
Abstract
Objective
To conduct the association between vitamin D levels in the acute phase of stroke and post-stroke depression (PSD) in stroke patients.
Methods
Five international databases (PubMed, Web of Science, Embase, Ovid MEDLINE(R), Cochrane Library) and one Chinese database (Wanfang Data) were searched for observational studies in any language reporting on PSD and vitamin D levels tested in the acute phase of stroke in stroke patients from inception to May 2024. Data extraction and study quality assessment were conducted by two authors independently. Qualitative and quantitative analyses of data were performed. The meta-analysis was registered in the PROSPERO database (CRD42023398581).
Results
We included 7 studies containing 3537 participants in the systematic review and meta-analysis. All studies that met the inclusion and exclusion criteria were conducted in China. Vitamin D levels in the acute phase of stroke were lower in PSD patients compared with non-PSD patients (weighted mean difference = −14.97 nmol/L; 95% confidence interval = −19.54, −10.40). Stroke patients with vitamin D deficiency (<50 nmol/L) had an increased risk of PSD compared with stroke patients with vitamin D sufficiency (≥75 nmol/L) (odds ratio = 3.59; 95% confidence interval = 2.05, 6.27). However, the association between vitamin D insufficiency (50-75 nmol/L) and PSD were not statistically significant (odds ratio = 4.15; 95% confidence interval = 0.87, 19.78).
Conclusion
Vitamin D deficiency in the acute phase of stroke may be a risk factor for PSD.
Introduction
Post-stroke depression (PSD) was the most common and serious neuropsychiatric complication after stroke. 1 The estimated cross-sectional prevalence of PSD was 18%–33%, and the cumulative prevalence of PSD was 39%–52% within 5 years of stroke.2,3 PSD was linked to higher mortality, more long-term disability, poorer health-related quality of life and higher rates of suicidal ideation.4-7 Therefore, it is necessary to find out the risk factors for PSD to prevent the onset of depression or reduce depressive symptoms.
Vitamin D, an essential nutrient for skeletal health, can convert to the steroid hormone, 1, 25-dihydroxyvitamin D3 (1,25 [OH]2D3), which has been found to play a great role in preventing cancers, modulating the immune system, and controlling endocrine systems by activating vitamin D receptor (VDR).8,9 Recently, some studies presented the potential association between lower vitamin D levels and PSD.10-12 Serum vitamin D levels measured in the acute phase of stroke were lower in the PSD group as compared to the non-PSD group at the time of 6 months after stroke onset. 10 Several prospective cohort studies suggested that lower serum levels of vitamin D determined at admission were associated with a higher presence of PSD at follow-up.10,11
However, it is still indeterminate whether there is a difference in the vitamin D levels between PSD and non-PSD patients, and whether the incidence of PSD differs significantly between patients with lower vitamin D levels and higher vitamin D levels. Therefore, we conducted a systematic review and meta-analysis to investigate whether there was a difference in vitamin D levels measured in the acute phase of stroke between the PSD and non-PSD patients, and whether lower vitamin D levels increased the risk of PSD.
Methods and Materials
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 13 The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with a registration number of CRD42023398581 at https://www.crd.york.ac.uk/prospero/.
Search Strategy
We searched five international databases (PubMed, Web of Science, Embase, Ovid MEDLINE(R), Cochrane Library) and one Chinese database (Wanfang Data) in any language from the earliest data available until May 2024. The search strategy was used as follows (Supplemental Table 1-6): (1) Stroke, merged the Medical Subject Headings (MeSH) and the free text words; (2) Depression, merged the MeSH and the free text words; (3) Post-stroke depression, combined different forms (Post stroke depression OR Poststroke depression); (4) Vitamin D, Cholecalciferol, Ergocalciferols, merged the MeSH and the free text words. We combined these terms: [(1 and 2) or 3] and 4. References quoted by retrieved articles were also searched for any other eligible studies.
Eligibility Criteria
The inclusion criteria for eligible studies were as follows: (1) Design: cohort or case-control studies; (2) Participants: patients diagnosed as acute stroke; (3) Exposure: vitamin D levels were tested in the acute phase of stroke, which was defined as stroke onset within one month. 25-hydroxyvitamin D (25 [OH]D) was used for the measurement of vitamin D levels. 14 Vitamin D deficiency was defined as serum 25 [OH]D levels <50 nmol/L; vitamin D insufficiency was defined as 50 nmol/L≤ serum 25 [OH]D levels <75 nmol/L; vitamin D sufficiency was defined as serum 25 [OH]D levels ≥75 nmol/L15-17; (4) Comparison: stroke patients without depression; (5) Outcome: PSD was diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria or a score above a cut-off point in a professional scale test; (6) Available data: studies presented the mean and standard deviation (SD) of vitamin D levels in PSD and non-PSD group, or odds ratio (OR) or relative risk (RR) or hazard ratio (HR) and 95% confidence interval (CI) for PSD for vitamin D deficiency or insufficiency v. Vitamin D sufficiency. The exclusion criteria were as follows: (1) other study designs (reviews, comments, case reports, study protocol, letters, interventional studies); (2) no association was presented between vitamin D levels and PSD; (3) no full paper. In case of overlapping cohorts, we chose the most recent comprehensive results with the largest sample size from the report. Two researchers worked independently to assess the eligibility of the literature. Disagreements were solved by consulting the third researcher.
Data Extraction
Data were independently extracted from eligible studies by two researchers, including the first author’s name, study type, location, sample size, sex, age, type of stroke, stroke assessment method, depression assessment method, time points of depression assessment, vitamin D levels in PSD and non-PSD group, P-value/OR/RR/HR for PSD.
