
Abstract
Purpose of Research
Lucidity is the transient recovery of abilities and communication that were seemingly lost among people living with dementia (PLWD). This study describes lucid episodes reported by Alzheimer’s dementia (AD) and Lewy Body Dementias (LBD) caregivers. We analyzed survey data from 212 current AD (n = 191) and LBD caregivers who reported the frequency, duration, and characteristics of 653 lucid episodes witnessed in the past month.
Major Findings
Most AD caregivers (67%) and LBD caregivers (81%) witnessed a lucid episode within the past month. LBD caregivers reported lucid episodes with greater changes in awareness and communication, compared to AD caregivers. LBD caregivers reported longer lucid episodes and that the PLWD knew about their change in lucidity, compared to AD caregivers.
Conclusions
Findings suggest that differences in lucid episode intensity, timing, and meta-awareness between AD and LBD are possible and may inform care strategies for PLWD.
Introduction
Alzheimer’s Dementia (AD) and Lewy Body Dementias (LBD)—which include dementia with Lewy bodies (DLB) and Parkinson disease dementia (PDD)—are the most common causes of neurodegenerative dementia, accounting for 60-80% and 20-30% of all dementia cases, respectively. Over 8.1 million people have AD and LBD, and they receive care from 11.5 million family caregivers in the U.S.1,2 While AD and LBD share some clinical symptoms, research has also focused on their clinical differentiation in order to inform diagnosis, treatment, and care planning.3-5
In contrast to the routine cognitive fluctuations that are expected among people living with dementia (PLWD), 6 lucid episodes are periods when there is a transient recovery of communication or other abilities that had seemingly been permanently lost.7,8 Lucid episodes provide brief but meaningful windows of connection, but their existence conflicts with fundamental assumptions about the downward and permanent trajectory of cognition that typically defines dementia. 9 Occurring during the later course of disease progression, they are often described as diverse in presentation. They are sometimes prompted by external stimuli but can also occur spontaneously.10-14 No studies, however, have compared lucid episodes between different dementia types, including AD and LBD, and it is unclear if, like their differing clinical presentations and symptoms, lucid episodes by type of dementia also differ. Characterizing the frequency, duration, and intensity of lucid episodes across AD and LBD, including changes in awareness and communication as reported by family caregivers, is a critical first step towards understanding if lucid episodes are shaped by disease specific pathology. This study analyzes AD and LBD family caregiver reports of lucid episodes to understand these differences and their implications for diagnosis and care.
Methods
Data and Sample
This study’s protocol was published elsewhere. 15 To recruit informal caregivers of PLWD, this study used a purposive sampling strategy. Participants were recruited through dementia caregiver registries at five organizations: (a) the A-LIST® administered by UsAgainstAlzheimer’s (usagainstalzheimers.org), (b) University of Minnesota Caregiving Registry, (c) the Brain Health Registry administered by the University of California, San Francisco, (d) Banner Alzheimer’s Institute, and (e) Mayo Clinic’s Alzheimer’s Disease Research Center. These organizations had different strategies for identifying potential caregivers for their registries (e.g., mailed and emailed letters; educational events; community outreach events, such as health fairs; podcasts, social media posts, and newsletters). Electronic invitations were sent via email to registry members. The invitation briefly described the study and a version of the National Institute on Aging’s working definition of the LE phenomenon (“a lucid episode is when there is a spontaneous return of meaningful, relevant communication or other abilities that were believed to be permanently lost”)7,8 and provided a hyperlink to an electronic screening questionnaire from the Mayo Clinic Survey Research Center to assess eligibility (i.e., adult caregivers who currently provide unpaid assistance to PLWD; possible to complete online surveys). Informed consent was obtained verbally, and the study was approved by the Mayo Clinic Institutional Review Board.
A total of 522 participants completed a survey from July 2023 to December 2024. Given the focus of this study on the AD-LBD caregiver comparisons, we first selected 311 caregivers (59.6%; AD caregiver n = 285 and LBD caregiver n = 26), excluding 27 caregivers who reported no dementia diagnosis and 184 caregivers who reported other dementia types (unspecified n = 85; vascular n = 41; frontotemporal n = 19; mixed dementia n = 39). Among 311 caregivers, 67% of AD caregivers (n = 191) and 81% of LBD caregivers (n = 21) reported witnessing a lucid episode within the past month. The present study analyzed caregiver-reported data from these 212 caregivers who described the frequency, duration, and characteristics of lucid episodes they witnessed in the past month.
