
Abstract
Objective
Social factors can influence the brain’s dopaminergic function. This study investigated the relationship between socioenvironmental factors and dopamine transporter (DaT) availability in healthy individuals (n = 74) and those with Parkinson’s disease (PD) (n = 240).
Methods
All single photon emission computed tomography (SPECT) DaT data and clinical data used in this study were obtained from the Parkinson’s Progression Markers Initiative (PPMI) dataset. Socioenvironmental data was obtained from Social Explorer analyses of the American Community Survey (2014-2018) using the residential ZIP codes of the subjects available in the PPMI dataset.
Results
Participants resided in 302 ZIP code tabulation areas across 38 U.S. states. In healthy individuals
Conclusion
The study findings suggest that socioenvironmental factors, such as median household income, education level, and poverty rate, are significantly associated with DaT availability in the caudate of healthy individuals but not in those with PD. This indicates that PD might disrupt the connection between the social environment and dopaminergic function. These results underscore the importance of considering socioenvironmental variables when studying dopaminergic function in the human brain.
Introduction
Social and environmental factors have been shown to influence brain dopaminergic function across different species.1-3 Neighborhood socioeconomic status (NSES) and individual-level socioeconomic status (SES) are the two main determinants of social health that can affect each other, as well as brain and psychiatric conditions. 4 Previous studies exploring the association between SES and dopamine function in humans using in vivo molecular imaging tools such as positron emission tomography (PET) and single photon emission computed tomography (SPECT) have shown mixed results. 5 While some studies reported a decrease in dopaminergic function under higher SES-related stressors in healthy humans and subjects with neurological disorders,6,7 others have showed opposite results.8,9 There are also studies that have shown no significant or inconsistent results.10-12 Most of the studies examining the effects of SES-related factors on dopaminergic functioning examined D2/3 receptor density with PET or SPECT imaging using different radiotracers (e.g., [11C]PHNO, [11C]raclopride, [18F]fallypride, [123I]IBZM) which might partially explain the heterogenous results.
Importantly, only a few studies reported data on dopamine transporter (DaT),13-15 a plasma membrane protein responsible for the reuptake of dopamine from the synaptic cleft into presynaptic neurons and essential for regulating synaptic dopamine levels. 16 Additionally, these available studies used subjects with recent-onset Parkinson’s disease (PD) 13 or Lewy Body dementia 14 diagnoses, and only a single study examined healthy humans. 15 Furthermore, individual educational levels were the only SES-related measure examined in the DaT studies, excluding other social features. 15 Thus, a recent review study on social stressors and dopaminergic function concluded that the generalizability of DaT findings is limited, and studies with more robust SES-related variables, along with examining healthy humans, are needed. 5
The first goal of the present study was to investigate the relationship between NSES and DaT signaling in the caudate and putamen, as well as individual-level educational status, in healthy humans. For NSES, we used each individual’s residential ZIP code. The second goal was to investigate whether NSES was associated with the DaT signal when we replicated the analyses in a disease known to be a main disruptor of the dopaminergic system, such as PD. This large cohort analysis attempts to fill the gap in this field by exploring large-scale associations of residential populations and socioeconomic variables with DaT availability.
