
Abstract
Objectives
To examine associations between immigration-related factors and mild cognitive impairment (MCI) or dementia among Hispanics; and associations between immigration-related factors and cognitive performance among cognitively unimpaired Hispanics.
Methods
Data from the Health & Aging Brain Study-Health Disparities study were used. 1231 Hispanic participants were included. Six indicators, including time living in the US, nativity, age of migration, primary language, bilingualism, and acculturation level, were considered immigration-related factors. Both the three-category (dementia, MCI, and cognitively unimpaired) and binary (cognitively impaired and cognitively unimpaired) outcomes were used. The cognitive performance was evaluated by the Mini-Mental State Examination (MMSE). Multiple logistic, multinomial logistic, and linear regression models adjusted for age, sex, and education were applied.
Results
The likelihood of cognitive impairment did not differ significantly between native-born and foreign-born Hispanics, whereas foreign-born cognitively unimpaired Hispanics had significantly lower global cognition than their native-born counterparts. When stratifying by age of migration, a significant association between time living in the US and cognitive impairment was observed among early-life immigrants. A higher acculturation level was associated with lower odds of both dementia and MCI among native-born Hispanics, but was insignificant in foreign-born Hispanics. Bilingualism was significantly associated with dementia or MCI in foreign-born Hispanics. Monolingual foreign-born cognitively unimpaired Hispanics had significantly lower MMSE scores than bilingual foreign-born Hispanics.
Conclusions
Foreign-born Hispanics might be more vulnerable to cognitive aging. Bilingualism may play a more important role in cognitive health in foreign-born Hispanics than in native-born Hispanics. Acculturation may have distinct effects on foreign-born and native-born Hispanics.
Introduction
Hispanics represent the largest minority population in the US, accounting for 17.8% of the United States (US) population (57 million) in 2016.1,2 Alzheimer’s disease (AD) is a major health concern and one of the leading causes of death among the Hispanic population in the US. 3 In 2020, among Hispanics aged 65 and older, the estimated prevalence of AD dementia and all-cause mild cognitive impairment (MCI) was 14.0% (0.71 million) and 25.9% (1.30 million), respectively, substantially higher than those in the non-Hispanic White population. 4 By 2060, the total number of Hispanics aged 65 and older with AD dementia and all-cause MCI is projected to reach 3.72 million and 5.64 million, respectively. 4 Studies have shown that Hispanics developed MCI and dementia at a younger age and in more advanced stages when they were diagnosed, compared to non-Hispanic Whites.5-9 It is, therefore, of critical importance to understand the factors contributing to cognitive outcomes in Hispanics.
About one-third of Hispanics in the US are foreign-born. 2 Immigrants who are non-Hispanic White, Hispanic, or of other races and ethnicities, but not non-Hispanic Black, have been reported to have a higher prevalence of dementia than their US-born counterparts,10-12 potentially related to immigration-related factors such as access to healthcare, language barriers, and acculturation to the US. Immigration-related factors refer to a range of indicators capturing aspects of the immigration experience, which may be relevant for both foreign-born and US-born individuals. An immigrant is defined as first-generation (foreign-born) individuals, although some US-born individuals may be referred to as second- or third-generation immigrants and may still be influenced by immigration-related social and cultural contexts. Few studies have examined the impact of immigration-related factors, such as nativity, language use, and acculturation, on cognition in Hispanics. Language barriers, low socioeconomic status, and uninsured status, may lead to health disparities by health care access, health care quality, and healthcare-seeking behaviors.11,13,14 Acculturation refers to the changes resulting from intercultural interaction and exposure to a new environment, including shifts in customs, language, economic status, political life, and cultural identity. 15 Existing studies on acculturation and cognition have reported mixed findings. Some studies have indicated that higher acculturation levels are related to better cognitive performance,16,17 while another study suggested that acculturative stress was negatively associated with cognitive performance among middle-aged and older Hispanics. 18 In addition, prior studies have suggested that time living in the US and age at migration may capture cumulative and life-course exposures that are relevant to cognitive health; however, findings have been inconsistent across studies.19-23 Taken together, prior studies suggest that immigration-related factors may reflect different dimensions of social, cultural, and life-course exposures that are relevant to cognitive health. Considering these factors as multiple dimensions of the immigration experience may help to better understand how immigration experiences are associated with cognitive outcomes in Hispanics.
Therefore, the current study aims to 1) examine the associations between immigration-related factors (nativity, age of migration, time living in the US, primary language, bilingualism, and acculturation levels) and cognitive impairment (MCI or dementia) among Hispanics; 2) examine the associations between immigration-related factors and cognitive performance among cognitively unimpaired Hispanics. We hypothesized that these immigration-related factors would be associated with cognitive outcomes, and that the direction of associations may vary across factors.
Methods
Data Source and Study Population
Data from the Health & Aging Brain Study-Health Disparities (HABS-HD) study, were used.24,25 The HABS-HD study is a multiethnic, longitudinal, and community‐based study examining health disparities in AD. The initial study began in September 2017, focusing on Hispanics and non-Hispanic Whites, and expanded in February 2021 to include non-Hispanic Blacks. Participants were recruited using a community-based participatory research approach (CBPR) through community outreach and media campaigns in Tarrant County, Texas, US, which has the highest Hispanic population density. 26 As such, the study represents a community-based sample rather than a probability-based population cohort. Participants were adults aged ≥50 years who were fluent in English or Spanish. Interviews were conducted in either English or Spanish, based on the participant’s language preference. More details of the study can be found elsewhere. 24 Baseline data on Hispanic participants were used in the current study.
Written informed consent was obtained from all participants (or his/her legal representative).
Study Measures
Demographics
Age in years at baseline was measured. Sex was classified into males and females.
Immigration-Related Factors
Six indicators, including 1) time living in the US, 2) nativity (foreign-born vs native-born), 3) age of migration, 4) primary language, 5) bilingualism, and 6) the Short Acculturation Scale for Hispanics (SASH) language use subscale score, were considered immigration-related factors.
Data on participants’ time (in years) living in the US were collected by asking ‘How long have you lived in the United States?’. For those born in the US, their time living in the country is typically equal to or close to their age. Therefore, time living in the US is influenced by participants’ age and nativity and is of great interest among foreign-born populations.
As data on participants’ nativity were not collected, we defined nativity (foreign-born vs native-born) by comparing their time living in the US with their age. Specifically, if participants’ time living in the US was equal to their age, we classified them as potential native-born populations; if their time living in the US was less than their age, we classified them as potential foreign-born populations. Despite the limitations of this method for determining nativity, it is a reasonable approach for selecting the foreign-born group in cases where data on nativity were not collected.
