
Abstract
Background
Aggressive behavior affects 30-50% of patients with dementia, yet agitation and aggression are frequently conflated despite distinct etiologies and treatment implications.
Objectives
To examine how many recent studies define and distinguish agitation from aggression in adults with dementia or related disorders.
Methods
A systematic review was conducted following a PROSPERO-registered protocol (CRD420251141548) and PRISMA guidelines. PubMed, Scopus, and Web of Science were searched for original studies published between 1st January 2017 and 28th February 2026. Definitions, assessment tools, and correlates were extracted. Study quality was appraised using CASP checklist.
Results
Of 236 identified studies, after deduplication 19 studies were reviewed in full. Only 5 studies distinguished agitation from aggression, all using the Cohen–Mansfield Agitation Inventory.
Conclusions
Failure to distinguish agitation from aggression remains common and likely contributes to suboptimal management and overuse of antipsychotic medications in neurocognitive disorders.
Keywords
Introduction
The World Health Organization estimates there are approximately 47 million people worldwide suffering from some type of dementia, this number is furthermore expected to almost triple by 2050. 1 Aggressive behavior affects approximately 30-50% of patients with dementia.2,3 An increased risk of aggressive behavior may subsequently increase the risk of reciprocal aggressive behavior on the part of caregivers. 4
Agitation is likewise common in neurocognitive disorders, with reported prevalence ranging from 5% to 88%. This marked variability likely reflects heterogeneity in definitions and assessment approaches, including the incorporation of verbally and physically aggressive behaviors within broader agitation measures. 5
In 2017, Volicer emphasized the necessity of distinguishing between agitation and aggression. He subsequently highlighted in 2020 in this journal the importance of differentiating reactive and proactive forms of aggression in people with dementia, as these behavioral manifestations differ in etiology, triggers, and appropriate management strategies.5,6 Furthermore, Volicer and Galik (2018) argued that labeling individuals with dementia as “aggressive” can be misleading, as such behaviors often represent defensive reactions to perceived threats or intrusive care, rather than intentional harm.7-9
From a neurobiological perspective, agitation is linked to dysregulation of arousal and affective circuits, specifically an imbalance between reduced prefrontal control and heightened limbic/subcortical reactivity involving locus coeruleus-noradrenergic dysfunction, serotonergic deficits and possibly dopaminergic dysregulation. This may result in generalized hyperexcitability and emotional distress rather than consistently goal-directed hostility. These mechanisms overlap with those implicated in aggression and may contribute to the co-occurrence of agitation with verbal or physical aggression in the same individual.10-12
Aggression engages orbitofrontal-amygdalar and related prefrontal pathways, and in some models hypothalamic regions, that govern threat perception, impulsivity and inhibitory control. However, despite some overlap in neurocircuitry and neurochemistry with agitation, aggression is better regarded as a related but not synonymous construct.11,12
These neurobiological differences are broadly consistent with clinical observations that agitation more often presents as internal tension and restlessness, whereas aggression reflects externally directed harmful acts. Recognizing these mechanisms supports viewing agitation and aggression as distinct syndromes within BPSD, requiring separate assessment and, crucially, tailored management.4,10-12
Stahl and Volavka further proposed that aggression may be subdivided into impulsive, psychotic, and predatory subtypes, each linked to distinct neurobiological substrates and therapeutic approaches.13,14 Our team has previously applied this differentiation when analyzing violent acts among acutely psychotic inpatients. 15 However, it remains unclear whether similar distinctions can be identified within the spectrum of neurocognitive disorders.
This review examined how many studies published between 2017 and 2026 differentiated agitation from aggression in neurocognitive disorders as recommended by Volicer.4,6,15-17
Methodology
The protocol for this systematic review was registered in PROSPERO under the registration number CRD420251141548 prior to commencing the study. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18
We identified all studies available in the Scopus and PubMed databases that reported original data on neurocognitive disorders.
A. Search Strategy
All literature published between January 1st, 2017 and February 28th, 2026 was retrieved from the electronic databases of PubMed, Scopus, and Web of Science Core Collection. The search period was from 2017 till February 2026 to capture contemporary evidence published after the influential work by Volicer et al. in 2017. The strategy combined MeSH and free-text title/abstract terms. Full text filter was used, when available. Only studies published in English or Czech were considered.
