
Abstract
A good nutritional status and healthy diets may decelerate disease disability and symptom severity and quality of life of peoples with multiple sclerosis (MS). Mediterranean diet (MD) can prevent several chronic diseases, including neurodegenerative disease. This is an observational, cross-sectional study on 279 older adults with MS, aiming to investigate the effects of MD against several aspects of mental health. Qualified questionnaires were used to assess disability and symptom severity, depression, anxiety, stress, sleep quality, cognitive status, physical activity, and MD adherence. Multivariate analysis showed that enhanced MD adherence was independently associated with lower prevalence of disability and symptom severity (P = .0019), depression (P = .0201), anxiety (P = .0287), perceived stress (P = .0021), inadequate sleep quality (P = .0033), cognitive impairment (P = .0018) and physical inactivity (P = .0028). Adopting MD may ameliorate mental health disturbances in older adults with MS. Future public health policies should inform older adults with MS for the favorable impacts of MD in improving the mental health MS comorbidities.
Introduction
Multiple sclerosis (MS) constitutes a chronic inflammatory, degenerative and demyelinating disease of the central nervous system (CNS) with both genetic and environmental factors contributing to its development that can lead to a broad range of sensorimotor, cognitive, visual, and autonomic function symptoms.1,2 MS is initially evolved through myelin destruction and subsequent deposits of scar tissue, which result in debilitating physical and cognitive disturbances and a considerable worsening on daily quality of life and performance functionality.3,4 It is the most common demyelinating condition of the CNS affecting about 2.5 million people worldwide with its prevalence being gradually increasing, especially in women.5-8 As the disease progresses, its symptoms become more prominent, deteriorating the performance of daily living activities, and worsening the quality of life.5,9 Novel treatment approaches seem promising to promote longevity; however, MS overall mortality rates remain still unaltered.5,9
Changes in MS pathophysiology appear to be age dependent and several studies have identified a consistent phase of disability worsening in the later stages of the life.10-12 Several clinical studies indicated significantly diminished anti-inflammatory efficacy in patients older than 40 years old.13,14 Also, MS itself may be closely related to cognitive impairment, even though its exact etiopathogenic mechanisms remain still unclear. 15 Moreover, COVID-19 infection, and hospitalization rates were higher among peoples with MS during pandemic. 16 There is also substantial evidence that older adults constitute a population group with a high prevalence of non-communicable chronic diseases and high risk of malnutrition.17,18 Nutritional status plays a key role on healthy ageing. 19 Diet quality and quantity are declining in this age group, making the older adults as a group at high risk of malnutrition and mortality, 20 worsening health status and quality of life. 21 In this aspect, a few studies documented that a better nutritional status was associated with lower prevalence if worse health-related quality of life, higher physical activity, and adequate sleep quality, cognitive impairment, and depression.22,23 These studies highlighted that public health strategies and policies should be applied for informing older adults for the necessity to improve their nutritional status and lifestyle habits to improve their health status and to obtain better life expectancy.22,23
Neuropsychiatric symptoms have frequently been reported in peoples with MS. Among them, cognitive impairment, clinical depression, and anxiety seem to be the most common with a higher frequency in peoples with MS compared to the general population. 24 An improved understanding of the pathophysiological mechanisms underlying these conditions could lead to the development of several neuropsychological batteries and scales to better identify and monitor disease symptoms. 25 Psychiatric symptoms are common comorbidities in MS, interacting with the disease course, and affecting patients’ compliance to the conventional therapy.26,27 Despite its importance, mental health remains overlooked in this patient group. 28 Treating psychiatric symptoms is crucial to enhance mental health, which may further improve the quality of life and sleep quality of peoples with MS.29,30
In this aspect, nutrition may act as a possible co-factor influencing the inflammatory cascade by acting on both on the molecular pathways and gut microbiota involved in MS. 31 Alarmingly enough, the question whether dietary habits and lifestyle may positively influence on the course of MS remains an extremely matter of debate, while the potential benefits from any health dietary pattern diet in MS have not yet been proven by strong evidence.32-34 In this aspect, there are several evidence that nutritional assessment and support may exert crucial impacts by slowing down the development and progression as well as by monitoring peoples with neurodegenerative diseases, including MS. 35 In support of this view, there is recent preliminary evidence that a high intake of saturated fat increased the incidence of MS, while unsaturated fatty acids may exert a positive effect on the course of MS.36,37 Notably, there are some pilot studies that some healthy dietary patterns such as low-fat vegan, modified Paleolithic, and gluten free diets as well as Mediterranean diet (MD), and intermittent fasting have been associated with an improvement of disease disability and symptom severity.38,39 However, the above findings have been derived by few and mainly small pilot studies and can not provide conclusive results.