Age of migration among foreign-born Hispanics was determined by subtracting years living in the US from age at baseline. Additionally, based on previous research, 3 life course stages of migration were defined among foreign-born Hispanics: 1) early-life immigrants (migrated at age 0-19), 2) midlife immigrants (migrated at age 20-49), and 3) late-life immigrants (migrated after age 50).22,27,28 We acknowledge the limitation of this method in identifying age of migration, but the risk of misclassification was likely reduced by categorizing age of migration into 3 life course stages.
Participants were asked, ‘What is your primary language? (English/Spanish/Other).’ We then categorized their responses into two groups: ‘English’ and ‘Spanish or other’. Participants were considered bilingual if they responded ‘yes’ to the question, ‘Do you speak a secondary language? (Yes/No)’, and monolingual if they responded ‘no’.
The SASH is designed to measure the degree of acculturation among Hispanics, with the 5-item SASH Language Use subscale specifically assessing the usage of English compared to Spanish in different contexts. 29 It has been shown that the 5-item SASH Language Use subscale can be a valid and reliable short acculturation scale for use with Hispanics in large studies, as its reliability and validity coefficients are comparable to the full 12-item SASH scale. 29 Items in the Language Use subscale were answered on a 5-point Likert-type scale (Only Spanish = 1 point; Spanish better than English = 2 points; Both equally = 3 points; English better than Spanish = 4 points; Only English = 5 points). The subscale score ranges from 1 to 5, calculated by averaging the scores of the 5 items. A higher value indicates a greater acculturation level to the US culture. 29 The internal reliability of the 5-item SASH Language Use subscale was high in the current study sample (Cronbach’s α = 0.957 among Hispanics; 0.955 among foreign-born Hispanics).
Outcomes
Dementia and MCI
Diagnoses of dementia and MCI were assigned algorithmically and adjudicated by consensus review.30,31 Cognitive diagnoses were determined by self-reported and informant-reported daily functioning, clinician-assigned Clinical Dementia Rating (CDR) sum of boxes scores, and neuropsychological assessment results.
A neuropsychological test battery was used to assess global cognition (Mini-Mental State Examination, MMSE), attention/executive functioning (Wechsler Memory Scale-Third Edition-Digit Span (WMS-III-Digit Span); Trail Making Test Parts A and B), memory (Spanish-English Verbal Learning Test (SEVLT); Wechsler Memory Scale-Third Edition-Logical Memory (WMS-III- Logical Memory)), language (Animal Naming; Verbal fluency (FAS)), and Premorbid IQ (the American National Adult Reading Test (English-speakers) and Word Accentuation Test (Spanish-speakers)). 24 Cognitive tests normative ranges were stratified by education (0-7 years, 8-12 years, and 13+ years), primary language (English or Spanish), and age (≤65 years and >65 years), which were used to calculate Z-scores and for the assignment of cognitive diagnoses. 32 The CDR is used to assess the staging and severity of dementia. The instrument evaluates 6 domains of cognitive and functional performance: 1) memory, 2) orientation, 3) judgment and problem solving, 4) community affairs, 5) home and hobbies, and 6) personal care.33,34 Each domain is scored on a 5-point scale (no impairment = 0 points; questionable impairment = 0.5 points; mild impairment = 1 point; moderate impairment = 2 points; severe impairment = 3 points). The CDR sum of boxes score, ranging from 0 to 18, was calculated by adding up the points from 6 domains.
Dementia was diagnosed if participants with the CDR sum of boxes score ≥2.5, 31 and 2 or more cognitive test scores 2 standard deviations (SDs) below the normative mean for the relevant group on tests (Z-score <-2). MCI was determined if participants with cognitive complaints (self or other), the CDR sum of boxes score of 0.5-2.0, 31 and at least 1 cognitive test 1.5 SDs below the normative mean for the relevant group (Z-score <-1.5). Cognitively unimpaired was defined as participants with no complaints of cognitive change (self or informant), CDR sum of boxes score = 0, and cognitive test scores broadly within normal limits (Z-score >-1.5). Notably, if an individual had an isolated poor performance on 1 neuropsychological test, without any functional decline or cognitive complaints, they were also classified as cognitively unimpaired.
In addition to the three-category outcome (dementia, MCI, and cognitively unimpaired), we also defined a binary outcome, combining dementia and MCI into a single ‘cognitively impaired’ (or ‘cognitive impairment’) category. Both the three-category and binary outcomes were used for analyses. The three-category outcome provided more detailed information by differentiating between dementia and MCI, whereas the binary outcome increased the sample size of the events, increasing statistical power and simplifying the statistical models.
Cognitive Performance
Global cognitive performance was evaluated by the Mini-Mental State Examination (MMSE), which includes 11 questions among 4 domains: 1) orientation, 2) registration and recall (memory), 3) attention and calculation, and 4) language. 35 The total MMSE score ranges from 0 to 30, with a lower score indicating lower global cognitive function. 35 The internal reliability of the MMSE was acceptable in the current study sample (Cronbach’s α = 0.763). The continuous MMSE score was used as the outcome instead of categorizing it based on cutoffs, considering inconsistent cutoffs recommended for different populations. Specifically, using the continuous MMSE score helps avoid misclassification associated with applying fixed cutoffs across diverse groups. MMSE was used to measure global cognitive performance among cognitively unimpaired Hispanic participants as a standardized and widely used summary measure of overall cognitive function, complementing the domain-specific neuropsychological tests.
Statistical Analysis
Demographic characteristics among participants at baseline are presented as means ± standard deviations (SDs) or numbers (percentages). Univariate linear regression, logistic regression, or multinomial logistic regression models were used to assess differences by nativity status.
To examine the associations between immigration-related factors and cognitive impairment (binary outcome: cognitively impaired vs cognitively unimpaired), multiple logistic regression analyses adjusted for age (years), sex, and education (years) were conducted among the Hispanic participants and stratified by nativity. Additionally, the associations between immigration-related factors and the three-category outcome (dementia, MCI, and cognitively unimpaired) were assessed using multinomial logistic regression models adjusted for age (years), sex, and education (years). Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. A 95% CI for an OR that does not include 1 indicates a statistically significant association.