Quality Assessment
Methodological quality assessment was independently performed by two calibrated authors using the Newcastle-Ottawa Scale (NOS) for cohort and case-control studies. 18 We assessed the quality of the included studies on three domains: selection (5 points), comparability (2 points), and outcome (3 points). The follow-up rate >80% was defined as follow-up within the acceptable range. Scores of 7-10, 4-6, and 0-3 indicate high, moderate, and low-quality studies, respectively. Disagreements would be figured out through consulting the third researcher.
Statistical Analysis
Statistical analysis was performed using Stata statistical software 14.0. Considering the heterogeneity in clinical (demographic characteristics) and methodological (measurement method) aspects of included studies, we applied a random effect model to perform the meta-analysis. For the continuous variable, mean ± SD was obtained to estimate the pooled effects using weighted mean difference (WMD) and 95% CI. Related equations were performed to obtain the preferred data from the median ± range or interquartile range.19,20 For the categorical variable, OR/RR/HR was obtained to calculate the pooled OR/RR/HR and 95% CI.
Heterogeneity was checked using the I2 test. Low, moderate, and high levels of heterogeneity correspond to I2 values of
Results
Literature Search
Overall, the search yielded a total of 613 records (Figure 1). After duplicate removal, 454 records were screened for titles and abstracts, and 27 records fulfilled the inclusion criteria. The authors retrieved and reviewed 27 records based on the full text. Lastly, seven records with eleven studies involving 3537 participants were included in the systematic review and meta-analysis. Flow diagram of articles related to PSD and vitamin D (VD).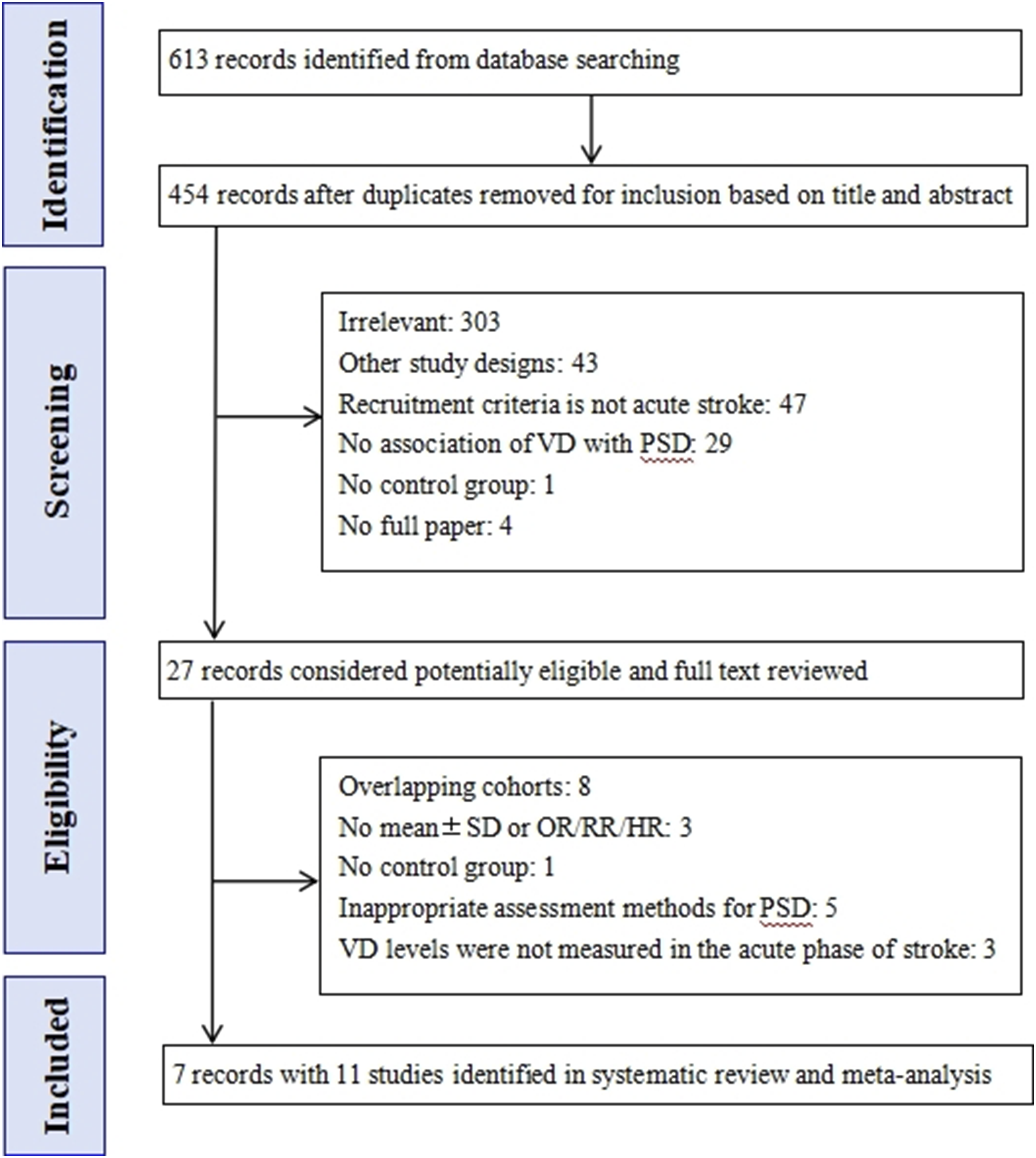
Study Characteristics
Characteristics of Included Studies.
