
Abstract
Objective
A mixed methods study was conducted to investigate how clinical neuropsychologists engage with and provide cognitive assessment to persons living with Parkinson’s disease (PD). Current practices were examined to identify service gaps and generate recommendations for future research.
Method
Australian neuropsychologists experienced in PD assessment were recruited to complete an online survey (N = 20) and semi-structured interviews (N = 5). Quantitative data was summarised descriptively. Qualitative data underwent coding reliability thematic analysis. Findings were combined through mixed methods integration to identify service gaps.
Results
Integration revealed four service gaps for neuropsychologists when assessing persons living with PD. These were: (1) varied assessment practices across neuropsychologists; (2) infrequent engagement of neuropsychologists; (3) suboptimal test availability for PD assessment; and (4) limited integration of digital modalities within practice.
Conclusions
The findings provide preliminary observation into service gaps for neuropsychologists in PD assessment to help direct future research.
Introduction
Parkinson’s disease (PD) is a prevalent and rapidly growing neurological disorder with poor cognitive outcomes. 1 Mild cognitive impairment due to PD (PD-MCI) occurs in one-fifth of persons at diagnosis, 2 with four-fifths developing PD dementia (PDD) by late disease stage. 3 Cognitive abilities observed in persons living with PD can be highly heterogeneous. 4 This is in part due to disease complexity, 5 but also inconsistent methods to determine and diagnose cognitive impairment. 6 Such inconsistencies are thought to contribute to failures in identifying cognitive disorders effectively in persons living with PD, which in turn can preclude early care planning and intervention. 7
Neuropsychological testing is a common method used in clinical settings to determine cognitive disorders due to PD. 8 Both PD-MCI and PDD can be diagnosed with a brief cognitive screen, administered by any clinician with appropriate training. Although for greater diagnostic certainty, a comprehensive cognitive assessment must be conducted and interpreted by a clinical neuropsychologist.8,9
Recent efforts have occurred to standardise neuropsychology practices for specialised memory clinics in Australia.10,11 However, this work does not account for persons living with PD, who are primarily cared for by movement disorder clinics where cognition is not the main focus. 12 Parkinson’s disease is the second most common neurological disorder in Australia with recent estimates predicting prevalence to double between 2020-2050. 13 More work is therefore required to understand and optimise Australian neuropsychology services for persons living with PD to accommodate a growing demand for care. To this end, a mixed methods study was conducted to investigate how neuropsychologists engage with and provide cognitive assessment in persons living with PD. Neuropsychologist practices in Australia were examined to identify service gaps when assessing persons living with PD and generate recommendations for future research. The study was conducted as part of the PDCogniCare project, which aims to enhance clinical assessment and diagnosis of cognitive impairment and dementia in PD.14,15