Measures
Demographic Characteristics of Caregivers and PLWD
We asked for demographic characteristics of caregivers and PLWD, including relation to PLWD (spouse/partner, child/in-law, and others), age (in years), gender (1 = female and 0 = male), marital status (1 = married or remarried and 0 = others), work status (1 = working full- or part-time and 0 = not working), education (1 = some primary or high school to 7 = doctoral degree), financial situation (1 = having difficulty paying bills to 4 = after paying bills, still enough money), race/ethnicity (1 = non-Hispanic White and 0 = ethnic and racial minority), and health status (1 = poor to 5 = excellent).
Caregiving Characteristics of Caregivers and PLWD
For caregiving characteristics, we assessed care duration (in months), co-residence with PLWD (1 = yes, 0 = no), PLWD’s limitations in activities of daily living 16 (ADL; mean of 5 items rated from 0 = normal/no difficulty to 3 = completely dependent on someone to help), PLWD’s limitations in instrumental activities of daily living 17 (IADL; mean of 10 items rated from 0 = normal/no difficulty to 3 = completely dependent on someone to help), caregiving hours (during weekdays and weekends; per day), and social support 18 (mean of 8 items rated from 1 = none of the time to 5 = all of the time; α = .93).
Characteristics of Lucid Episodes in PLWD
To assess if a lucid episode was witnessed (1 = yes, 0 = no), caregivers were asked “In the past month, have you witnessed a lucid episode?” (That is an unexpected change in his/her thinking or concentration, where he/she has been lucid, alert, aware of his/her surroundings or able to communicate in meaningful ways. This could be verbal or non-verbal communication.) Caregivers then reported the characteristics and attributes of up to five lucid episodes (episode N = 653). Caregiver-reported characteristics of lucid episodes included: (a) cognitive status prior to episode (seven categories; 1 = fully aware with no impairments—no problems with memory, attention, or focus; 2 = minor difficulty with memory, attention, or focus; 3 = moderate difficulty with memory, attention, or focus; 4 = extreme difficulty with memory, attention, or focus; 5 = most or much of the time awake, but not responding or reacting to anything around them; 6 = mostly asleep, but when awake, not aware of surroundings; and 7 = unconscious), (b) circumstances prior to an episode (e.g., no special circumstances; visits from family/friends; change in medication; change in healthcare setting; music playing; reminiscing; valued ritual/behaviors), (c) how it started (three categories; 1 = someone prompted; 2 = without a prompt from another person; and 3 = after a prompt, such as a song and prayer), (d) degree of change in awareness and communication ability (1 = very small change to 5 = very large change), (e) how long the episode lasted (1 = under 10 minutes to 8 = more than 7 days), (f) when it occurred (three categories; 1 = morning [5 a.m. to 12 p.m.]; 2 = afternoon [12 p.m. to 6 p.m.]; and 3 = evening/night [6 p.m. to 5 a.m.]), (g) communication quality during the episode (five categories; 1 = aware, communication made complete sense; 2 = aware, communication made some sense; 3 = aware, but not make any sense; 4 = aware, but only non-verbal communication; and 5 = drowsy, confused, not make any sense), and (h) whether PLWD knew about their change in lucidity (1 = yes, 0 = no).
Analysis Plans
Prior to the main analysis, assumptions of normality and homogeneity of variance for continuous variables were assessed using Shapiro-Wilk tests and Levene’s tests, respectively, particularly considering the substantial disparity in sample sizes between the AD and LBD caregiver groups. Although the data exhibited deviations from normality due to inherent skewness and imbalanced group sizes, Generalized Estimating Equations (GEE) were employed for the primary analyses. GEE is particularly advantageous in this context. It provides robust parameter estimates and does not require strict distributional assumptions, effectively handling non-normal data and unequal group sizes through the use of a Huber-White sandwich estimator (robust covariance matrix).19,20
First, we compared the sociodemographic and caregiving characteristics of caregivers and PLWD between the AD and LBD groups using chi-square tests and independent t-tests. To assess the practical significance of these differences, effect sizes were calculated using Cohen’s d for continuous variables and Cramér’s V for categorical variables.21,22 To mitigate potential bias arising from imbalanced sample sizes, 95% confidence intervals (CIs) for all effect sizes were estimated using bootstrapping with 1,000 resamples.