More recently, there are some preliminary studies that have assessed the potential beneficial impact of healthy dietary patterns such as MD on the disability and symptom severity of older adults with MS, even if they have been characterized by rather controversial and inconclusive results. More to the point, recent high-quality evidence has strongly supported that MD can exert anti-inflammatory and antioxidants effects against human diseases, including MS.40-42 The MD is a well-studied dietary pattern that has been associated with a reduced risk of developing MS and a decrease in disability during the course of the disease, which may lead to an overall improvement in quality of life and functionality of peoples with MS.43,44 A small pilot study initially showed that a diet rich in fruits and vegetables may modulate microbiota dysbiosis, improving clinical parameters in peoples with MS by increasing anti-inflammatory circuits. 45 On the other hand, a cross-sectional study including 102 adults with MS did not find any association between MD adherence and MS-related symptom checklist; however, it has revealed negative association of MD adherence with fatigue severity scale. 46 In a case-control study involving 70 peoples with MS, MD adherence has reduced MS risk. 47 Accordingly, a population-based case-control study recruiting incident cases of MS (1953 cases, 3557 controls) has documented that MD may exert a protective influence regarding the risk of subsequently developing MS compared ro Western-style diet. 48 In this context, a multicenter, cross-sectional study conducted on 478 peoples with clinically definite MS has further indicated that higher MD adherence has been associated with lower risk of overweight and obesity; however, the score of MD adherence did not show any significant relationship with mild, moderate, and severe levels of disability. 49
In view of the above consideration, there is currently a gap in the international scientific literature concerning the improvement of several aspects of mental health outcomes of older adults with MS. In this aspect, the present observational, cross-sectional study aims for the first time to investigate the potential impact of a healthy dietary pattern such as MD adherence in several aspects of mental health of older adults with MS, including their disease disability and symptom severity, depression, anxiety, stress, sleep quality, cognitive status, and physical activity. Several sociodemographic and anthropometric data of the study population were also collected or measured in order to be subjected to statistical analysis to minimize confounding effects.
Materials and Methods
Study Population
Initially, 468 community-dwelling older adults over 65 years old were randomly enrolled from 6 different, geographically diverse Greek regions, both urban and rural, namely Athens, Thessaloniki, Alexandroupoli, Larissa, Patra and Crete. Recruitment to the study was between April 2016 and December 2022 in community-dwelling older adults founding mainly during their visits in health care units, as well as in public centers related with entertainment activities for older persons. Eligibility criteria were any community-dwelling older adults over 65 years old diagnosed with MS without any additional severe chronic disease such as cardiovascular diseases, cancer, metabolic disorders, autoimmunity diseases, or other degenerative diseases. Recruitment strategy was focused only on community-dwelling older adults over 65 years with MS, who have available time to participate to the study.
During their thorough recruitment, 49 (10.5%) peoples with MS refused to participate in the study after giving to them the relevant information for the purpose of the study and they were excluded from the study. Among the remaining 419 older adults with MS, 94 (22.4%) of them had additionally another severe disease except for MS such as cardiovascular diseases, cancer, metabolic disorders, autoimmunity diseases, or other degenerative diseases and they were also excluded from the study. Among the remaining 325 older adults with MS, 46 (14.2%) of them did not finally complete all the given questionnaires, and thus they were excluded from the study. Finally, 279 older adults diagnosed with MS were included in the final analysis with a final response rate equal to 59.6%. In Figure 1, a flow chart diagram of the study enrollment is depicted. Flow chart diagram for study enrollment.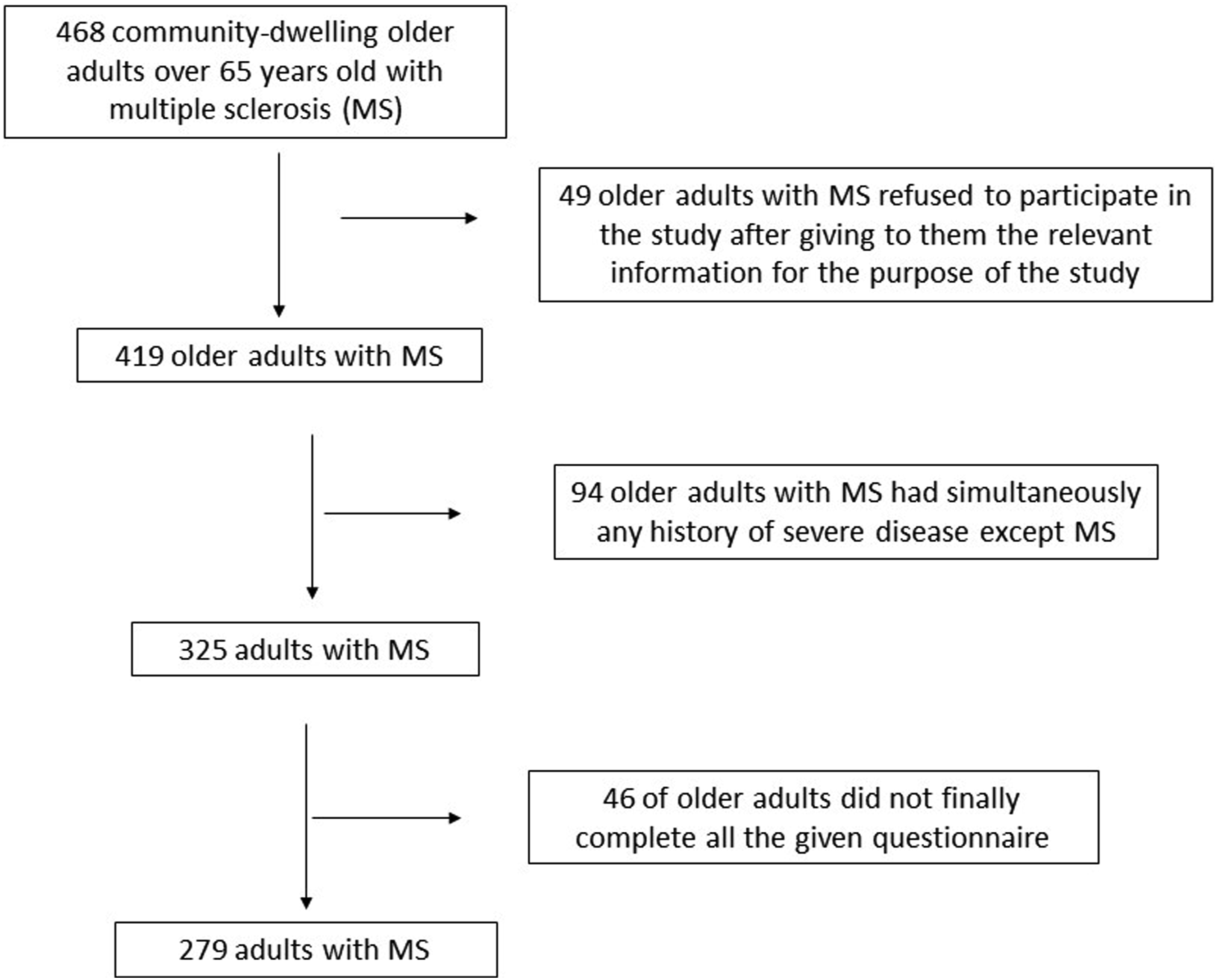
Sample size calculation was based on the use of PS: Power and Sample Size calculator program, while a simple randomization method was carried with the use of a sequence of random binary numbers (eg, 010101110 in which zero represented enrolment and 1 not enrolment to the study). PS software can calculate the sample size required to detect a specified alternative hypothesis with the needed power, the power with which a specific alternative hypothesis can be detected with a given sample size, or the specific alternative hypotheses that can be detected with a given power and sample size. The calculation of the power of our sample size indicated a power of 86.9%.
