
Abstract
Background
Idiopathic normal pressure hydrocephalus (iNPH) is a reversible cause of gait disturbance, cognitive decline, and urinary incontinence in older adults. Early detection with shunt surgery can significantly improve symptoms.
Methods
A systematic review following PRISMA guidelines evaluated the role of portable and smartphone-based accelerometers in quantifying gait parameters in iNPH.
Results
Across 32 studies, 22 different accelerometers were used, ranging from wearable inertial sensors to smartphone applications. The Three-Dimensional Pose Tracker for Gait Test (TDPT-GT) app was the most frequently utilized, enabling detection of pathological gait features such as shuffling, short steps, and wide-based walking. The G-Walk device was commonly used in clinical assessments, including before and after CSF tap tests. Several studies integrated accelerometry with machine-learning models, improving differentiation of iNPH from other neurological gait disorders.
Conclusion
Portable accelerometry offers an accessible, objective tool for diagnosis, monitoring, and prognostication in iNPH, with growing potential for routine clinical integration.
Keywords
Introduction
Idiopathic normal pressure hydrocephalus (iNPH) is a treatable form of communicating hydrocephalus mainly seen in elderly adults affecting men and women equally. Few studies have been conducted to determine its exact prevalence, currently estimated to lie between 10 and 22 per 100 000 in the general population, 1.3% in those over 65, and 5.9% in those over 80.1,2 Although the etiology and pathophysiology remain to be fully elucidated, iNPH is characterized by an increase in cerebrospinal fluid (CSF) volume, speculated to be due to a disruption of CSF flow dynamics and impaired CSF drainage and absorption. 1 This ultimately leads to ventricular enlargement, mechanical stress on brain parenchyma, hypoperfusion, neuroinflammation, and subsequent brain atrophy, despite normal intracranial pressure (ICP). 1
iNPH is described by a classic triad of gait instability, cognitive decline, and urinary incontinence. Diagnosis is often difficult, as these symptoms may be present in numerous other conditions of varying etiology such as dementia, cerebrovascular disease, and Parkinson’s disease (PD). 3 In order to make a diagnosis, current guidelines recommend using a combination of clinical history, brain imaging, and physical exam findings to categorize patients into “probable,” “possible,” and “unlikely” categories.3,4 Gait instability is typically the initial presentation, often described as “magnetic” and characterized by shuffling movements, difficulty in step initiation, and bradykinesia. Patients are generally placed in the “possible” category if they have more than one symptom of the triad not explained by any other neurological or non neurological disease, with evidence of ventriculomegaly on brain imaging. 3 Diagnostic criteria for each category are described in detail by the iNPH guidelines and Japanese Society of Normal Pressure Hydrocephalus.3,4
For detailed gait analysis, existing laboratories utilize cameras, force plates, and other instruments to quantify various gait parameters. However, these methods are expensive, cumbersome, and reserved for research studies. In most clinical settings gait is assessed through visual evaluation in the form of the timed-up-and-go (TUG) test, 10-meter walk test, and 2-minute walk test. The TUG test involves standing up from a chair, walking 3 meters, turning around, walking back to the chair, and sitting down. 5 If iNPH is suspected, these studies are often performed after lumbar puncture (LP), often referred to as a CSF tap test (CSF-TT), a diagnostic tool used to predict patient responsiveness to ventriculoperitoneal (VP) shunt placement. 6 Prior studies have shown discrepancies between objective and subjective evaluators of gait in iNPH patients. 7 Given that 70-90% of patients diagnosed with iNPH show clinical improvement following CSF drainage, early diagnosis and treatment are essential. 6