Second, to analyze the characteristics of lucid episodes, we utilized GEE to address the statistical limitations inherent in imbalanced sample sizes and to account for the nested structure of the data (ie, multiple episodes clustered within individual caregivers). Specifically, we employed robust estimators for the covariance matrix, which provide valid standard errors even under conditions of unequal group sizes. Group differences were analyzed with AD (coded as 0) serving as the reference group to evaluate the relative characteristics of the LBD group (coded as 1). Results are reported as odds ratios (OR) for categorical outcomes or unstandardized coefficients (B) for continuous outcomes, accompanied by 95% bias-corrected and accelerated (BCa) confidence intervals. This approach ensures a robust interpretation of the magnitude and direction of differences, independent of p values.
Results
Caregiver and PLWD Characteristics in AD and LBD Caregivers
Comparisons of Sample Characteristics Between AD and LBD Caregivers
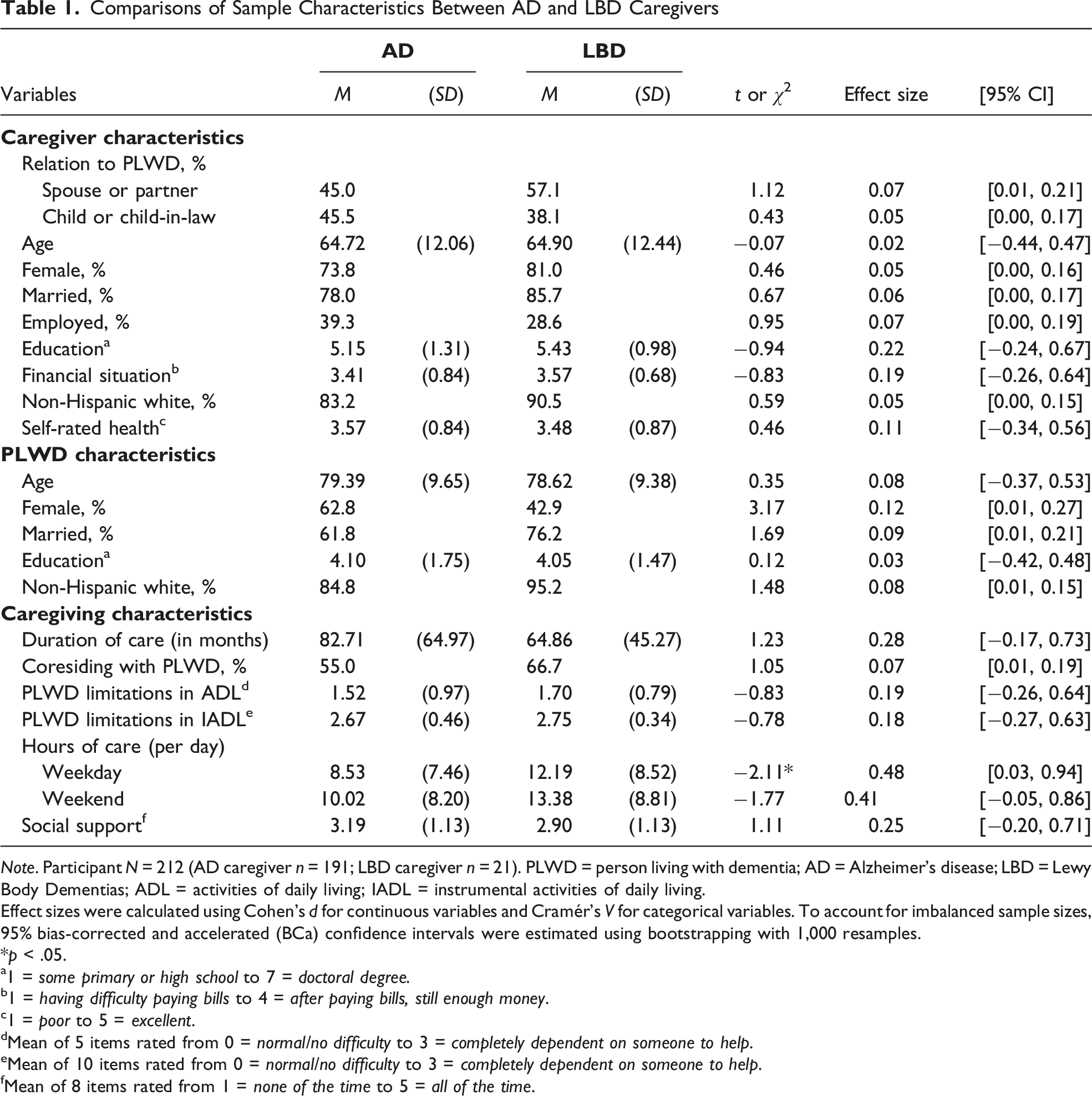
Note. Participant N = 212 (AD caregiver n = 191; LBD caregiver n = 21). PLWD = person living with dementia; AD = Alzheimer’s disease; LBD = Lewy Body Dementias; ADL = activities of daily living; IADL = instrumental activities of daily living.
Effect sizes were calculated using Cohen’s d for continuous variables and Cramér’s V for categorical variables. To account for imbalanced sample sizes, 95% bias-corrected and accelerated (BCa) confidence intervals were estimated using bootstrapping with 1,000 resamples.
*p < .05.
