
Abstract
Background
Advances in biomarker research allow precise diagnosis of Alzheimer’s disease (AD) in patients with Mild Cognitive Impairment (MCI). Communicating this diagnosis may reduce uncertainty and aid care planning but can also increase anxiety, distress, or anticipatory burden among care partners.
Objective
To characterise coping strategies used by caregivers of patients recently diagnosed with MCI due to AD and examine their evolution.
Methods
Thirty caregivers of patients with MCI due to AD were recruited from a memory clinic, assessed at baseline, and followed over 18 months. Caregiver personality, burden, depressive and anxiety symptoms, perceived relationship closeness, and distress related to patient neuropsychiatric symptoms were also assessed at baseline. Coping was assessed longitudinally using the Brief COPE, grouping its 14 subscales into problem-focused, emotion-focused, and dysfunctional coping.
Results
Caregivers used problem-focused (3.37 ± 1.02) and emotion-focused (2.91 ± 0.86) more often than dysfunctional coping (1.13 ± 0.56). Dysfunctional coping was associated with lower perceived relationship closeness, higher burden, and greater distress related to neuropsychiatric symptoms, while emotion-focused coping was inversely associated with anxiety and depression. Trends suggested associations between emotion-focused coping and extraversion, and between problem-focused coping and conscientiousness. Coping patterns remained stable over time. Caregivers reported elevated psychological distress.
Conclusion
Caregivers of patients with MCI due to AD experience considerable psychological distress but appear to rely primarily on adaptive coping strategies. The stability of coping patterns suggests that coping responses may begin to consolidate early in the caregiving trajectory. Given the exploratory nature of our study, further longitudinal research is needed.
Introduction
With global population ageing, the number of individuals living with Alzheimer’s disease (AD) and other forms of dementia is rising sharply, posing a significant public health challenge. 1 Dementia is now among the leading causes of disability and dependence amongst older adults, placing a substantial burden on families and societies, with informal caregivers providing most of the care and support. 2
Caregiving can be emotionally, physically, and financially demanding, often resulting in increased caregiver burden and higher levels of anxiety and depressive symptoms.3,4 Coping is the process by which individuals respond to stress related to caring for someone, 5 and it has emerged as a central factor in understanding the psychological outcomes of dementia caregivers.
There is substantial heterogeneity in how coping is conceptualized and operationalized in the dementia caregiving literature. The traditional framework by Lazarus and Folkman 5 distinguishes between problem-focused coping, which involves efforts to directly manage or resolve stressors (eg, planning, seeking instrumental support), and emotion-focused coping, which aims to regulate the emotional response to stress (eg, acceptance, positive reframing, finding comfort in spirituality). This model was later expanded to include dysfunctional coping, encompassing behaviours such as avoidance, denial, disengagement, wishful thinking, and self-blame, which may provide short-term relief but ultimately exacerbate distress over time.6,7 Although Lazarus and Folkman’s original model distinguished primarily between problem-focused and emotion-focused coping, contemporary dementia caregiving research frequently operationalizes coping strategies into adaptive (problem-focused and some emotion-focused strategies) and dysfunctional domains, an approach adopted in the present study.
This tripartite model reflects general or dispositional coping styles, that is, habitual ways of managing overall stress related to caregiving. In contrast, situational coping approaches focus on how caregivers respond to specific stressors or care-related events such as the behavioural and psychological symptoms of dementia (BPSD) which may fluctuate across time and contexts. 8 These distinctions are important because caregivers may report generally adaptive coping styles on global measures yet still struggle to manage discrete, high-intensity caregiving episodes effectively.
Coping in dementia caregivers has been studied through a range of assessment tools, reflecting the aforementioned heterogeneity in coping conceptualization across studies. The Brief COPE, 9 a 28-item questionnaire designed to measure ways in which individuals cope with stressful life events including health-related problems, has been widely used to assess general coping amongst dementia caregivers 10 and has demonstrated good internal consistency when its subscales are grouped into emotion-focused, problem-focused, and dysfunctional coping strategies. 11 Based on assessments with global coping measures, caregivers of individuals with dementia typically use a combination of coping strategies rather than relying on a single approach. They tend to report employing problem-focused and emotion-focused coping strategies more often than dysfunctional coping.7,12
Notably, the type of coping strategies employed by caregivers influences their psychological outcomes. Studies suggest that caregiver psychological factors, particularly coping processes, are important predictors of caregiver distress and burden, beyond objective disease-related variables such as cognitive impairment. 13 Recent evidence, including systematic review data, suggests that problem-focused coping is generally associated with lower caregiver burden and better psychological adjustment, whereas dysfunctional coping is linked to higher levels of anxiety, depressive symptoms, and burden.14-16 Emotion-focused coping may be beneficial in some situations, although its association with caregiver outcomes appears less consistent than that of problem-focused or dysfunctional strategies. 17
The way caregivers manage stress can have measurable effects not only on their own psychological health but also on the functional and behavioural trajectories of the individuals with dementia they care for. Longitudinal evidence from the Cache County Dementia Progression Study demonstrated that care recipients whose caregivers used more problem-focused and fewer avoidant coping strategies exhibited significantly slower rates of cognitive and functional decline over a 5-year period, even after adjusting for demographic and clinical covariates. 13 Intervention studies also indicate that programmes designed to enhance adaptive coping in caregivers can delay the institutionalization of the person with dementia. 18
