
Abstract
Introduction
Cognitive rehabilitation (CR) enhances the autonomy of patients with Alzheimer’s disease. Their daily activities are likely dependent on attention networks.
Method
This pilot resting-state fMRI study investigated the cerebral correlates of CR in participants with mild Alzheimer disease (n = 22), compared to a control intervention in patients (n = 21) and in healthy participants (n = 27). Connectivity changes between dorsal and ventral attention networks were expected after 3 months of rehabilitation.
Results
A mixed ANOVA comparing pre- and post-intervention data across groups revealed increased connectivity between the dorsal and the ventral attention network following CR (FDR-corrected P = .0072). A post hoc correlation analysis of post-intervention data in the CR group showed that greater autonomy in daily activities was associated with stronger functional relationship between the two attention networks (FDR-corrected P = .0001).
Conclusion
Enhanced connectivity between attention networks may be a characteristic of CR benefits in individuals with mild Alzheimer disease.
Keywords
Introduction
Alzheimer’s disease (AD) is characterized by behavioral, emotional, and cognitive symptoms that interfere with daily activities. Individualized cognitive rehabilitation (CR) programs can delay the progression of functional impairments.1,2 CR is a therapeutic approach in which patients and their relatives collaborate with health professionals to identify personally meaningful goals and to design and implement strategies to achieve them. 3 The efficacy of CR has been demonstrated in randomized controlled trials.4-11
However, little is known regarding the brain mechanisms that underlie the effect of CR in early AD. Some studies have reported changes in cerebral activity in individuals with mild cognitive impairment (MCI) following cognitive stimulation or training.12-14 These functional MRI (fMRI) studies have shown widespread increases in brain activity during memory tasks after such interventions, particularly in regions of the default mode network (DMN). 15 These changes have been interpreted as either normalization of previously dysfunctional regions or compensatory recruitment of alternative brain areas to support task performance.12,16 Beyond task-related fMRI, there is currently a growing interest in modifications of resting cerebral networks. For instance, a computerized cognitive training program targeting executive and memory functions was found to modify DMN functional connectivity measures in AD patients. 17 In a randomized controlled trial of 6-month cognitive training (compared to crossword training) in individuals with amnestic MCI, improved controlled cognition in the experimental group was associated with increased connectivity strength between the left dorsolateral prefrontal cortex and the medial prefrontal cortex during a working memory task fMRI. 18 In a recent study of cognitive stimulation in individuals with mild to moderate AD, seed-to-voxel analyses of resting-state fMRI revealed increased connectivity between the left posterior hippocampus and the left postcentral gyrus, correlating with cognitive improvement as measured by the Mini Mental State Exam (MMSE). 19 However, MMSE and cognitive scores do not typically improve after CR. 11 In a positron emission tomography (FDG-PET) study comparing CR to an active control intervention in patients with MCI and AD, an attenuated decline in glucose metabolism was observed in the left anterior temporal and anterior cingulate cortices of MCI participants. 20 The anterior cingulate cortex (ACC), a key node of the executive attention network, plays an important role in attentional processing. 21 Notably, the FDG-PET measures did not correlate with cognitive outcomes as assessed by MMSE. Regarding fMRI studies of CR, a participant with MCI demonstrated increased activation in prefrontal and temporoparietal regions, alongside improved performance in a face-name association task following CR. 22 In another study, 19 patients with early AD underwent the same face-name association task before and after a 6-week CR program that included memory strategies. 23 While behavioral performance did not improve after CR, increased activation was found in the frontal gyri, left insula and right medial parietal cortex. The authors interpreted these results as partial restoration of brain function in regions involved in the recognition of face-name associations.
The goal of our observational study was to investigate some cerebral plasticity mechanisms supporting the efficacy of an individualized CR program focused on the rehabilitation of daily activities in early AD. 24 This type of intervention is not expected to produce changes in memory- or executive-related neural networks as those functions are not targeted by CR procedures. However, the successful execution of consistent, goal-directed activities depends on the functioning of attentional networks. 25 Patients in early AD stages commonly exhibit attentional impairments.26,27 Research on brain-injured patients has shown that those who retain stronger attentional capacities are more likely to benefit from rehabilitation techniques, such as the use of external memory aids. 28 In our study, we specifically examined the interaction between two attentional networks: the dorsal attention network (DAN), involved in top-down attentional control, and the ventral attention network (VAN), involved in bottom-up, stimulus-driven attention. 29 These networks typically operate in an antagonistic manner, thereby protecting attention-demanding tasks from interference by non-target distractor information.30,31 The DAN and the VAN have been shown to interact during the resting state, 32 to play important roles in AD33-36 and to retain task-related modulation in the early stages of the disease. 37 In the latter study, we observed that the DAN activation was load-dependent and remained functionally connected to the VAN during a verbal short term memory task.
To explore changes in connectivity between attention networks, we compared pre- and post-intervention resting-state fMRI data from AD participants who received a 3 months CR program (ADR) with data from AD patients (ADC) and healthy older participants (HC) who received a control intervention. We hypothesized that stronger rehabilitation effects would be associated with greater connectivity between the two attentional networks under investigation.