Methods
Participants
Data used in the preparation of this article were obtained (March, 25, 2024) from the Parkinson’s Progression Markers Initiative (PPMI) database (https://www.ppmi-info.org/access-data-specimens/download-data), RRID:SCR_006431. For up-to-date information on the study, visit https://www.ppmi-info.org. Also, all the data used in this study is openly available from PPMI without utilizing any restricted dataset. Initially, PD subjects and HCs with available ZIP codes from the ‘FOUND_RFQ_Residential_History’ questionnaire were identified. ZIP codes where participants resided the longest were extracted and matched to each subject’s unique identifier ('patno'). During the ZIP code collection, 10 HCs and 1 PD subject were excluded due to incorrect or missing ZIP codes (inadequate digits in ZIP codes or ZIP codes outside of America). Data on DaT scans, obtained from the ‘DaTScan_SBR_Analysis' item, was used for further analysis. At this stage, eleven PD patients and three HCs were excluded due to missing DaT scan results. Consequently, 245 patients with PD diagnosis and 77 HCs were included in NSES data collection (see Figure 1). Flow diagram of the study population. *: Outliers are defined as 3 or more standard deviations above or below the mean.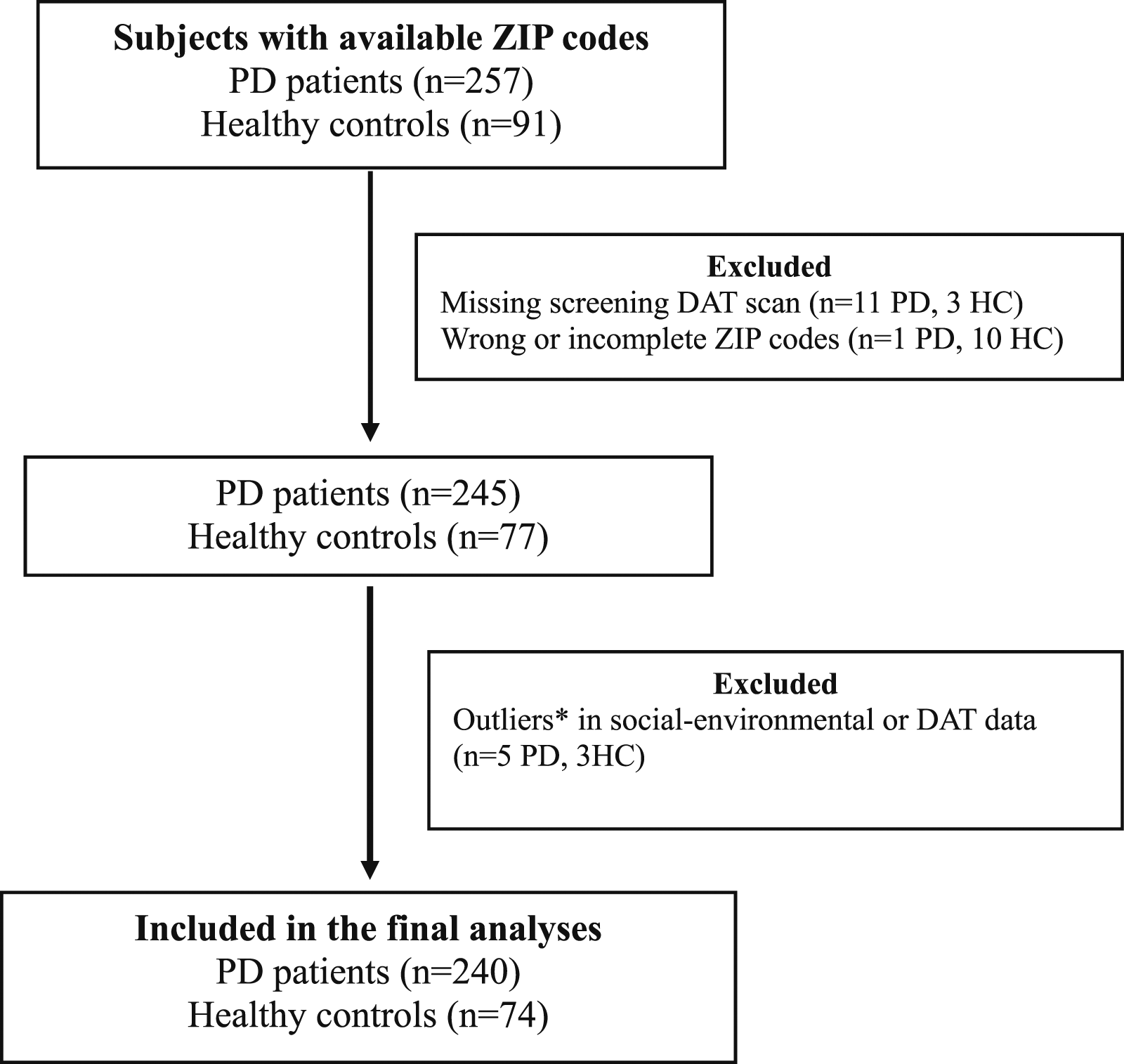
Regional DAT Data
DaT scan data was processed according to PPMI imaging protocols, available under the ‘DaTScan_SBR_Analysis' item, and was used in all analyses. Averages of mean regional striatal binding ratios (SBR; reference region: occipital lobe) for the caudate and putamen were calculated from the right and left hemispheres. Detailed information related to DaT scan processing procedures can be found at (https://www.ppmi-info.org/access-data-specimens/download-data/) and in published studies.17,18