Among the most challenging aspects of caregiving are BPSD. In their review of stress and resilience in dementia caregiving, de Vugt & van der Flier 19 concluded that caregivers who engage in adaptive coping strategies – such as seeking support, acceptance, and positive reappraisal – tend to foster more stable and emotionally supportive care environments, which may, in turn, help reduce the expression of BPSD and support maintenance of daily functioning in the person with dementia. Consistent with this, interventions that train caregivers in understanding and managing BPSD, through psychoeducation and problem-solving approaches, have been shown to reduce both caregiver stress and the frequency or severity of disruptive behaviours in care recipients. 20
Coping is not only shaped by situational stress but also by individual caregiver characteristics. Research grounded in the Five-Factor Model of personality 21 indicates that dementia caregivers high in neuroticism are more likely to use dysfunctional or emotion-focused coping, whereas those high in conscientiousness and extraversion tend to adopt more adaptive, problem-solving strategies. 22 Theoretically, coping has even been conceptualized as personality in action under stress, 23 reflecting the view that enduring personality traits may shape stress responses. However, empirical findings on the relationship between personality traits and coping remain heterogeneous. Meta-analytic evidence suggests that associations between the Five-Factor Model traits and coping strategies are generally modest and vary depending on contextual factors such as the type of stressor, the coping measures used, and characteristics of the study population. 24
Regarding the evolution of caregiver coping strategies over time, longitudinal research suggests that caregiver coping strategies tend to remain relatively stable over time in the context of ongoing care-recipient cognitive decline.11,25 However, certain caregiver subgroups may show shifts in coping over time. For example, adult-child caregivers may exhibit increasing use of avoidant (dysfunctional) coping as caregiving progresses. 25
While coping amongst dementia caregivers is relatively well-documented, it is unclear whether these patterns hold in the earlier stages of cognitive decline such as Mild Cognitive Impairment (MCI). MCI refers to a mild but noticeable decline in cognitive abilities, greater than expected in healthy ageing, but which does not yet qualify as dementia. 26 It is known that, despite the relative independence of individuals with MCI, the emotional toll on their caregivers is considerable.27,28 Caregivers of people with MCI report elevated levels of psychological distress, including anxiety, depression and burden, compared to non-caregivers. 29 In other words, the psychological impact begins early, even before advanced dementia. A key contributor to this stress is the diagnostic uncertainty that characterizes MCI. Caregivers must monitor subtle changes, provide intermittent support, and make long-term decisions without a clear prognosis. Many do not yet identify as caregivers, instead seeing themselves as family members in a transitional role. 30 McIlvane et al. 31 focused on caregivers of individuals with MCI and found that their beliefs about illness progression and controllability varied widely – some minimised the likelihood of progression to AD, while others endorsed health-promoting behaviours as a valid attempt to delay or prevent decline.
Using the Brief COPE, McIlvane et al. 31 found that caregivers of individuals with MCI predominantly employed problem-focused and emotion-focused coping strategies, with no significant difference in frequency between the two. Dysfunctional coping strategies were minimally used. This pattern appears broadly similar to that reported among dementia caregivers,15,32 although caregivers of individuals with MCI may show lower overall coping engagement due to reduced caregiving demands in this earlier stage of cognitive decline. However, it remains unclear whether coping strategies evolve as caregiving demands increase and which caregiver characteristics influence coping. Clarifying these patterns and trajectories is crucial for developing interventions that support caregiver well-being and maintain stable caregiving environments.
It is important to acknowledge that MCI is a syndromic diagnosis encompassing multiple possible aetiologies. 33 Diagnostic uncertainty may contribute to caregiver distress by limiting the sense of predictability and control over the disease trajectory.34,35 In situations where stressors are perceived as ambiguous or uncontrollable, caregivers may be more likely to resort to avoidant or disengagement-based coping strategies.36,37 Recent advances in biomarker based diagnostic precision, particularly the ability to identify MCI due to AD, 38 represent an important advance in MCI caregiver research. Establishing an etiological diagnosis of AD may reduce uncertainty about the cause and likely trajectory of cognitive decline, but it can also heighten awareness of the inevitable progression toward dementia. Thus, receiving a diagnosis of MCI due to AD may fundamentally shape how caregivers appraise their role and anticipate future challenges, with significant implications for their coping strategies and psychological well-being.
This study aimed to (1) describe the coping strategies used by caregivers of patients diagnosed with MCI due to AD; (2) ascertain caregiver characteristics, namely personality traits, that might influence the coping strategies; and (3) determine whether these coping strategies change over time.
Methods
Thirty dyads of community-dwelling patients and informal caregivers were consecutively recruited from a single memory outpatient clinic between March 2018 and June 2020. Recruitment occurred after the patient received a diagnosis of MCI due to AD – high likelihood. 38 The diagnosis of AD at an early stage was clearly communicated by the neurologist at a clinical consultation to both the patient and the informal caregiver.
Informal caregivers were aged 18 or above and had a significant personal relationship with the patient (ie, spouses, adult children or friends), lived with the patient or were frequently a part of their day-to-day and did not receive monetary compensation for assisting the patient. The decision to include significant people as participants intended to capture the diversity of support roles, to avoid excluding companions who provide care even if they do not recognize themselves as caregivers. Significant others who accompany the person with MCI were classified as caregivers, even though they might not view themselves as fulfilling a caregiving role.
Caregivers aged 65 years or older underwent the Mini Mental State Examination (MMSE)39,40 to rule out major cognitive disorders.
The study was carried out in accordance with the Declaration of Helsinki and approved by the local ethics committee. Written informed consent was obtained from all participants.
Baseline Assessment
The first caregiver assessment was carried out within 3 months of diagnosis communication. Information was gathered on caregiver and patient demographics, namely age, gender, educational level, caregiver employment and living status, the nature of the relationship with the patient, and patient MMSE scores.