Methods
Study Design
The study followed a convergent mixed methods research design.
16
Use of mixed methods enabled: (1) exploration into the contextual factors influencing neuropsychologists’ engagement and practice; and (2) substantiation of identified service gaps through multiple data sources. Data collection and analysis occurred separately over quantitative and qualitative strands. Following analysis, findings from both strands were integrated together to determine service gaps and develop recommendations. A schematic of the study design is provided in Figure 1. Study design flowchart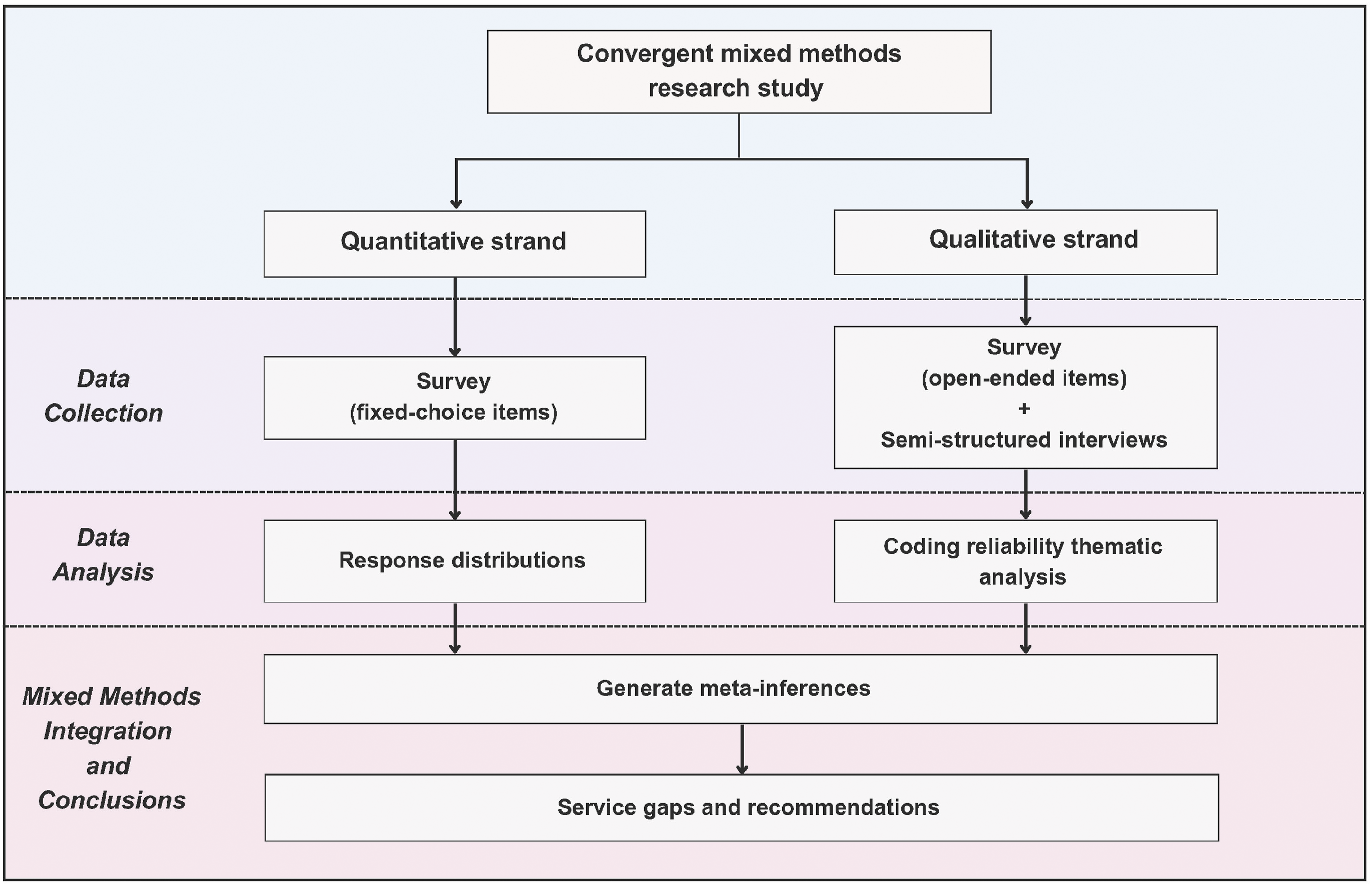
Participants
A purposive sample of clinical neuropsychologists in Australia, with experience conducting assessment in persons living with PD, were invited to participate. Snowball sampling was used to aid survey recruitment within this specialised field, 17 contacting Australian neuropsychology professional networks (eg, ADNeT, NPinOZ) and neuropsychologists affiliated with the PDCogniCare project. Moreover, recruitment for semi-structured interviews followed convivence-based sampling, inviting all neuropsychologists from PD services across two major healthcare departments in Queensland, Australia. No authors took part as study participants to minimise potential sample bias. Informed written consent was collected from all neuropsychologists prior to participation. Study activities were conducted in accordance with approved ethics obtained from the University of Queensland, Metro North Health Service, and Metro South Health Service Ethics Committees HREC/2023/MNHA/100098.
Survey Design and Procedure
Survey design was adapted from the Australia Dementia Network national memory clinic survey. 18 The survey collected demographic information on neuropsychologists’ clinic setting, location, and years of experience. It also collected information on several features of neuropsychological assessment specific to persons living with PD. Features included impairment and diagnostic criteria, use of guidelines and resources, referral questions, repeat assessments, use of digital modalities, and common challenges. Neuropsychological tests used to measure cognition, neuropsychiatric symptoms and premorbid functioning were also examined. Online development and distribution of the survey was facilitated by REDCap. A full copy of the survey is provided in Supplemental material S1.
Interview Design and Procedure
Two researchers (JY and LKM), with qualitative data collection experience, conducted the semi-structured interviews. An interview guide was used to aid discussion, including topics on current engagement, usual practice, and main needs for neuropsychologists when assessing persons living with PD. All interviews were completed over Zoom, with an average interview time of 43 minutes. All interviews were video recorded and transcribed professionally for later analysis. A summarised copy of the interview guide is provided in Supplemental material S2.
Data Analysis
Quantitative