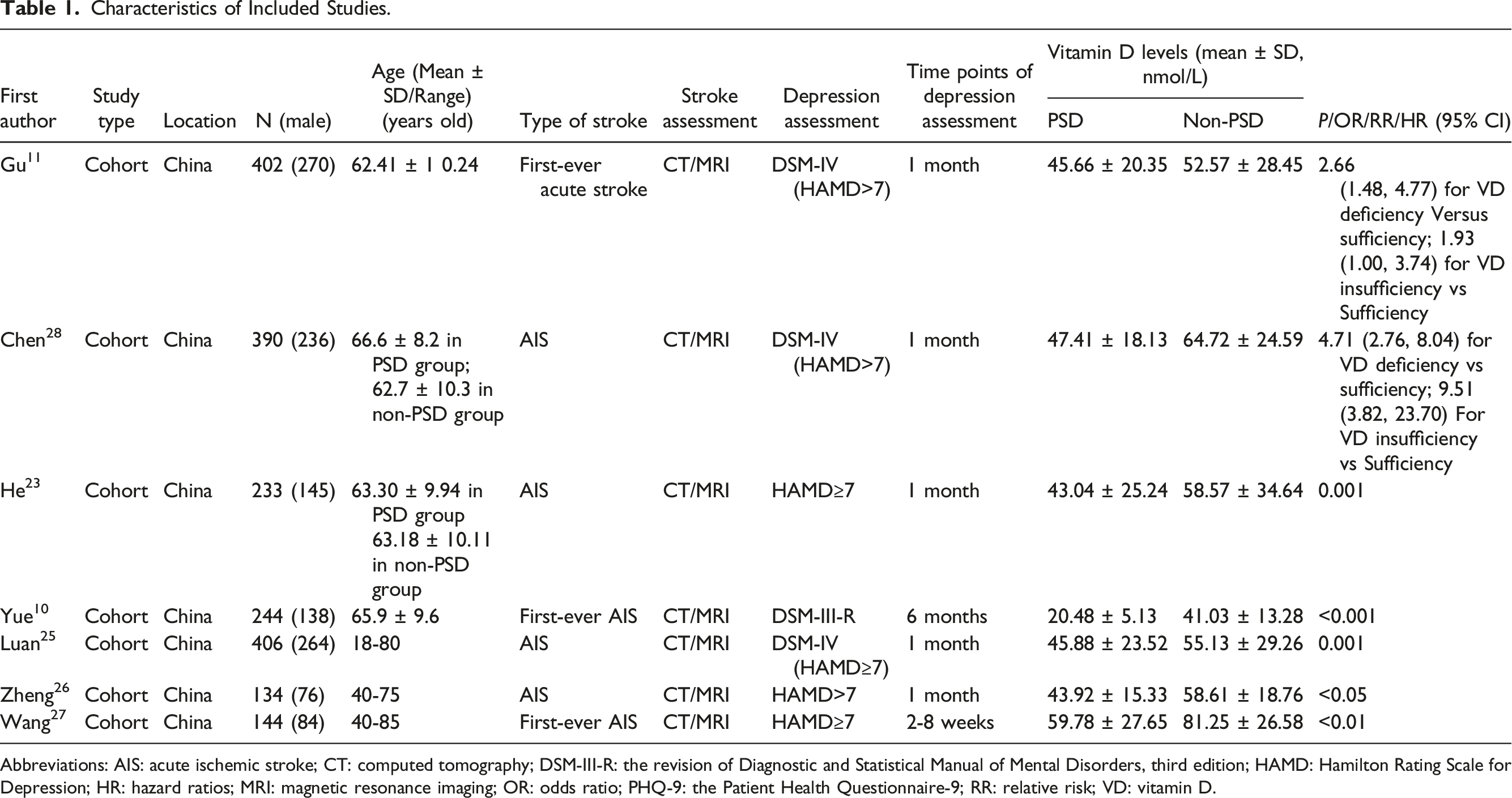
Abbreviations: AIS: acute ischemic stroke; CT: computed tomography; DSM-III-R: the revision of Diagnostic and Statistical Manual of Mental Disorders, third edition; HAMD: Hamilton Rating Scale for Depression; HR: hazard ratios; MRI: magnetic resonance imaging; OR: odds ratio; PHQ-9: the Patient Health Questionnaire-9; RR: relative risk; VD: vitamin D.
Ten studies presented that patients with pre-stroke depression history were excluded,11,23,25-28 but this medical history was not mentioned in one studies. 10 The follow-up period ranged from 2 weeks 27 to 6 months. 10 Overall, the P-value of all studies compared the mean vitamin D levels between PSD and non-PSD group was less than 0.05.
Quality Assessment
The NOS scores of the included studies are shown in Table S7. Ten studies had high-quality study designs11,23,25-28 and one studies were moderate-quality. 10 The main reason for bias arose from the comparability and non-response rate.
