
Abstract
The objective of this study was to summarize and review literature on treatment methods for stenoses of the posterior urethra. Stenosis of the posterior urethra, particularly of a bladder neck stenosis (BNS) or vesicourethral anastomotic stenosis (VUAS), presents significant clinical challenges, in part owing to the heterogeneity of the patient population and additionally secondary to morbidity of historic definitive treatments. Traditionally, this disease process has been preferentially managed with endoscopic interventions in the form of direct vision internal urethrotomy or dilation, with or without injectables, with variable success rates ranging from 40.0% to 72.0%; however, 90.0% of patients require repeat intervention within the first 2 years. Definitive treatments were often more challenging, requiring joint abdominoperineal approaches, and thus less utilized outside of academic centers with reconstructive urologists. Recent advancements in the endoscopic management of posterior urethral stenosis are synthesized in this review, specifically in populations at increased risk, including those with radiation therapy, transurethral prostate resections, or radical prostatectomy. Herein, a literature review of publications from 2014 to 2024 highlights key endoscopic techniques such as drug-coated balloon dilation and transurethral mucosal realignment aimed at treating BNS and VUAS. These novel techniques demonstrate short-term success rates approaching 85.0% to 90.0%, which represents a significant improvement in success compared with traditional endoscopic therapies. Overall, the current review emphasizes the evolution of minimally invasive treatment options for posterior urethral stenosis, focusing specifically on BNS and VUAS, demonstrating the evolution of the scope of minimally invasive techniques and improved patient outcomes.
Introduction
The posterior urethra consists of the bladder neck and membranous urethra; urethral stenosis refers to scar tissue formed in the posterior urethra where the corpus spongiosum is absent. Stenosis in this location is a known complication of common urologic procedures for treatment of benign prostatic hyperplasia and prostate cancer treated by either radiation or radical prostatectomy and is referred to as bladder neck stenosis (BNS) or vesicourethral anastomosis stenosis (VUAS), respectively. These complications cause distress and diminishing patient quality of life, increased cost for the medical system, and consternation to urologists across the globe. 1,2 Though membranous stenosis is included in the posterior urethra, this review will focus on the bladder neck.
The incidence of BNS varies depending on the type of method used for prostatic reduction. Transurethral resection of the prostate (TURP) and photovaporization of the prostate have similar bladder neck contracture (BNC)/BNS rates ranging from 0.4% to 4.9% to 0.0% to 5.9%, respectively. 3,4 The incidence of BNS from holmium laser enucleation of the prostate, a technique increasing in utilization, was recently summarized to have rates between 1.1% and 7.0%, with increased incidence in smaller prostates <50 cm3. 5 Historical literature demonstrated a higher incidence of BNS in men who had a TURP 30 days prior to external beam radiation therapy compared with the no TURP group, 15.0% vs 6.0%, respectively. 6 Given the age of these data, it is difficult to compare directly; however, radiation is certainly thought to diminish the wound healing capabilities of tissue. Specifically, radiation is thought to lead to fibrosis through the loss of oxygenation of the tissue owing to overproduction of cytokines. 7
Success rates associated with common procedures examine modifiable risk factors. The risk factors for BNS include low adenoma weight, the use of large resecting loops, and extensive resection of the bladder neck. It is thought to occur because of hypertrophic scarring from extensive heat, resection, and fulguration at the bladder neck. Modifiable risk factors include diabetes, smoking, and cardiovascular disease. 5,7 Radical prostatectomy is another source of iatrogenic posterior urethral stenosis and, because of the altered anatomy, is referred to as a VUAS. VUAS is proposed to be mechanistically more likely if a narrow anastomosis is created between bladder and urethra or if there is a lack of complete mucosal apposition. It is thought to occur secondary to obliterative endarteritis at the anastomosis. The range of incidence after radical prostatectomy varies from 2.7% to 25.7%, 2 with a potentially higher risk for open radical prostatectomy compared with robotic approaches. 8
The Société Internationale d’Urologie (SIU) guidelines from 2010 recommend initial evaluation of posterior urethral stenosis to include laboratory analysis with urine culture, urodynamics, when possible, to evaluate for voiding dysfunction or urinary incontinence, and cystoscopy for initial evaluation of nontraumatic strictures. 9 Transurethral resection or direct vision internal urethrotomy (DVIU) according to American Urologic Association (AUA) and European Urologic Association (EAU) guidelines are first-line therapies, though the AUA recommendations allow for urethral dilation while the EAU guidelines do not. 10,11 In refractory cases the AUA and EAU guidelines suggest consideration of reconstruction of the bladder neck with T-plasty or V-Y plasty to be the next step (discussed in Yu et al. 12 ).