Participant demographics were summarised using descriptive statistics. Response distributions of fixed-choice survey items were calculated and summarised to determine the most common practices conducted by neuropsychologists. All analyses were run in R software v4.4.1.
Qualitative
Thematic analysis was conducted to systematically understand the neuropsychologists’ experiences and thoughts on PD assessment described in semi-structured interviews and open-ended survey items. 19 A post-positivist theoretical stance was adopted alongside thematic analysis to acknowledge that perspectives on complex healthcare phenomena are inherently shaped by contextual and experiential influences. 20 Coding reliability analysis was conducted as a method of thematic analysis which aligned with this position. 21
First, data familiarisation occurred to develop themes inductively from the data corpus. Developed themes were than refined and formalised into a codebook (Supplemental table S1). Two independent coders (JMK and RG) than applied the codebook to guide data extraction into the developed themes. All data was coded in NVivo software v14.0. Coding discrepancies were discussed between the coders to reach consensus before final interpretation. Cohen’s Kappa coefficient 22 was calculated to assess reliability between the coders. Interpretations of intercoder agreement followed Fleiss’ kappa guidelines. 23
Mixed Methods Integration
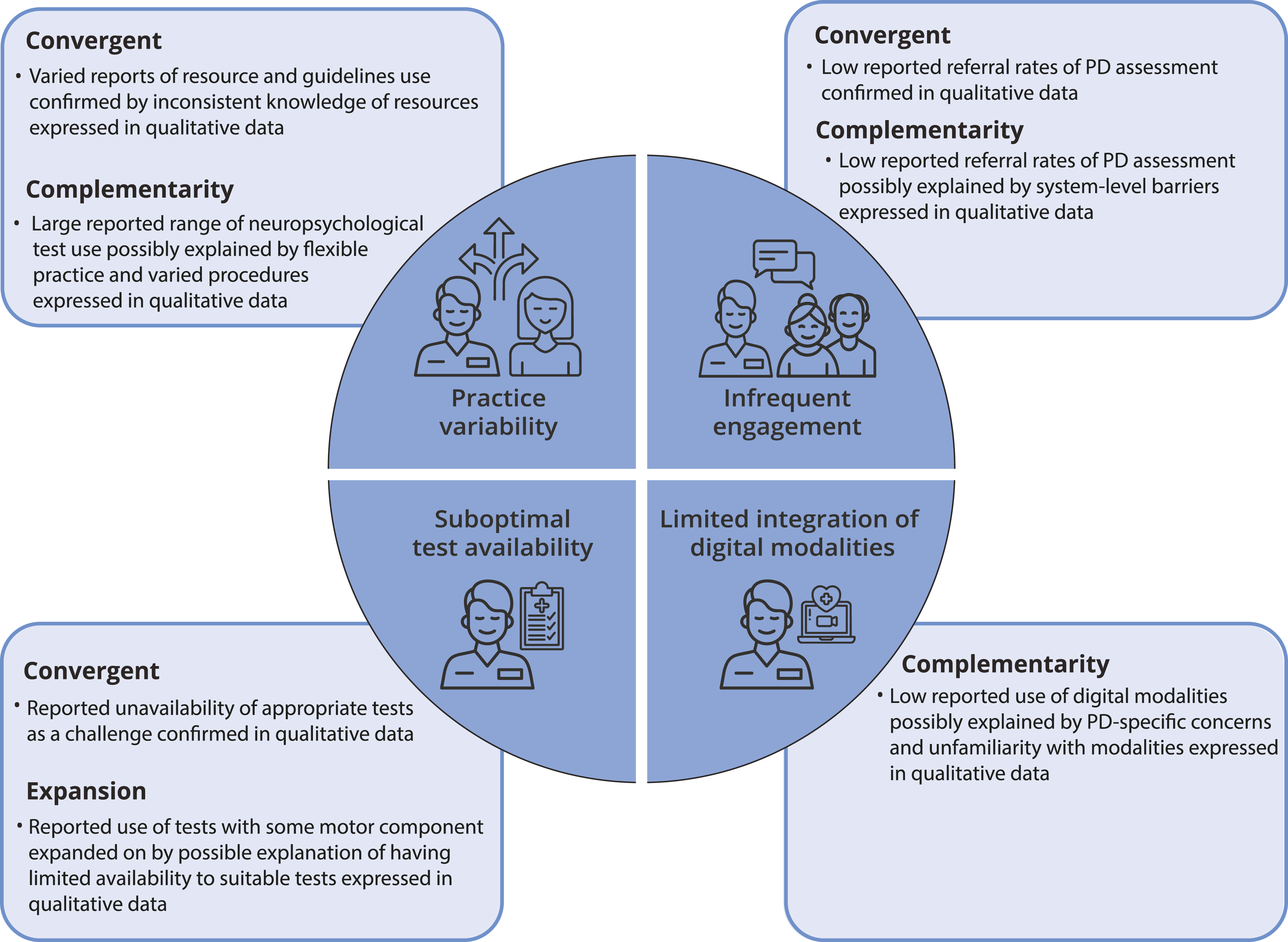
Quantitative and qualitative strand findings were integrated together to critically interpret data patterns and identify service gaps for neuropsychologists. Links between the mixed methods findings were explained using four meta-inference types. 24 These included: (1) confirmation (findings from both strands confirmed one another); (2) complementarity (findings from both strands differed but did not contradict one another); (3) expansion (findings from both strands overlapped, but room remained for further interpretation); and (4) discordance (findings from both strands conflicted with one another). To ease interpretation, a joint display was created to present the integrated mixed methods findings per service gap.
Results
Participant Characteristics
Participant Characteristics
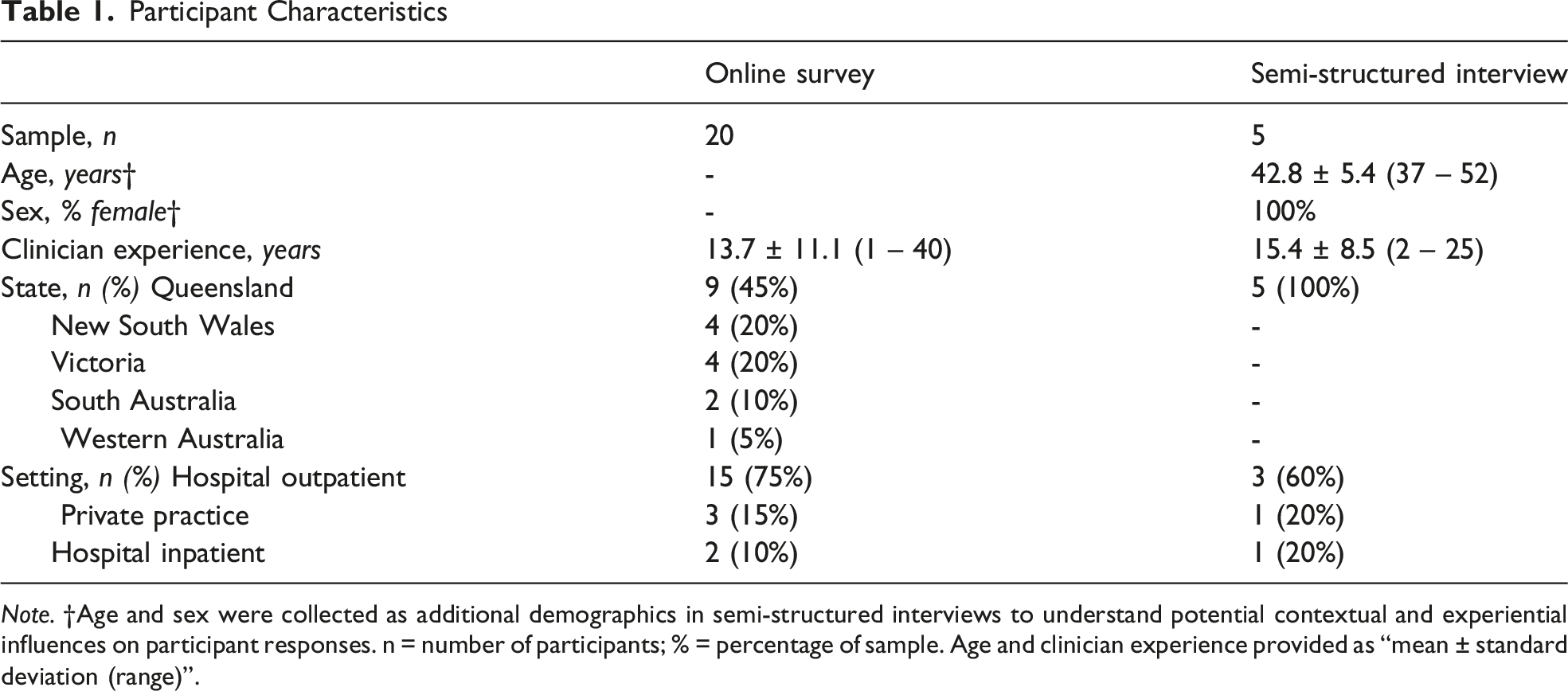
Note. †Age and sex were collected as additional demographics in semi-structured interviews to understand potential contextual and experiential influences on participant responses. n = number of participants; % = percentage of sample. Age and clinician experience provided as “mean ± standard deviation (range)”.
Quantitative Findings
Neuropsychology Practice
Referral Question and Frequency
Neuropsychologists’ assessment in persons living with PD was primarily referred for Deep Brain Stimulation (DBS) surgery (55%). General enquiries into PD-MCI (20%), PDD (10%), differential diagnosis (10%), and cognitive profiling for support planning (5%) were other reasons reported for primary referral. Interestingly, PD referrals were less than half of caseload assessments for almost all neuropsychologists (95%), and less than ten percent in over one-third (35%).
Resources and Guideline Use