Accelerometers, present in commonly used electronic devices such as cell phones, tablets, smart watches, cameras, and video game controllers are used to measure linear acceleration. Accelerometry has been increasingly used to measure gait patterns and accurately quantifies gait, a variable historically defined by subjective and qualitative interpretation. These devices are small, portable, inexpensive in comparison to current gait-analyzing technologies, and do not interfere with patients’ inherent gait patterns. 8 Numerous studies have shown that portable accelerometers are equally effective, and potentially more effective, at quantifying gait parameters as compared to the gold standard laboratory gait assessment. Not only this, but because of their portable nature, gait analysis is possible both in the clinic and real-world settings. 9 A substantial amount of research has provided evidence that portable accelerometers can be used as a tool to enhance diagnostic accuracy, monitor disease progression, stratify risk, and evaluate therapeutic response in movement disorders such as PD, ataxia, and dementia. 10 It has been reported that portable accelerometry can even detect prodromal PD years before clinical diagnosis better than other methods such as genetics, lifestyle, biochemistry, and reported symptoms. 11 Given their affordability and utility they may be more accessible to iNPH patients and have the potential to measure multiple gait parameters including speed, cadence, stride length, step time, stance, swing, double support, lateral step variability, and foot strike angle. 12
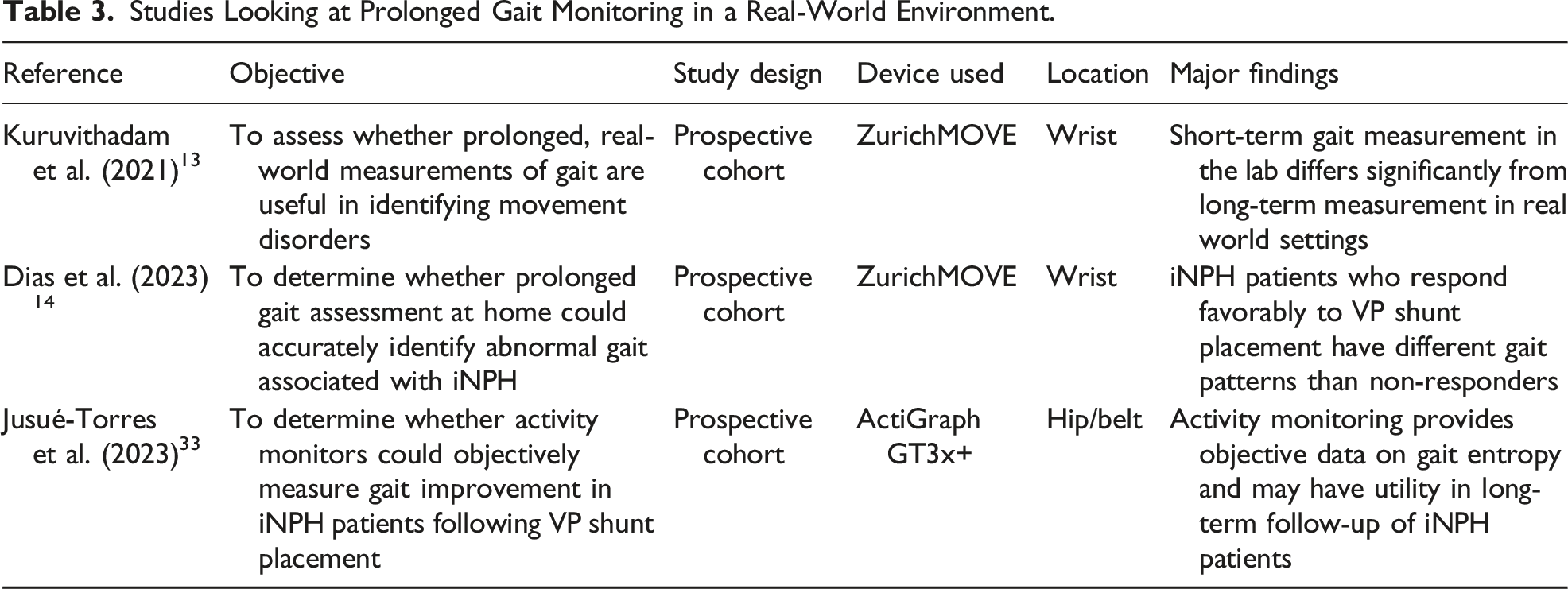
Gait improvement in iNPH remains the principal clinical outcome guiding both treatment decisions and postoperative follow-up, making changes in gait performance one of the most sensitive and clinically meaningful markers of therapeutic response. Contemporary reviews highlight the multidimensional nature of gait disturbance in iNPH, encompassing not only reduced speed and shortened stride length, but also abnormalities in balance, variability, turning, and gait initiation. This complexity suggests that brief, in-clinic assessments may fail to capture the full spectrum and temporal dynamics of gait impairment. Wearable accelerometry is therefore uniquely positioned to provide real-life, multiparametric, and continuous monitoring, extending beyond daytime walking to potentially include nocturnal or sleep-related movement patterns and smartphone-based assessments.13,14
Despite these advantages and growing evidence in other movement disorders, data on the use of portable accelerometers in iNPH remain limited. The purpose of this review is to identify how portable accelerometers can be used to quantify gait patterns in iNPH patients to facilitate early detection, accurate diagnosis, selection for surgery, and treatment.
Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were followed during the literature search. 15 This systematic review was prospectively registered in PROSPERO (Registration No. CRD420251249620) prior to the initiation of data extraction.
Search Strategy
A review of the literature was conducted using PubMed, Embase, Ovid, and Web of Science databases in July 2025. The search terms included: accelerometry, accelerometer, gait analysis, software, and normal pressure hydrocephalus. Terms included in either title, abstract, or key words were used to identify all relevant literature. Detailed search strategy for each data base is reported in Supplemental File 1.
Eligibility Criteria
Articles included were (i) any observational studies (cross-sectional, case–control, prospective, or retrospective cohorts), interventional trials (randomized, non-randomized, proof-of-concept), case-series, and case reports, (ii) published in a peer-reviewed journal, (iii) reported original data on gait assessment using portable or smartphone based accelerometry, (iv) in people with idiopathic normal pressure hydrocephalus (iNPH) only, or in mixed cohorts where iNPH patients were included, with or without a comparison to a control group. Articles were excluded if they (i) were published before 2008 or written in a language other than English, (ii) primary investigators did not use portable or smartphone-based accelerometers to analyze gait, (iii) or iNPH was not included in the primary clinical focus.
Selection Process
Results of the literature search were imported to reference manager software (EndNote20). After removing duplicates, references were imported to the Rayyan web platform to proceed with the screening and the first selection. Titles and abstracts were independently screened by two reviewers (RD, EB). Any disagreements were blindly screened by a third reviewer (JA). The same process was repeated for full text review of the papers that past first selection.