The following boolean search strategy was used in PubMed: (“Psychomotor Agitation”[Mesh] OR agitation[tiab] OR agitated[tiab] OR “psychomotor agitation”[tiab] OR restlessness[tiab] OR restless[tiab]) AND (“Aggression”[Mesh] OR aggression[tiab] OR aggressive[tiab] OR “aggressive behavior”[tiab] OR “aggressive behaviour”[tiab] OR violence[tiab] OR violent[tiab] OR hostility[tiab]) AND (“Neurocognitive Disorders”[Mesh] OR “Dementia”[Mesh] OR “Alzheimer Disease”[Mesh] OR “Mild Cognitive Impairment”[Mesh] OR “Brain Injuries, Traumatic”[Mesh] OR “Huntington Disease”[Mesh] OR “Wernicke-Korsakoff Syndrome”[Mesh] OR dementia[tiab] OR dementias[tiab] OR “neurocognitive disorder”[tiab] OR “neurocognitive disorders”[tiab] OR “major neurocognitive disorder”[tiab] OR “major neurocognitive disorders”[tiab] OR “mild neurocognitive disorder”[tiab] OR “mild neurocognitive disorders”[tiab] OR “mild cognitive impairment”[tiab] OR MCI[tiab] OR Alzheimer*[tiab] OR “frontotemporal dementia”[tiab] OR “frontotemporal lobar degeneration”[tiab] OR “vascular dementia”[tiab] OR “Lewy body dementia” [tiab] OR “Lewy body disease” [tiab] OR “Parkinson disease dementia” [tiab] OR “traumatic brain injury” [tiab] OR “traumatic brain injuries” [tiab] OR TBI[tiab] OR “acquired brain injury” [tiab] OR “acquired brain injuries” [tiab] OR “Wernicke-Korsakoff syndrome” [tiab] OR Korsakoff[tiab] OR “alcohol-related neurocognitive disorder” [tiab] OR “alcohol induced neurocognitive disorder” [tiab] OR “Huntington disease” [tiab] OR “Huntington’s disease” [tiab] OR “organic brain disorder” [tiab] OR “organic brain disorders” [tiab] OR “organic brain syndrome” [tiab] OR “organic brain syndromes” [tiab] OR “organic mental disorder” [tiab] OR “organic mental disorders” [tiab]) NOT (review[pt] OR meta-analysis[pt] OR systematic review[ti] OR editorial[pt] OR letter[pt] OR comment[pt]) NOT (animals[mh] NOT humans[mh]). Equivalent search strings adapted to database syntax were used for Scopus and Web of Science. No additional restrictions were applied regarding study design, publication status, or setting.
The search strategy is depicted in the Figure 1. To ensure robustness, separate searches were performed independently by the first author and replicated by a large language model (ChatGPT 5.4). The two sets of results were compared, merged, and deduplicated in Mendeley. At the end of the review process, references of all included studies were hand-searched to identify any further relevant data. PRISMA-based strategy flow-chart of article selection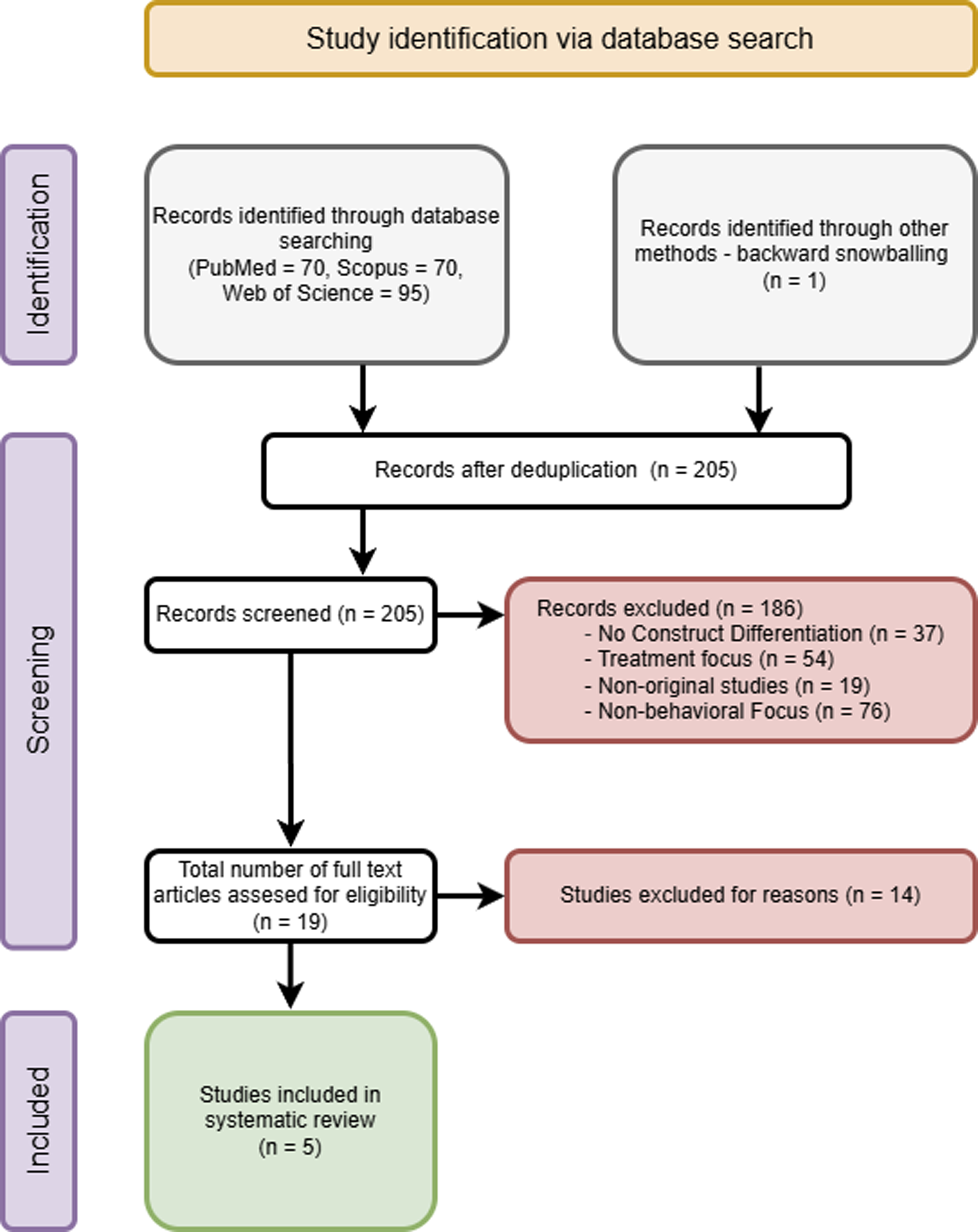
B. Role of the LLM in Search Strategy