Population and Social-Environmental Data
NSES measures for participants’ residential ZIP codes were obtained from the Social Explorer analyses of the 2014-2018 U.S. Census Bureau American Community Survey. 19 Selected variables included education level (percentage of the population aged ≥25 years with a bachelor’s degree or higher), median household income (in thousands of dollars, adjusted for inflation), poverty rate (percentage of the population aged 18-64 years living below the poverty threshold), total population, and population density per square mile. In addition to the demographic variables (age, sex, and education), clinical variables were collected for each subject. These included the Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) and the Montreal Cognitive Assessment (MoCA).
Statistical Analyses
Statistical analyses were performed using R version 4.4 and GraphPad Prism. The normality of continuous variables was assessed with a one-sample Shapiro-Wilk test. Total population, population density, and income data were found to be non-normally distributed and were log-transformed for analysis. Population and social-environmental data were then standardized (converted to z-scores). Five PD patients (with z-scores: −3.1, −3.2, 3.6, 3.9, and −3.4) and one HC (z-score = 3.2) were identified as outliers (≥3 SD from the mean) and excluded from further analysis.
Demographic, clinical, and neuroimaging data between PD and HC groups were compared using t-tests and chi-squared tests. Descriptive statistics are presented as means and standard deviations (SD). Correlations between ZIP code-related NSES characteristics and DaT data in the caudate and putamen of PD and HC groups were analyzed using two-tailed partial correlations with the ‘ppcor_1.1′ package, controlling for age, sex, and cognitive function (MoCA scores) due to known effects on DaT. 20 The analysis was repeated for PD subjects with available motor symptom severity data (n = 192), using the part 3 MDS-UPDRS score to control for disease severity. Tremor items were excluded from the total MDS-UPDRS-III score as they are not considered to be directly related to the dopamine signal. 21 P values were not corrected for multiple comparisons, considering the exploratory nature of the study.
Results
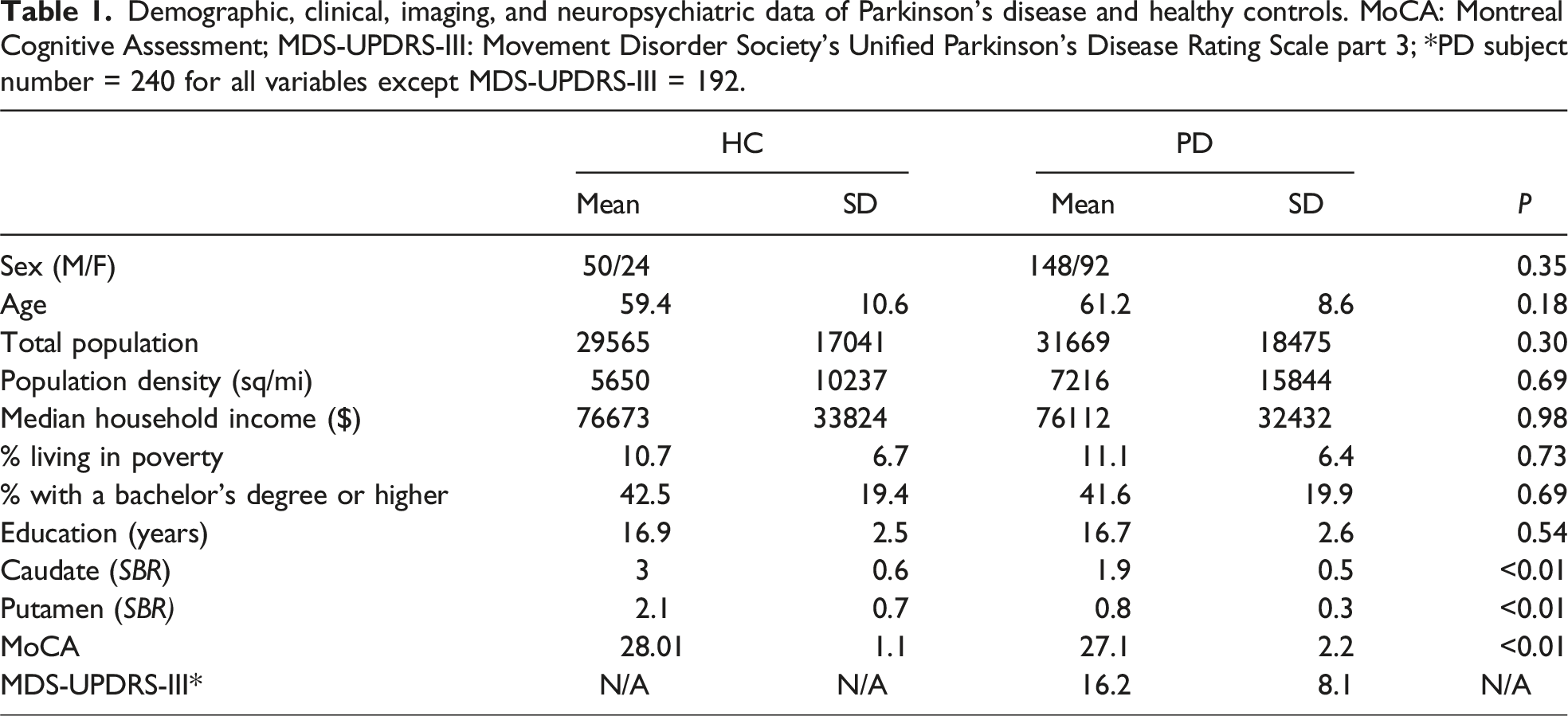
Demographic, clinical, imaging, and neuropsychiatric data of Parkinson’s disease and healthy controls. MoCA: Montreal Cognitive Assessment; MDS-UPDRS-III: Movement Disorder Society's Unified Parkinson's Disease Rating Scale part 3; *PD subject number = 240 for all variables except MDS-UPDRS-III = 192.
r: Pearson’s partial correlation coefficient for the association of neighborhood socioeconomic status with caudate and putamen dopamine transporter (DaT) results of healthy controls and subjects with Parkinson’s disease (PD) diagnosis. All results are corrected for age, sex, and Montreal Cognitive Assessment Scores. Movement Disorder Society's Unified Parkinson's Disease Rating Scale part 3 (MDS-UPDRS-III) corrected PD results are from a subset of PD subjects with Available MDS-UPDRS-III Scores.