Linear regression analyses were performed to examine the associations between immigration-related factors and global cognitive performance among cognitively unimpaired Hispanic participants. The linear regression models were adjusted for age (years), sex, and education (years). Coefficients (βs) along with 95% CIs were reported, and a 95% CI for a β that does not include 0 suggests a statistically significant association.
Due to structural differences (eg, time living in the US and age at migration being applicable only to foreign-born individuals) and potential correlations among immigration-related variables, these factors were examined in separate models to avoid multicollinearity and ensure interpretability. Further, associations between time living in the US and cognition were analyzed by stratifying participants by age at migration. Multicollinearity in regressions was evaluated by tolerance and variance inflation factor (VIF). A tolerance value below 0.2 or a VIF value exceeding 5 or 10 is typically indicating high multicollinearity. All tolerance values were above the cutoff of 0.2, and VIF values were below the threshold of 5 in the analyses, suggesting no evidence of multicollinearity. Data analyses were conducted using SAS, version 9.4 (SAS Institute, Cary, North Carolina). Two-sided P values <0.05 were considered statistical significance. Cronbach’s α was calculated using SPSS version 29.0.2.0.
Results
The sample selection is shown in Figure S1. A total of 1231 Hispanic participants were included in the analyses, including 874 cognitively unimpaired Hispanic participants.
Characteristics of the Overall Hispanic Participants
Characteristics of the Overall Hispanic Participants by Nativity
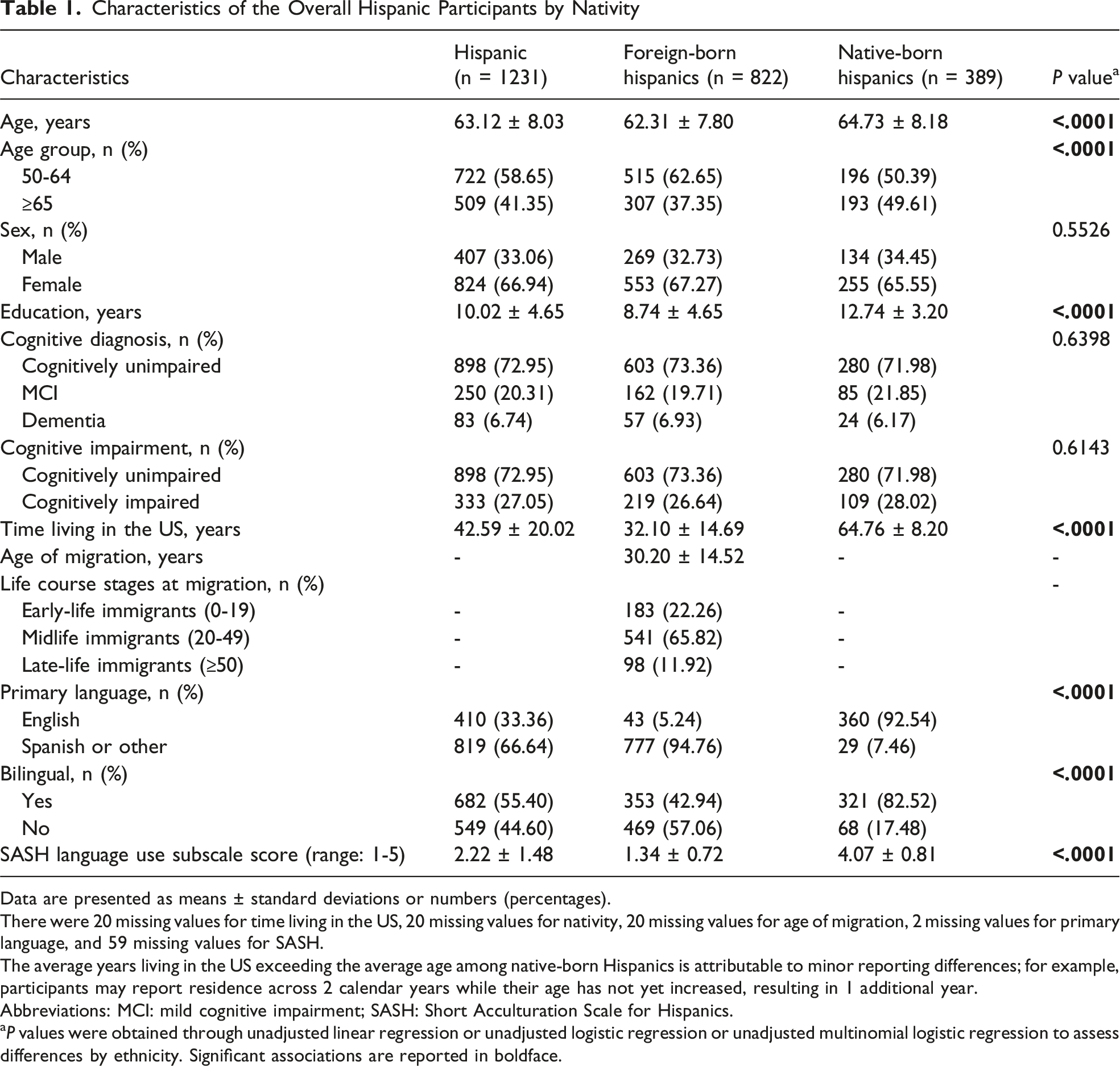
Data are presented as means ± standard deviations or numbers (percentages).
There were 20 missing values for time living in the US, 20 missing values for nativity, 20 missing values for age of migration, 2 missing values for primary language, and 59 missing values for SASH.
The average years living in the US exceeding the average age among native-born Hispanics is attributable to minor reporting differences; for example, participants may report residence across 2 calendar years while their age has not yet increased, resulting in 1 additional year.
Abbreviations: MCI: mild cognitive impairment; SASH: Short Acculturation Scale for Hispanics.
aP values were obtained through unadjusted linear regression or unadjusted logistic regression or unadjusted multinomial logistic regression to assess differences by ethnicity. Significant associations are reported in boldface.