An LLM (ChatGPT 5.4) was used only as a supportive tool to reproduce and stress-test database queries, provide a second, deliberately critical triage of titles/abstracts and cross-check extraction tables for completeness/consistency. Evidence for the feasibility and accuracy of such LLM-assisted data extraction approaches has recently been documented by Simsa et al. (2025). 19 Similarly, the practical use of LLM in working with databases is documented by Homiar et al. (2025). 20
The LLM did not make any final inclusion/exclusion decisions or risk-of-bias judgements. All final decisions were made by the first author, with uncertainties discussed with a second human reviewer.
C. Eligibility Criteria
Study designs: Only original human studies (cross-sectional, cohort, case–control, and clinical trials) were included. We excluded reviews, meta-analyses, editorials, letters, protocols, conference abstracts without full data, case reports and purely conceptual, qualitative, Delphi, or stakeholder-only studies without empirical patient data.
Participants: Adults (≥18 years) with neurocognitive disorders (Alzheimer’s disease, vascular dementia, Lewy body dementia, frontotemporal dementia, Parkinson’s disease dementia, mild cognitive impairment, mild and major neurocognitive disorders, traumatic or acquired brain injury, Huntington’s disease, Wernicke–Korsakoff syndrome, alcohol-related/alcohol-induced neurocognitive disorder and older diagnostic terms such as organic brain disorder/syndrome and organic mental disorder) were eligible. Animal studies and studies of children/adolescents were excluded.
Exposures/Comparators: Studies had to define, measure and explicitly differentiate agitation and aggression. Comparisons could include agitation vs aggression, presence vs absence of either symptom, or across dementia subtypes.
Outcomes: Articles were included if they reported definitions or criteria of agitation and aggression, measurement tools used, or clinical or contextual correlates distinguishing the two constructs.
D. Study Selection
Studies obtained from the literature were evaluated using Mendeley Reference Manager, where they were summarized and deduplicated. After deduplication, the titles and abstracts were reviewed by the first author according to eligibility criteria. In parallel, ChatGPT 5.4 was instructed to apply the same criteria as critically as possible. Both screening paths were compared, and discrepancies were resolved by human review of the full texts. Selected articles were obtained for full-text evaluation. During the full-text evaluation, a snowball search was performed to check for potentially missed articles.