Quality Assessment
Following the screening process, thirty-two articles that adhered to all inclusion criteria were assessed for quality and potential bias using the Joanna Briggs Institute (JBI) Critical Appraisal Tools. Each article was evaluated by using the appropriate JBI checklist and further classified as low risk of bias (>70%), moderate risk of bias (50-70%), or high risk of bias (<50%). After discussion amongst researchers, all thirty-two articles were deemed as low risk of bias (>70%) and included in this systematic review (Supplemental File 2).
Results
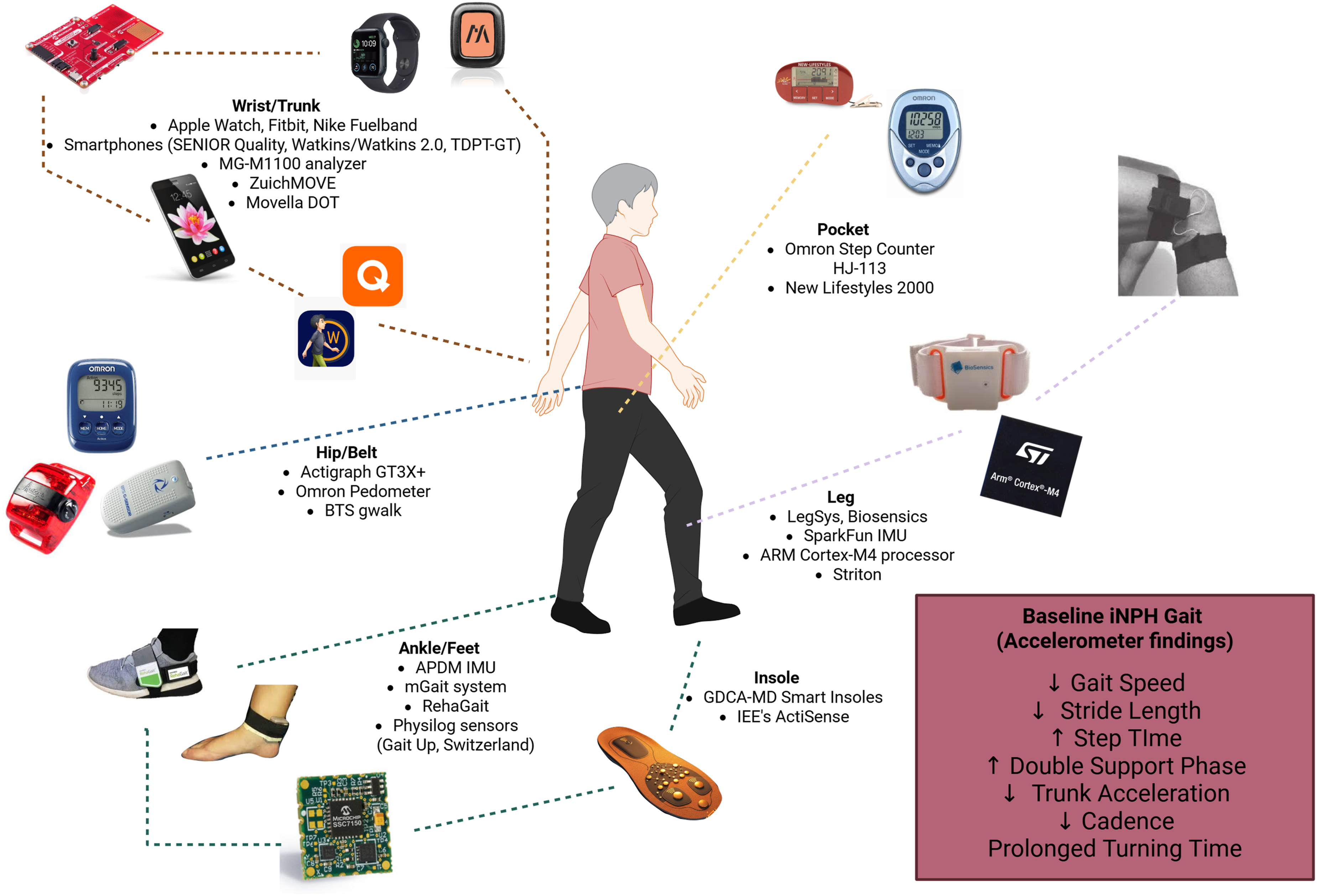
Using the search criteria, a total of 3894 articles were identified. After deduplication, a total of 660 were screened for abstract and title, of which 58 were chosen for full-text review. Following full-text review, 32 papers were selected to be included in the review (Figure 1). In total 22 different accelerometers were used across studies with findings in patients with iNPH ranging from decreased gait speed, increased step time, and decreased trunk acceleration (Figure 2). These