Population and Methods
Participants
Fifty-one patients with Alzheimer’s disease and 35 healthy older control participants were included in this observational study. Since CR is not appropriate for healthy volunteers without cognitive complaints, randomization was not an option for this pilot study. Among recently diagnosed AD patients, 26 who met the inclusion criteria for the CR program (mild dementia, willingness to maintain daily activities at home with caregiver support, and absence of mood disorder) were included in the CR group. Among patients who postponed CR, 25 AD participants and their caregiver accepted to be included in the study. They postponed CR because they could not identify an activity suitable for adaptation at that time, they lacked time or interest in learning new strategies, or they did not perceive their daily difficulties as significant. Following participants drop-outs (between the pre- and post-rehabilitation session) and exclusions due to poor quality fMRI, data from 43 AD patients and 27 healthy control participants were retained for analysis (see Supplemental Figure 1 for a flow chart of the experimental design). Of these, 22 patients who underwent the individualized CR program were assigned to the AD Rehabilitation (ADR) group. The remaining 21 patients participated in an active control program and were assigned to the AD Control (ADC) group.
Demographic Characteristics of Participants
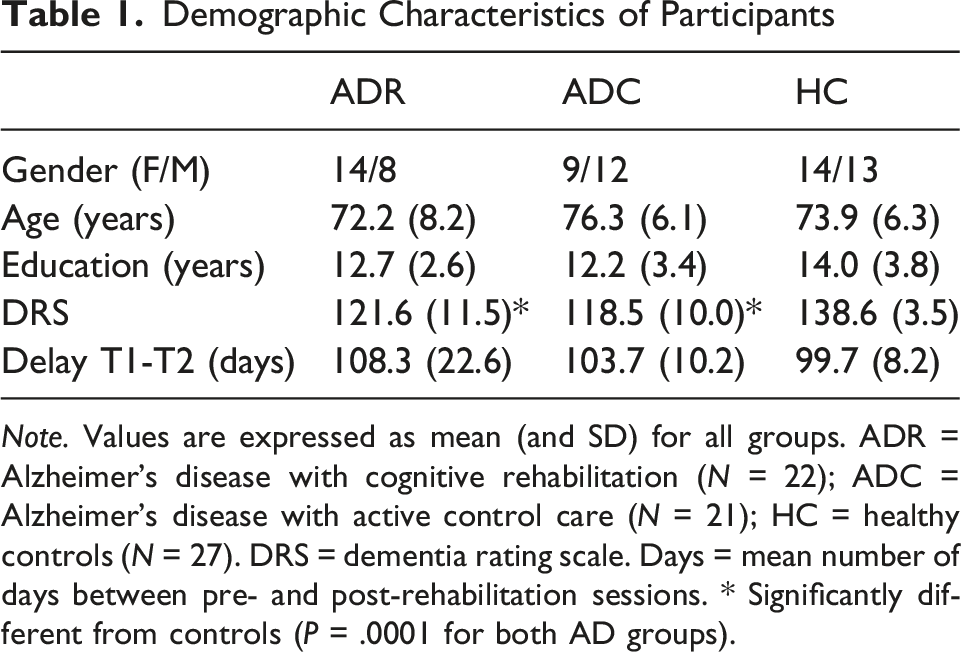
Note. Values are expressed as mean (and SD) for all groups. ADR = Alzheimer’s disease with cognitive rehabilitation (N = 22); ADC = Alzheimer’s disease with active control care (N = 21); HC = healthy controls (N = 27). DRS = dementia rating scale. Days = mean number of days between pre- and post-rehabilitation sessions. * Significantly different from controls (P = .0001 for both AD groups).
Experimental Design of the Intervention Between fMRI Sessions
Individualized Cognitive Rehabilitation Program in the ADR Group
The CR program was delivered by neuropsychologists and occupational therapists who were not involved in the neuroimaging experiment. The rehabilitation goals were chosen by the patient and their caregiver, ensuring personal relevance. These goals typically fell into three broad categories: using memory aids, adapting tools or devices, and organizing daily activities (see Supplemental Table 1). The number of activities trained for each patient ranged between two and six (mean 3.7 ± 1.1). Interventions followed one or more standardized procedures: facilitation of performance, learning of new knowledge or tools using different methods (spaced retrieval, errorless learning, vanishing cues) or use of external aids and environmental adaptations.4,24 A common feature across all procedures was the need for sustained attention, engaging the patient’s attentional resources. Most rehabilitation sessions (1-h session per week for 3 months) took place at the patient’s home, although some were held at the memory clinic.
Outcome Measures of the Rehabilitation Program
Because one of the most important goals of CR is the maintenance of a certain level of autonomy in daily activities, we used as outcome measure the Profinteg scale, an experimental tool for measuring adaptive behavior across a broad range of activities. 46 Ninety-eight daily and leisure activities of varying complexity were evaluated. The therapist explained the scoring method to the caregiver and recorded the caregiver’s ratings for the different activities. 24 Scores ranged as follows: 0 points indicated no difficulties; 1 point was given for failure to initiate the activity, for omission of one or more steps, or for wrong execution of one or more steps (maximum 3 points); 4 points corresponded to perseverative errors (despite prompting and supervision); and 5 points meant the activity could not be carried out. Additionally, caregivers rated both objective burden (time required for assistance with problematic activities) and subjective burden (effort required to help the patient performing the problematic activity) on a scale ranging from 0 to 3. Dependence and burden scores were summed across all the assessed activities and expressed as a percentage of the maximum score. This assessment was conducted at baseline (T1) and after 3 months of CR (T2) to evaluate the program’s effectiveness.