Associations Between Immigration-Related Factors and Cognitive Impairment
Associations Between Immigration-Related Factors and Cognitive Impairment
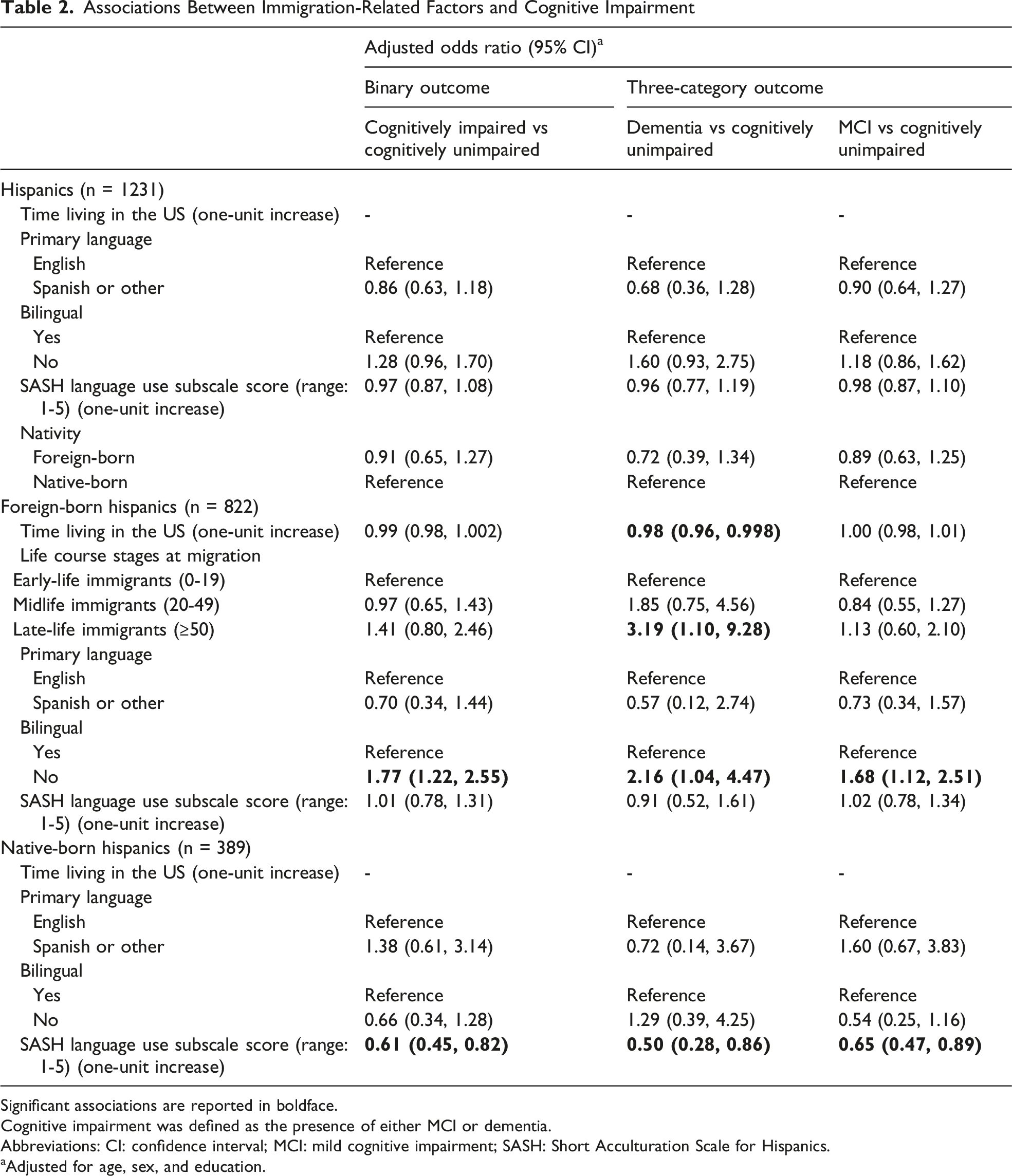
Significant associations are reported in boldface.
Cognitive impairment was defined as the presence of either MCI or dementia.
Abbreviations: CI: confidence interval; MCI: mild cognitive impairment; SASH: Short Acculturation Scale for Hispanics.
aAdjusted for age, sex, and education.
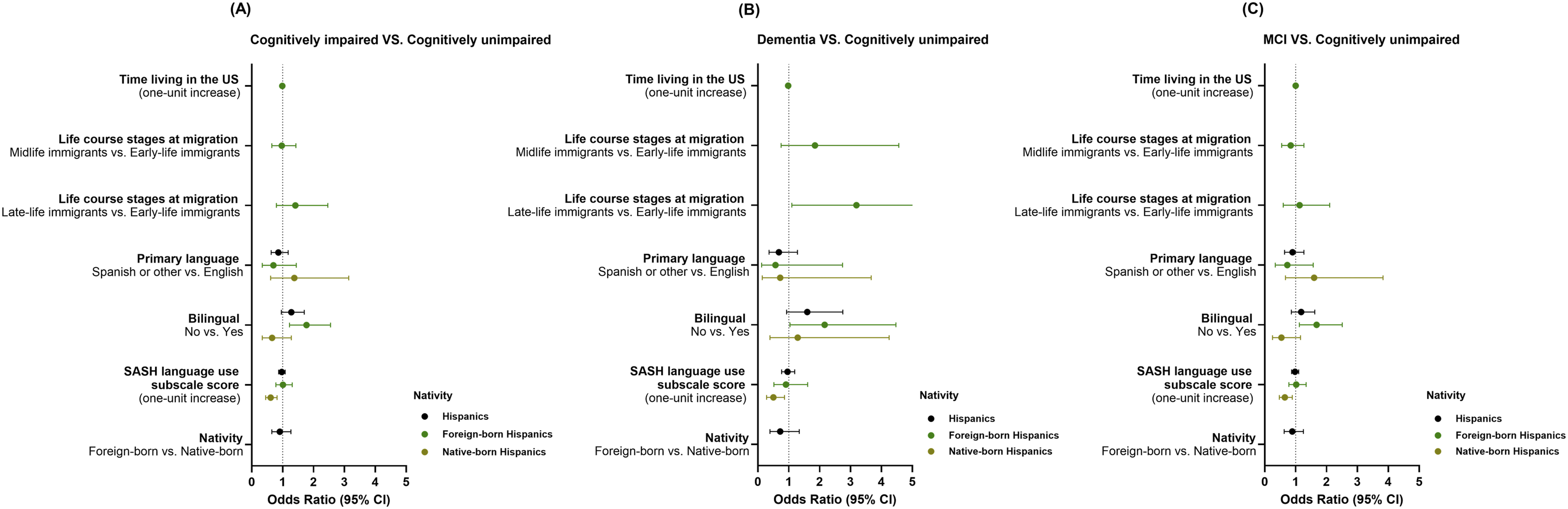
Adjusted odds ratios and 95 % CIs for cognitive impairment, dementia, and MCI by immigration-related factors and nativity
Among foreign-born Hispanics, each additional year living in the US was associated with a 2% reduction in the odds of dementia (adjusted OR = 0.98, 95% CI: 0.96, 0.998) (Table 2 and Figure 1). Compared to early-life immigrants, late-life immigrants had significant higher odds of dementia (adjusted OR = 3.19, 95% CI: 1.10, 9.28), while midlife immigrants did not differ significantly from early-life immigrants (adjusted OR = 1.85, 95% CI: 0.75, 4.56) (Table 2 and Figure 1). When stratifying the analysis of the association between time living in the US and cognitive impairment, a significant association between longer time living in the US and higher odds of dementia was observed in early-life immigrants (adjusted OR = 1.19, 95% CI: 1.01, 1.41) (Table S1 and Figure S2).