E. Data Extraction and Quality Assessment
Data extraction focused on study design, population and setting, operational definitions of agitation and aggression, assessment tools and reported correlates. Extraction was carried out by the first author, with ChatGPT 5.4 used to cross-check the extracted information for completeness and consistency. All final decisions were confirmed by the researcher. The methodological quality of the included studies was assessed using the Critical Appraisal Skills Programme (CASP) checklists for cross-sectional and case-control studies. Detailed appraisal outcomes are provided in Supplemental Table 1. The checklist consists of 11 items with possible answers of “yes,” “no,” or “can’t tell”. 21 Risk of bias was considered “high” when up to 49% of responses were rated “yes,” “moderate” when 50-69% were rated “yes,” and “low” when ≥70% were rated “yes.” A meta-analysis was not performed due to the methodological heterogeneity of the included studies.
Results
A. Search Results
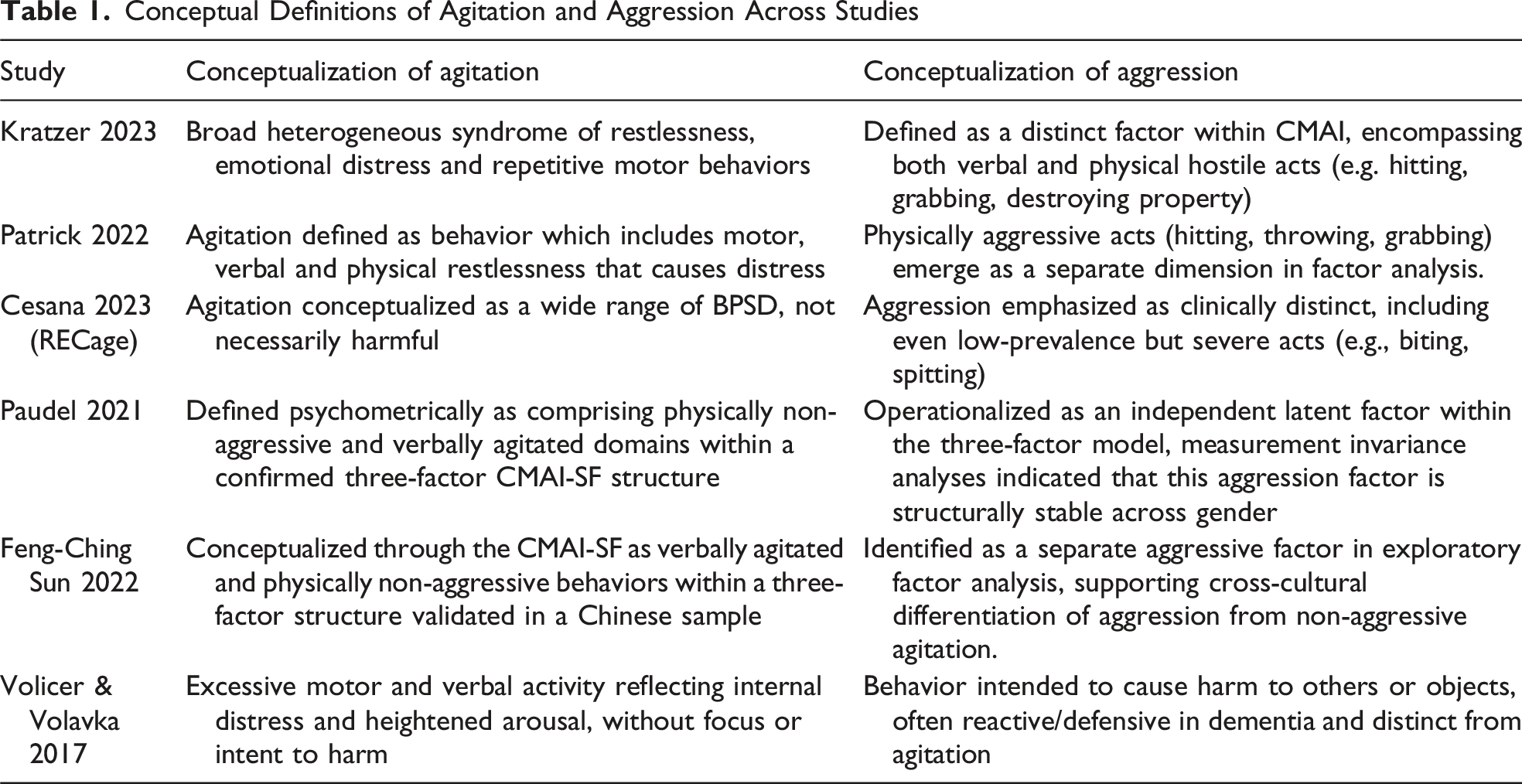
Conceptual Definitions of Agitation and Aggression Across Studies
B. Study Characteristics and Findings
Study Characteristics and Measurement Approaches
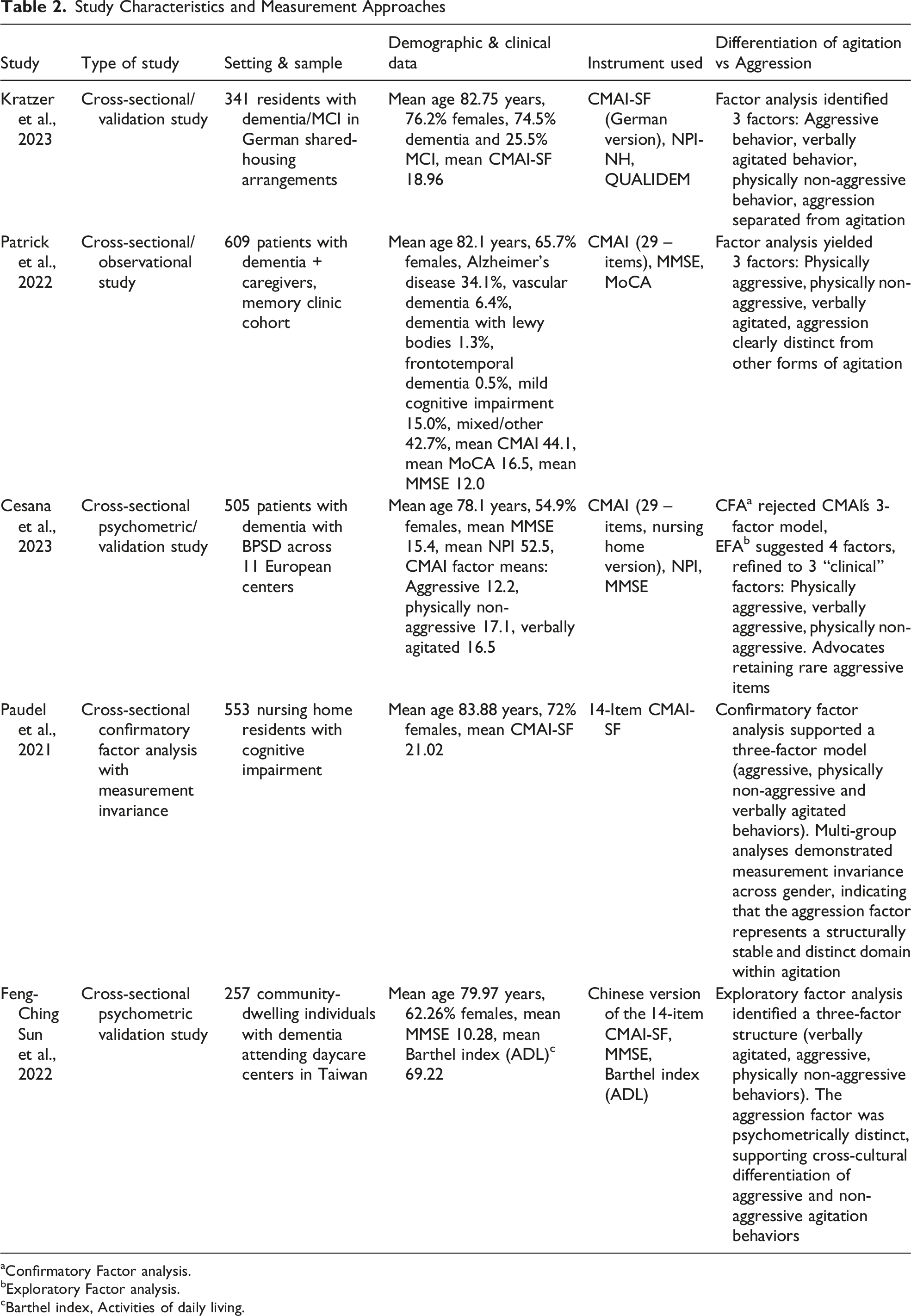
aConfirmatory Factor analysis.
bExploratory Factor analysis.
cBarthel index, Activities of daily living.
Kratzer et al. (2023) provided a rigorous psychometric validation of the German short form of the CMAI (CMAI- SF) in a cohort of 341 residents with dementia and mild cognitive impairment. The sample was drawn from 97 German shared-housing arrangements, had a mean age of 82 years, was predominantly female (76.2%) and included participants ranging from MCI to severe dementia. Their factor analysis yielded a stable three-domain structure, i.e., physically aggressive, physically non-aggressive, and verbally agitated behaviors. This selection closely mirrors the architecture of the original instrument while confirming the robustness of aggression as an empirically discrete subdomain of agitation. 22
Patrick et al. (2022) analyzed a larger sample of 609 individuals with dementia from a memory clinic and replicated this three-part structure using the complete 29-item CMAI questionnaire. The care recipients had a mean age of 82 years and 65.7% were female. 23 Patrick et al. (2022) used a diagnostically heterogeneous memory-clinic sample and excluded very low-frequency aggressive items before factor analysis.