Active Control Program in the ADC and Healthy Participants Groups
The ADC and healthy participants groups followed an active control comparison program to ensure that post-rehabilitation MRI changes in the ADR group were specific to the individualized rehabilitation program. The program provided psychosocial support and cognitive stimulation. Participants received an informational booklet about memory impairment and strategies for coping with daily difficulties. Over the 3-month period (between T1 and T2), participants in both groups were asked to complete paper-based exercises (eg, crosswords, word searches or related activities) for 1 h twice per week. To control for the social interaction provided in the ADR group, control participants received three follow-up phone calls during the active control program to discuss topics related to daily activities. Because such a control intervention was previously shown to offer no functional benefit to AD patients, 47 levels of dependence in daily activities were not assessed in the ADC or healthy participants, ensuring better compliance.
Statistical Analyses
Neuropsychological measures were compared between groups using analysis of variance (ANOVA) and Tukey’s HSD as post-hoc comparison. Profinteg scores in the ADR group were compared between T1 and T2 using repeated measures ANOVA.
Experimental Design of Neuroimaging Acquisition
All participants underwent a resting state fMRI session before (T1) and after (T2) the rehabilitation program or the control intervention. During the 8-minute resting-state sequence, participants were asked to lie still in the scanner, to close their eyes and to let their minds wander. A total of 200 volumes were acquired per session and the first three volumes were discarded to avoid T1 saturation effects.
Due to a scanner change during the study, data were acquired on two different 3-Tesla MRI scanners. The same machine was always used pre- and post-intervention. Data for 19 controls, 10 ADR, and 8 ADC patients were collected at T1 and T2 on a 3-Tesla head-only Siemens Allegra scanner (Siemens, Allegra, Erlangen, Germany) with the standard transmit-receive quadrature head coil. For the resting sequences, T2*-weighted functional images were acquired using a gradient-echo echo-planar imaging (EPI) sequence with TR = 2040 ms, TE = 30 ms, flip angle = 90°, FoV = 192 × 192 mm2, matrix size = 64 × 64, voxel size = 3 × 3 × 3 mm3. Thirty-four 3-mm thick transverse slices were acquired, with an interslice gap of 25%, covering the whole brain. Gradient-recalled sequences were applied directly after the functional sequences to acquire two complex images with different echo times (TE = 4.92 and 7.38 ms respectively) and generate field maps for distortion correction of the EPI images. A high-resolution T1-weighted image was acquired for each participant with the T1-weighted 3D magnetization-prepared rapid gradient echo (MPRAGE) sequence with TE = 4.35 ms, TR = 1960 ms, inversion time (TI) = 1100 ms, field of view = 230 × 173 mm2, resolution = 256 × 192 × 176, voxel size = 0.9 × 0.9 × 0.9 mm3.
Data for the remaining 8 controls, 12 ADR and 13 ADC patients were collected at T1 and T2 on a whole-body 3-Tesla Siemens Prisma scanner operated with a 20-channel receiver head coil (Magnetom Prisma, Siemens Medical Solutions, Erlangen, Germany). For the resting fMRI sequences, multislice T2*-weighted functional images were acquired with a gradient-echo EPI sequence using axial slice orientation and covering the whole brain (36 slices, FoV = 216 × 216 mm2, voxel size 3 × 3 × 3 mm3, 25% interslice gap, matrix size 72 × 72 × 36, TR = 2260 ms, TE = 30 ms, FA = 90°). A gradient-recalled sequence was applied to acquire two complex images with different echo times (TE = 10.00 and 12.46 ms respectively) and generate field maps for distortion correction of the EPI images. For anatomical reference, a high-resolution T1-weighted image was acquired for each subject (T1-weighted 3D MPRAGE sequence, TR = 1900 ms, TE = 2.19 ms, TI = 900 ms, FoV = 256 × 240 mm2, matrix size = 256 × 240 × 224, voxel size = 1 × 1 × 1 mm3).
Neuroimaging Analyses
Preprocessing
Data were preprocessed and analyzed using SPM12 (Wellcome Department of Imaging Neuroscience, https://www.fil.ion.ucl.ac.uk/spm) implemented in MATLAB 7.12 (Mathworks Inc, Sherborn, MA). For each participant, EPI time series were corrected for motion and distortion using Realign and Unwarp 48 together with the FieldMap toolbox. 49 Functional scans were realigned using rigid body transformations, iteratively optimized to minimize the residual sum of squares between the first image and each subsequent image. A mean realigned functional image was then calculated by averaging all realigned scans. This mean functional image was coregistered to its corresponding structural T1-weighted image acquired during the first session. The resulting coregistration parameters were subsequently applied to the realigned functional images. The mapping from participant to MNI space was estimated from the structural image using the “unified segmentation” approach. 50 The warping parameters were then separately applied to the functional and structural images, resulting in normalized images with resolutions of 2 × 2 × 2 mm3 and 1 × 1 × 1 mm3, respectively. Finally, the warped functional images were spatially smoothed using a Gaussian kernel of 8 mm full-width at half maximum (FWHM). Further details on motion and noise reduction in MRI images are provided as supplemental material (Supplemental material: Motion and noise reduction in neuroimages).