Meta-Analysis
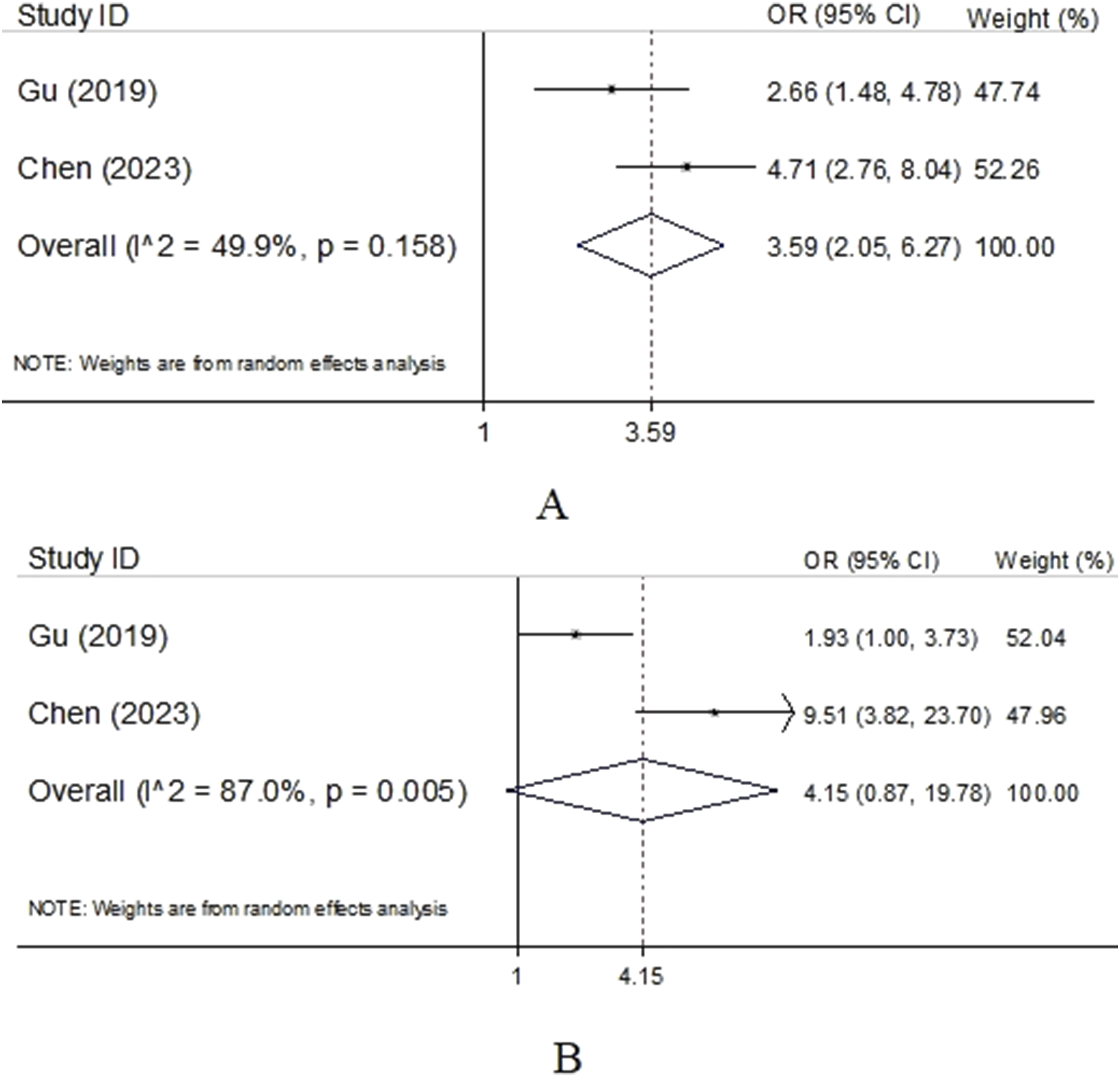
Seven studies,10,11,23,25-28 involving 1953 (PSD: 569 vs non-PSD: 1384) stroke patients, were analyzed to compare mean 25 [OH]D levels between patients with PSD and non-PSD. 25 [OH]D levels measured in the acute phase of stroke were significantly lower in the PSD group as compared to non-PSD group (WMD = −14.97 nmol/L; 95% CI = −19.54, −10.40; I2 = 82.6%; P < 0.001) (Figure 2). A meta-analysis of two prospective cohort studies comparing vitamin D-deficient (<50 nmol/L) stroke patients with vitamin D-sufficient (≥75 nmol/L) stroke patients found a statistically significantly increased PSD risk (OR = 3.59; 95% CI = 2.05, 6.27; I2 = 49.9%; P < 0.05) (Figure 