Characteristics of Cognitively Unimpaired Hispanic Participants
Characteristics of cognitively unimpaired Hispanic participants by nativity are presented in Table S2. The average time living in the US among foreign-born Hispanics who were cognitively unimpaired was 32.23 years, significantly shorter than that of native-born cognitively unimpaired Hispanics (mean: 63.97 years) (P value <0.0001) (Table S2). Additionally, 23.08% of foreign-born cognitively unimpaired Hispanic participants were early-life immigrants (migrated before age 20), 66.32% were midlife immigrants (migrated between age 20-49), and 10.60% were late-life immigrants (migrated at or after age 50) (Table S2). 5.31% of foreign-born Hispanics reported English as their primary language, while the proportion was 93.43% native-born Hispanics (P value <0.0001) (Table S2). In addition, a lower proportion of bilingual individuals was observed in the foreign-born subsample (47.35%) compared to those who were native-born (81.02%) (P value <0.0001) (Table S2). Moreover, native-born Hispanics who were cognitively unimpaired had a greater level of acculturation (ie, greater English language use preference) than Hispanics who were foreign-born (P value <0.0001) (Table S2).
Associations Between Immigration-Related Factors and Cognitive Performance Among Cognitively Unimpaired Participants
Associations Between Immigration-Related Factors and Cognitive Performance Among Cognitively Unimpaired Hispanics
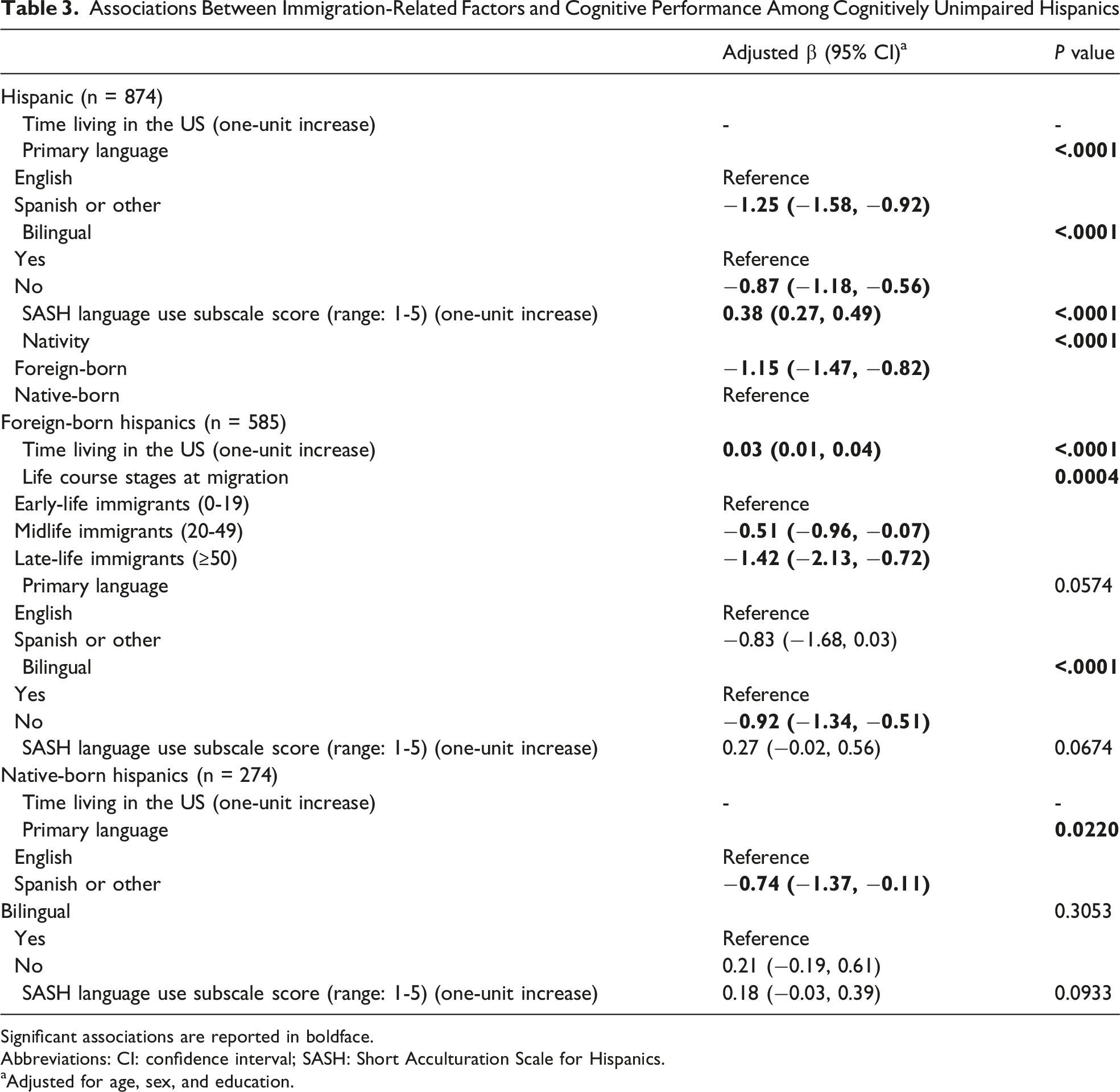
Significant associations are reported in boldface.
Abbreviations: CI: confidence interval; SASH: Short Acculturation Scale for Hispanics.
aAdjusted for age, sex, and education.