Statistical Analyses of Resting State fMRI
Data from this pilot study were analyzed using the CONN toolbox
51
implemented in MATLAB. Scanner type was introduced as a covariate in all statistical analyses. A bivariate correlation was conducted to examine pairwise connectivity between a priori selected regions of interest (ROIs)
30
in the dorsal (DAN: right and left intraparietal sulcus 24, -56, 46 and −25, −57, 46; right and left superior frontal gyrus 26, −2, 47 and −22, −3, 49 and right middle frontal gyrus 48, 7, 34; MNI template coordinates) and ventral attention networks (VAN: right and left temporoparietal junction 52, −52, 25 and −52, −53, 23; right and left orbitofrontal cortex 34, 27, −10 and −37, 27, −8 in MNI space). Each region of interest coordinate was used as the centre of a 10-mm radius sphere created with Marsbar (https://marsbar.sourceforge.net) (see Supplemental Table 2 and Figure 1). For each ROI, a representative BOLD time series was extracted by averaging the signal across all voxels within the 10-mm radius sphere. Functional connectivity between ROIs was estimated using bivariate Pearson correlation coefficients calculated from the extracted time series. Correlation coefficients were Fisher z-transformed prior to group-level statistical analyses. The resulting connectivity values reflect the temporal correlation between activity in the selected regions. The fMRI-based outcome variables for the between-network connectivity were represented as a 5 (DAN ROIs) × 4 (VAN ROIs) connectivity matrix, yielding 20 pairwise tests. Exploratory within-network connectivity analyses were additionally conducted separately for DAN and VAN, using the same ROI-to-ROI mixed ANOVA design and FDR correction procedure. False discovery rate (FDR) correction was applied to account for multiple comparisons. Two main analyses were conducted. The first resting state fMRI analysis tested for between group differences in connectivity between attentional networks at T1. The second fMRI analysis was an interaction. To explore pre- and post-rehabilitation or control intervention differences and group effects, a 3 (groups) by 2 (sessions: T1 and T2) mixed ANOVA was conducted on the connectivity values for each ROI-ROI pair (T-stat). To test if results were reproducible using a different method of data analysis, we also performed a follow-up (confirmatory) 3 (groups) by 2 (sessions: T1 and T2) mixed ANOVA on seed to whole brain voxels connectivity in SPM12, using as seed a ROI obtained in the second (ANOVA on ROI to ROI) analysis. Regions of the of the dorsal (blue) and the ventral (red) attention networks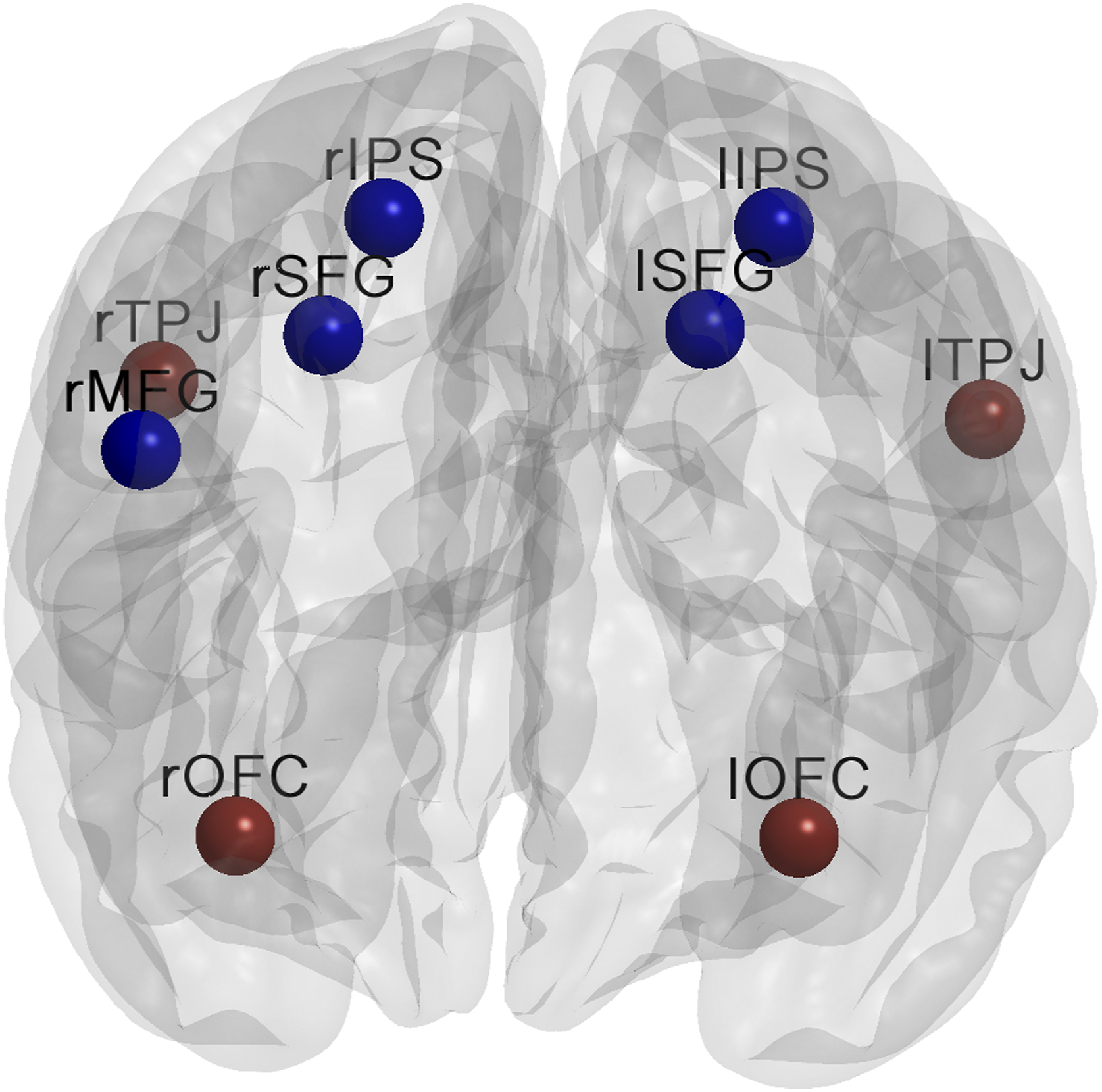
Lastly, a post-hoc (complementary) brain – behavior correlation analysis was conducted in the ADR group only. This was a classical correlation analysis at T2 (post-rehabilitation) between behavioral (autonomy in daily activities) and functional (connectivity between brain regions) data. The statistical threshold was set at P < .05 FDR-corrected.