Cesana et al. (2023), drawing on the multinational RECage project with 505 participants across 11 European centers, extended the field by subjecting the CMAI to both confirmatory and exploratory factor analyses. The cohort had a mean age of 78 years, 54.9% were women and the mean MMSE was 15.4, indicating at least moderate overall cognitive impairment. Rejecting the adequacy of the conventional three-factor model, they proposed a more differentiated four-factor solution, parsing verbal and physical aggression into separate clusters. 24 This four-factor model is in accordance with previous studies.25,26 Cesana et al. (2023) also demonstrated how exclusion of low-prevalence aggressive acts can substantially affect the resulting factor structure.
Paudel et al. (2021) further supported the three-factor structure of the CMAI-SF in a sample of 553 nursing home residents with cognitive impairment, confirming distinct aggressive, physically non-aggressive and verbally agitated domains. Measurement invariance across gender reinforced the structural stability of this differentiation. Participants had a mean age of 83 years, 72% were female, and the sample was characterized by marked cognitive impairment. 27 Notably, Paudel et al. were the only authors to formally test sex invariance and found no significant latent mean differences across gender.
Sun et al. (2022) extended these findings cross-culturally by validating a Chinese version of the CMAI-SF in 257 individuals with dementia. Participants had a mean age of 79 years, 62.26% were females and showed substantial cognitive and functional impairment. The factor analysis identified separable aggressive, verbally agitated and physically non-aggressive domains, demonstrating the reproducibility of this structure across cultural settings. 28 The study also supported concurrent validity against the NPI agitation/aggression domain and the Cornell agitation item.
Clinical and Research Implications
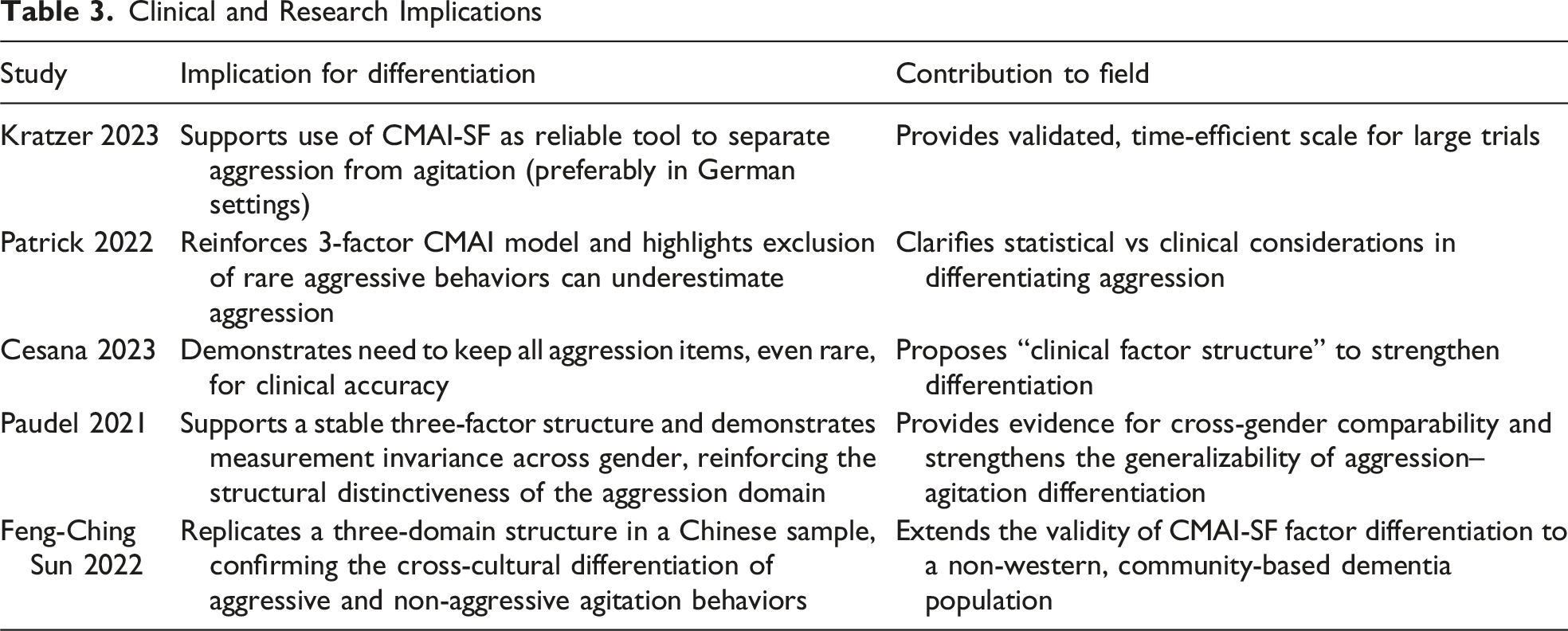
In total, the five studies encompass 2265 participants, providing a solid empirical foundation. They cover a wide range of settings, from memory clinics to residential care facilities. Despite minor differences in the identified three-to four-factor structures, all converge on a consistent finding, i.e., aggressive behaviors can be reliably distinguished from non-aggressive agitation.