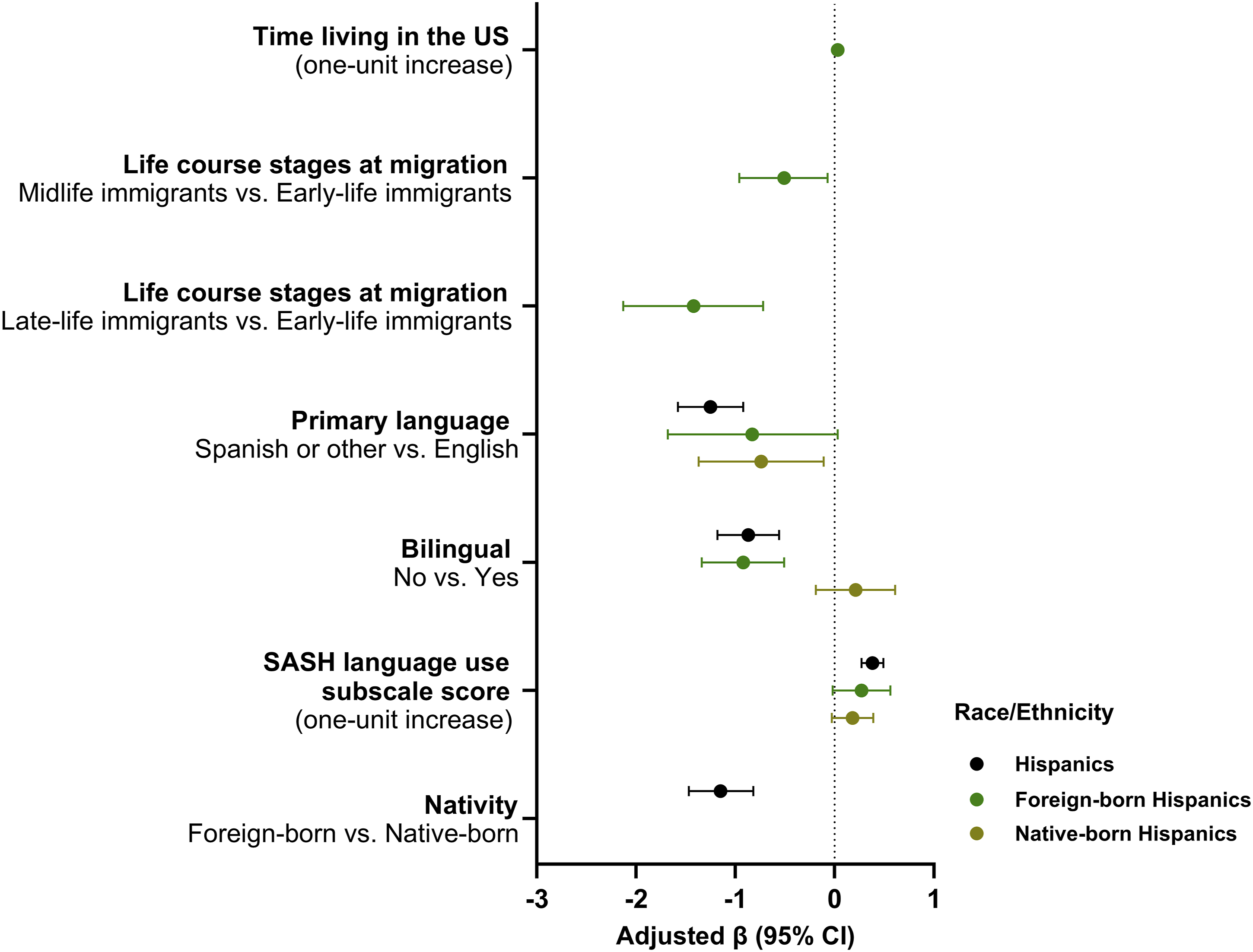
Adjusted Coefficients (βs) and 95 % CIs for global cognition (MMSE) among cognitively unimpaired Hispanics participants by immigration-related factors and nativity. Models were adjusted for age, sex, and education. Values outside the range of the x-axis were not shown. Abbreviations: CI: confidence interval; MMSE: Mini-Mental State Examination
Among foreign-born cognitively unimpaired Hispanics, each additional year living in the US was associated with a 0.03-point increase in MMSE score (adjusted β = 0.03, 95% CI: 0.01, 0.04) (Table 3 and Figure 2). Compared to early-life immigrants, late-life immigrants were associated with a 1.42-point decrease in MMSE score (adjusted β = −1.42, 95% CI: −2.13, −0.72), while midlife immigrants were associated with a 0.51-point decrease in MMSE score (adjusted β = −0.51, 95% CI: −0.96, −0.07) (Table 3 and Figure 2). In the stratified analyses, no significant associations were found between time living in the US and global cognitive performance (P values >0.05) (Table S3 and Figure S3).
Discussion
We found that bilingualism was significantly associated with dementia and MCI in foreign-born Hispanics, and with global cognitive performance in foreign-born cognitively unimpaired Hispanics. Whereas the associations were insignificant in native-born Hispanics. The associations of acculturation with dementia and MCI were observed in native-born Hispanics, but not in foreign-born Hispanics. Moreover, we found that longer time living in the US was associated with lower odds of dementia among foreign-born Hispanics, and longer time living in the US was associated with higher global cognitive performance among foreign-born cognitively unimpaired Hispanics. However, the associations between time living in the US and cognition were no longer significant when stratified by age at migration, except for the association with dementia among early-life immigrants. Further, the results showed that late-life immigrants had significant higher odds of dementia than early-life immigrants, and both cognitively unimpaired midlife and late-life immigrants had significant worse global cognitive performance than cognitively unimpaired early-life immigrants.