a1 = some primary or high school to 7 = doctoral degree.
b1 = having difficulty paying bills to 4 = after paying bills, still enough money.
c1 = poor to 5 = excellent.
dMean of 5 items rated from 0 = normal/no difficulty to 3 = completely dependent on someone to help.
eMean of 10 items rated from 0 = normal/no difficulty to 3 = completely dependent on someone to help.
fMean of 8 items rated from 1 = none of the time to 5 = all of the time.
Comparisons of Lucid Episodes Between AD and LBD Caregivers
Comparisons of Lucid Episodes Between AD and LBD Caregivers
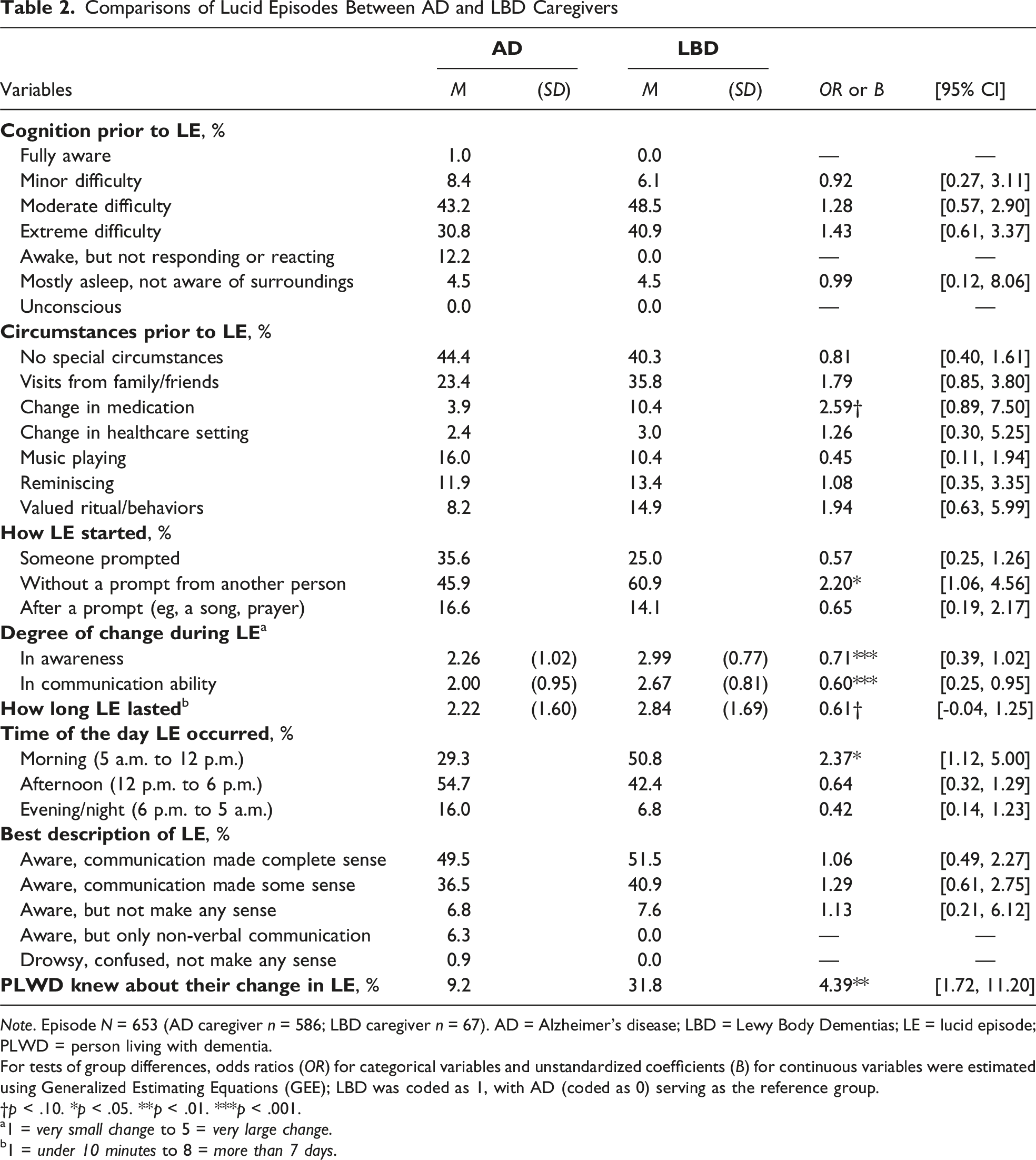
Note. Episode N = 653 (AD caregiver n = 586; LBD caregiver n = 67). AD = Alzheimer’s disease; LBD = Lewy Body Dementias; LE = lucid episode; PLWD = person living with dementia.
For tests of group differences, odds ratios (OR) for categorical variables and unstandardized coefficients (B) for continuous variables were estimated using Generalized Estimating Equations (GEE); LBD was coded as 1, with AD (coded as 0) serving as the reference group.
†p < .10. *p < .05. **p < .01. ***p < .001.
a1 = very small change to 5 = very large change.
b1 = under 10 minutes to 8 = more than 7 days.
While most lucid episodes contained communication that was coherent, AD caregivers more frequently reported episodes involving only non-verbal awareness without verbal communication (6.3% vs. 0.0%; χ2 = 4.43; p = .035). Finally, LBD caregivers were more likely to report that the PLWD exhibited meta-awareness, or knowledge of their own change in lucidity (OR = 4.39, p = .002, 95% CI [1.72, 11.20]).
Discussion
The current study aimed to describe differences in reports of lucid episodes from family caregivers of people living with AD and LBD. The specific pathology causing each type of dementia dictates the differences in behavioral trajectories and pharmacological risks experienced by the PLWD 24 and the unique care burden for family caregivers. 25 Clinical presentations are different in AD and LBD. 3 Based on our current scientific understanding, while AD typically presents with progressive episodic memory loss, language deficits, and communication difficulties, and motor symptoms can be rare until late stages. LBD, on the other hand, is characterized by fluctuating cognition and neuroleptic sensitivity; and the clinical presentation could include parkinsonism. 5 Our findings suggest that, just as there are unique clinical presentations and associated symptoms between AD and LBD, lucid experiences may also be different. For example, AD caregivers reported more non-responsiveness prior to lucid episodes than LBD caregivers. LBD caregivers, however, reported more medication changes prior to lucid episodes and episodes characterized by a greater magnitude of change in awareness and communication ability than AD caregivers. These presentations by dementia type may be especially helpful in distinguishing routine “good days and bad days” or typical symptoms from the unexpected and transient recovery of abilities characterizing lucidity and could provide guidance for future research to explore antecedents to lucidity and the possible neurological pathways that can result in lucidity.