Endoscopic procedures have the benefit of not requiring a major operation, incisions, or increased recovery time; however, they have traditionally had the lowest success rates (Table 1). Based on the data for anterior urethral stricture treatment, endoscopic interventions have had lower success rates than open repairs. Large series of open abdominoperineal reconstructions are uncommon given the rarity of the disease process. Since the location of the posterior urethra poses significant challenges in open repair, a novel endoscopic technique with a higher success rate has been sought out. Two novel endoscopic techniques have been described within the past 5 years for treatment of posterior urethral stenoses. Although these techniques require adopting a new skill set, they have the potential for reduced morbidity when compared with open procedures as well as increasing the interval until the next intervention. More data are necessary before widespread use of these techniques, but they have the potential for dramatic improvement over standard methods of endoscopic stenosis treatment such as dilation and DVIU.
Summary of Outcomes Data by Intervention
DCB = drug-coated balloon; DVIU = direct vision internal urethrotomy; TURP = transurethral resection of the prostate.
This review focuses predominantly on the management of BNS and VUAS. Mechanistic underpinnings will be discussed for each technique as well as a discussion of novel minimally invasive procedures.
Methods
A literature review of publications within the past 10 years from 2014 to 2024 regarding minimally invasive management of posterior urethral stenoses was performed. Using PubMed, search terms of “bladder neck contracture,” “vesicourethral anastomosis stenosis,” “posterior urethral stricture,” AND “minimally invasive” were employed to identify relevant articles. These were then reviewed by two separate reviewers (C.N.H. and T.D.) to determine inclusion in the study. Additional articles were obtained via reference lists of relevant systematic reviews and published guidelines on urethral stricture. Articles in languages other than English were excluded. Prior trends in management of urethral stricture disease were identified. Two novel treatment strategies were identified, namely transurethral mucosal realignment (TUMR) and drug-coated balloon (DCB).
Dilation and urethrotomy
Dilation and urethrotomy are by far the most common endoscopic treatments for urethral strictures of all locations. 27 Dilation refers to the sequential placement of dilators to stretch the urethra with the goal of stretching scar tissue without creating further scar tissue. This often results in a shearing force on the surrounding spongiosum tissue, which has been hypothesized to result in progression of stricture disease. Meanwhile, internal urethrotomy refers to a transurethral procedure to incise the scar tissue to allow release of scar contracture and healing to a larger lumen. The transurethral incision can be performed via knife (hot or cold) or by laser. In the majority of studies evaluating dilation and urethrotomy techniques for the posterior urethra, the etiology of the stenosis is VUAS. 11 Studies have not demonstrated a difference in recurrence-free outcomes based on DVIU technique alone. 13 In two studies investigating dilation and cold-knife DVIU on radiation-induced bulbomembranous stricture, patency ranged from 69.0%, 28 compared with 51.0%, with median follow-up time before stricture recurrence of 16 months. 29
Treatment recommendations for posterior urethral stenosis in the 2016 AUA guidelines are limited. Specifically, recommendations are given based on the etiology of the stricture, and no minimally invasive treatment option (dilation, incision, or resection) is recommended above the others in treatment of VUAS or BNS. 10 The 2010 SIU and 2022 EAU guidelines on urethral strictures provide further specific recommendations for posterior urethral stenosis, along with treatment recommendations that are given on the basis of etiology, including pelvic fracture urethral injuries and posterior urethral stenosis after prostate cancer treatment, which is further subcategorized into radical prostatectomy, radiation, and TURP. 30
Patency rates after controlled dilation and DVIU vary widely, from 0% to 90% to 25% to 100%, respectively. 11,31 In a single study comparing dilation, cold-knife urethrotomy, transurethral resection, and incision with holmium laser, it was reported that laser incision (55% overall treatment success) was superior to the other modalities (13%, 33%, and 41%, respectively). 14 In urethrotomy of VUAS, care should be taken to avoid incision at the 6 o’clock position, as there can be only a thin plane between the rectum and urethra, and this carries a risk of rectal injury and fistula. 11,31 An additional devastating complication considered after endoscopic treatment is fistulization to the symphysis pubis, which can lead to osteomyelitis. The EAU and SIU guidelines further specify recommendations for VUAS by obliterative vs non-obliterative stenosis and only recommend endoscopic procedures for initial treatment if the stenosis is non-obliterative. 9 According to the EAU and SIU guidelines, a VUAS that is obliterative should be managed with either open or robotic reconstruction of the bladder neck, which differs from the recommendations of the AUA. 9