Coping
Caregiver coping strategies were assessed using the Portuguese version of the Brief COPE inventory. 9 The Portuguese Brief COPE was adapted and validated by Pais Ribeiro and Rodrigues. 41 This version retains the original structure of 14 two-item subscales (28 items) scored on a 4-point Likert scale. Because each dimension comprises only two items, internal consistency is typically evaluated at the subscale level rather than as a total score. Reported Cronbach’s alpha coefficients for the Portuguese version are acceptable for brief two-item scales, ranging approximately from 0.55 (acceptance) to 0.84 (emotional expression), indicating adequate reliability for research purposes. In addition, the instrument is designed to produce a coping profile rather than a global index, which is consistent with its theoretical framework. Regarding sensitivity, the Portuguese Brief COPE has been shown to discriminate between different coping patterns across clinical and non-clinical contexts, supporting its usefulness for detecting variations in coping responses to stressors.
This questionnaire includes 28 items and asks caregivers to rate, on a four-point Likert scale from 0 (“I haven’t been doing this at all”) to 3 (“I’ve been doing this a lot”), how frequently they have used various coping strategies in the past month to manage stressful events related to the patient’s health. The 28 items form 14 subscales, with two items per subscale.
For analysis, the 14 sub-scales were grouped into three broader categories of coping strategies: problem-focused (active coping, planning and seeking instrumental support), emotion-focused, (seeking emotional support, acceptance, positive reframing, religion and humor) and dysfunctional coping (self-distraction, denial, substance use, behavioural disengagement, venting and self-blame).
Because each coping category contained a different number of items, a weighted mean score was calculated for each category to enable direct comparisons. As demonstrated in previous studies, 10 these composite categories have showed good internal consistency, as well as convergent and concurrent validity, supporting their utility in clinical research.
Other Caregiver Measures
Caregiver personality was measured using the Portuguese version 42 of the NEO-Five Factor Inventory (NEO-FFI), 43 a 60-item questionnaire based on the Five Factor Model 22 which classifies universal personality traits across five dimensions – neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. Each question is scored on a 5-point Likert scale. The total scores for each personality dimension range from 0 to 48, with a higher score meaning a stronger presence of that personality trait.
Caregiver burden was assessed using the Portuguese version 44 of the Zarit Burden Interview (ZBI), 45 a 22-item self-report measure that evaluates caregivers’ perceptions of burden in relation to their physical, emotional, social, and financial well-being. Items are rated on a five-point Likert scale, with higher scores indicating greater burden. Following the criteria established by Schreiner et al, 46 a total score ≥24 was considered indicative of a clinically significant burden.
Depressive symptoms in caregivers were assessed using the Portuguese version 47 of the Centre for Epidemiological Studies–Depression Scale (CES-D). 48 This 20-item self-report measure asks caregivers to indicate how frequently they experienced various symptoms of depression during the past week. Responses are rated on a 4-point Likert scale, with higher total scores reflecting greater levels of depressive symptoms, and the maximum possible score is 60. The commonly used clinical cut-off score is 16. 48
Symptoms related to caregiver anxiety were assessed using the State Anxiety Subscale from the Portuguese version 49 of the State–Trait Anxiety Inventory (STAI). 50 This subscale includes 20 items, each rated on a 4-point Likert scale. Higher total scores reflect more severe anxiety symptoms, with a maximum possible score of 80. Although no universally established clinical cut-off exists for the STAI, a score ≥40 was used for descriptive purposes, as this threshold is commonly applied in screening contexts to indicate elevated anxiety symptoms. 51
Caregivers’ perceptions of behavioural and personality changes in patients were assessed using the Portuguese version 52 of the Neuropsychiatric Inventory (NPI). 53 The tool includes screening questions for 12 neuropsychiatric domains: delusions, hallucinations, agitation/aggression, depression, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor behaviour, nighttime disturbances, and appetite/eating changes. After endorsing a symptom in each domain, the caregiver is asked to rate its frequency (on a 4-point Likert scale) and severity (on a 3-point Likert scale). The score for each domain was calculated by multiplying frequency by severity, and a total score (ranging from 0 to 144) was obtained by summing across all domains, with higher scores indicating more severe neuropsychiatric symptoms. Additionally, caregiver distress related to each behavioural symptom was assessed using the NPI Distress Scale. Caregivers rate how distressing each symptom is for them on a scale from 0 (“not at all distressing”) to 5 (“extremely distressing”). Total scores, ranging from 0 to 60, were interpreted dimensionally, with higher scores reflecting greater caregiver distress related to behavioural symptoms.
Caregiver’s perception of the quality of the current caregiver–care recipient relationship was measured using the Relationship Closeness Scale (RCS).54,55 The RCS was developed specifically to capture caregiver–care recipient closeness and is comprised of six items, each rated on a four-point Likert scale. Total scores range from 6 to 24, calculated by summing responses across all items.
Follow-up Assessment
Caregiver coping strategies were reassessed using the Brief-COPE and relevant caregiver demographic information updated (age, employment status, living arrangements) at least 12 months after baseline assessment. Conversion to dementia was established according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision diagnostic criteria. 56
Statistical Analysis
Sample size was estimated a priori from a power analysis using the Power and Precision software (v.4; BioStat; Englewood, NJ). Assuming the baseline values for the dysfunctional coping score, emotion-focused coping score and problem-focused coping score previously reported, 11 recruitment of 25 participants would allow detection of a 20% difference between the baseline and follow-up evaluations, assuming common variance, a correlation between ratings = 0.75, P < .01 to account for Bonferroni correction, power >80%, and a 2-tailed test.
Statistical analyses were performed with IBM SPSS Statistics, version 30 [SPSS Inc, Chicago, IL]. Statistically significant differences were assumed for P < .05.