Neuropsychologists’ use of resources and guidelines to plan assessment in persons living with PD varied. Most reported to rely on clinical judgement only (60%). Otherwise, neuropsychologists reported to use internally developed hospital batteries (30%), Goldman, Holden, Ouyang, Bernard, Goetz and Stebbins 25 paper (5%), and the Movement Disorder Society (MDS) task force guidelines (5%)
Criteria
To diagnose PD-MCI, most neuropsychologists reported using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) criteria for mild neurocognitive disorder due to PD (75%). 26 Other neuropsychologists reported using the MDS level II criteria for PD-MCI (25%), 8 with none using MDS level I criteria. To diagnose PDD, most neuropsychologists reported using the DSM-5-TR criteria for major neurocognitive disorder due to PD (81%). Other PDD diagnostic criteria included clinician judgement (13%), and MDS task force criteria (6%).
To determine cognitive impairment, most neuropsychologists reported primary criteria as interpreting performance relative to individualised estimates of premorbid functioning (56%). Other criteria included interpreting performance relative to cohort-matched normative scores (25%), profile analysis (13%), and performance relative to previous assessment (6%). Of note, almost all neuropsychologists reported to use more than 1 of these criteria often in practice (94%).
Repeat Assessment
Neuropsychologists undertaking repeat assessment in persons living with PD was uncommon. Most reported to undertake repeat assessment with a quarter or less of their PD cliental (70%), with only a small proportion assessing on most occasions (20%). Of the neuropsychologists who undertook repeat assessment in some capacity (N = 14), almost all conducted no more than 1 per client typically (93%). Reported time length between repeat assessments varied, including 6 months (7%), 12 months (64%), 18 months (14%), and 24 months (14%). To identify performance change over repeat assessment, neuropsychologists primarily used a standard deviation score greater than 1 between assessments (57%). Reliable change indices (36%), and standardised regression-based methodology (7%) were also reported.
Digital Modalities
Neuropsychologists reported to rarely use digital modalities in assessment with persons living with PD. Telehealth was used by a minority of neuropsychologists (19%), all in less than ten percent of their assessments with PD cliental. Use of specialty computerised testing batteries in assessment was reported by one neuropsychologist.
Practice Considerations and Challenges
When considering responsiveness to anti-parkinsonian medication, most neuropsychologists reported assessing persons in the ‘On’ state, when anti-parkinsonian medication is most effective (59%). Other neuropsychologists reported conducting assessment in either ‘On/Off’ state, or do not consider responsiveness to anti-parkinsonian medication (29%). One neuropsychologist reported to assess cognition in the ‘On’ state for DBS surgery referrals, and the ‘Off’ state for diagnostic enquires. Motor symptoms interfering with assessment tasks (60%) was the most reported challenge by neuropsychologists for cognitive assessment in persons living with PD. Other challenges included limited time for assessments (26%), unavailability of appropriate tests (16%), clients declining to engage (16%), and meeting response deadlines for referrals (11%).