Adjunctive endoscopic treatments
Although dilation and incision are common, the recurrence rates after endoscopic treatment of posterior urethral stenoses are high. For this reason, adjunct endoscopic treatments aimed at increasing success rates and decreasing the risk of need for a second procedure have been studied. In a study that investigated adjunct injection therapy in all locations of urethral strictures during endoscopic treatment, mitomycin C was associated with the lowest rate of recurrence. 1 Mitomycin C is an alkylating drug that inhibits DNA transcription, thereby preventing protein synthesis and cellular reproduction. 32 In a similar fashion to its inhibition of cellular reproduction of urothelial carcinoma cells, it may reduce recurrent scar formation associated with tissue disruption from DVIU or dilation. Of note, mitomycin C when used in the anterior urethra has been documented to cause necrosis 15 ; thus, it is the opinion of the authors that its use should be limited to the bladder neck or vesicourethral anastomosis. Corticosteroid (triamcinolone) injections reduce fibroblast collagen production, decrease inflammation, and increase fibroblast apoptosis. 33
Radial urethrotomy and intralesional mitomycin C for the management of recurrent BNCs have become the standard of care for this management. Patency rates after DVIU and mitomycin C injection at the 12-month mark are reported from 72.0% to 89.0% 16 and 91.0% at 21 months in nonirradiated populations. 17 In the irradiated population, patency rates were 76.0% at the 21-month mark. 17 Similarly, though with a smaller patient population of 24, patency rates after triamcinolone injection demonstrated rates of 83.0% at the 24-month mark. 18 Recently, the technique for DVIU with mitomycin injection was demonstrated in a video format specifically for prostatic or bladder neck urethral stenosis with incisions described at the 4 and 7 o’clock positions followed by 2 mg mitomycin C in 5 cc. 34
Although the data on efficacy of adjunct therapy for posterior urethral stenosis are not extensive, mitomycin C injection after urethral dilation for treatment of recurrent VUAS post-radical prostatectomy has been shown to be safe, and although long-term data are not yet present, 79.0% of the cohort in one study had a patent vesicourethral anastomosis at 12-month cystoscopy after single dilation and injection of mitomycin C. 19 Unfortunately, most of the data on adjuncts and DVIU are limited to 2 years or less follow-up, which limits its utility when counseling patients for long-term expectations.
Balloon dilation
Balloon dilation applies radial force along the stricture and is believed to cause less trauma, fracture scar tissue evenly circumferentially, and minimize compromise to the vascular supply of the urethral tissue. 35 In a systematic review investigating the success of balloon dilation, defined as no recurrence or no further stricture treatment during the follow-up period, only one study out of 15 targeted treatment of the posterior urethra, and three of these studies completely excluded the posterior urethra. 20 Studies that included both anterior and posterior urethral strictures analyzed these data together and therefore are not specific to the posterior urethra. In the single study that investigated only the posterior urethra, the etiology of the stricture was VUAS after radical prostatectomy. The success rate was defined as no evidence of re-stricture during 24-month follow-up, and success was at a rate of 80.0% in n = 10. 21
Drug-coated balloon dilation
DCB dilation is only approved by the Federal Drug Administration (FDA) in the United States for use in the anterior urethra. The recently published ROBUST III 2-year data have ensured that DCB will remain a mainstay for anterior strictures. As urologists become increasingly familiar and comfortable with using DCBs (Fig. 1), it is expected that individuals will expand the use of DCB to the posterior urethra. Data generated by performing paclitaxel balloon dilation in the posterior rabbit urethra demonstrated that the drug was delivered to the urothelial, submucosal, and smooth layers of the urethra immediately after dilation. 36 Paclitaxel targets tubulin, which disrupts metaphase of mitosis and triggers apoptosis of dividing cells. 37 When compared with mitomycin C, both chemotherapeutic agents target cellular division, though one could argue that mitomycin C may have a broader effect on cellular protein production when compared with paclitaxel.