3). However, a combined analysis of two prospective cohort studies comparing vitamin D-insufficient (50-75 nmol/L) stroke patients with vitamin D-sufficient stroke patients found no statistically significantly increased PSD risk (OR = 4.15; 95% CI = 0.87, 19.78; I2 = 87.0%; P > 0.05) (Figure 3). Forest plot of studies of evaluating vitamin D levels in patients with and without PSD. Meta-analysis of the incidence of PSD with low versus normal vitamin D levels (>75 nmol/L) (A: vitamin D levels < 50 nmol/L; B: 50 nmol/L ≤ vitamin D levels < 75 nmol/L).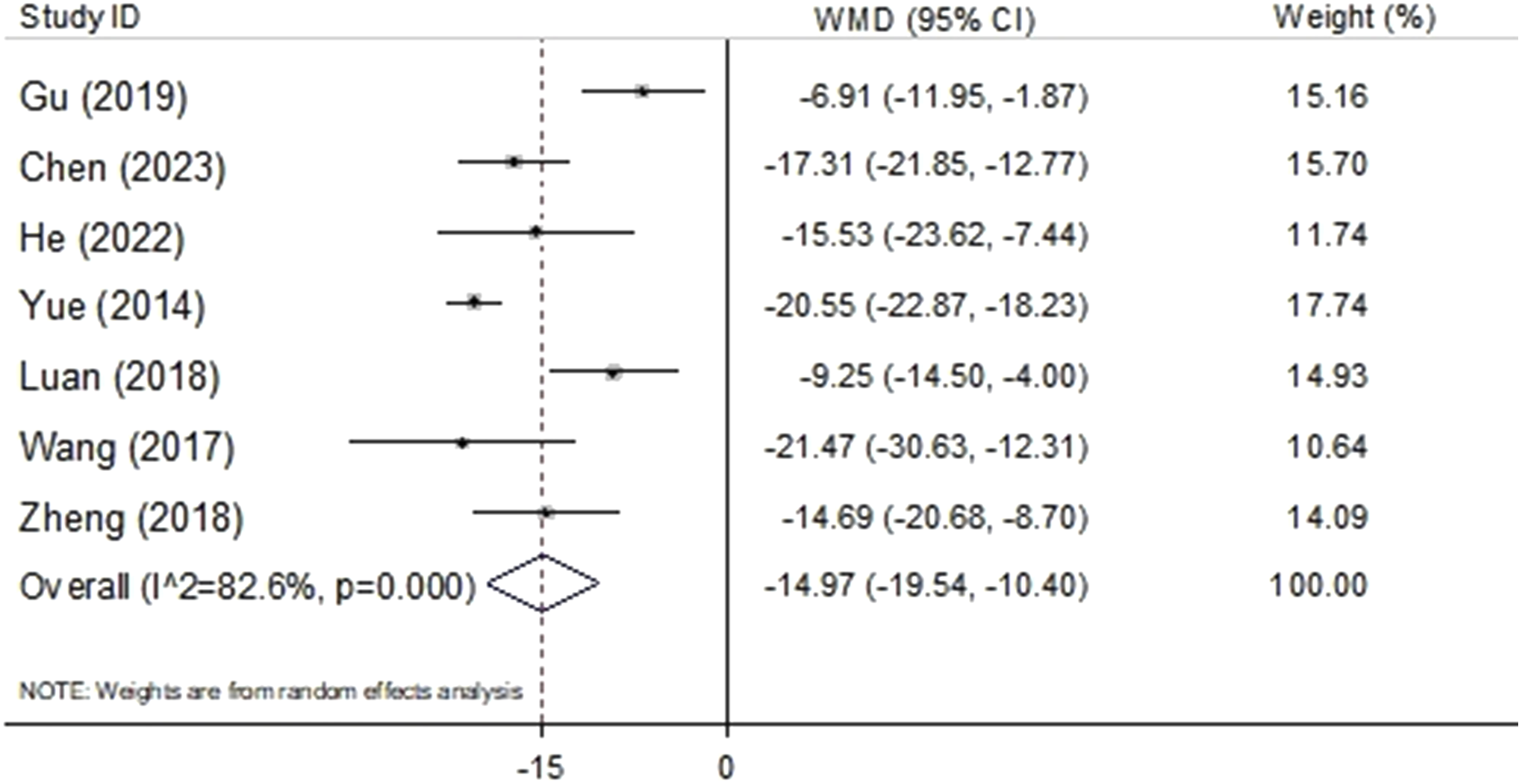
Subgroup Analysis
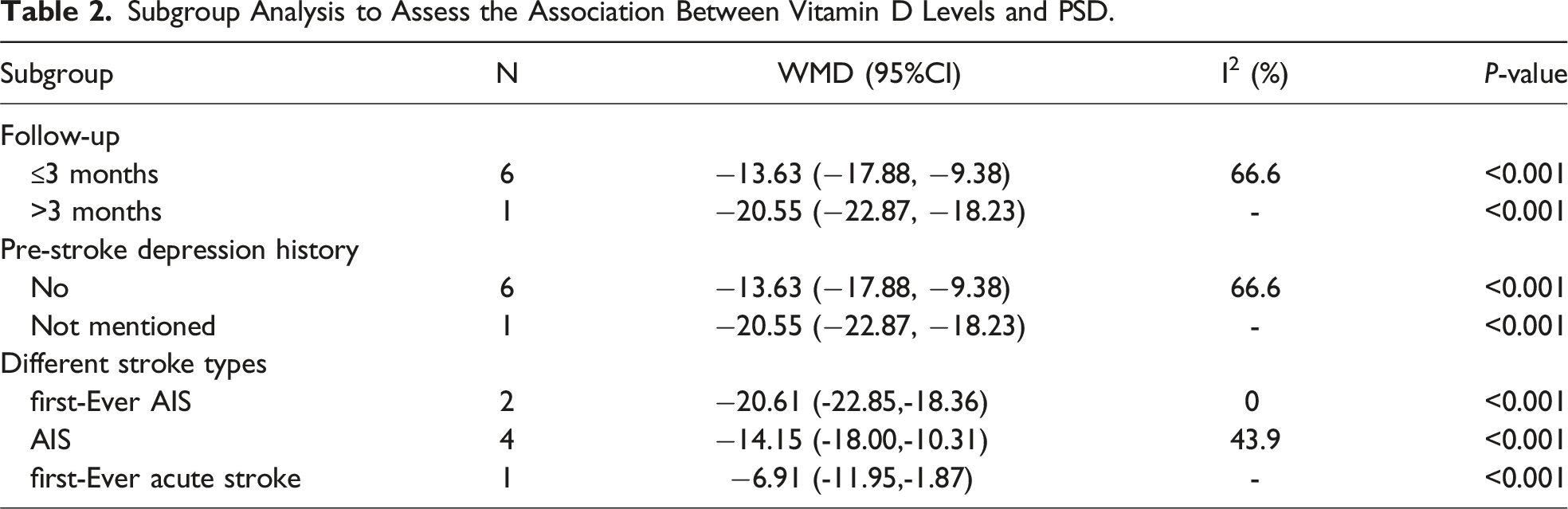
Subgroup Analysis to Assess the Association Between Vitamin D Levels and PSD.