Discussion
To our knowledge, this is the first systematic review explicitly aimed at disentangling agitation from aggression in dementia and other neurocognitive disorders. Only five studies explicitly differentiated these constructs. The limited number of included studies reflects the effort for explicit conceptual differentiation rather than a broader absence of research on agitation or aggression. Nevertheless, the included studies offer important insights into the measurement and conceptualization of agitation and aggression. Future research should prioritize longitudinal studies examining the triggers, course and management of these behaviors, including coping responses among caregivers and healthcare staff.
Earlier systematic reviews have generally grouped these behaviors under the broad umbrella of behavioral and psychological symptoms of dementia, without clearly differentiating agitation from aggression, 29 while more recent works have sought to distinguish them more explicitly, although the boundary remains blurred in contemporary definitions.30,31
Overall, the reviewed studies support a clear conceptual and empirical distinction between agitation and aggression (Table 1). Across settings and samples, aggression can be psychometrically isolated from non-aggressive agitation. Factor-analytic approaches consistently show that physically and verbally aggressive behaviors cluster separately from restlessness, pacing, or repetitive questioning.22,23,27 Importantly, this distinction is clinically meaningful rather than merely statistical. Aggressive behaviors impose a qualitatively different caregiver burden, causing embarrassment and fear, whereas non-aggressive agitation primarily disrupts daily routines. Excluding rare but severe aggressive acts (e.g. biting or spitting) for statistical convenience would therefore eliminate behaviors of high clinical relevance.23,32
Crucially, Cesana et al. (2023) emphasized retaining low-prevalence but high-severity aggressive acts (eg, biting, spitting, sexual advances), warning that statistical exclusion risks obscuring clinically salient behaviors. Their clinically grounded factor structure corrects purely statistical approaches and reinforces aggression as multifaceted yet distinct from non-aggressive agitation. These findings confirm that agitation and aggression should not be conflated in either clinical research or practice. 24
Paudel et al. (2021) further supported this distinction by confirming a three-factor CMAI-SF structure comprising aggressive, physically non-aggressive and verbally agitated behaviors. The stability of this structure across gender further reinforces aggression as a distinct domain. 27
Sun et al. (2022) extended these findings cross-culturally by validating the CMAI-SF in a Chinese sample, again identifying separate aggressive, verbally agitated and physically non-aggressive domains. This supports the reproducibility of the agitation-aggression distinction across cultural settings. 28
In addition to psychometrics, Patrick et al.’s contribution lies in carefully connecting agitation to caregiver burden. They demonstrated that physically aggressive behavior had a significant psychosocial burden, i.e., it caused embarrassment and frustration in caregivers, while non-aggressive manifestations, such as restlessness or repeated questioning, primarily disrupted the daily routine. This difference in impact underscores the practical need to distinguish aggression from other agitated behaviors. 23
Current consensus definitions have improved the characterization of agitation, but some conceptual overlap remains. The International Psychogeriatric Association´s definition distinguishes excessive motor activity, verbal aggression, and physical aggression, while still placing the latter two within the broader agitation construct. 30
Instruments such as the Neuropsychiatric Inventory (NPI) reflect this partial overlap by combining agitation and aggression within a single domain. 6 In contrast, the Cohen-Mansfield Agitation Inventory (CMAI) consistently treats aggressive behavior as a distinct factor and has been central to advancing empirical differentiation. 6 Analyses of the CMAI identify separable domains for physically aggressive, physically non-aggressive, and verbally agitated behaviors.22,23,26 Refinements proposed by the RECage project and validation of the CMAI–Short Form further confirm the robustness of an independent aggression domain across diverse clinical settings.22,24 Memory-clinic and outpatient studies, including Patrick et al. (2022), additionally demonstrate that this distinction has tangible clinical consequences, particularly with respect to caregiver burden. 23
Agitation vs Aggression
The reviewed evidence shows significant progress in measurement. Shortened versions of the Cohen-Mansfield Agitation Inventory have strengthened the empirical distinction between aggression and non-aggressive agitation while increasing feasibility for clinical and research use. Replication in memory clinics, nursing homes, and multinational cohorts supports the robustness and contextual validity of this distinction. Despite heterogeneity in samples, analytical approaches, and cultural settings, the results converge on one consistent conclusion: physically and verbally aggressive behaviors, such as hitting, spitting, or destroying property, represent a distinct domain of behavior, rather than a quantitative escalation of agitation.22-24 This distinction is further supported by psychiatric research indicating that verbal aggression is comparable to physical aggression in clinical severity and burden. 32
At the same time, Hendrix et al. (2025) cautioned that reliance on CMAI subdomains alone may miss clinically relevant behavioral signals and recommended using the total CMAI score alongside individual item assessment. 33 This suggests that, although aggression and non-aggressive agitation remain conceptually and psychometrically distinguishable, their measurement may still reflect partially continuous symptom expression.