To compare the mean scores among the three coping categories (emotion-focused, problem-focused, and dysfunctional coping), a repeated measures ANOVA was conducted. Bonferroni-adjusted pairwise comparisons were used for post-hoc analyses. Bivariate Pearson correlations were carried out to examine the associations between coping categories and caregiver characteristics. After checking for normality, changes in coping categories over time were examined using paired-samples t-tests.
Results
Baseline Assessment
Characteristics of Family Caregivers and Patients at Baseline Assessment.
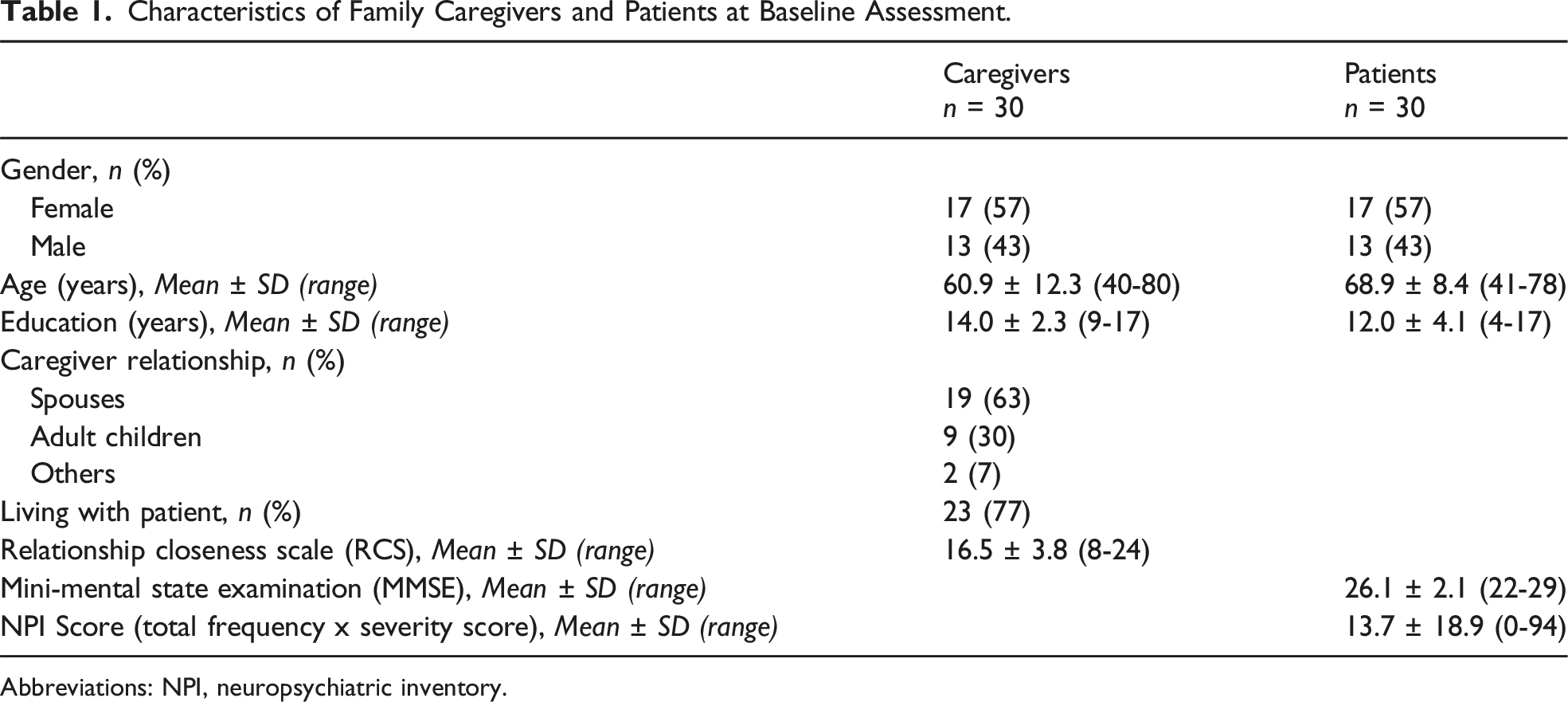
Abbreviations: NPI, neuropsychiatric inventory.
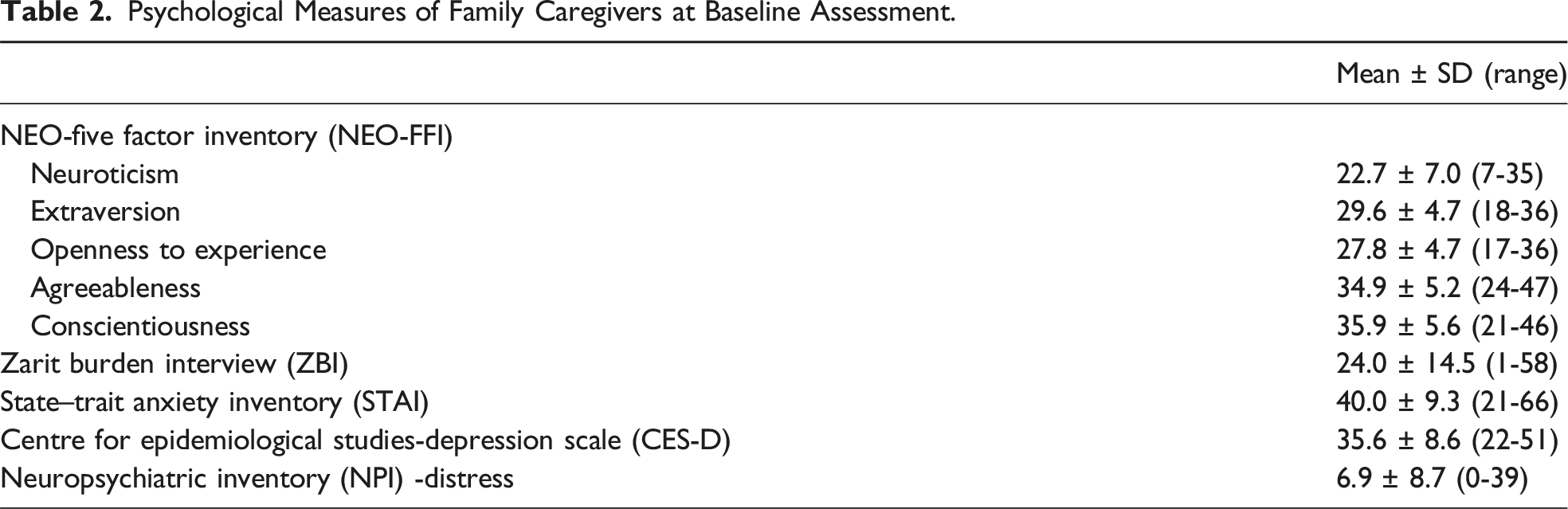
Psychological Measures of Family Caregivers
Psychological Measures of Family Caregivers at Baseline Assessment.