All participants’ information was confidential, and all participants were informed about the purpose of the study and signed a written consent for accepting to anonymously publish their data. In our study, we carried out all the guidelines of the Declaration of Helsinki and in accordance with the World Health Organization (52nd WMA General Assembly, Edinburgh, Scotland, 2000). The Ethical Organization of the University of Aegean (ethics approval code: no 18/22.9.2016) approved the design and the implementation of the present study, as well as the consent approval of the participants.
Study Design
This is an observational, cross-sectional study on older adults diagnosed with MS. Participants’ sociodemographic characteristics such as age, gender, educational level, family economic status, living status, smoking habits and nationality were self-reported during face-to-face interviews between the enrolled older adults with MS and qualified personnel in an isolated and relaxed environment to reduce recall bias. The educational level was categorized into 3 classes: (a) primary education, (b) secondary education, and (c) university studies. Economic status was categorized based on the annual income as: 0 ≤ 5000€, 1 ≤ 10,000€, 2 ≤ 15,000€, 3 ≤ 20,000€, 4 ≤ 25,000€ and 5 > 25,000€, according to per capita gross domestic product. We further classified economic status as low for annual income ≤ 10,000€, medium for annual income >10,000€ and ≤ 20,000€, and high for annual income > 20,000€.
Body weight and height were also measured at the time of study enrolment to calculate Body Mass Index (BMI). Participants weight was determined utilizing a Seca scale [Seca, Hanover, MD], without shoes, to the near 100 grams, while height was determined utilizing a portable stadiometer (GIMA Stadiometer 27335) with no shoes on, to the nearby 0.1 cm. The WHO recommendations were applied to classify the assigned individuals as normal weight, overweight or obese. 50 The enrolled older adults were classified according to the type of MS into 3 classes: (a) relapsing-remitting MS, (b) secondary progressive MS and (c) primary progressive MS based on the McDonald 2010 diagnostic criteria. 51
Seven qualified and validated questionnaires were used to evaluate disability and symptom severity, depression, anxiety, stress, sleep quality, cognitive status and MD adherence of the study population, respectively. Specifically, Expanded Disability Status Scale (EDSS) was used for evaluating disability and symptom severity of older adults with MS. The Expanded Disability Status Scale (EDSS) is a validated and well-recognized method of quantifying disability in MS and monitoring changes in the level of disability over time. 52 EDSS steps 1.0 to 4.5 refer to patients who are fully ambulatory, while EDSS steps 5.0 to 9.5 are defined by the impairment to ambulation and usual equivalents and impairment to walking. 52
Depression status was assessed using the Geriatric Depression Scale (GDS) questionnaire which includes 30 items. 53 In each question accounted 2 possible answers, “yes” or “no” marked as 0 or 1, respectively. Total GDS scores were calculated as the summation of 30 component scores ranging from zero to 30. A total global GDS score of ≥15 is indicative of depression. 53
The six-item versions of the State form of the anxiety inventory (STAI-6) questionnaire were used to evaluate the anxiety status of the enrolled patients with MS. 54 STAI-6 is a short-form version of the state scale, consisting of 6 items chosen for reliability and validity. It is designed to be administered in circumstances that prohibit the use of the full-form and produces scores that are comparable to using the full version. 54