studies were categorized into five groups based on their use of accelerometers for iNPH management: (1) diagnosing abnormal gait patterns in iNPH patients, (2) smartphone-based accelerometry, (3) prolonged gait monitoring in real-world environments, (4) prognostication of fall risk, and (5) prognostication of response to shunt placement. Prisma flow Chart. Portable and software-based accelerometers and findings in iNPH Fig 2. Line diagram created in BioRender by Martin R (https://www.biorender.com).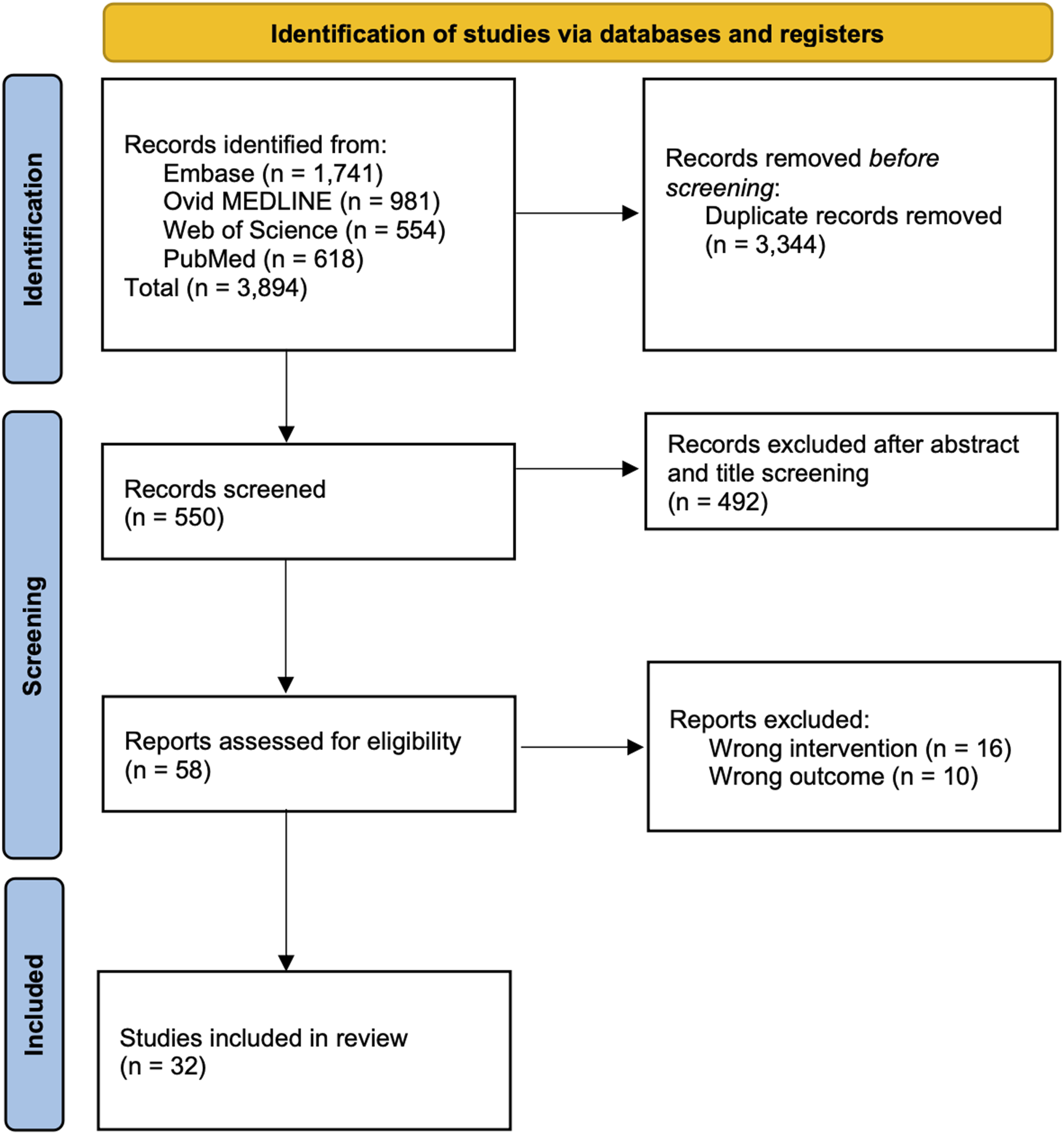