Results
Behavioral Assessment Prior to Intervention
Both patient groups showed impaired performance on most neuropsychological measures compared to the healthy control group (see Supplemental Table 3 for descriptive data and statistical significance tests). With the exception of poorer performance for the ADC relative to the ADR group on the memory subtest of the Dementia Rating Scale (DRS), no other significant differences were found between the two AD groups. The depression score was higher in the ADR than in the HC group, but no differences were observed between the two AD groups.
Pre-Versus Post-Intervention Neuropsychological Measures
There was no significant effect of time or time-by-group interaction in any of the neuropsychological measures (data not shown).
Pre- and Post-Rehabilitation Level of Autonomy in Daily Activities in the ADR Group
Pre- and Post-rehabilitation Measures for the Rehabilitation Group
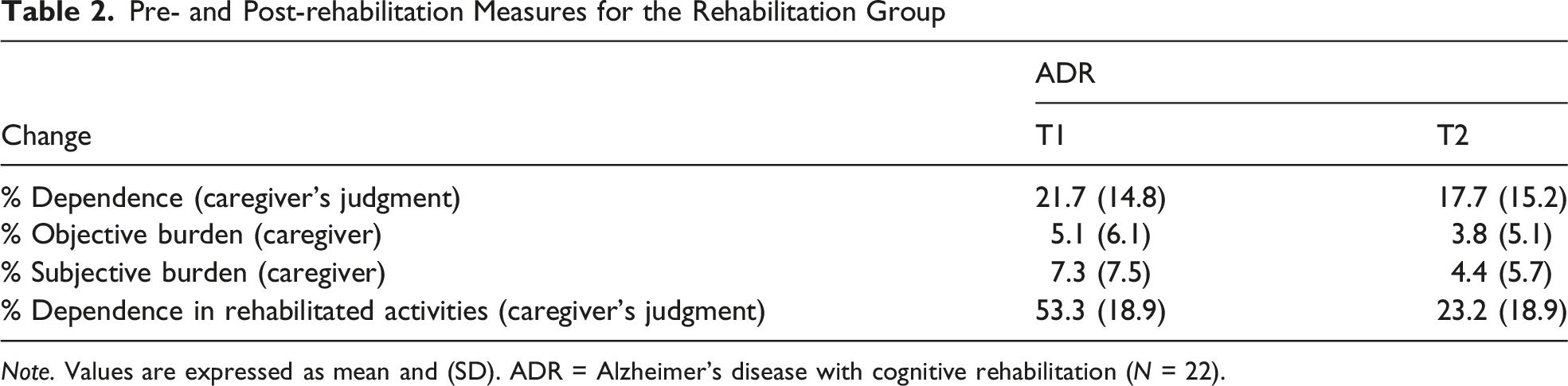
Note. Values are expressed as mean and (SD). ADR = Alzheimer’s disease with cognitive rehabilitation (N = 22).
Resting-State fMRI Results
First, when considering connectivity between the attention networks at baseline, there was no significant differences between the three groups.