Neuropsychological Tests
Neuropsychologists’ Test Use in Persons Living With Parkinson’s Disease
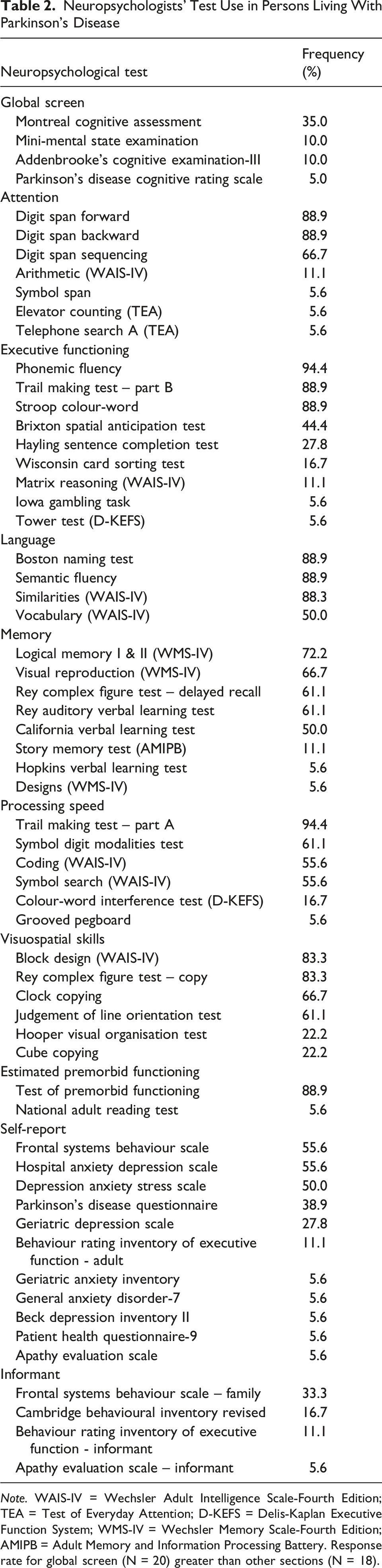
Note. WAIS-IV = Wechsler Adult Intelligence Scale-Fourth Edition; TEA = Test of Everyday Attention; D-KEFS = Delis-Kaplan Executive Function System; WMS-IV = Wechsler Memory Scale-Fourth Edition; AMIPB = Adult Memory and Information Processing Battery. Response rate for global screen (N = 20) greater than other sections (N = 18).
Qualitative Findings
Neuropsychologist responses on semi-structured interviews and open-ended survey items were summarised into four themes. Cohen’s kappa value from the coding reliability thematic analysis was 0.76, indicating very good intercoder agreement.
Theme 1. Application of Resources and Guidelines
Knowledge on the current resources and guidelines to assess persons living with PD was generally inconsistent. Neuropsychologists stated to be most familiar and apply relevant resources when developing their assessment protocols. They also made a note of either rarely revisiting or not returning to the literature following protocol development. One neuropsychologist explained their long period between PD patients as the reason for becoming unfamiliar. Development of specific resources and guidelines to standardise assessment in persons living with PD was endorsed. “Depending on what measures you use, I think it would be great to have a systematic approach to tracking things.” [Interviewee3010]
Theme 2. Experiences of Cognitive Assessment
Referral Infrequency
Neuropsychologists consistently highlighted the infrequency in which they receive assessment referrals for persons living with PD. This was acknowledged in both their current and prior clinical settings. Neuropsychologists explained the low referral numbers are particularly noticeable for general enquiries into cognitive impairment, expressing confusion and uncertainty over why this occurs. One neuropsychologist speculated a possible lack of focus on cognition by physicians managing persons living in PD. Others speculated whether physicians were seeking cognitive assessment from alternative sources such as research projects. “I tried to get them [colleagues] to do the survey. They're like, but we don't really see any PD patients. I might have seen them a few years ago. It's not something that they do see.” [Interviewee3013] “I'm surprised we receive only occasional referrals for PDD. I'm surprised that we're not getting more. I'm not quite sure why that is.” [Interviewee3011]
Accompanying Motor and Non-motor Symptoms
Neuropsychologists flagged the prevalence of motor dysfunction due to PD, and the negative impact it can have on assessment validity. Administering tests without a motor component was stated as common practice to help mitigate the effect of motor symptoms. However, one neuropsychologist acknowledged this as an ongoing challenge, explaining persons living with PD demonstrate impairment in several motor functions (eg, handwriting, speech), and the difficulty in identifying tests suitable to assess cognition under these circumstances. “While I would attempt to administer visuoconstructional type tasks, I am very aware about the effects of tremor and slowness of movement, so I might look for alternatives to certain tasks.” [Interviewee3009]
Neuropsychologists also described the prevalence of neuropsychiatric disorders in persons living with PD, the influence these disorders can have on cognitive functioning, and the need to capture these disorders to ensure accurate interpretation of test results. Use of supplementary tests to detect neuropsychiatric symptoms and other possible explanations for cognitive impairment was noted as important practice. Again, one neuropsychologist explained persons living with PD who co-present with neuropsychiatric symptoms and cognitive impairment as a common diagnostic challenge. “There are often psychological difficulties that people are struggling through.” [Interviewee3011]
Flexible Practice
Neuropsychologists regularly described having a flexible practice approach when assessing persons living with PD. Assessment batteries were said to be dynamic, including and omitting tests throughout as more information is gathered and new hypotheses tested. Neuropsychologists described their deliberate flexibility as being useful for conducting efficient and personalised practice with persons living with PD. “We have maybe half a dozen suggested assessment protocols. And then we will add and subtract, depending on referral questions, how the patient is presenting so hypotheses that we generate during the assessment itself.” [Interviewee3011]
Barriers to Assessment
Neuropsychologists raised multiple barriers which complicate or preclude assessment in persons living with PD. Availability of appropriate tests was a common problem. Neuropsychologists stated test selection becomes substantially more limited once removing tests impacted by motor function. Test selection was also described to become further restricted when assessing persons from culturally and linguistically diverse backgrounds.