In the present study, no significant association was found between nativity and cognitive impairment. In contrast, Moon et al reported a higher prevalence of dementia among Hispanic immigrants enrolled in Medicare compared to US-born Hispanic Medicare beneficiaries. 12 However, Moon’s study focused on Medicare beneficiaries, and immigrants who were not eligible for Medicare were not included. This may partially explain differences in research findings. Whereas using the HRS data, Weden et al found that foreign-born Mexican Americans had a lower hazard of incident cognitive impairment than US-born non-Hispanic Whites during 2000-2010, while US-born Mexican Americans had a higher hazard of incident cognitive impairment than US-born non-Hispanic Whites. 36 Using the HRS data, Garcia and colleagues found that older US-born Hispanics had poorer cognitive function than older US-born non-Hispanic Whites and foreign-born Hispanics. 37 They concluded that US-born Hispanics are likely more vulnerable to cognitive impairment than foreign-born Hispanics. 37 One major explanation for their finding is that foreign-born Hispanic males may be more positively selected for health with respect to cognitive functioning (positive health selection). 37 Additionally, Garcia and colleagues found that foreign-born Mexican immigrants have a longer total life expectancy than US-born Mexican Americans, but the foreign-born Mexican immigrants spend more years living with cognitive impairment after age 65 compare to their US-born counterparts, indicating a greater need for support and time-intensive care in late life among foreign-born Mexican immigrants. 27 However, the results of the current study did not support their findings. It is also possible that the effect of nativity on cognitive impairment was not detected in the current study due to the categorical outcome’s inability to capture cognitive differences before the onset of cognitive impairment. Our finding that foreign-born status was associated with lower MMSE scores compared to native-born status among cognitively unimpaired Hispanics supports this assumption. In our study, models were adjusted for age, sex, and education, and language-appropriate cognitive tests were administered, suggesting that factors beyond educational attainment and test language may contribute to these disparities. One possible explanation is that immigrants may have lower health literacy than native-born individuals, 38 which may hinder health-promoting behaviors to improve cognition. It is also possible that foreign-born participants might have difficulty understanding cognitive tests and limited verbal comprehension, 11 which could lead to lower cognitive scores. Future research on nativity and cognition is needed to provide further evidence.
Importantly, it was found that each additional year living in the US was associated with a 2% reduction in the odds of dementia in foreign-born Hispanics, and each additional year of living in the US was associated with a 0.03-point increase in MMSE score among foreign-born cognitively unimpaired Hispanics. Whereas prior studies suggest that immigrants are initially healthier than native-born individuals upon arrival (healthy immigrant effect), their health advantage tends to wane over time with longer residence in the US.19,20 The erosion of health advantages over time among immigrants might be due to acculturative stress, exposure to hazardous environments, and unhealthy assimilation. 23 In the present study, when stratifying by age of migration, a significant association between time living in the US and dementia was observed only among early-life immigrants. This may suggest that age of migration plays a more important role than duration of residence in the US in relation to cognitive outcomes in foreign-born Hispanics. Hill et al found that Mexican midlife immigrants have higher levels of baseline cognitive functioning than their US-born counterparts. 23 Although both women and men who migrated in midlife show this advantage, immigrant men tend to maintain the advantage for a longer period of time, indicating the contribution of sex in the associations. 23 Additionally, Garcia and colleagues reported that Mexican late-life immigrant women had a higher risk of cognitive impairment than US-born Mexican American women, while Mexican midlife immigrant men had a lower risk than their US-born counterparts. 28 Similarly, Downer et al found that, after adjusting for education, Mexican late-life migrant women had a higher risk of cognitive impairment than US-born women, whereas the risk among Mexican late-life migrant men did not differ from that of US-born men. 22 One explanation for those findings is positive health selection, where foreign-born Hispanic men may be more positively selected for cognitive health. 37 In the current study, after adjusting for age, sex, and education, we found that, compared to early-life immigrants, late-life immigrants had significantly higher odds of dementia; and among cognitively unimpaired participants, both late-life and midlife immigrants had lower MMSE scores compared to early-life immigrants. Our findings suggest that, after controlling for age, sex, and education, the timing of migration is associated with cognitive health. The elevated odds of dementia observed among late-life immigrants may be attributable to their migration patterns, as they often relocate with family members and are less likely to experience the positive health selection commonly observed among midlife immigrant men. The poorer global cognitive performance in cognitively unimpaired late-life and midlife immigrants compared to early-life immigrants might be related to language barriers and lower acculturation levels in the US. These findings suggest that age at migration reflects distinct subgroups within the sample, with early-, mid-, and late-life immigrants differing in levels of acculturation, language use, healthcare access, and health selection. In addition, other life-course factors, such as occupational pathways, socioeconomic mobility, and cumulative stress exposure, may also differ by age at migration and contribute to variation in cognitive aging trajectories. As a result, comparisons across age-of-migration groups should be interpreted with consideration of these underlying differences. Future research should incorporate more detailed measures of migration history and experiences to examine how these factors interactively shape cognitive outcomes across the life course.
Prior studies suggested that a higher acculturation level is associated with better cognitive performance,16,17,39,40 while acculturative stress may be negatively related to cognitive performance among Hispanics. 18 In the current study, the association between acculturation and cognitive impairment was not found among foreign-born Hispanics. The insignificant associations among foreign-born Hispanics might be due to acculturative stress counteracting the potential benefits of higher acculturation. However, this assumption needs to be tested in future research. Additionally, a higher acculturation level was found to be associated with a lower likelihood of both dementia and MCI among native-born Hispanics in the present study. Despite being born in the US, native-born Hispanics may have varying levels of integration into mainstream US culture. 41 A higher level of acculturation may protect cognition by contributing to greater levels of some protective factors, such as physical activity and healthcare utilization.42,43 More research is needed to support this assumption. Moreover, acculturation was significantly associated with global cognitive performance in overall cognitively unimpaired Hispanic participants, while the association with acculturation level was no longer significant when stratified by nativity. Studies with larger sample sizes of cognitively unimpaired Hispanic participants are needed to further investigate whether the associations with acculturation differ by nativity. Of note, in the current study, language acculturation measured by the SASH Language Use subscale, rather than overall acculturation, was assessed. Despite the reliability and validity coefficients of the 5-item SASH Language Use subscale being comparable to those of the full 12-item SASH scale, 29 the language use subscale may not adequately capture acculturation in other domains such as media use and social integration. Hence, more comprehensive acculturation assessments are needed in future research.