The Perceived Stress Scale (PSS) questionnaire was used to assess the stress of the enrolled patients with MS. 55 This validated questionnaire includes 10 questions evaluating feelings and thoughts during the last month. Individual scores on the PSS can range from 0 to 40 with higher scores indicating higher perceived stress. Scores ranging from 0-13 would be considered low stress. Scores ranging from 14-26 would be considered moderate stress, while scores ranging from 27-40 would be considered high perceived stress. 55
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI) which consists of 19 items that are rated on a four-point scale (0-3) and grouped into 7 components (sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medications, and daytime dysfunction). 56 The item scores in each component were summed and converted to component scores ranging from 0 (better) to 3 (worse) based on the relevant guidelines. 57 Total PSQI scores were calculated as the summation of 7 component scores ranging from zero to 21, where a higher score indicates worse condition. A total global PSQI score of <5 is indicative of adequate sleep quality. 56
The Mini Mental State Examination (MMSE) questionnaire was applied for evaluating the cognitive status of the enrolled patients with MS. 58 The MMSE is effective as a screening tool for cognitive impairment in older, community dwelling, hospitalized and institutionalized adults. It is an 11-question measure that tests 5 areas of cognitive function: orientation, registration, attention and calculation, recall, and language. The maximum score is 30. A score of 23 or lower is indicative of cognitive impairment. In fact, a score between 20 and 23 is indicative of mild cognitive impairment, while a score less than 20 is indicative of moderate or severe cognitive impairment. 58
We also assessed physical activity levels utilizing the International Physical Activity Questionnaire (IPAQ) in which subjects mention how much exercise they do in a typical week. This self-administered questionnaire, used worldwide, can assess the overall physical activity over the last 7 days, to categorize it as low, moderate, or high. 57 IPAQ instruments have comprehensively been tested and demonstrated good reliability and acceptable validity properties, at least as good as other self-answered PAQs. 57
For the assessment of the MD adherence, we used the Mediterranean Diet Score (MedDietScore) by Panagiotakos et al 59 This is a Food Frequency Questionnaire (FFQ) with 11 selected food groups based on MedDietScore index. 59 In each question accounted 6 possible answers, marked from 0 to 5, depending on the level of adherence for each foodstuff group. The sum of the 11 questions leads to an overall score ranging from 0 to 55 and a higher score represents elevated MD adherence. For cereals, potatoes, fruits, vegetables, dairies and olive oil, the scale of 6 possible responses adjusted per day. For legumes, seafood, red meat and poultry, the scale of 6 possible answers adjusted per week. 59 The 11th question assessed wine consumption per day with moderate consumption (≤1 and ≤2 drinks/day for women and men, respectively; 1 drink = 100 mL = 12 g ethanol)) taking the highest score. 59 The enrolled older adults were classified into quartiles according to their MedDietScore. A MedDietScore below 23 shows very low MD adherence, and a MedDietScore between 23-26 indicates low MD adherence. A MedDietScore between 27-30 shows moderate MD adherence, while a MedDietScore 31 and above indicates high MD adherence.