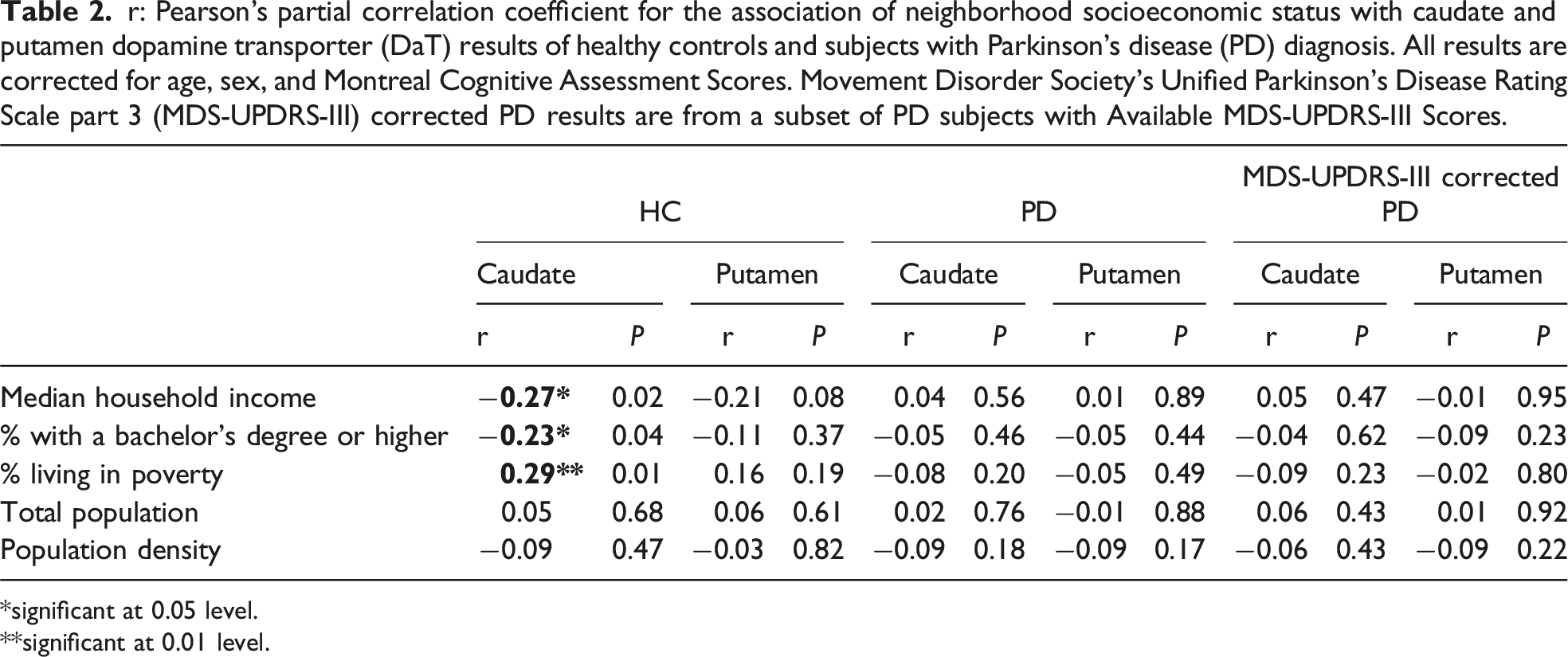
*significant at 0.05 level.
**significant at 0.01 level.
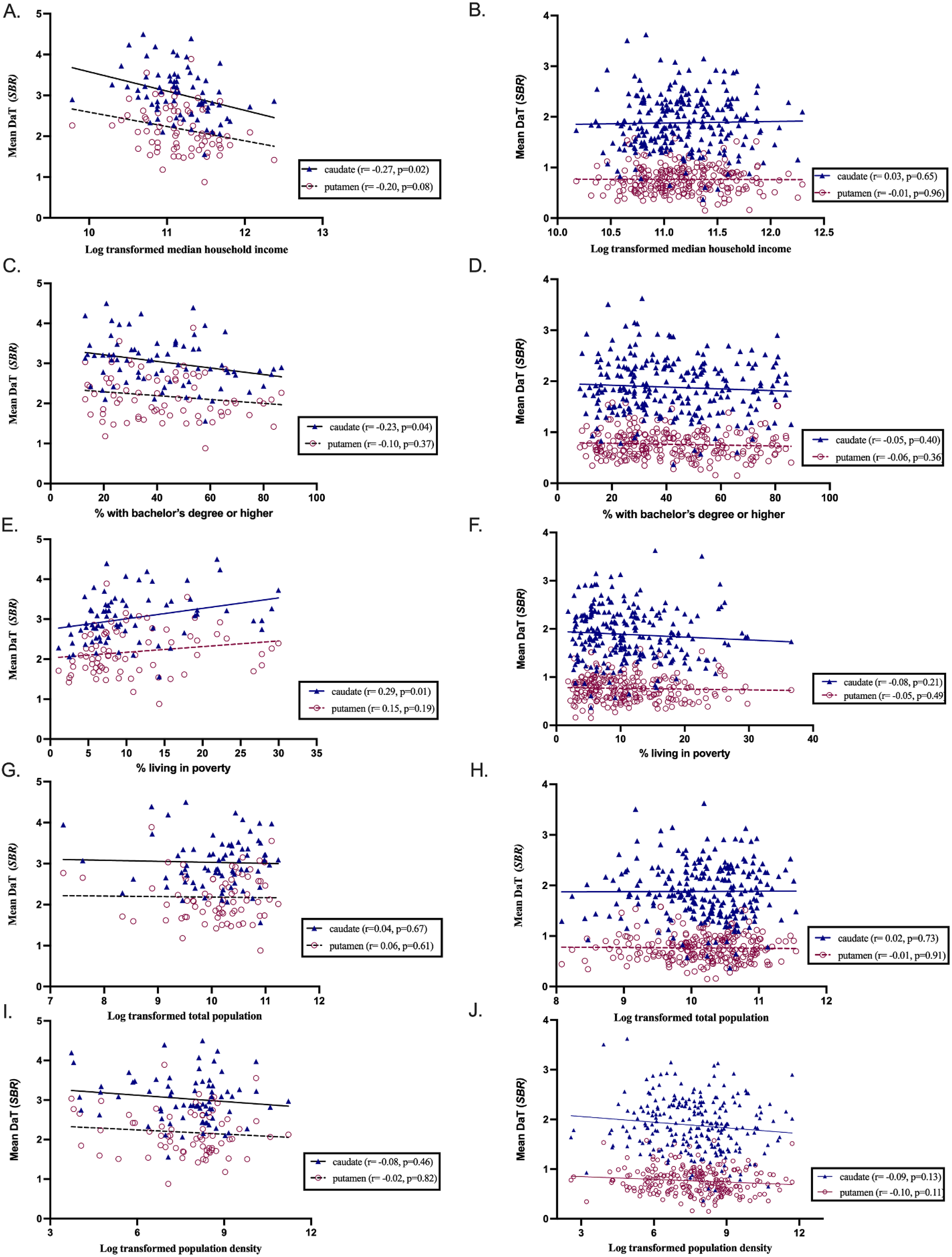
Scatterplots of the associations of neighborhood socioeconomic status with caudate and putamen DaT scan results (SBR). Pearson’s correlation results are significant at alpha = 0.05 level (uncorrected).
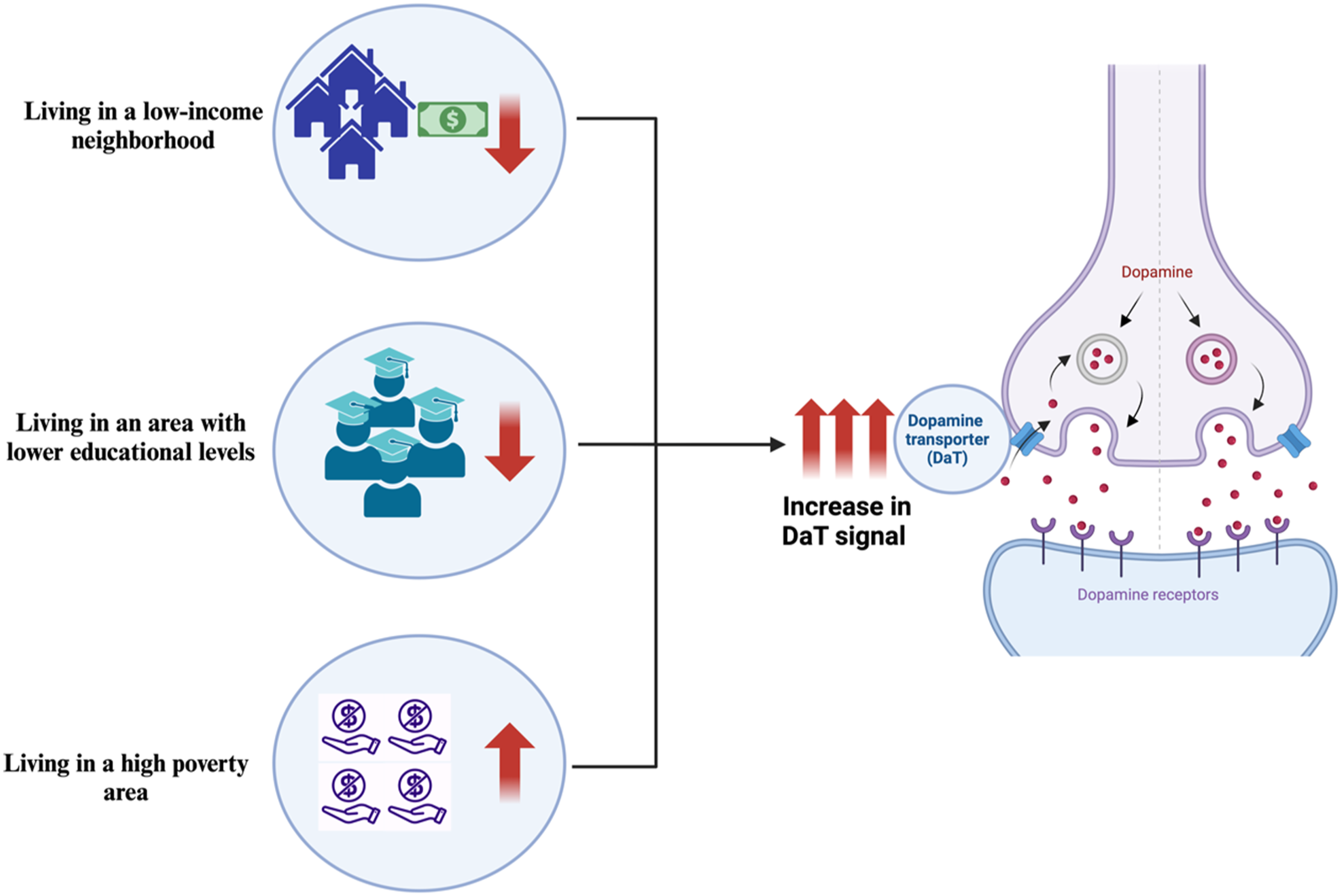
Schematic illustration of main findings.
In the PD group, no significant associations were found between any ZIP code-related NSES characteristics and DaT signals in the caudate and putamen (Table 2, Figure 2). When we repeated the analysis by controlling for motor symptom severity in subjects (n = 192) with available part 3 MDS-UPDRS scores, the results remained non-significant (Table 2).
Discussion
This study showed that living in an area with a lower percentage of residents holding bachelor’s degrees, lower household incomes, and higher poverty rates are associated with an increased DaT signal in the caudate. When we examined the PD subjects, no significant associations were found for any of those variables. Our findings suggest that socioenvironmental factors might influence the DaT signal in the caudate of a healthy human brain but not the PD, in which DaT loss is mostly driven by disease pathology. To our knowledge, socioenvironmental factors have not been examined in DaT PET or SPECT studies in HC and/or people with PD diagnosis. This report expands on the connections between neural functions and individual education levels, linking them to broader population characteristics.