Second, for the ANOVA, there was no main effect of group or time. However, when considering interactions between the attention networks, the analysis revealed one significant result, as illustrated in Figure 2. When contrasting the ADR group with the ADC group (contrast vector 0, 1 -1), we found greater connectivity at T2 compared to T1 between two core regions, respectively of the VAN network (left temporoparietal junction) and the DAN network (right intraparietal sulcus) [T (67) = 3.33; FDR corrected P = .0220]. The same result was found when contrasting the ADR group with the control group [contrast vector −1 1 0; T (67) = 2.88; FDR corrected P = .0302] and also when contrasting connectivity in the ADR group with the mean value of the other two groups [contrast vector −.5 1 −.5; T (67) = 3.60; FDR corrected P = .0072]. In a post-hoc analysis, no significant difference in connectivity between T2 and T1 was observed in either the healthy control or the ADC group. In contrast, in the ADR group, connectivity was increased at T2 compared to T1 between the left temporoparietal junction and the right intraparietal sulcus (rIPS) [T (21) = 4.57, FDR corrected P = .0012], as well as between the right temporoparietal junction and the rIPS [T (21) = 4.49, FDR corrected P = .0024]. These findings indicate that connectivity between the VAN and DAN regions was specifically increased following CR treatment in the ADR group. Moreover, in a confirmatory SPM12 mixed ANOVA on seed to whole brain voxels, we introduced the left temporoparietal junction (lTPJ) ROI as seed. The analysis showed significant result (T (66) = 3.22) with a cluster centered on the right intraparietal sulcus (cluster FDR corrected P = .006) at T2 compared to T1 in the ADR compared to the two other groups (Supplemental Table 4). In this SPM12 mixed ANOVA, there was no significant correlation between lTPJ and any DMN region. Correlation between left temporoparietal junction and right intraparietal sulcus at T1 and T2 in HC (red), ADR (black) and ADC (blue) groups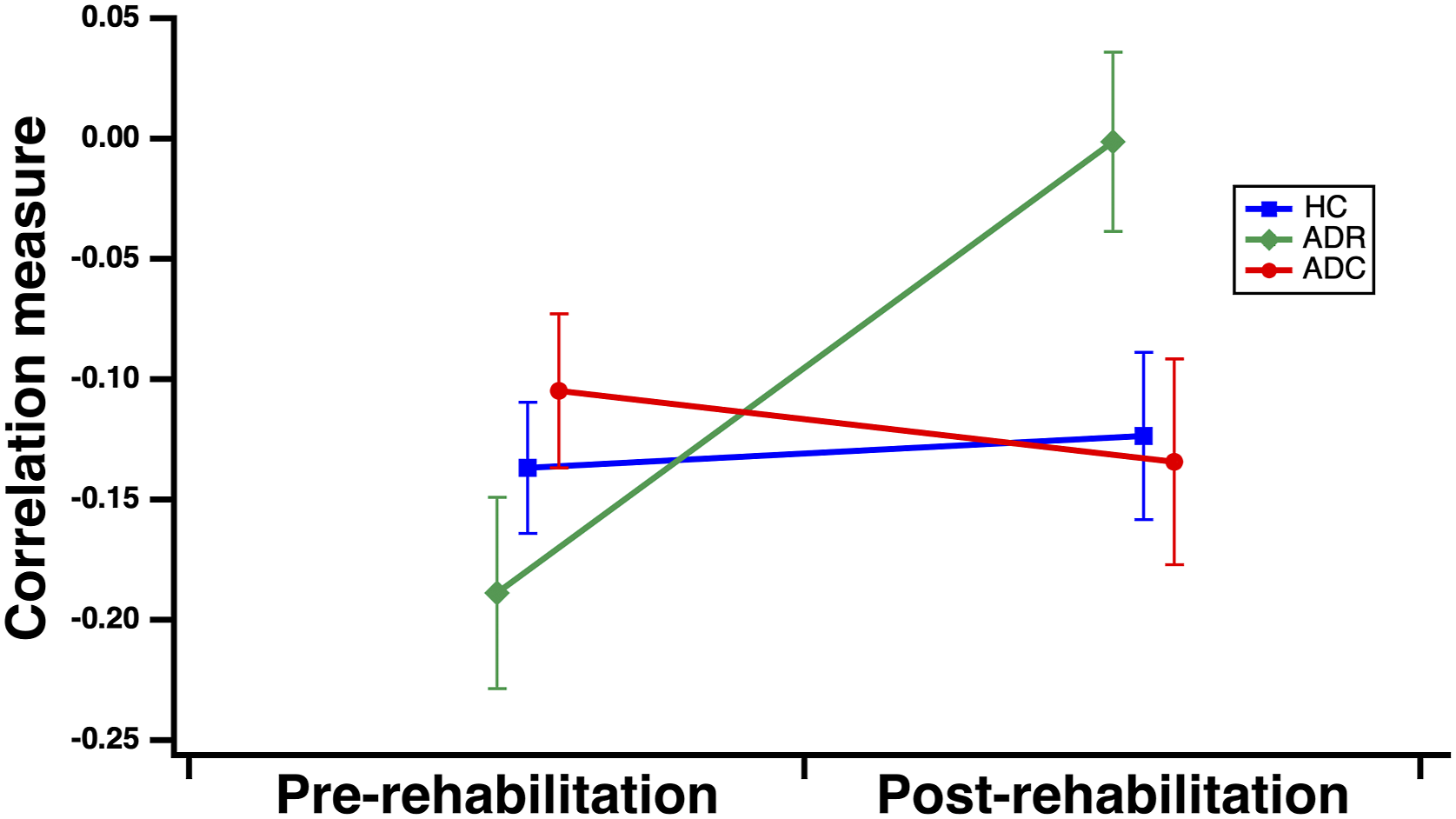
The exploratory analyses of within-network connectivity did not reveal any significant group-by-session interaction for either DAN or VAN connectivity after FDR correction.