Coping Categories
Coping Categories Used by Family Caregivers at Baseline.
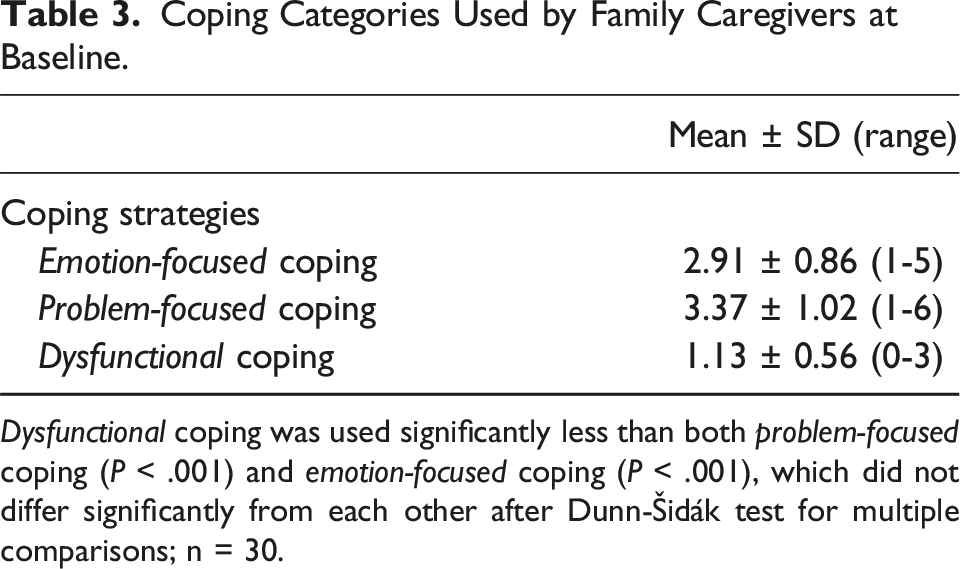
Dysfunctional coping was used significantly less than both problem-focused coping (P < .001) and emotion-focused coping (P < .001), which did not differ significantly from each other after Dunn-Šidák test for multiple comparisons; n = 30.
Coping Categories and Caregiver Characteristics
Correlations Between Coping Strategies and Caregiver Personality Traits at Baseline.
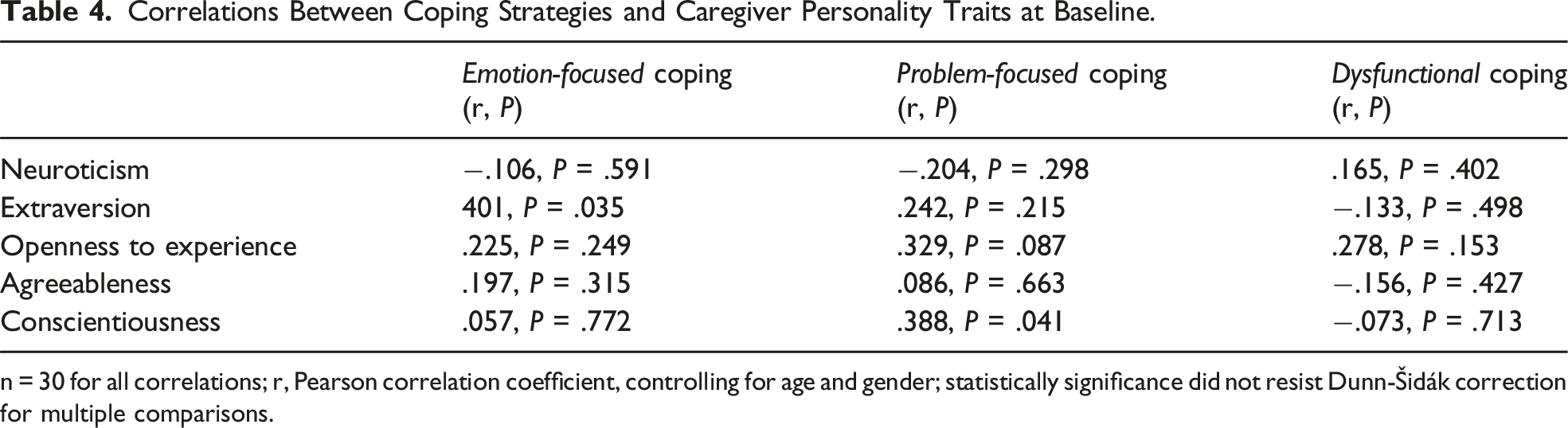
n = 30 for all correlations; r, Pearson correlation coefficient, controlling for age and gender; statistically significance did not resist Dunn-Šidák correction for multiple comparisons.