Using Accelerometers to Diagnose Abnormal Gait Patterns in iNPH Patients
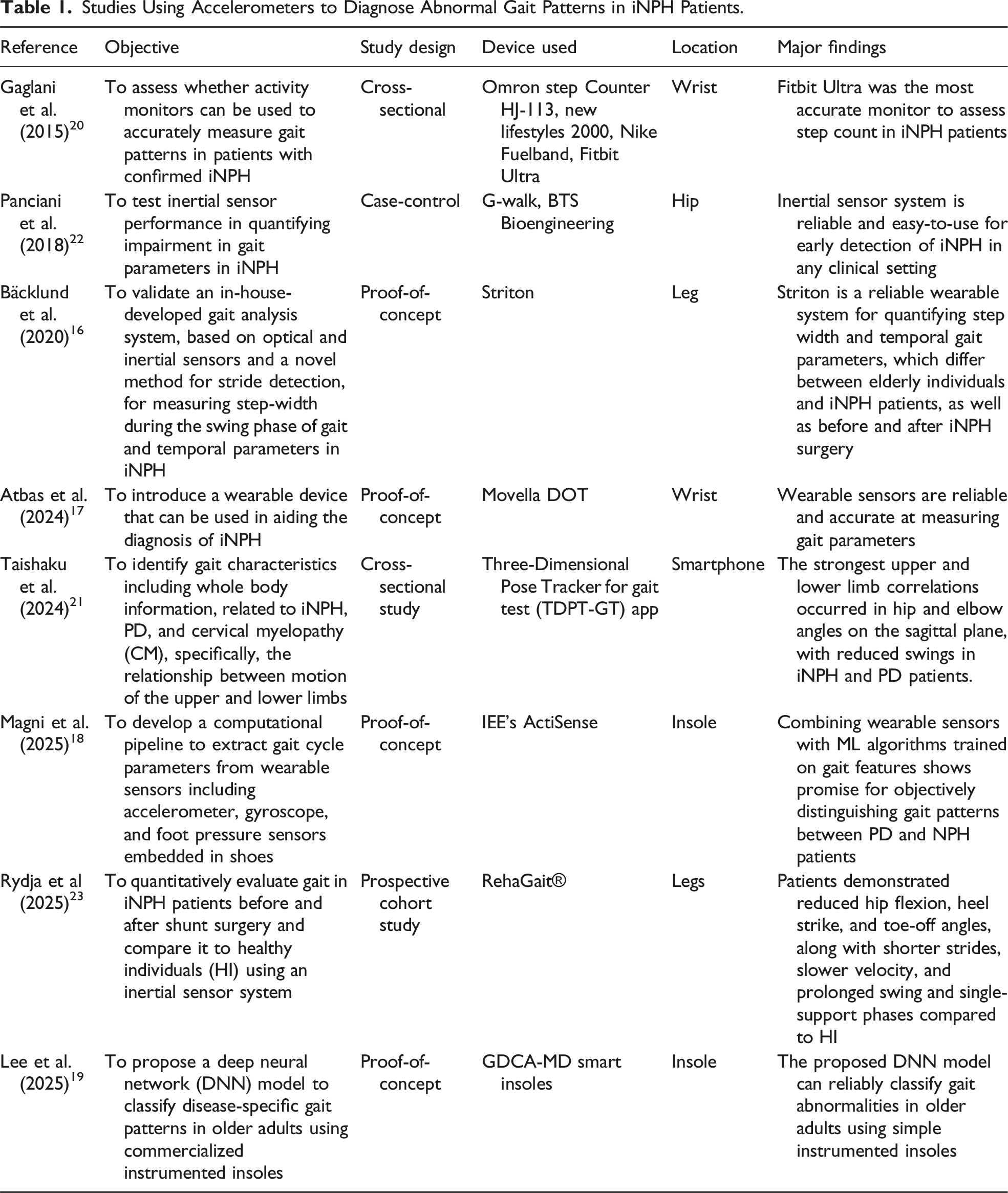
Studies Using Accelerometers to Diagnose Abnormal Gait Patterns in iNPH Patients.
Using Smartphone-Based Accelerometry as a Diagnostic Tool
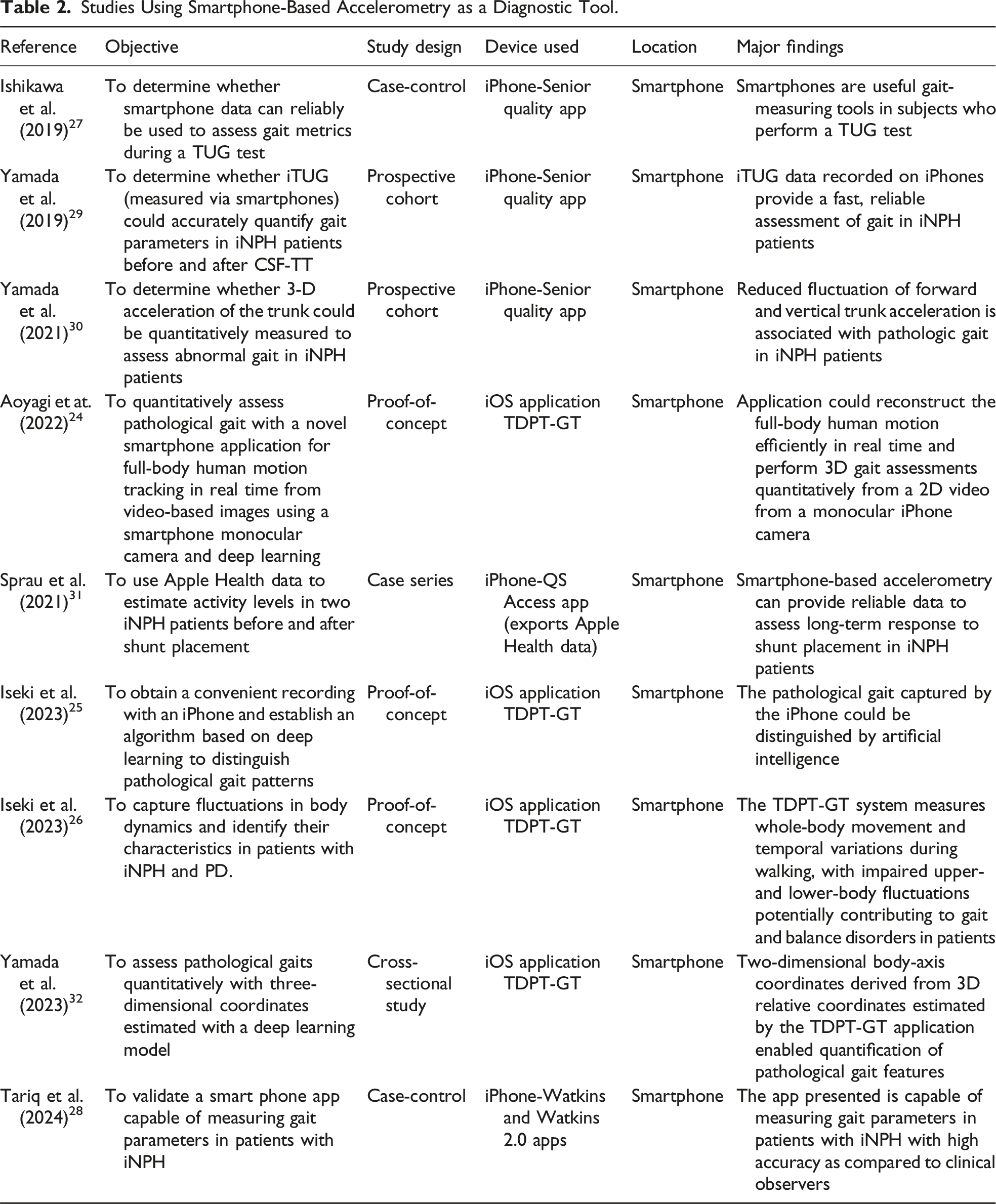
Studies Using Smartphone-Based Accelerometry as a Diagnostic Tool.
Prolonged Gait Monitoring in a Real-World Environment
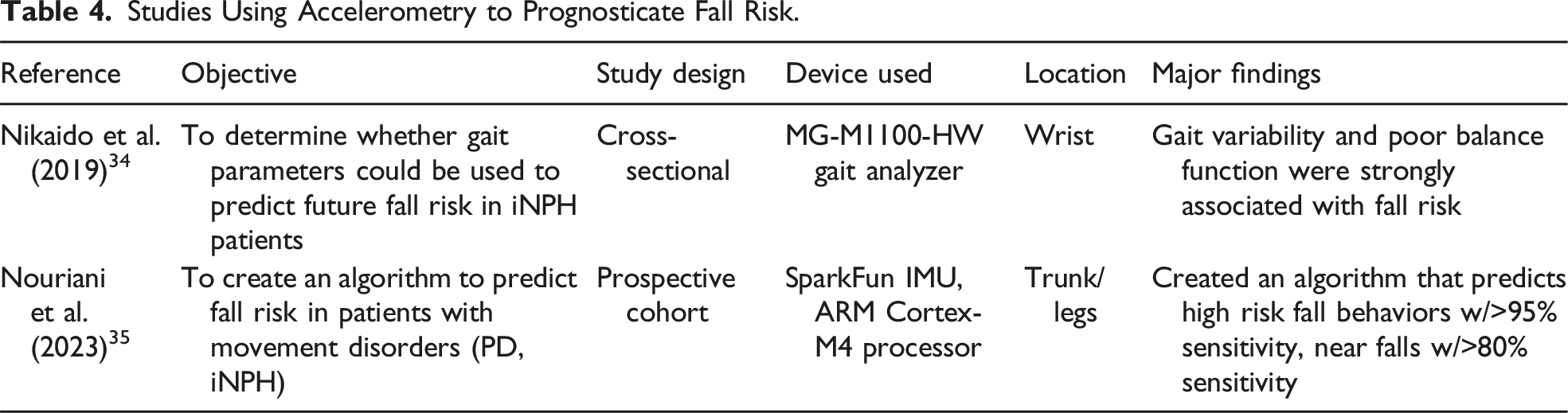
Using Accelerometry to Prognosticate Fall Risk
Studies Using Accelerometry to Prognosticate Fall Risk.