All questionnaires were completed by trained medical personnel (eg, medical and nursing personnel) and nutritionists and dietitians by face-to-face interviews with community-dwelling older adults with MS to minimize recall biases. The qualified personnel explained in detail to the community-dwelling enrolled older patients’ adults all the questions of the questionnaires to ensure the reliability and accuracy of responses.
Statistical Analysis
Descriptive statistics analysis has initially been performed to analytically describe and summarize the main features of our study population. Student’s t-test was used for continuous variables that followed the normal distribution. Kolmogorov-Smirnov test was applied for examining whether the continuous variable follow the normal distribution. Chi-square test was used for categorical variables. The normally distributed quantitative variables are presented as mean value ± Standard Deviation (SD), and the qualitative variables as absolute or relative frequencies. The no-normally distributed quantitative variables are presented as median values, interquartile range (IQR). Multiple binary logistic regression was applied to assess whether MD adherence can be independently associated with any of the collected or measured covariates (patients’ age and gender, educational and family economic level, living and smoking status, BMI, type of MS, EDSS, depression, anxiety, stress, sleep quality, cognitive status and IPAQ). Multiple regression results are presented as Odds Ratios (OR) and 95% confidence intervals (CI). Differences were considered significant at P < .05 and 95% Confidence Interval. Statistica 10.0 software, Europe (Informer Technologies, Inc., Hamburg, Germany) was applied for the statistical analysis of the survey data.
Results
Descriptives Statistics of the Study Population
Descriptive Statistics of the Study Population.
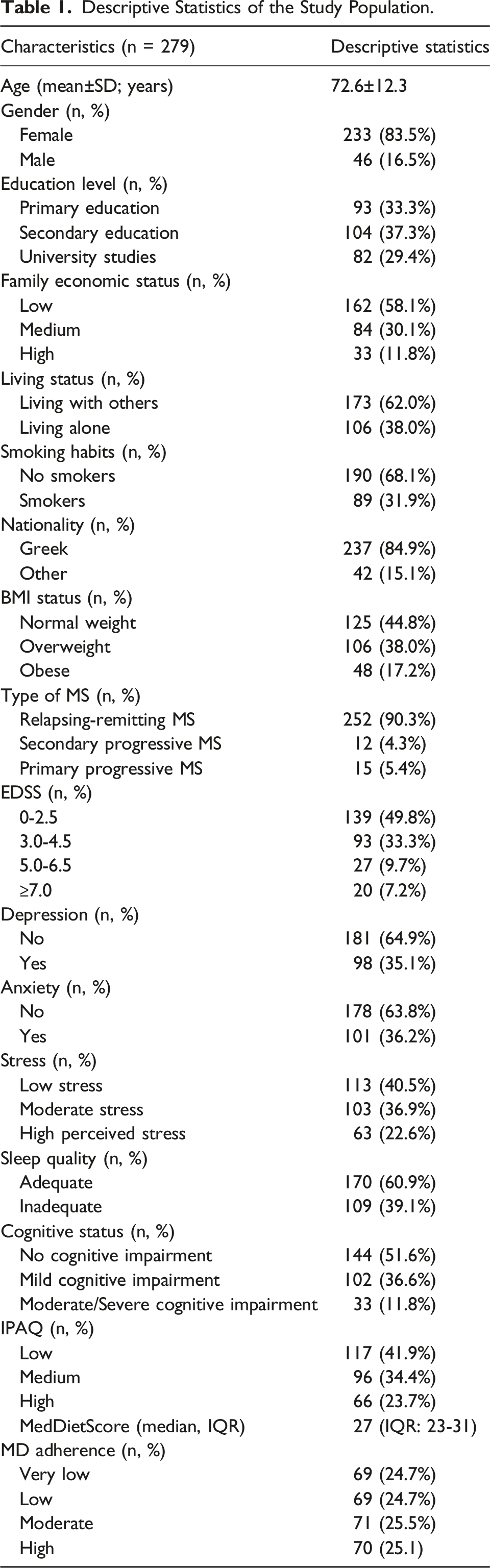
Concerning the type of MS of the enrolled older adults, 90.3% of them were diagnosed with relapsing-remitting MS, 4.3% of them with secondary progressive MS and 5.4% of them with primary progressive MS. As far as EDSS classification related with disability and symptom severity as concerns, 49.8% of individuals with MS had a score between 0-2.5, 33.3% of them exhibited a score between 3.0-4.5, 9.7% presented a score between 5.0-6.5% and 7.2% of them had a score ≥ 7.0. Based on GDS, 35.1% of the enrolled individuals with MS were categorized as depressed and the remaining 64.9% as undepressed. 36.2% of the enrolled older adults with MS showed anxiety symptomatology, while 63.8% of them did not show any anxiety symptoms according to STAI-6 questionnaire. Based on PSS scoring, 22.6% of the enrolled individuals with MS showed high perceived stress, 36.9% of them exhibited moderate stress and 40.5% of them did not show any sign of stress, being classified as individuals with low stress. According to PSQI classification, 39.1% of the enrolled older individuals with MS showed inadequate sleep quality, while 60.9% of them exhibited adequate sleep quality. Based on MMSE, 11.8% of the assigned individuals with MS were diagnosed with moderate or severe cognitive impairment, 36.6% of them with mild cognitive impairment, while the remaining 51.6% of them had no signs of cognitive impairment. According to IPAQ classification, 41.9% of the enrolled older adults with MS showed low physical activity levels, 34.4% of them had medium physical activity levels and 23.7% of them exhibited high activity levels. The median MedDietScore was 27 (IQR: 23-31).
MD Adherence in Association with Sociodemographic and Anthropometric Characteristics of the Enrolled Older Adults’ Patients with MS
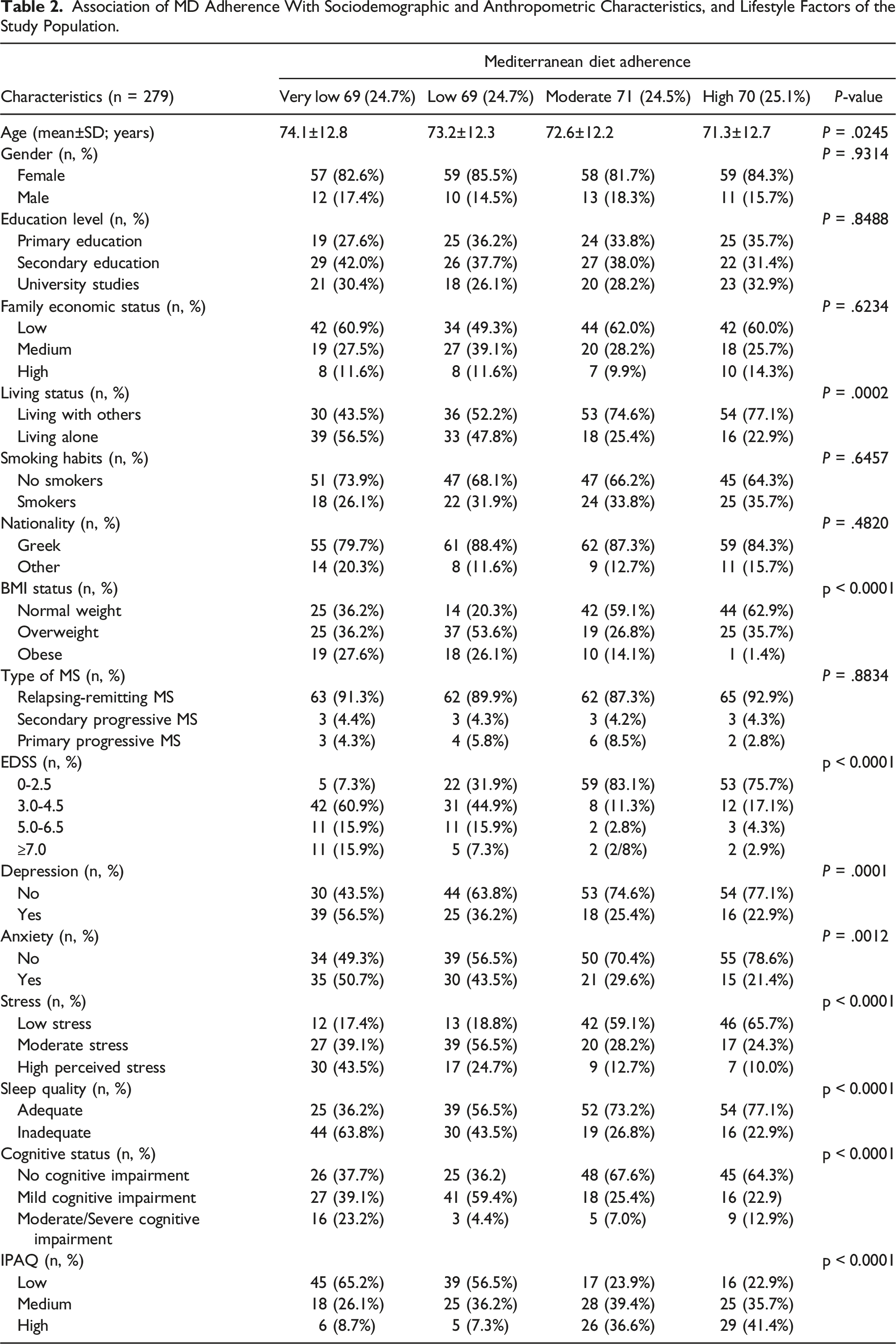
Association of MD Adherence With Sociodemographic and Anthropometric Characteristics, and Lifestyle Factors of the Study Population.