Post hoc Correlation Analysis
We tentatively examined the functional relevance of these treatment-related differences in attention network connectivity by performing a correlation analysis between dependence scores and connectivity values in the ADR group post-rehabilitation (at T2). We observed that a lower level of dependence in rehabilitated activities at T2 was associated with a higher degree of functional connectivity between the VAN (right temporoparietal junction) and the DAN (left superior frontal gyrus) regions [r(20) = −.57; r2 = .32; t = −3.15; FDR corrected P = .0001] (Figure 3). This result indicates that lesser dependence (ie, higher levels of autonomy) in instrumental activities of daily living (IADL) after rehabilitation was associated with greater connectivity between VAN and DAN regions in AD participants. Correlation between dependence in daily activities and connectivity index between the right temporoparietal junction (rTPJ) and left superior frontal gyrus (lSFG) at T2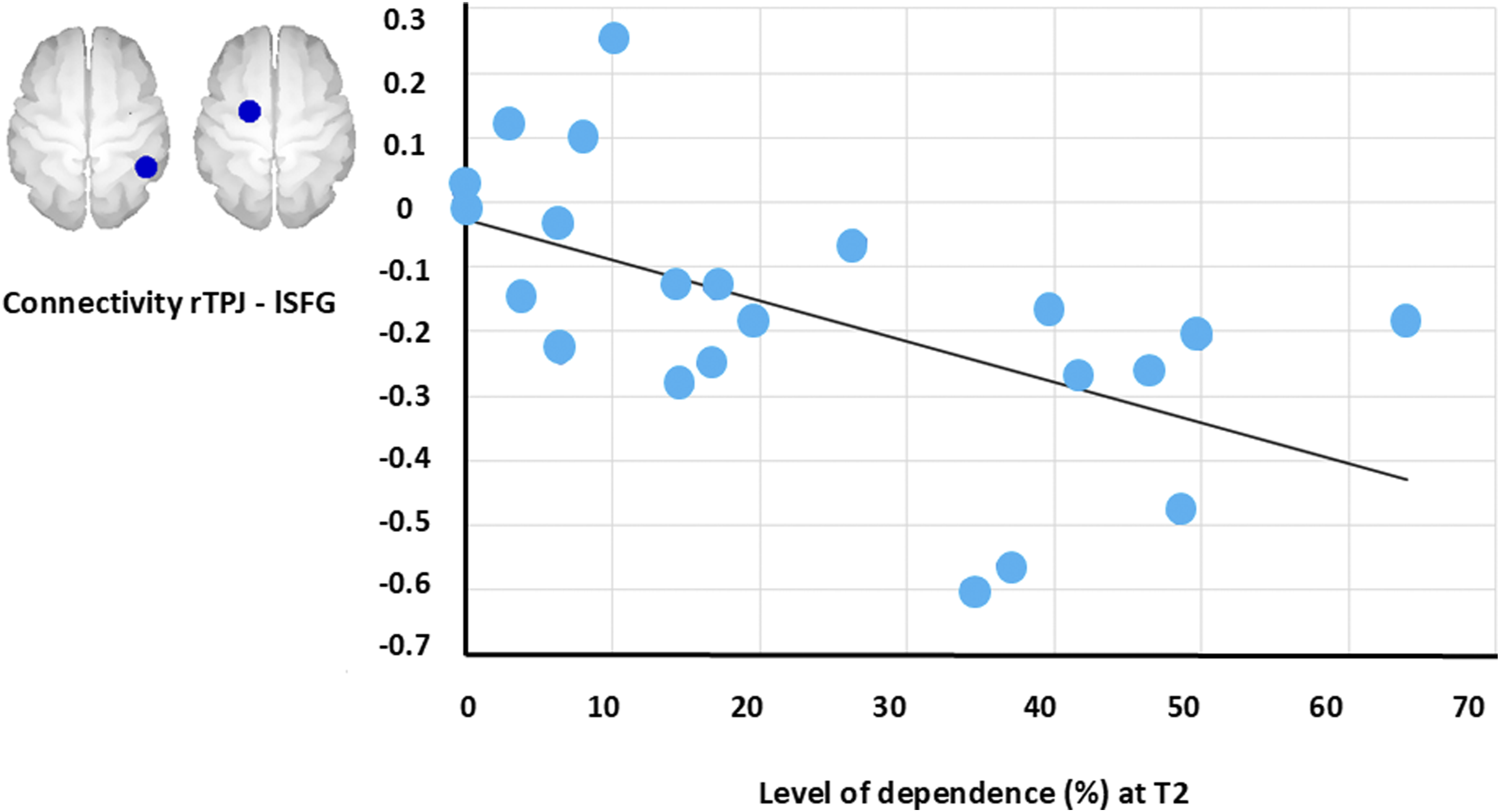
Discussion
The possible mechanisms underlying functional improvement following CR remain unclear, particularly given that CR strategies are individualized for each patient. In our study, resting state fMRI was used to examine changes between attention networks in participants with AD following a CR program (ADR group) compared to a group of AD participants (ADC) and a group of healthy older participants receiving a control intervention. An increase in connectivity between core regions of the ventral (VAN) and dorsal (DAN) attention networks was observed in the ADR group.