Poor access to assessment for persons living with PD was also raised. Neuropsychologists discussed issues at multiple levels, including extensive wait times to receive assessment, higher costs for persons seeking quicker self-funded services, and speculation around specialised physicians referring for assessment only at the point of severe impairment. Restricted patient availability was also raised by neuropsychologists, noting the difficulties in organising appointment times which align with the person’s PD medication regimen, pre-planned travel needs, and pre-existing medical appointments. “Many patients are quite elderly and transport to appointments is challenging, as is trying to find time to conduct assessment given their many appointments.” [Survey Respondent 7]
Lastly, neuropsychologists discussed professional restrictions as a barrier. Insufficient funding dedicated to movement-disorder-affiliated neuropsychology positions, and the constraint it has on tracking cognitive progression overtime. One neuropsychologist described their experience of assessment in persons living with PD as being channelled through a handful of services rather than being conducted broadly across clinics, attributing this problem to current funding models. “I think what would need to happen is we'd need more FTE clearly. We’d need a position where we could be more actively part of a movement disorders clinic.” [Interviewee3014]
Theme 3. Experiences of Repeat Assessment
The referral processes for repeat assessment were heterogenous. One neuropsychologist reported all PD patients undergo a baseline measure of cognition at diagnosis and then receive a follow-up assessment by default 2 years later. Another neuropsychologist described their PD patients require a new referral to trigger a repeat assessment. The latter neuropsychologist expressed irritation with their system, noting the degenerative nature of PD. “In terms of do we then routinely bring them back in a year or two years? No, we would wait for another referral. That is something that always, like, irritates me with these degenerative ones that maybe we should have them more on a recurring system.” [Interviewee3010]
Practice differences for repeat assessment were also described. One neuropsychologist noted cognitive decline being gradual in PD patients, stating to first administer a brief cognitive screen to determine if another comprehensive battery is required or if an abridged version can be administered. Considerable attention was also placed on circumstances where repeat assessment yield value for neuropsychologists and persons living with PD. One neuropsychologist emphasised importance in pursuing comprehensive assessment only when there is reasonable concern for cognitive impairment. They described the finite resources available to neuropsychologists, in conjunction with the ethical concerns and impracticality of subjecting PD patients with intact cognition to hours of unnecessary testing. Certain neuropsychologists indicated specific time intervals to review persons living with PD for repeat assessment, again varying in their preference. “I think in an ideal world it's nice to review patients every 6 months or so, and check in with them about any cognitive difficulties.” [Interviewee3011]
Theme 4. Perceptions of Digital Modalities
Several challenges were discussed on using digital modalities for cognitive assessment in persons living with PD. Neuropsychologists described multiple contraindications (eg, poor technology literacy, fine motor dysfunction, sensory impairment) thought to potentially impact telehealth and computerised testing use in PD patients. Neuropsychologists also stated the insufficient normative data and validity studies for test use with digital modalities further reduces an already limited test range for PD assessment.
Challenges specific to digital modalities were also raised. Neuropsychologists expressed concern over telehealth impacting behavioural observation, in particular the impact of motor dysfunction on test performance. Computerised testing was mentioned to experience problems with budget constraints impacting access to necessary equipment. Unsupervised online testing had issues raised over performance validity with the unregulated environment. Unfamiliarity with how to incorporate digital modalities into assessment was also expressed by neuropsychologists. “With PD, I find being in the room very helpful to get a good picture of their physical symptoms. I think telehealth may not provide a full picture of their presentation.” [Survey Respondent 12] “I am barely able to get the hospital to fund record forms, let alone computerised tests!” [Survey Respondent 8]