Previous studies examining SES and DaT signals in humans have reported conflicting results, often with only education levels as SES-related variables. Sunwoo et al. reported a lower striatal DaT signal in the posterior putamen in PD patients with over 12 years of education compared to those with lower educational attainments. Meanwhile, Lamotte et al. have shown a positive correlation between educational level (years after the first grade) and DaT binding in the striatum in patients with Lewy Body dementia. Differences in subject characteristics may explain the different results observed across the two studies. Hoenig et al. recently conducted a study using the same dataset (PPMI) as in the current study, examining the education level as the only SES-related variable and DaT signal in the striatum of both HC and PD subjects. They found no significant associations between educational levels and DaT when correlating across the entire cohort, either in PD or HCs. However, significant associations were found when the analysis was repeated in specific age groups and different educational statuses. 15 Similarly, we did not observe any association between educational levels and DaT in our sample upon repeating the analyses. It is important to note that the mean level of education in both our PPMI cohort and that of Hoenig et al. was approximately 16 years, which may not reflect real-life circumstances. According to a major national population survey, only 35% of the population in the USA holds a bachelor’s degree or higher. 22 Although current literature on NSES and the dopamine system is insufficient for making conclusive statements, there may be explanations for the observed negative associations between NSES and the dopamine system in the current paper and our previous publication. 9 We believe that the higher binding of DaT or D2/3 ligands in the dopamine system might be due to a hypoactive dopamine system (i.e., less endogenous dopamine). Thus, observed lower NSES status in subjects with higher DaT availability might be explained by the effect of having fewer educational and financial resources that are stressors causing changes in the dopamine system. 23 However, more robust individual SES measures are needed to draw conclusive statements about these associations.
Aside from DaT, several epidemiological studies explored the association between SES and dopaminergic activity by examining the D2/3 receptor availability in healthy individuals and subjects with different neuropsychiatric conditions. 5 Findings across these studies were mixed. Heterogenous results in these studies might reflect the different radioligands used in various studies. Specifically, while some tracers ([11C]PHNO) used in these studies have high D3 specific affinity, others such as [11C]raclopride have a higher affinity for D2 receptors, which can introduce tracer-related variability. 24 Among these studies, two particularly examined the ZIP-code-based neighborhood-level SES and D2/3 receptor binding in HCs.9,10 Interestingly, in line with our findings, one of these studies concluded by Calakos et al. found an inverse relationship between D2/3 receptor binding and both the percentage of the population with a bachelor’s degree or higher and median household income. However, Wiers et al have shown no significant or inconsistent results when explored the socio-environmental factors and D2/3 receptor binding. Thus, similar to studies examining DaT, there is also limited literature to make a conclusive statement pertaining to the association between D2/3 receptor signaling and social factors.
Limitations
Several limitations emerge for the current study. The primary limitation is its cross-sectional and retrospective nature, which prevents the examination of changes in DaT levels in response to environmental factors longitudinally. Secondly, our study utilized ZIP codes as the basis for residential information to assess socioenvironmental factors. This approach limits the precision in capturing individual-level socioenvironmental characteristics, as ZIP code areas encompass broader neighborhoods that may exhibit significant heterogeneity in these factors. Additionally, we were unable to determine the exact duration of residence in the ZIP code area, which could introduce bias since this duration may vary among subjects. Third, P-values were not corrected due to the exploratory nature of our study which uses preliminary data without a well-designed study setting and more robust statistics. Lastly, there was male dominance in both HC and PD groups, which might introduce sex-related differences in the results. However, a previous study suggested no significant effects of gender on striatal D2/D3 receptor availability and social status in healthy volunteers. 6 Despite these limitations, this study has notable strengths, including a large sample size and the revelation of new connections between the brain and the environment.
Conclusion
In summary, the results demonstrate that living in an area with fewer collective educational resources, lower household income, and a more impoverished population is associated with higher caudate DaT availability. This is the first study to examine the relationship between socioenvironmental factors and DaT availability in both healthy controls and subjects with PD. Future prospective PET/SPECT studies with superior radioligands and more robust individual and neighborhood SES data are needed to explore further the influence of social factors on neural dopaminergic mechanisms.
Footnotes
Authors’ Contributions
Conception and design of the study: SC and DM. Data acquisition, analysis, and interpretation: SC, MT, DM. Statistical analysis: SC, MT. Drafting of the manuscript: SC. Revising the manuscript: SC, MT, DM.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health (NIH) with a grant number of R01NS124819.