This overall convergence represents a meaningful conceptual advance. Establishing aggression as a separable construct provides a stronger empirical basis for clinical assessment, improves diagnostic precision and facilitates the development and evaluation of targeted interventions.
Management of BPSD, including agitation and aggression, remains heavily reliant on pharmacological treatment in dementia care. Behavioral symptoms are associated with increased psychotropic prescribing, and psychotropic polypharmacy is common, often contributing to inappropriate use and adverse outcomes such as sedation and falls. These findings further underscore the need for more precise, symptom-targeted management.34,35
The incorporation of palliative care principles into dementia care further reinforces this perspective. As emphasized by Volicer and Simard (2014), management should aim not only to suppress aggressive behavior but also to enhance comfort, dignity, and quality of life. Recognizing aggression as a heterogeneous construct enables clinicians to balance safety-focused interventions with individual care goals. 36
Limitations
Our review has important limitations. Few studies explicitly distinguished agitation from aggression, limiting the strength and generalizability of conclusions. Heterogeneity in design, samples and analytic approaches, despite universal use of the CMAI or its derivatives, may have influenced construct definitions. In addition, limiting the search to studies published since 2017 may have excluded earlier relevant literature. However, this decision was made in advance with the aim of assessing whether current research reflects a clearer conceptual distinction. An important next step will be to use longitudinal and multimethod designs to determine whether agitation and aggression differ in triggers, phenomenology, clinical course and treatment response.
Conclusion
Our review identifies a clear gap in the literature, with only five studies explicitly distinguishing aggression from non-aggressive agitation, all using the CMAI or related measures. Across settings, findings consistently show that aggression is a distinct BPSD dimension rather than an escalation of agitation. Separating aggression from agitation improves measurement validity and intervention assessment and is particularly important given the unique burden of aggression on patients and caregivers.
Supplemental Material
Supplemental material - Distinguishing Agitation From Aggression in Neurocognitive Disorders: A Systematic Review of Conceptualization, Assessment and Correlates
Supplemental material for Distinguishing Agitation From Aggression in Neurocognitive Disorders: A Systematic Review of Conceptualization, Assessment and Correlates by Pavel Kubíček and Jan Vevera in Journal of Geriatric Psychiatry and Neurology
Supplemental Material
Supplemental material - Distinguishing Agitation From Aggression in Neurocognitive Disorders: A Systematic Review of Conceptualization, Assessment and Correlates
Supplemental material for Distinguishing Agitation From Aggression in Neurocognitive Disorders: A Systematic Review of Conceptualization, Assessment and Correlates by Pavel Kubíček and Jan Vevera in Journal of Geriatric Psychiatry and Neurology
Footnotes
Acknowledgments
The authors would like to thank the Faculty of Medicine in Pilsen, Charles University, for institutional support.
Ethical Considerations
Ethical approval was not required for this study as it is a systematic review of previously published literature and does not involve new data collection from human participants.
Author Contributions
Pavel Kubíček conducted the review, data analysis, and manuscript preparation. Jan Vevera conceived the study idea, provided guidance, and critically revised the manuscript. Both authors approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Charles University’s Specific University Research (SVV) programme under grant number: SVV260631. The study was supported by the Charles University, project GA UK No. 388226.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.