets off a cascade of reactions that typically result in significant psychological distress, leaving the patient feeling confused and alone and uncertain about the future. The traditional PD treatment paradigm of diagnosis, initiation of dopaminergic medications, and follow-up in six months with little to no discussion about psychosocial or mental health issues 13 is not optimal. Evaluating patients for the presence of mental health issues is one crucial element of quality care and if challenges are identified, collaboratively working with patients to find effective coping strategies, foster resilience through the steps outlined above, and cultivate an effective social support system through social prescribing.
The movement disorders specialist does not provide patient care alone; engagement of the multidisciplinary team including psychologists, social workers and psychiatrists early in disease can improve quality of life and set up for a more favorable long-term trajectory. Whether in early- of late-stage PD, establishing a holistic, biopsychosocial approach to living with PD that emphasizes a patient-centered collaboration with the healthcare team focused on proactive wellness strategies may be the first step to achieving better long-term outcomes for PwP.
Footnotes
Author Note
Dr. Pontone has consulted for Acadia Pharmaceuticals Inc. We have no other conflicts of interest to disclose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.