Correlations Between Coping Categories and Other Caregiver Psychological Measures at Baseline.
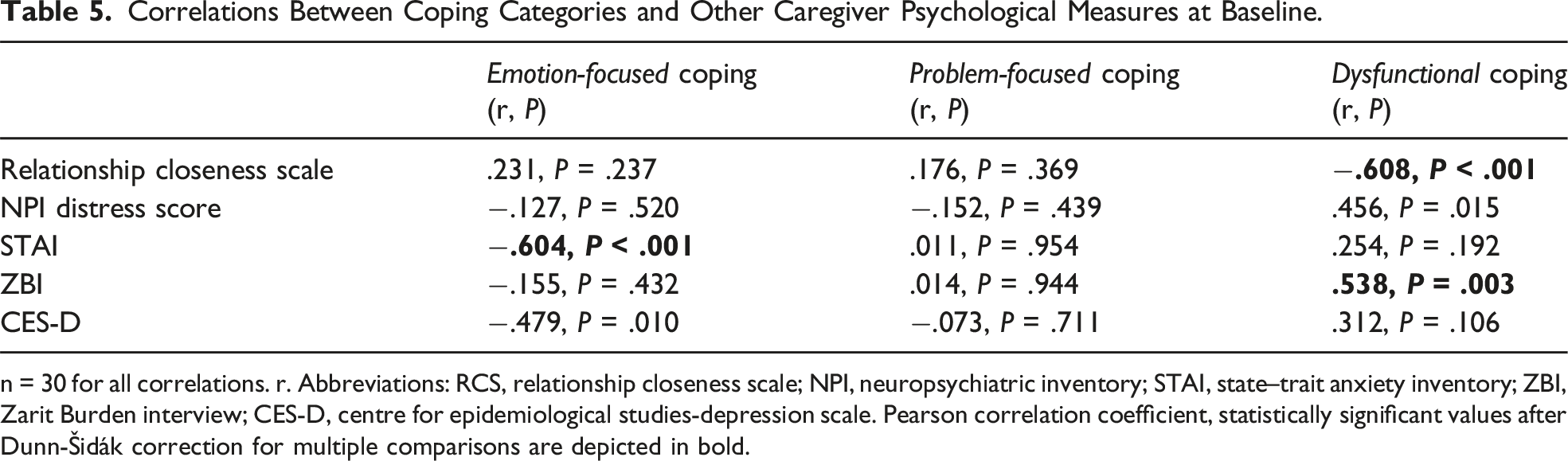
n = 30 for all correlations. r. Abbreviations: RCS, relationship closeness scale; NPI, neuropsychiatric inventory; STAI, state–trait anxiety inventory; ZBI, Zarit Burden interview; CES-D, centre for epidemiological studies-depression scale. Pearson correlation coefficient, statistically significant values after Dunn-Šidák correction for multiple comparisons are depicted in bold.
Follow-up
The mean follow-up time was 17.7 ± 9.4 months. Follow-up assessment was possible in 25/30 (83%) of the caregivers interviewed at the baseline assessment. Five caregivers were not re-assessed for the following reasons: moved to distant cities (2); were no longer available for re-evaluation (2) and withdrew consent (1). Except for age, where caregivers who did not complete the follow-up were significantly older than those who did (P < .05), no statistically significant differences were found in other caregiver demographic or psychological measures.
Three MCI patients converted to dementia over the course of the study. The caregiver coping strategies employed at baseline were not different in caregivers of patients who maintained the diagnosis of MCI as compared to those who progressed to dementia. In a sensitivity analysis, removing the caregivers of patients who converted to dementia did not modify the results of the study.
Evolution of Caregiver Brief COPE Strategies Over Time.
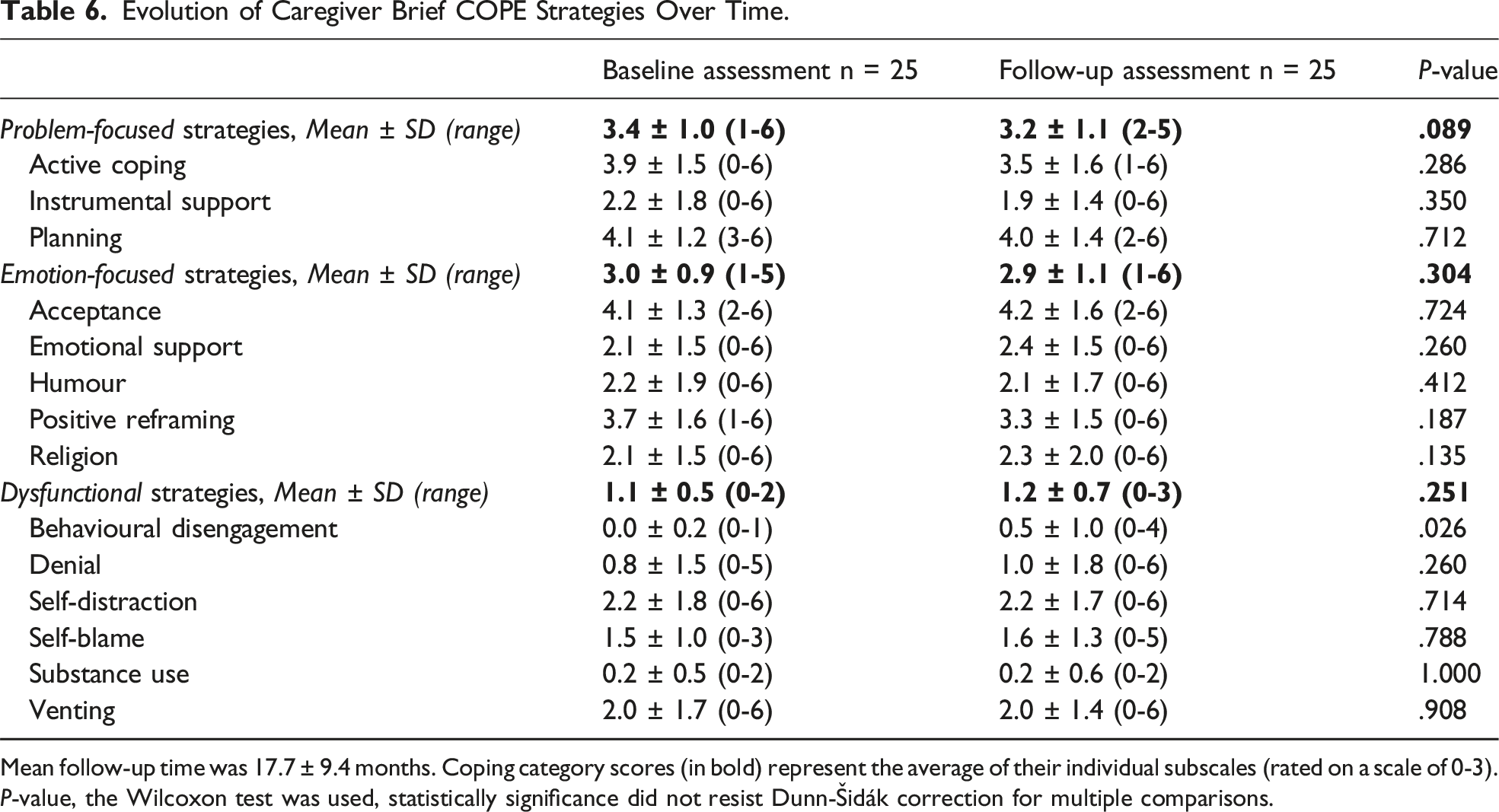
Mean follow-up time was 17.7 ± 9.4 months. Coping category scores (in bold) represent the average of their individual subscales (rated on a scale of 0-3). P-value, the Wilcoxon test was used, statistically significance did not resist Dunn-Šidák correction for multiple comparisons.
Discussion
This study aimed to describe the coping strategies employed by caregivers of patients recently diagnosed with MCI due to AD. Caregivers most frequently relied on problem-focused and emotion-focused coping, whereas dysfunctional coping was used significantly less often. Dysfunctional coping was associated with lower perceived relationship closeness, higher burden, and greater distress related to patients’ neuropsychiatric symptoms, while emotion-focused coping was inversely associated with anxiety and depressive symptoms. Regarding personality traits, trends for associations between emotion-focused coping and extraversion, as well as between problem-focused coping and conscientiousness were detected, and need confirmation in future studies. Coping patterns remained essentially stable over an average follow-up of 18 months.