Using Accelerometry to Prognosticate Response to Shunt Placement
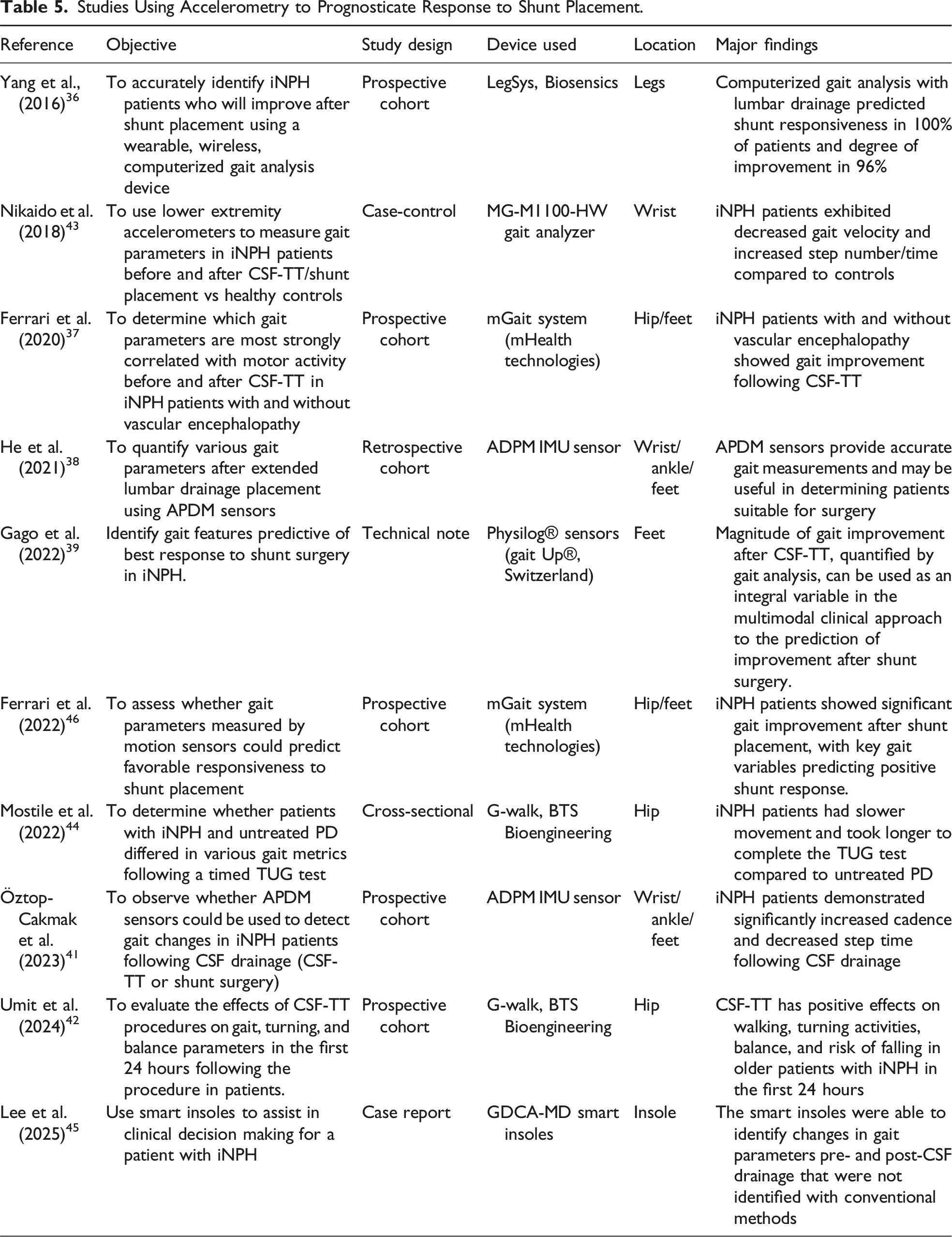
Studies Using Accelerometry to Prognosticate Response to Shunt Placement.
Discussion
The purpose of this review was to identify the various means by which portable accelerometers can be used to quantitatively assess gait in iNPH patients. Characterized by broad-based walking, decreased speed, step-length variability, hesitancy, and postural instability, gait is usually the first symptom that patients with iNPH present. Assessing gait in these patients is important not only for differential diagnosis, but also for determining shunt placement eligibility, establishing a baseline for monitoring, and facilitating long-term follow-up of symptom progression. In the past, gait could only be assessed subjectively in a clinical setting, but with the advent of accelerometry, gait can now be objectively and quantitatively measured. However, it was not until the early 2010s that portable accelerometers began to be used in clinical research to diagnose iNPH by measuring gait parameters such as speed, stride length, and turning speed.22,47 Due to their ubiquity, portability, and ability to measure multiple parameters simultaneously, accelerometers provide a quick and accessible means to evaluate gait in iNPH patients. In addition, they overcome the limitations of poor inter-rater reliability through objective assessment.
This review identified 32 studies that used a variety of portable accelerometers to quantify gait parameters in patients with iNPH. In total, 22 different accelerometers were used across studies, ranging from wearable wristbands to smartphone-based applications. Among the smartphone applications, the TDPT-GT App was the most widely used, implemented in five studies.21,24-26,48 This application uses a smartphone camera to capture motion by generating 30 Hz coordinates for 27 body points, which are then analyzed for iNPH gait features such as shuffling, short steps, and wide-based walking patterns. 26 Among the wearable accelerometers, the G-Walk device from BTS Bioengineering was the most commonly used, reported in three studies22,42,44 Unlike software-based accelerometers, the G-Walk device is an inertial sensor capable of recording 3D accelerometric and gyroscopic data, most often used before and after diagnostic interventions such as the CSF-TT. 49 However, recent quantitative gait-analysis studies suggest that gait improvement following CSF-TT may not manifest within the first hours as traditionally assumed, but can emerge gradually over a 48-72-hour window. In this context, wearable accelerometry offers an opportunity for more ecologically valid, real-world monitoring that can capture delayed or progressive gait responses that may be missed during brief in-clinic assessments.37,50 This suggests that software-based accelerometers could be implemented more regularly in real-life scenarios, where patients do not necessarily need to be in a clinical setting. In contrast, wearable accelerometers with inertial sensor technology may be better suited for clinical environments, where the use of a device other than a smartphone is required and where a greater technological learning curve may be involved.