Benefits of digital modalities were shared as well. Certain neuropsychologists were encouraged by the potential of computerised batteries to streamline, automatise, and standardise assessment in persons living with PD. Improved access to assessment through telehealth was also acknowledged, stating its notable advantage for PD patients as a group vulnerable to mobility and travel constraints. Finally, one neuropsychologist mentioned telehealth can improve tolerability by allowing persons living with PD to remain comfortable in a familiar environment. “I think there's some real potential benefits [telehealth]. Reaching the masses, being able to screen for more cognitive impairment and maybe not having to see everybody in a really long in-depth kind of traditional neuro-assessment way.” [Interviewee3011]
Mixed Methods Integration
From the mixed methods integration, four service gaps were identified for neuropsychologists in PD assessment. These included: (1) variable assessment practices used across neuropsychologists; (2) infrequent engagement of neuropsychologists; (3) suboptimal availability of neuropsychological tests suitable for persons living with PD; and (4) limited integration of digital modalities within practice. A joint display mapping the mixed methods findings onto each service gap is provided in Figure 2. Furthermore, alignment between the quantitative and qualitative strand findings were evident with three convergent, three complementarity, and one expansion meta-inference generated. All meta-inferences and their relevant service gap are detailed in Figure 3. Joint display of mixed methods integration. Note. PD = Parkinson’s disease; DBS = Deep brain stimulation; PD-MCI = Parkinson’s disease mild cognitive impairment; PDD = Parkinson’s disease dementia Neuropsychology service gaps and associated meta-inferences. Note. PD = Parkinson’s disease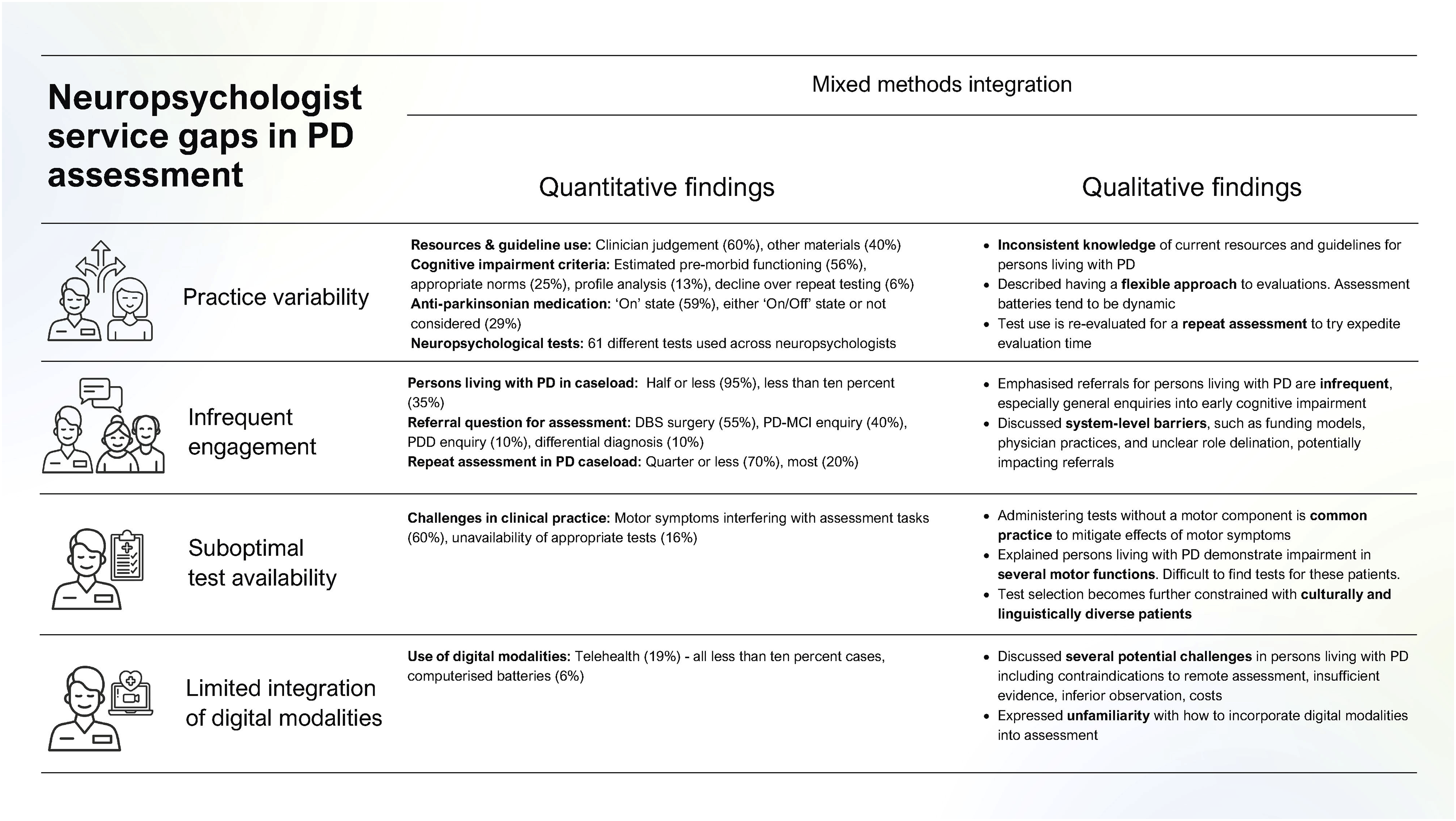
Discussion
The present study used a mixed methods design to investigate how neuropsychologists engage with and provide cognitive assessment to persons living with PD. Analysis of the integrated data indicated four service gaps for neuropsychologists in PD assessment.
Service Gaps and Recommendations
Practice Variability
Neuropsychologists were found to use heterogenous assessment practices in persons living with PD. Practice differences may stem partly from clinician flexibility, stated as a deliberate and useful feature of PD assessment. However, inconsistent knowledge on assessment guidelines, and contradictory ideas around diagnostic criteria, medication state, and characterising impairment suggest inadvertent practice variability among neuropsychologists. Differences in assessment procedures can impact both the incidence rate and presentation of cognitive impairment in persons living with PD.27,28 Practice variability may therefore stir inconsistent decision-making around diagnosis and care of cognitive impairment, as reflected in prior research where PD patients reported receiving unclear direction and information about their cognitive disorder.29,30 Recent efforts to derive best practices for assessment in PD and improve clinician standardisation have occurred.14,31-33 Yet, further implementation work to educate and encourage practice adoption among neuropsychologists may be required to minimise practice variability and improve resource awareness.
Infrequent Engagement
Neuropsychologists reported to assess cognition infrequently in persons living with PD. Assessments were primarily referred for elective DBS surgery, where significant barriers to treatment exist and estimated occurrence among PD patients is under 2 percent.34,35 Interestingly, general referrals to characterise and support diagnosis of cognitive impairment were less common despite high prevalence of cognitive disorders in PD patients and expert recommendation to conduct neuropsychological assessment for greater diagnostic precision.7,8
Neuropsychologists suggested irregular referral patterns may be driven by system-level factors. Funding models, physician practices, and unclear role delineation across healthcare teams were indicated as possible contributors impacting engagement. This is consistent with another evaluation of PD cognitive services in the United Kingdom, 29 with calls for greater awareness of available cognitive services to persons living with PD.29,36 Best practice guidelines which establish system-level processes for diagnosis and management of cognitive disorders due to PD may enhance neuropsychologists’ engagement by coordinating multidisciplinary communication and delivering a pipeline for effective use of neuropsychology services. 31 Practice guidelines may also help to increase provision of repeat assessments; however further clarification is needed to understand whether low reported rates are due to system and patient level barriers or clinical decision-making.