A decrease in brain connectivity related to cognitive decline was mainly observed in the DMN in the AD continuum. 52 We did not observe reduced connectivity within the DAN of our mild AD patients, but decreased connectivity is well established in AD participants, dependent on disease stage and on network regions.53-55 VAN connectivity would be relatively preserved, at least in early AD stages. 56 Increased connectivity between the DAN and the DMN during attentional tasks has previously been reported in AD compared to control participants, though the interpretation is complicated as it was also true in baseline condition. 57 The literature suggests that the VAN and the DAN specialize respectively in the detection of unexpected, behaviorally relevant stimuli and in top-down controlled attentional selection. It was originally thought that these networks were anti-correlated during task performance29,30,37,58 and resting fMRI. 59 However, recent findings suggest that this interaction pattern is flexible and depends on the task demands: flexible attentional control can only be achieved through a dynamic interaction between the VAN and DAN, where their activity may be either correlated or anti-correlated. 60 We explored one potential neural mechanism of non-pharmacological intervention, and CR was associated with increased connectivity between two core regions of the VAN and DAN. This modulation of attention networks aligns with a previous study that showed DAN activation and interaction with the VAN in mild AD patients performing a fMRI short-term memory task. 37 Another resting fMRI study compared CR to cognitive training in a small sample of participants with AD using a seed (posterior cingulate) to voxel connectivity analysis. 61 They found uncorrected effects (both increases and decreases in connectivity in both groups) when comparing baseline and follow-up data. Improved quality of live correlated with increased connectivity over time between the posterior cingulate cortex and the precuneus in the CR group. It is important to note that increased connectivity between brain networks is not always beneficial, as we previously showed that high resting fMRI connectivity between the DMN and DAN was related to poor familiar facial recognition in moderate AD patients. 62 Likewise, an attenuated DMN-DAN anticorrelation predicted cognitive decline in AD pathology. 63
In our post-hoc complementary analysis in the ADR group at T2, the correlation we observed between the connectivity level of the VAN (right temporoparietal junction) and DAN (left superior frontal gyrus) regions and IADL dependence scores suggested that greater connectivity between these attention networks was associated with better functioning in daily life following CR. Although resting-state fMRI data do not allow us to infer directional influence, a stronger causal influence of the DAN on the VAN has previously been associated with better visual attention performance. 64
Both AD groups performed similarly to each other but were less efficient than controls on most neuropsychological measures. As expected for our personalized CR and control interventions, there was no effect on neuropsychological measures of memory and attention in any of the three groups, which contrasts with selective cognitive improvements observed in some studies specifically targeting memory deficits.12,22 In line with most previous studies, individualized CR had a positive functional impact, as autonomy (lower level of dependence assessed by the caregiver for a large set of daily activities and for activities specifically targeted by the treatment) improved after treatment.4,6,24 Furthermore, both objective and subjective caregiver burden decreased after 3 months of rehabilitation. It is noteworthy noting that not all CR studies in AD have shown improvements in daily activities. Our treatment approach sought to address some of the limitations identified by previous researchers by delivering rehabilitation at home, defining personalized goals, and involving caregivers from an early stage.65,66 In a recent review of CR in AD, small effect sizes were observed for improved competences in daily activities. 67 Although caregiver assessment of IADL is subjective, they are considered reliable in AD participants.41,68 We also note that the benefits of CR are most frequently characterized by increased autonomy in IADL, rather than improvements on standardized neuropsychological tests.4,47
There are several limitations to this observational study. First, the relatively limited sample size warrants a conservative interpretation of the findings. Reproducibility is a concern, but data on CR are not yet available in large databases like ADNI. In the current study, we used the CONN toolbox for functional connectivity analyses (https://www.nitrc.org/projects/conn) which implements robust methods (eg, CompCor strategy for physiological and noise reduction, removal of movement, temporal covariates, and temporal filtering) for data processing. 51 Moreover, we obtained similar results with ROI-to-ROI analysis using the CONN toolbox and with seed to all brain voxels analysis using SPM12. A second limitation concerns group assignment. We could not implement CR in healthy volunteers without complaints regarding daily activities, and randomization was not feasible for this pilot study. Furthermore, the study was conducted in collaboration with a care center where patients chose their treatment activities, making random assignment impossible. Patients did not differ on most demographic and clinical factors; however there was a lower DRS memory score in the “control AD group” that might influence our results. We previously demonstrated that there was no improvement in IADL dependence for control AD participants, 47 and this relatively heavy assessment was not performed in the ADC group of this pilot neuroimaging study. Additionally, the caregivers who provide the IADL assessments cannot remain blind to the intervention in a cognitive rehabilitation study. A third limitation is that we did not record the time spent by participants in both programs, and the programs differed in their content and processes. However, the control intervention provided more cognitive encouragement than usual treatment. 47 Finally, it remains to be determined whether our results are also valid for more severe AD stages, where pre-treatment connectivity in the dorsal attention network is likely to be much more reduced. 69
In conclusion, our results show that CR in mild AD patients improves autonomy in IADL and is associated with increased neural connectivity between attention networks. These findings suggest that correlation, rather than anti-correlation, between the DAN and VAN may determine the success of individualized CR in early AD.
Supplemental Material
Supplemental material - Attention Networks Connectivity After Cognitive Rehabilitation in Alzheimer’s Disease
Supplemental material for Attention Networks Connectivity After Cognitive Rehabilitation in Alzheimer’s Disease by Eric Salmon, Mohamed Ali Bahri, Sophie Kurth, Fabienne Collette, Christophe Phillips, Steve Majerus, Françoise Lekeu, Anne Quittre, Vinciane Wojtasik, Catherine Olivier, Vinciane Godichard, and Christine Bastin in Journal of Geriatric Psychiatry and Neurology
Footnotes
Acknowledgments
The authors would like to thank all the participants and their relatives and the members of the GIGA Cyclotron Research Center, who helped with the study. This study was conducted at the GIGA-In Vivo Imaging technological platform of the University of Liège, Belgium.
Ethical Considerations
The study was approved by the Ethics Committee of the University of Liège (Belgian reference B707201215717). All participants gave their written informed consent prior to their inclusion in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SAO-FRA (Grant S#12005); the University of Liege (ARC 12/17-01 REST); the Belgian Scientific Policy (Inter-University Attraction Pole P7/11); the National Fund for Scientific Research (F.R.S.-FNRS); and the Fondation Roi Baudouin (Fonds Maria-Elisa and Guillaume de Beys). FC and CP are Research Directors at F.R.S.-FNRS, and CB is Senior Research Associate at F.R.S.-FNRS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.