It is critical to understand that language acculturation, primary language, and bilingualism assess different aspects of language use and its influence among Hispanics. In the current study, language acculturation assessed the preference for using English compared to Spanish in various contexts; primary language referred to the main language spoken; and bilingualism focused on proficiency in 2 languages without specifying preference or dominance. No significant associations between cognitive impairment and primary language were found among Hispanic participants or by nativity in the present study. While a significant association between primary language and global cognitive performance was observed among cognitively unimpaired overall Hispanic participants and native-born Hispanic participants. However, unlike the results for primary language, monolingual foreign-born Hispanics had significantly higher odds of having both dementia and MCI, while bilingualism was not significantly associated with dementia or MCI among native-born Hispanics. It is likely that bilingual foreign-born Hispanics are primarily Spanish speakers (94.76% primarily speak Spanish or another non-English language in the current study), and a certain level of English proficiency (42.94% were bilingual in the current study) may help them adapt to life in the US and have greater access to health care.44,45 In contrast, native-born Hispanic participants in the current study were primarily English speakers (92.54% primarily speak English), and 82.52% are bilingual. As native-born Hispanic participants were primarily English speakers, acquiring another language may have a limited effect on their adaptation to life in the US. Prior studies have shown that bilingualism may contribute to better cognitive reserve;46-48 however, this effect did not translate into measurable cognitive differences in the current study. This discrepancy may be explained by the heterogeneous nature of bilingualism, as its cognitive effects may vary according to language dominance, frequency of use, and switching demands.46,49 Cognitive benefits from bilingualism may arise from sustained engagement in language control processes,46,47,49 which may be more pronounced among foreign-born Hispanics adapting to a new linguistic environment. In contrast, US-born bilingual Hispanics may be more likely to be English-dominant, with less frequent or less cognitively demanding use of a second language. Although language acculturation and primary language were assessed, these measures may not fully capture key aspects of bilingual experience, such as frequency of use or switching patterns. Similar results were found among cognitively unimpaired Hispanics. Monolingual foreign-born cognitively unimpaired Hispanics had significantly lower MMSE scores, but no significant associations were found among native-born cognitively unimpaired Hispanics after controlling for age, sex, and education. Likewise, this result can be explained by the fact that foreign-born Hispanics are primarily Spanish speakers, and bilingualism in the context of the US for individuals who immigrate usually implies the acquisition of English, which may help them adapt to the US society; while native-born Hispanics were primarily English speakers, and bilingualism may not help their adaptation to life in the US. Our finding can be supported by the study by Downer et al, which found that a higher frequency of English use among non-native speakers was associated with higher MMSE scores. 50 Further, according to Linton and Jiménez, bilingualism in US-born Hispanics is closely tied to ethnic and culture identity. 51 It is possible that bilingualism may not play the same adaptive role for US-born Hispanics as it might for immigrants.
The present study has multiple strengths. The study adds to the limited literature on the associations between immigration-related factors and cognition. Additionally, the full spectrum of cognition, including dementia, MCI, and cognitive performance among cognitively unimpaired participants, was investigated. Lastly, the dataset included comprehensive variables, allowing for the capture of various immigration-related factors. The study also has limitations. First, the cross-sectional analyses limit the ability to draw causal inferences. Hence, longitudinal analyses are needed to further examine causation. Second, nativity was not directly collected in the study but instead identified by comparing time living in the US with age, which may lead to misclassification. If feasible, data on nativity should be collected in future cognitive research, especially among diverse racial/ethnic populations. Third, subgroup analyses (eg, Spanish primary, foreign-born Hispanics) were not conducted due to small comparison group sizes and may be explored in future research. Finally, the study is limited to the US population, therefore, the findings cannot be generalized to other populations in other countries or regions. In addition, the non-probability sampling and the higher proportion of foreign-born Hispanics relative to national estimates may limit the representativeness of the sample, and the findings should be interpreted accordingly. More research on other populations is crucial to further understanding the role of immigration-related factors and cognitive health.
Conclusions
The present study contributes to the growing literature on the associations between immigration-related factors and cognition. We found the likelihood of cognitive impairment did not differ significantly between native-born and foreign-born Hispanics, whereas foreign-born cognitively unimpaired Hispanics had significantly lower global cognition than their native-born counterparts. Foreign-born Hispanics might be more vulnerable to cognitive aging. Bilingualism may play a more important role in cognitive health in foreign-born Hispanics than in native-born Hispanics. Acculturation may have distinct effects on foreign-born and native-born Hispanics. Tailored interventions are needed in Hispanics by nativity.
Supplemental Material
Supplemental Material - Associations Between Immigration-Related Factors and Cognition Among Hispanics, the HABS-HD Study
Supplemental Material for Associations Between Immigration-Related Factors and Cognition Among Hispanics, the HABS-HD Study by Shanshan Wang, Uyen-Sa Nguyen, Zhengyang Zhou, Stephanie Grasso, Sid E. O’Bryant, Kristine Yaffe, Leigh Johnson and Rajesh R Nandy in Journal of Geriatric Psychiatry and Neurology
Footnotes
Acknowledgment
Research reported on this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R01AG054073, R01AG058533, R01AG070862, P41EB015922 and U19AG078109. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Health and Aging Brain Study (HABS-HD) Study Team: HABS-HD MPIs: Sid E O’Bryant, Kristine Yaffe, Arthur Toga, Robert Rissman, & Leigh Johnson; and the HABS-HD Investigators: Meredith Braskie, Kevin King, James R Hall, Melissa Petersen, Raymond Palmer, Robert Barber, Yonggang Shi, Fan Zhang, Rajesh Nandy, Roderick McColl, David Mason, Bradley Christian, Nicole Phillips, Stephanie Large, Joe Lee, Badri Vardarajan, Monica Rivera Mindt, Amrita Cheema, Lisa Barnes, Mark Mapstone, Annie Cohen, Amy Kind, Ozioma Okonkwo, Raul Vintimilla, Zhengyang Zhou, Michael Donohue, Rema Raman, Matthew Borzage, Michelle Mielke, Beau Ances, Ganesh Babulal, Jorge Llibre-Guerra, Carl Hill and Rocky Vig.
Ethical Considerations
The HABS-HD study was approved by the University of North Texas Health Science Center Institutional Review Board (IRB).
Consent to Participate
Written informed consent was obtained from all participants (or his/her legal representative).
Author Contributions
Shanshan Wang, Uyen-Sa Nguyen, Zhengyang Zhou, Stephanie Grasso, Leigh Johnson, and Rajesh R. Nandy conceptualized the research idea and supervised the data analysis. Shanshan Wang performed the statistical analyses, created the visualizations, and wrote the original draft. Sid E. O’Bryant, Kristine Yaffe, and Leigh Johnson acquired funding, supervised and managed the project, and collected and maintained the research data. Shanshan Wang, Uyen-Sa Nguyen, Zhengyang Zhou, Stephanie Grasso, Sid E. O’Bryant, Kristine Yaffe, Leigh Johnson, and Rajesh R. Nandy reviewed, revised, and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging of the National Institutes of Health (R01AG054073, R01AG058533, R01AG070862, P41EB015922 and U19AG078109).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Investigators may request access to anonymized individual data at the HABS-HD study website (![]() ). Prior to use the data, proposals need to be approved by an independent review panel at https://apps.unthsc.edu/itr/.
). Prior to use the data, proposals need to be approved by an independent review panel at https://apps.unthsc.edu/itr/.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.