MD Adherence in Association with Disability and Symptom Severity, Type of Disease, Depression, Anxiety, Stress, Sleep Quality, Cognitive Status and Physical Activity of the Study Population
Disability and symptom severity of the enrolled older adults with MS showed a strong inverse association with their MD adherence (Table 2, p < 0.0001). More to the point, older adults with MS who highly adopting MD had significantly lower scores concerning EDSS related with disability and symptom severity (Table 2, p < 0.0001). In contrast, older adults with a very low or low MD adherence exhibited significantly higher scores based on ESSD (Table 2, p < 0.0001). The enrolled older adults with MS adopting higher MD adherence showed significantly lower prevalence of depressive symptoms compare to those with reduced levels of MD adherence (Table 2, P = .0001). In addition, the enrolled older adults with MS presenting lower levels of MD compliance exhibited a significantly higher frequency of anxiety symptoms compared to those with elevated MD compliance (Title 2, P = .0012). Older adults with MS adopting lower MD levels were also significantly associated with higher prevalence of stress symptoms than those with greater MD adherence (Table 2, p < 0.0001). Moreover, a lower MD adherence was significantly associated with a higher incidence of inadequate sleep quality (Table 2, p < 0.0001). Accordingly, older adults with MS presenting lower MD levels significantly exhibited a worse cognitive status (either mild or moderate/severe cognitive impairment) compared to those presenting higher MD adherence (Table 2, p < 0.0001). Lastly, elevated MD adherence was significantly associated with higher physical activity levels of older adults with MS (Table 2, p < 0.0001). On the contrary, the type of MS was not associated with MD adherence (Table 2, P = .8834).
Multivariate Binary Logistic Regression Analysis for MD Adherence
Multivariate Analysis of MD Adherence.
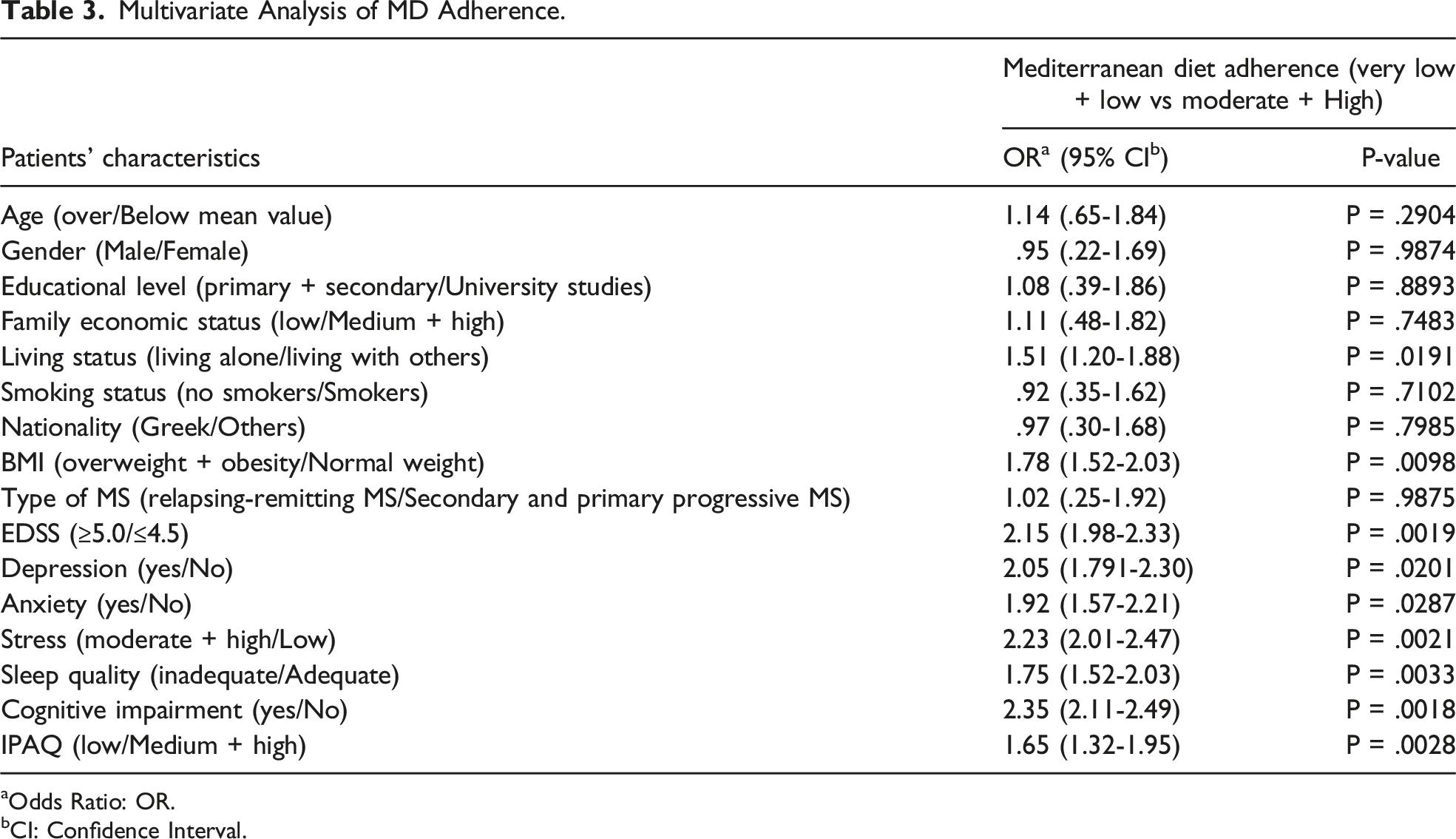
aOdds Ratio: OR.
bCI: Confidence Interval.