Suboptimal Test Availability
Tests to assess cognition in persons living with PD were suboptimal for neuropsychologists. Test availability was reported to be complicated by both co-presenting motor problems and cultural factors, with similar difficulties to evaluate impairment reported in PD cognitive services across the United Kingdom. 29 Limited test selection may impact both the certainty and scope of conclusions neuropsychologists can draw to support diagnosis and management of cognitive impairment due to PD. Such concerns have incited development of novel tests, adaptation of existing tests, and generation of PD-specific normative data to better optimise test selection. 32 Advancement within this space has begun 37 ; however greater evidence is needed to support larger scaled adjustments to neuropsychologists’ practice. Reviews of existing tests to recommend the most optimal choices for assessment in persons living with PD have occurred as an immediate response to improving test selection.14,32,33
Limited Integration of Digital Modalities
Neuropsychologists reported limited integration of digital modalities into assessment for persons living with PD. Concerns over use and unfamiliarity with incorporating telehealth and computerised methods into assessment were shared, only applied by a small minority in practice. These findings conflict with recent research reporting both higher rates and a general upward trend in telehealth use among neuropsychologists following onset of the COVID-19 pandemic. 38 Digital modalities hold potential to improve service provision and access to assessment for persons living with PD. 39 Preliminary research suggests digital modalities are feasible and acceptable when used in assessment for persons with PD,40-42 yet further work is required to support neuropsychologists seeking to provide this practice model. Potential areas for development include more validation studies of neuropsychological tests administered with digital modalities and generating training resources to educate and upskill neuropsychologists on its practice.
Limitations and Future Directions
Findings from the study should be interpreted in line with its limitations. The sample size was small, in part due to the specialised target population of neuropsychologists practicing in Australia with PD experience. Furthermore, data from semi-structured interviews were derived solely from neuropsychologists based in Queensland. These factors impact use of the results to draw broader conclusions about neuropsychologist practice patterns across other contexts and regions. Nevertheless, the findings align with recent evidence from the United Kingdom, 29 indicating its relevance to certain settings, and may benefit hypothesis generation of future research exploring service gaps in other settings. Future research examining post-assessment practices by neuropsychologists may also be helpful to understand cognitive rehabilitation, post-diagnostic care and support planning in PD.
Conclusion
The present study explored engagement and practices of Australian neuropsychology services to assess cognition in persons living with PD. Neuropsychologists were revealed to use variable practices and have infrequent engagement with persons living with PD. They were also revealed to have suboptimal test materials and rarely integrated digital modalities into their assessments. Further work to improve provision of neuropsychology services for persons living with PD is needed to ensure effective diagnosis and management is provided.
Supplemental Material
Supplemental material - Neuropsychologists’ Engagement with and Cognitive Assessment in Parkinson’s Disease: A Mixed Methods Australian Investigation
Supplemental material for Neuropsychologists’ Engagement with and Cognitive Assessment in Parkinson’s Disease: A Mixed Methods Australian Investigation by James M. King, BPsychSc, Nadeeka N. Dissanayaka, PhD, Deborah Brooks, PhD, Leander K. Mitchell, PhD, Kumareshan Sivakumaran, DPsych, Jihyun Yang, PhD, Deepa Sriram, PhD, Sharon L. Naismith, DPsych, Nancy A. Pachana, PhD, Rebecca Gough, BPsychSc, Dana Pourzinal, PhD in Journal of Geriatric Psychiatry and Neurology.
Footnotes
Acknowledgements
We acknowledge the contributions of our Consumer and Community Involvement Group and PDCogniCare team members: Tiffany Au, Dr Elton Lobo, Prof Elizabeth Beattie, A/Prof Annette Broome, Prof Gerard Byrne, Mark Chatfield, Anna Kelder, Dr Sabrina Lenzen, Prof Peter Nestor, Stuart Robertson, Dr Kirstine Shrubsole, Dr Ada Lo, Helen Tinson, Professor Martie-Louise Verreynne, Dr Peter Worthy, and Em Prof Neil Page. We also acknowledge PDCogniCare partners: Parkinson’s Queensland Inc, Dementia Australia, Royal Brisbane & Women’s Hospital, Princess Alexandra Hospital, OPN365 Pty Ltd, the Australian Dementia Network (ADNeT), Lions Club of Brisbane Inner North, and Lions District 201Q3.
Ethical Considerations
The PDCogniCare project was approved by the Metro North Health HREC (HREC/2023/MNHA/100098).
Consent to Participate
Written or electronic informed consent was collected from all participants.
Author Contributions
Research project: A. Conception, B. Funding, C. Organization, D. Execution.
Data analysis: A. Design, B. Execution, C. Review and Critique.
Manuscript Preparation: A. Writing of the first draft, B. Review and Critique.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Government MRFF Dementia Aging and Aged Care Mission Grant 2022. JMK was also supported by the Commonwealth through an Australian Government Research Training Program Scholarship [DOI: https://doi.org/10.82133/C42F-K220]. Funding bodies were not involved in any decision-making processes for this study. National Health and Medical Research Council; 2022/MRF2024389
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data files may be shared, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.