More specific uses of portable accelerometers in iNPH were mentioned by Sprau et al. (2021), who stated that remote monitoring of patients allows for the capture of unbiased data for the detection of improvements or setbacks. This is particularly relevant for patients following shunt surgery, where clinical gait improvement can typically be maintained for about 5-7 years. 51 Activity monitoring data could be used in these instances to detect changes from a post-shunt baseline to the early stages of symptom recurrence, thus allowing physicians to intervene earlier through revision surgeries and potentially prevent disease regression. Remote monitoring also enables physicians to track patient symptoms without requiring in-person follow-up when gait metrics remain stable. 31
Currently, portable accelerometers are more widely used in other diseases that affect gait, such as Parkinson’s disease (PD) and stroke. Five studies included in this review used accelerometers to compare iNPH symptoms with those of PD and other gait disorders, as well as to train accelerometer algorithms for diagnosis.18,21,26,35,44 Magni et al. combined wearable accelerometers with a machine learning (ML) algorithm to differentiate between PD and iNPH. This also reflects the increasing number of studies investigating the ability of machine and deep learning models to diagnose various neurological conditions that affect gait.52-54 For example, Iseki et al. developed a deep learning model capable of detecting iNPH using only an iPhone camera. 25 The rapid advancement of such technologies has the potential to make diagnosis of these conditions more accurate and precise from the earliest signs of symptoms.
Nevertheless, a possible limitation of portable and software-based accelerometers is the learning curve and comfort associated with wearable sensors, particularly in older patients who represent the primary population affected by iNPH. Furthermore, because one of the hallmark symptoms of iNPH is dementia, many patients may struggle to independently set up or use software and wearable accelerometers. As a result, independent use of these technologies may only be feasible during periods of symptom resolution, or they may instead need to be implemented as preventive strategies with caregiver or clinician assistance.
Limitations
The current body of evidence is limited by the significant heterogeneity across studies. This includes variability in accelerometer models, study populations, and the specific gait parameters measured by each study. This heterogeneity not only makes direct comparison challenging but prevents a formal meta-analysis from being conducted. Establishing a core set of gait parameters, such as gait velocity, stride length, cadence, variability, and symmetry, that should be consistently reported would further facilitate meaningful cross-study synthesis. Adopting a replicable assessment protocol, including standardized walk distance, pace instructions, sensor placement, and recording duration, would help reduce methodological heterogeneity. Incorporating these elements into future studies would substantially strengthen the evidence base and support more reliable clinical integration of accelerometer-derived gait metrics in iNPH. Additionally, most studies also had a relatively small sample size and short follow-up periods, which limit the generalizability of findings. Another limitation is the lack of standardized protocols for data collection and analysis, which introduces bias and reduces reproducibility. Future studies should focus on standardizing their outcome by identifying and measuring specific gait parameters. Larger, multicenter trials with longer follow-up would also strengthen the body of literature.
Conclusion
This review identified 32 studies utilizing 22 different portable accelerometers to quantify gait parameters in patients with iNPH, ranging from wearable wristbands to smartphone-based applications. These devices provide objective and reproducible measures of gait, overcoming the limitations of subjective clinical assessments and poor inter-rater reliability. Remote monitoring with accelerometers not only facilitates early detection of symptom progression following shunt surgery but also reduces the burden of in-person follow-up. Furthermore, accelerometer-based assessments are increasingly being integrated with machine learning and deep learning models, which have shown promise in differentiating iNPH from other movement disorders such as Parkinson’s disease. While these technologies represent a significant advance, further studies must be conducted to standardize the outcomes obtained by these devices and applications to make a diagnosis. Overall, portable accelerometers and smartphone-based applications can represent a practical and accessible tool for the diagnosis, monitoring, and long-term management of iNPH.
Supplemental Material
Supplemental Material - Emerging Role of Portable Accelerometers for Assessment of Gait Instability in Idiopathic Normal Pressure Hydrocephalus: A Systematic Review
Supplemental Material for Emerging Role of Portable Accelerometers for Assessment of Gait Instability in Idiopathic Normal Pressure Hydrocephalus: A Systematic Review by Ryan J. Davis, MS, Emanuella M. Brito, Julia Armstrong, Roberto Martin, Jehan Bista, Bryan A. Lieber, Regina M. Graham in Journal of Geriatric Psychiatry and Neurology
Supplemental Material
Supplemental Material - Emerging Role of Portable Accelerometers for Assessment of Gait Instability in Idiopathic Normal Pressure Hydrocephalus: A Systematic Review
Supplemental Material for Emerging Role of Portable Accelerometers for Assessment of Gait Instability in Idiopathic Normal Pressure Hydrocephalus: A Systematic Review by Ryan J. Davis, MS, Emanuella M. Brito, Julia Armstrong, Roberto Martin, Jehan Bista, Bryan A. Lieber, Regina M. Graham in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
The study was conceptualized and supervised by Bryan Lieber. Data acquisition and initial writing were done by Emanuella Brito, Ryan Davis, Julia Armstrong, and Roberto Martin. Review and revision were done by Jehan Bista, Regina M. Graham. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by HCA Florida University Hospital for RMG.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.