Older adults with MS adopting MD at higher levers had a 51% higher frequency to live with others than those presenting lower MD compliance (Table 3, P = .0191). Older adults with MS presenting higher MD adherence levels exhibited 78% lower odds to be affected by overweight or obesity compared to those with reduced MD adherence (Table 3, P = .0098). Older adults with MS having higher MD compliance showed at a significant, independent level a more than 2-fold lower incidence of disability and symptom severity (EDSS score ≥5.0) compared to those with decreased MD compliance (Table 3, P = .0019). Older adults with MS adopting MD at higher levels had about 2-fold lower odds of depressive and anxiety symptoms than those with reduced MD compliance (Tabe 3, P = .0201 and P = .0287, respectively). Accordingly, older adults with MS presenting elevated MD adherence showed a more than 2-fold lower incidence of stress symptomatology than those with decreased MD adherence (Table 3, P = .0021). Older adults with MS implementing MD at elevated levels also showed 75% higher odds of presenting adequate sleep quality compared to those with reduced MD adherence (Table 3, P = .0033). Moreover, older adults with MS implementing MD at higher levels exhibited a more than 2-fold lower frequency of cognitive impairment than those with reduced MD compliance (Table 3, P = .0018). Lastly, older adults with MS and higher MD adherence had 65% greater odds of high physical activity levels compared to those with decreased MD compliance (Table 3, P = .0028).
Discussion
To the best of our knowledge, this study is 1 of the few currently available observational, cross-sectional studies that have provided evidence that higher levels of MD adherence may be associated with lower prevalence of disease disability and symptom severity, depression, anxiety, stress, sleep disturbances, cognitive impairment, and physical inactivity in older adults with MS. It should be noted thar most of the currently available studies have been performed on children, adolescence, young and middle-aged adults with MS. In contrast, relevant studies including older adults with MS remain extremely scarce, presenting several controversies.38,39 Moreover, only a few recent studies have exclusively assessed the impact of MD on disability and symptom severity of older adults with MS, whereas studies examining the impact of MD adherence in several aspects of mental health of older adults with MS remain highly scarce. Our results are in accordance with certain previous studies that a higher compliance to MD may be associated with an improvement in disease disability and symptom severity, exerting also positive effects in several aspects of the mental health of older adults with MS such as depression, anxiety, and stress, reinforcing also daily quality of life, sleep quality and physical activity.40-49
In this context, recent high-quality evidence has strongly supported that MD can exert anti-inflammatory and antioxidants effects against human diseases, including MS.50-52
Notably, an update of the Cochrane Review 'Dietary interventions for MS has suggested that there is insufficient evidence to determine whether supplementation with antioxidants or other dietary interventions have any impact on MS-related outcomes, while some of the currently available studies suffers from high risk of bias at present. 60 Beyond MD, a recently published study found that a paleo diet, may be useful in MS treatment by reducing perceived fatigue, improving mental and physical quality of life, increasing exercise capacity, and improving arm and leg function. 61 According to other researchers, similar dietary interventions with paleo diet could reduce fatigue and improve quality of life in peoples with progressive MS.62,63 A pilot study reported by Brenton et al. has also suggested that a modified ketogenic diet may benefit peoples with MS. 64 Despite the small study sample, this study has firstly shown that modified ketogenic diet may alleviate fatigue and depressive symptoms, reducing body fat and pro-inflammatory adipokines. 64 The same research group has further performed a 6-month interventional study on 53 peoples with relapsing-remitting MS receiving a ketogenic diet and indicating significant improvements in their disability status and quality of life, by reducing at the same time fatigue and body fat levels. 65 A recent study by Armon-Omer et al. has also found that peoples with MS had reduced levels of total serum antioxidant capacity, highlighting that poor antioxidant capacity in severe MS may exert a negative effect by worsening disability and symptom severity. 66 In support of this view, a randomized clinical trial by Mousavi-Shirazi-Fard et al has shown that peoples with relapsing-remitting MS who followed an antioxidant and anti-inflammatory diet showed improvements in quality of life and fatigue levels. 67 The last 2 studies are in line with our results taking into consideration that MD is rich in numerous bioactive compounds with strong antioxidant and anti-inflammatory properties.