Recent advances in biomarker-based diagnosis have enhanced diagnostic precision in identifying MCI due to AD. Although greater etiological clarity may reduce some uncertainty and aid in care planning, it can also heighten anticipatory distress and burden among care partners.58,59 A recent longitudinal study found that nearly half of caregivers of people with MCI due to AD reported clinically significant burden at baseline, which increased over time. 60 Together, these findings suggest that, even in MCI due to AD, the caregiving experience may already be psychologically taxing. In this context, examining coping responses following an early AD diagnosis is crucial for understanding adaptation at this early stage of the disease. Caregivers in the present study most frequently relied on problem-focused and emotion-focused strategies, with significantly lower use of dysfunctional coping. This pattern is consistent with findings from McIlvane et al. 31 – who studied caregivers of individuals with a general MCI diagnosis – and aligns with broader dementia caregiving literature, which shows greater reliance on problem-focused and emotion-focused coping compared to dysfunctional strategies.7,12 Within Lazarus and Folkman’s coping framework, 5 this suggests that caregivers at the prodromal stage primarily engage in coping efforts aimed at managing stressors directly or regulating emotional responses, rather than resorting to avoidant or disengaged strategies. The continuity of this pattern across disease stages suggests that adaptive coping processes may be mobilized early in the caregiving trajectory, even before substantial functional dependence develops.
Although caregiving demands in MCI are typically less intensive than in established dementia, existing evidence suggests that psychological distress is already evident at this stage.27,60 In the present study, caregivers reported elevated levels of anxiety and depression and nearly half scored above the established clinical threshold for burden. These findings suggest that the predominance of adaptive coping does not necessarily imply the absence of distress. Caregivers may be employing adaptive coping strategies while simultaneously experiencing significant emotional distress namely linked to anticipatory concerns regarding the timing and trajectory of cognitive decline, even though participants had received a biomarker-supported diagnosis of MCI due to AD.
Elevated distress in the absence of entrenched maladaptive coping may represent a critical window for early intervention. Evidence from psychosocial intervention research suggests that caregivers who already rely heavily on dysfunctional coping may respond less effectively to stress management interventions. 61 In contrast, caregivers at the MCI stage, like those in our sample, may be receptive to early, preventative support aimed at strengthening strategies that help regulate distress before it becomes chronic. Clinically, these findings highlight the importance of identifying caregivers experiencing significant distress even in the absence of overt coping dysfunction, and of providing tailored interventions to buffer anticipatory stress and promote long-term psychological well-being.