AD and LBD caregivers reported lucid episodes with similar frequency and descriptions. Lucid episodes differed in intensity, as LBD caregivers reported greater changes in awareness and communication ability compared to AD caregivers. Particularly, LBD caregivers were more likely to report on PLWD’s meta-awareness about their change in lucidity, which raises the possibility that meta-awareness could be an attribute of lucid episodes in LBD and that aspects of self and self-awareness may persist throughout the LBD trajectory,10,26 though this interpretation requires further exploration. This finding aligns with the concept of preserved consciousness, or the idea that many aspects of memory, cognition, emotion, and perception are preserved among PLWD. 27 Exploration of meta-awareness in LBD, including its changes over time, may help disentangle the mechanisms underlying awareness 28 and help to determine if awareness is an attribute or indicator of lucidity for LBD.9,14,26
LBD caregivers reported more lucid episodes occurring in the morning and they lasted longer than episodes reported by AD caregivers. It is possible that lucid episodes in LBD are associated with sleep disturbances including excessive daytime sleepiness, and rapid eye movement behavior disorder which are present in 90% of people with LBD. 29 The finding that lucid episodes were reported to be more frequently in the morning hours may be an indication that lucidity occurs temporarily upon waking and before daytime sleepiness sets in, but further research is needed. These preliminary findings raise the possibility that interventions targeting sleep regulation may enhance lucid episodes by optimizing alertness and mood in the morning hours. The longer duration of lucid episodes in LBD may also provide opportunities for other forms of data capture about lucidity, such as video or ecological momentary assessments, instead of solely relying on caregiver reports. Other forms of data may provide nuanced details about lucidity that could help develop interventions to support caregivers witnessing lucidity and offer them actionable feedback on the experience, given that some caregivers find lucid episodes stressful.30,31 Future research should integrate these approaches to capture the flow and awareness of attention of lucid episodes in real-time.
Our results suggest that the type of dementia influences the intensity, timing, and presence of meta-awareness experienced during lucid episodes. Given the observational and retrospective nature of the data and the small LBD caregiver sample, these exploratory findings should be interpreted with appropriate caution pending replication in larger, prospectively designed studies. Further research with larger, more diverse caregiver samples is needed to validate these results and provide a clearer understanding of lucid episodes across dementia types. While some PLWD may have had biomarker confirmed diagnosis, the diagnoses were not clinically verified, but rather reported by caregivers, and therefore, there may be some misclassification of dementia type. Additionally, while caregivers were provided with practical guidelines to identify and report lucid episodes, caregiver reports of lucidity may reflect cultural interpretations or emotional perceptions of the experience. Finally, our study relied on caregiver’s retrospective accounts over a 30-day period, which introduces potential bias. Future studies should assess lucid episodes in real-time and may offer more precise insights into the nature and dynamics of lucid episodes.
Despite these limitations, our study reveals novel findings on how LBD and AD caregivers experience and report lucid episodes. These results can help guide caregiver education, inform future hypotheses on neurological pathways for lucid episodes, and provide clinical guidelines on how best to support caregivers.
Footnotes
Ethical Considerations
The study was approved by the Mayo Clinic Institutional Review Board (IRB Number 22-00686).
Consent to Participate
Verbal consent was obtained prior to participation.
Author Contributions
Dr. Bangerter drafted the manuscript. Dr. Kim conducted data analysis. Drs. Griffin, Lapid, Kim, Graff Radford, and Liu provided critical revision of the manuscript and valuable contributions to study design.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the National Institute on Aging (R33AG069767, Definition and Caregiver Appraisal of Paradoxical Lucidity in Dementia, PI: J. M. Griffin; 1K01AG081566, Cognitive Health and Modifiable Factors of Daily Sleep and Activities Among Dementia Family Caregivers, PI: Y. Liu). K. Kim was supported by the New Faculty Startup Fund from Seoul National University.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Graff Radford serves on the DSMB for NINDS StrokeNET, is the site-PI for grants sponsored in part by Eisai and Cognition Therapeutics, and is an associate editor for JAMA Neurology. All other authors declare no conflicts of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.