In a randomized-controlled, assessor-blinded study, a very-low fat, plant-based diet like MD was well adhered to and tolerated, and exerted significant improvements in measures of fatigue, BMI, and metabolic biomarkers of peoples with MS compared to await-listed control group. 68 Although the above dietary intervention led to a beneficial effect on the self-reported outcome of fatigue, these results should be interpreted cautiously as a wait-list control group may not completely be control for a placebo effect and there was a baseline imbalance on fatigue scores between the groups. 68 In another randomized parallel-arm clinical trial, a comparison between the modified Paleolithic elimination (Wahls) diet and the low-saturated fat (Swank) diet in individuals with relapsing-remitting MS was performed and both diets were associated with clinically meaningful within-group reductions in fatigue and improvements in quality of life. 69
From a molecular mechanism of view, in a murine experimental autoimmune encephalomyelitis (EAE) model, a periodic 3-day cycles of a fasting mimicking diet (FMD) were found effective in ameliorating demyelination and symptoms. 70 The FMD decreased the clinical severity of MS in all mice and completely reversed symptoms in 20% of them. Notably, these improvements were associated with increased corticosterone levels and regulatory T (Treg) cell numbers and decreased levels of pro-inflammatory cytokines, TH1 and TH17 cells as well as antigen-presenting cells, promoting oligodendrocyte precursor cell regeneration and remyelination in axons and suppressing both autoimmunity and remyelination. 70 Importantly, a recent systematic review and network meta-analysis of 12 randomized trials, comparing 8 dietary interventions (low-fat, Mediterranean, ketogenic, anti-inflammatory, Paleolithic, fasting, calorie restriction, and control/usual diets) and enrolling 608 participants was performed to assess the efficacy of different dietary approaches on MS-related fatigue and quality of life. 71 In accordance with our results, this meta-analysis supported evidence that MD may exert greater reductions in fatigue as well as in physical and mental health and quality of life compared to control group. 71 However, because of the limitations of the network meta-analysis, which were driven by the low quality of the included trials, the above findings should be confirmed by high-quality, randomized, controlled trials.
Despite the recent advances in immune-modulatory drugs, pharmacological therapies have been proven ineffective in severe presentations of MS. 72 Among complementary treatments, nutritional interventions have been considered a promising and decisive factor to control symptoms and enhance the wellness of peoples with MS. Several nutritional supplements revealed differences in antioxidant and anti-inflammatory parameters among patients, with a subsequent improvement in fatigue. 73 Moreover, several substantial studies have documented a systematically high prevalence of vitamin A, B12 and D3 deficiency amongst peoples with MS, which could be ameliorated by dietary supplements administration. 74 At present, clinical data have suggested that most of the dietary supplements under study may exert antioxidant and anti-inflammatory properties which are highly related with MD, improving depression symptomatology, quality of life overall and life expectancy. 73 However, there is currently non effective and adequate clinical indication for applying dietary supplementation as complementary treatment against MS symptomatology. 74
The present study has several strengths as it was performed in an adequate sample size of older adults with MS who had non any additional severe chronic disease except for MS. This fact has provided substantial evidence for the impact of MD against disability and symptom severity, independently of potential comorbidities, which may affect the potential beneficial effect of MD against MS. 12 A strength of our study also deals with the assessment of several sociodemographic characteristics and BMI status which may exert a confounding effect concerning the association of MD with disease disability and symptom severity as well as quality of life. Another strength of our study was the used of qualified questionnaires such as EDSS, GDS, STAI-6, PSS, MMSE, IPAQ, PSQI and MedDietScore, to assess disability and symptom severity, depression, anxiety, stress, cognitive status, physical activity, sleep quality, and MD adherence of the enrolled study population, respectively. Moreover, another advantage is the performance of face-to-face interviews in an isolated relaxed environment with the individuals with MS which increase the reliability and accuracy of their responses and reduce recall biases. Moreover, the study population was carefully selected to include an equal representation of all age groups beyond 65 years old. In addition, the present study has reinforced the evidence of previous studies concerning the positive impact of MD on disability and symptom severity, depression, anxiety, stress, and cognitive status.
However, the interpretation of the present findings should be made with some limitations in mind. The cross-sectional design of the present study limits the possibility for etiological conclusions and exhibits the potential of recall biases, especially for self-reported questions, even if we have performed face-to face interviews. Furthermore, although a comprehensive approach for confounding adjustment was applied, we should recognize the probability of undetermined confounders. Although we have applied adjustment for age, gender, educational and financial status, living status, smoking habits, nationality, and BMI status, there is still the possibility that residual confounding may affect our findings. On the other hand, the fact that no conclusions about causality can be obtained due to the cross-sectional design of our study should be emphasized. Drug prescriptions and supplementation usage may be another potential confounding factors that should be taken into consideration in future studies.
Conclusions
To the best of our knowledge, this is 1 of the few observational, cross-sectional clinical studies, which has investigated the association of MD adherence with several aspects of mental health in older adults with MS. This study has provided evidence that adopting MD at higher levels was associated with lower prevalence of disability and symptom severity, depression, anxiety, perceived stress, inadequate sleep quality, cognitive impairment, and physical inactivity in older adults with MS. Further well-designed, population-based prospective studies should be performed to obtain conclusive results for the potential beneficial effects of MD in this age group of adults with MS. Future public health strategies and policies should inform the general population as well as the older adults with MS for the favorable impacts of MD in preventing human diseases and in improving potential mental health disturbances in MS such as depression, anxiety, perceived stress, inadequate sleep quality and cognitive impairment.
Footnotes
Author Contribution
Conceptualization: T.V., K.V., G.T., A.S., andand C.G.; Data curation: C.T., E.P., O.A., M.M., D.A., S.K.P. and E.-P.A; Formal analysis: C.T., E.P., T.V., O.A., M.M., and G.A.; Investigation: C.T., E.P., S.K.P., K.V., A.S., S.K.P., E.-P.A., and C.G.; Methodology: C.T., T.V., K.V., G.T., A.S., S.K.P., and C.G.; Project administration: C.G.; Resources: C.T., E.P., M.M., O.A., G.T., and G.A.; Supervision: C.G; Visualization: T.V., K.V., G.T., A.S., S.K.P, and C.G.; Roles/Writing - original draft: C.T, E.P., O.A., G.T., and C.G.; and Writing - review & editing: K.V., T.V., and C.G.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Christina Tryfonos was funded by YPATIA, a scholarship of the University of the Aegean.
Data Availability Statement
Data are available upon request to the corresponding author.