Regarding the relationship between coping strategies and caregiver personality, moderate correlations were observed between emotion-focused coping and extraversion, as well as between problem-focused coping and conscientiousness, although they did not remain statistically significant after Dunn–Šidák correction. The direction of these correlations is nonetheless consistent with theoretical expectations derived from the Five-Factor Model, 21 which links extraversion with greater use of social and emotional support and conscientiousness with more structured, problem-solving approaches to stress. 62 These trends suggest that personality dispositions influence coping tendencies in caregivers at an early stage of AD, although the modest sample size may have limited the statistical power to confirm these relationships reliably. Research with dementia caregivers has also shown that caregivers’ personality traits were associated with the coping strategies, namely more extraverted caregivers were less likely to use confronting approaches. 63
A range of contextual and psychosocial factors may contribute to how caregivers cope with the challenges of MCI due to AD. In the present study, emotion-focused coping was negatively correlated with symptoms of anxiety as well as depression (this did not resist statistical correction for multiple comparisons). Emotion-focused coping strategies such as acceptance, positive reframing, and seeking emotional support, aim to regulate the emotional response to stress rather than directly alter the stressor itself. 5 In situations where stressors are chronic and largely uncontrollable, such as progressive neurodegenerative conditions, these strategies may help reduce the perceived impact of caregiving-related stress and lower symptoms of anxiety and depression. Although caregivers who reported greater use of emotion-focused coping tended to report fewer anxiety symptoms relative to others, the sample as a whole still displayed elevated anxiety levels. Dysfunctional coping was associated with higher burden as well as distress related to patients’ neuropsychiatric symptoms (this did not resist statistical correction for multiple comparisons). These findings are noteworthy, as previous research with dementia caregivers has shown that dysfunctional coping strategies not only correlate with higher burden but also mediate the relationship between caregiving stressors and psychological morbidity. 7 Characterized by avoidance, denial, or self-blame, dysfunctional coping strategies may provide temporary emotional relief but are generally considered maladaptive because they do not address the underlying sources of stress and may therefore contribute to the accumulation of caregiver strain over time. The observed association between distress related BPSDs and dysfunctional coping is also consistent with evidence that BPSDs represent some of the most challenging and emotionally taxing aspects of caregiving, often eliciting avoidant or self-blaming responses in caregivers.64,65 Dysfunctional coping was significantly less employed by caregivers who perceived their relationship with the care recipient as being closer. In dementia caregiving research, higher relationship quality is consistently linked to greater use of adaptive coping and lower reliance on dysfunctional strategies, 66 likely because a close relationship fosters empathy, motivation, and mutual emotional support, buffering against stress. Conversely, caregivers who perceive their relationship as weaker or more strained are more prone to engage in avoidance, denial, or self-blame, which amplifies emotional burden and psychological distress. 66 The present findings extend this literature by suggesting that even at the prodromal stage of AD, differences in perceived relationship closeness are already linked to coping tendencies.
Our findings showed that emotion-focused, problem-focused and dysfunctional coping remained stable over an average follow-up of 18 months, indicating relative consistency in how caregivers respond to the challenges of MCI due to AD. This aligns with longitudinal studies in dementia caregiving showing that the overall pattern of preferred coping styles tends to remain stable over time, even though the frequency of coping responses may increase as caregiving demands intensify in the long term.11,25 This relative stability may partly reflect the tendency of instruments such as the Brief COPE to capture general coping dispositions rather than highly dynamic, situation-specific responses 67 ). It should be noted that, among all coping strategies, only behavioural disengagement showed a modest increase during follow-up; however, this change did not remain statistically significant after correction for multiple comparisons. Despite this, the trend is noteworthy and merits further investigation, as behavioural disengagement reflects a tendency to withdraw effort from dealing with stressors and may represent an early indicator of emotional fatigue or adjustment difficulties as caregivers confront the progressive nature of the disease.15,67
Limitations
Limitations of this study include a small sample size which might have restricted the robust statistical confirmation of detected associations, especially in the analyses of personality and coping. The sample was drawn from a single memory clinic, possibly with a specific socioeconomic and cultural profile, and most caregivers in the sample are spouses, reducing representativeness and generalizability. Another limitation is that the follow-up period did not fully capture the trajectory of patients with MCI due to AD, who are expected to convert to dementia eventually. Additionally, although validated and widely used in caregiver research, the Brief COPE primarily assesses dispositional coping, which may not fully capture the situational nuances of coping in early-stage caregiving and limits the interpretation of coping “stability” over time. Finally, we assume that including other clinical and psychological variables longitudinally would have been an opportunity to gather a more comprehensive perspective of the evolving role of caregivers of patients diagnosed with MCI due to AD, in this sense the present study has an exploratory character.
Despite these limitations, the study provides valuable insights into coping processes in a relatively understudied population – caregivers of individuals with MCI due to AD. The design combined a validated coping instrument with a comprehensive assessment of caregiver psychological characteristics, personality, and relationship quality, providing a nuanced understanding of the early caregiving experience.
Conclusion
Caregivers of individuals with MCI due to AD predominantly use adaptive problem-focused and emotion-focused coping strategies, with dysfunctional coping being less frequent – a pattern similar to caregivers of individuals with general MCI. In this study, dysfunctional coping, although moderately used, was associated with higher burden, greater distress related to patients’ neuropsychiatric symptoms, and lower perceived relationship closeness, while personality traits appeared to have less influence on coping at this early stage. Coping patterns remained essentially stable over the follow-up period.
Understanding the coping strategies when patients and caregivers receive a definite diagnosis of AD at an initial stage of the disease may open opportunities to promote adaptive coping strategies, and eventually to anticipate and manage caregiver distress as the disease progresses. Future studies should employ larger, more diverse samples, incorporate both dispositional and situational coping measures, longitudinally track multiple psychological outcomes, include direct patient assessments over time, and extend follow-up periods to track changes as care demands increase.
Footnotes
Acknowledgements
The authors thank the participants who took part in this study and MemoClínica for the facilities provided.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Ethics Committee of Faculdade de Medicina da Universidade de Lisboa on January 2018. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to enrolment in the study.