Sensitivity Analysis and Publication Bias
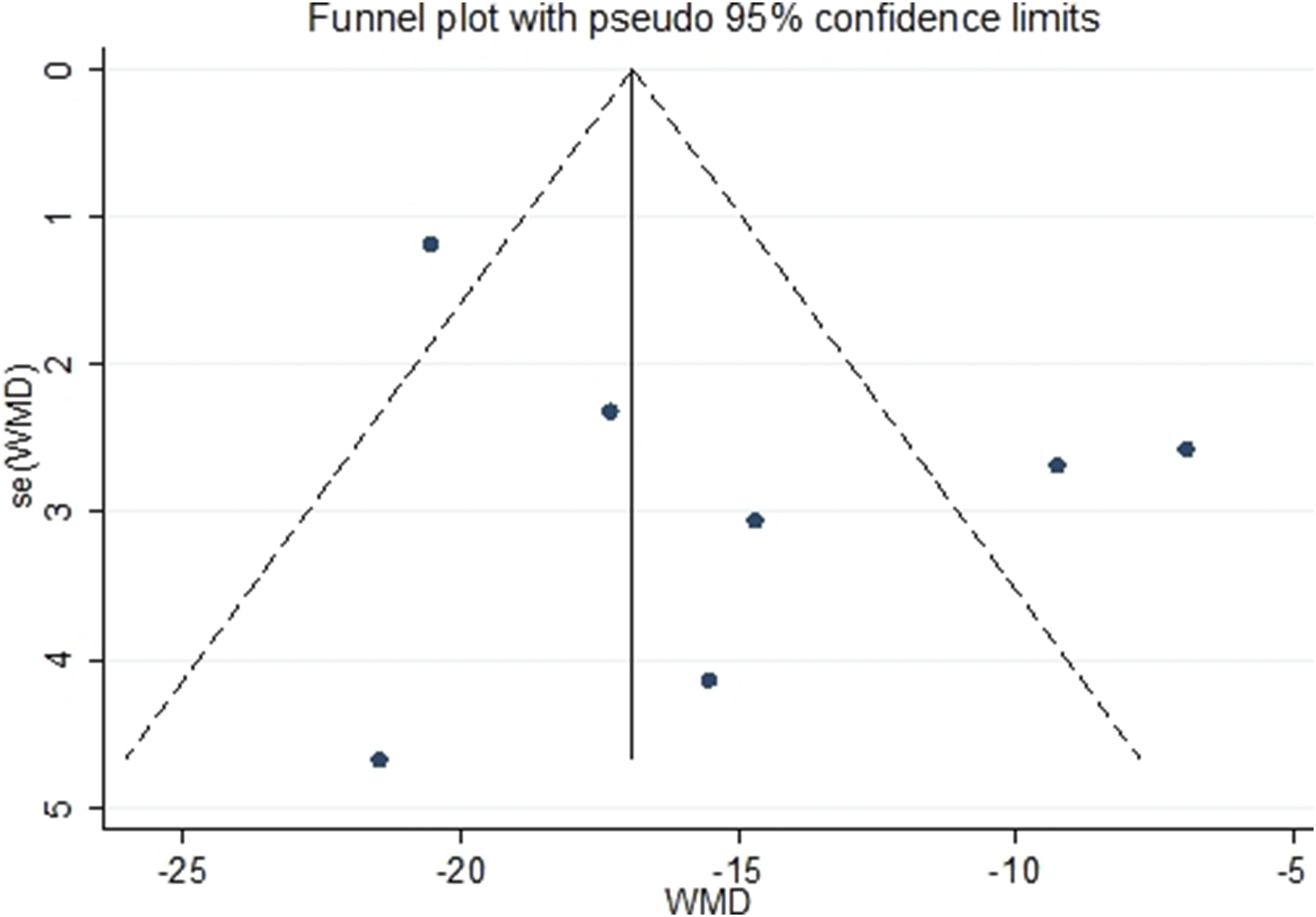
The sensitivity analysis demonstrated stable results (Figure 4). The funnel plot was symmetry (Figure 5). Egger’s test (P = 0.22) suggested no publication bias. Sensitivity analysis showing the impact of every study on the overall WMD estimate. Funnel plot of studies comparing vitamin D levels in patients with and without PSD.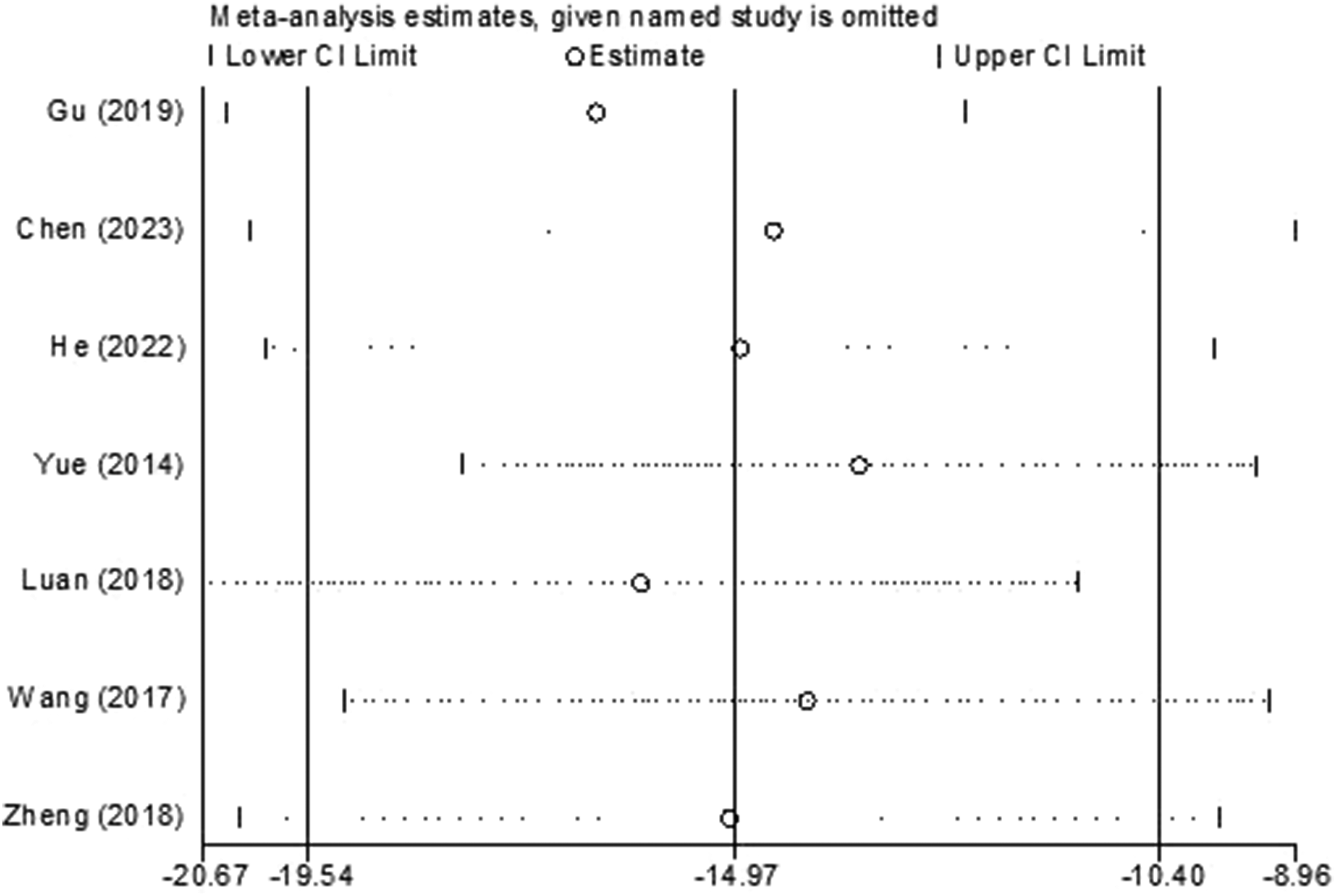
Discussion
The present meta-analysis summarized the existing evidences and synthesized the results of studies on the relationship between vitamin D levels tested in the acute phase of stroke and the incidence of PSD. The results suggested that 25 [OH]D levels were lower in the PSD group as compared to the non-PSD group in the acute phase of stroke. It indicated that vitamin D deficiency increased the risk of PSD.
Some studies also pooled evidence addressing the correlation between vitamin D status and the risk of PSD. Hung et al pooled incidences of vitamin D deficiency (25 [OH] D levels <50 nmol/L) and PSD of 60.1 and 26.1% in stroke patients, respectively. The study presented that lower circulating vitamin D levels in patients with PSD and a higher risk of PSD in patients with lower vitamin D levels, which was consistent with our findings. 29 Kurra et al showed significant clinical depression in the vitamin D deficient group on the BDI-II (SMD = 6.90, 95% CI = 3.32, 10.48; P = 0.0002) and PHQ-9 (SMD = 3.20, 95% CI = 1.84, 4.56; P < 0.00001) scales. 30 However, the results by Hung et al and Kurra et al were inaccurate because they pooled the standardized mean difference and adjusted odds ratio from overlapping cohorts. We chose the most recent comprehensive results with the largest sample size from the report, which made the results more persuasive. The two studies did not show a link between PSD and vitamin D deficiency or insufficiency. We presented the relationship between PSD and serum 25 [OH]D levels <50 nmol/L or 50 nmol/L ≤25 [OH]D levels <75 nmol/L, which was more relevant for clinical practice.
Genetic models suggested that the polymorphisms of vitamin D metabolic pathway genes VDR and CYP27B1 may be associated with PSD in patients with ischemic stroke. 31 After stroke, uncorrected vitamin D deficiency would continue to act on the central nervous system and then may result in the incidence of PSD. There were several possible pathophysiologic mechanisms on the correlation between vitamin D deficiency and PSD. Firstly, VDR were expressed widely throughout the human brain, including neurons and glia, 32 which mediated the effects of vitamin D on brain development and function. 33 Secondly, vitamin D regulated the expression of neurotrophic factors, such as glial cell line-derived neurotrophic factor (GDNF), nerve growth factor (NGF), and brain-derived neurotrophic factor (BDNF), which play a great role in the occurrence of PSD.34,35 Thirdly, 1,25 [OH]2D3 coordinated the biosynthesis of neurotransmitters, such as serotonin, norepinephrine, and dopamine, which may explain the putative role in the development of PSD.36-38 Lastly, vitamin D exerted acute anti-inflammatory and neuroprotection actions after stroke. 39
Several studies presented the association between vitamin D and PSD, but we cannot perform a meta-analysis based on these studies according to our eligibility criteria. Yue et al 10 suggested that the optimal cutoff value of serum 25 [OH]D levels as an indicator for predicting PSD was 28 nmol/L according to the receiver operating characteristic (ROC) curves and 25 [OH]D <28 nmol/L was associated with an increased risk of PSD (OR = 10.32; 95% CI = 4.97, 28.63; P < 0.001), after adjustment for age, sex, BMI, season of admission, stroke syndrome, stroke etiology, the NIHSS score, infarct volume, vascular risk factors, high-sensitivity C-reactive protein levels, homocysteine levels and a history of depression. The optimal cutoff value of 25 [OH]D level as an indicator for predicting of PSD may not be equal to the cutoff value of vitamin D deficiency, which suggested that researchers could try to find out the optimal predictive value for PSD with a larger sample size in the future. Asuman et al 40 revealed that vitamin D levels negatively correlated with the severity of depression symptoms in PSD (r = - 0.234; P < 0.001). Vitamin D levels measured within 3 months before the onset of stroke were not correlated to PSD at the 3-month and 12-month follow-up based on the TriNetX Diamond research network (Cambridge, MA, United States). 41 In clinical practice, the vast majority of stroke patients were screened for vitamin D after admission to predict the prognosis of stroke. Therefore, this study was limited in clinical application.
When we combined the results of the studies, a large degree of heterogeneity was observed (I2 = 82.6%). Subgroup analysis and sensitivity analysis were conducted to explore the source of heterogeneity. We set three subgroups, including whether PSD occurred within three months of stroke, whether patients had a pre-stroke depression history, and which stroke type was used as the inclusion criterion. Depressive symptoms often occurred within the first three months after stroke and less frequently later. 42 Therefore, we divided the participants into two groups as follow-up time within three months and beyond three months. We found that vitamin D levels were lower in the PSD group compared with the non-PSD group within three months with decreased heterogeneity (I2 = 66.6%). Pre-stroke depression history as an important confounding factor may interfere with the results. On the one hand, participants with pre-stroke depression may present lower levels of vitamin D than those without pre-stroke depression. On the other hand, pre-stroke depression history may influence the assessment of PSD and antidepressant therapy may decrease the prevalence of PSD. Our results showed that PSD patients without pre-stroke depression history had lower vitamin D levels compared to non-PSD with decreased heterogeneity (I2 = 66.6%). The different stroke types affected the heterogeneity of the results combined. There was no heterogeneity in the subgroup of the first-ever AIS (I2 = 0), and middle heterogeneity was observed in the subgroup of AIS (I2 = 43.9%). AIS contains first-ever AIS and recurrent AIS. Evidence supported that 25 [OH]D levels in patients with recurrent stroke were significantly lower as compared to patients without recurrent stroke and 25 [OH]D levels were negatively correlated with the risk of stroke recurrence.43,44 After excluding the study by Gu et al, 11 the I2 decreased to 71.4%, which may be the reason for recruiting patients with acute stroke, including atherothrombotic, cardioembolic, lacunar, and hemorrhage stroke, which was different from other studies for recruiting patients with acute ischemic stroke. After excluding the study by Yue et al, 10 the I2 decreased to 66.6%, which may contribute to the longest follow-up time (6 months) in this study.
This study had several advantages. Firstly, we applied a pragmatic design and comprehensive search strategy to provide the most up-to-date evidence on vitamin D and PSD. Secondly, the meta-analysis included an expanded sample size, which decreased sampling error and made it possible to draw reasonable conclusions. Lastly, the pooled OR from the original studies was obtained after adjustment for possible confounding factors, which made the results more credible.
This study also had several limitations. Firstly, it was a pity that all the studies in our review were conducted in China, and we did not obtain studies from other countries that could be included in our meta-analysis. We looked forward to researches from other countries or regions in the future. Secondly, we did not conduct a dose-response analysis of the association between PSD and vitamin D levels. Thirdly, the value of these diagnostic tools for PSD were still questionable. The depressive symptoms of PSD were closely linked to the vascular injury, which were different from depressive symptoms of major depressive disorders without vascular injury in physiopathologic mechanisms. Brain damage, changed environment or diet, or neurological disability in the acute stage of stroke may result in some overlap symptoms for PSD such as decreased interest, sleep disturbances and appetite loss. Although PSD can be diagnosed using DSM-5 in criteria of depressive disorder due to another medical condition (stroke), these overlap symptoms were one of the difficulties in distinguishing between PSD and post-stroke symptoms. 45 One strategy for determining whether symptoms indicated PSD was to keep an eye on the presence or absence of non-somatic symptoms like guilt, depressed mood, hopelessness, or worthlessness, which was more likely to indicate PSD. 2 Lastly, there was a large degree of heterogeneity in the pooled results. The variations in the PSD severity, assessment method for vitamin D, comorbidities’ proportions, and standard care treatment strategies may influence the heterogeneity and the pooled result. However, we cannot conduct a subgroup analysis based on these factors because the included studies did not present relevant information.
Conclusion
This systematic review and meta-analysis showed that vitamin D deficiency in the acute phase of stroke may be a risk factor for PSD. It reminds clinicians or researchers to explore whether vitamin D supplementation can prevent PSD in the future. However, it is necessary to conduct more high-quality cohort studies based on a larger sample size and a longer follow-up time to better understand the association between vitamin D levels and PSD in stroke patients.
Supplemental Material
Supplemental Material - Vitamin D Deficiency in the Acute Phase of Stroke May Predict Post-stroke Depression: A Systematic Review and Meta-Analysis
Supplemental Material for Vitamin D Deficiency in the Acute Phase of Stroke May Predict Post-stroke Depression: A Systematic Review and Meta-Analysis by Yongjun Tan, Xiaojun Jing, Jiani Wang, Li Zhou, Yilin Wang, Hua Zhang, and Qin Yang in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
Qin Yang, Yongjun Tan, and Xiaojun Jing made substantial contributions to the conception or design of the work. Yonjun Tan drafted the manuscript. Qin yang revised it critically for important intellectual content and gave final approval of the version of the manuscript to be published. All authors contributed to the acquisition, analysis, and interpretation of data for the work and agreed to be accountable for all aspects of the work, in terms of ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Chongqing Municipality; cstc 2021jcyj-msxmX0263; National Natural Science Foundation of China; 81971229; National Natural Science Foundation of China; 82171456.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.