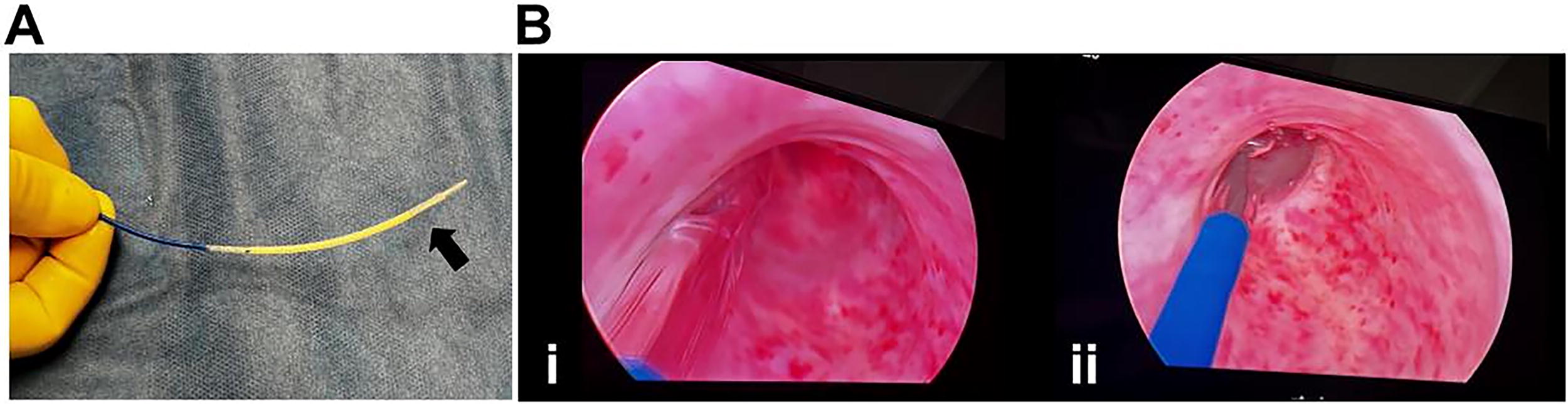
Treatment of urethral stricture with drug-coated balloon therapy.
A case report was published looking at a single patient’s course after treatment with DCB for recurrent BNC after DVIU and multiple mitomycin C treatments. 22 This patient had DCB treatment with dilation to 36F and was evaluated at 3 and 6 months post-procedure and was found to have minimal post-void residuals and minimal lower urinary tract symptoms (LUTS). This case report marked a novel application of DCB in the posterior urethra. A prospective cohort study examining DCB treatment for recurrent urethral stricture disease included three patients with vesicourethral anastomotic stricture after prostatectomy and one with a BNC within their cohort of 17. Similar success rates to those reported after treatment of the anterior urethra were reported, with 75.0% surviving free of recurrence at median follow-up of 30 months. 23 One patient in the posterior urethral stricture group had retreatment; she had had a urethral diverticulectomy prior to developing her stricture. If this female patient with BNS from urethral diverticulectomy is excluded, then the recurrence-free rate of the study is increased to 100% at the 3-month mark.
As DCB use expands through its recent FDA approval for treatment of benign prostatic hypertrophy, it is expected that closer to on-label use in the posterior urethra for BNSs and VUAS will also increase. In summary, although there is currently a paucity of published data to support posterior urethral stenosis, treatment with DCB is being increasingly utilized and will likely have increased published data in the coming years.
Treatment outcomes of posterior urethral strictures with DCB therapy may differ from anterior urethral stricture outcomes; however, more long-term data exist for DCB therapy of anterior strictures. The ROBUST III trial results led to FDA approval for treatment of DCB therapy of strictures in the anterior urethra, and it included adult males with anterior strictures <12F and less than 3 cm in length with at least two prior endoscopic treatments. One-year outcome results were measured by anatomical success and defined as the ability to pass a 16F flexible cystoscope or a 14F catheter through the treated area at 6 months. Freedom from repeat intervention evaluated at 1 year found 83% recurrence-free survival in the DCB cohort vs 21.7% in the standard balloon dilation cohort, p < 0.0001. 24 This was redemonstrated at the 2-year mark—treatment success was maintained with 77.8% in the DCB arm with freedom from intervention at the 2-year mark compared with 23.6% in the control arm. 38
Transurethral mucosal realignment
In 2021, the results of an efficacy trial for a new management strategy for BNC and VUAS were reported. The technique described was entitled TUMR and involves incising the bladder neck or VUAS at the 3 and 9 o’clock positions and using an endoscopic suturing device to bring normal mucosa across the defect in a similar fashion to the V-Y plasty, which is commonly performed robotically. 25 The study contained 19 patients in total, with a median age of 73 years. Repair of the stricture was defined as the ability to pass a 17F cystoscope at 4 months. The results of the study demonstrated that 89% of patients were stricture-free at 6 months. No de novo stress urinary incontinence or major complications were observed. A multi-institutional study of the technique is currently underway and will provide additional data in the coming years. Furthermore, longer-term data will likely be forthcoming from this cohort and have promise to further extend the reintervention rate compared with prior therapies.
In what amounts to an expansion of the TUMR, there are now examples of membranous urethral stricture urethroplasty being performed endoscopically. Though this article has not focused on membranous urethral strictures, it is not difficult to imagine extending the technique to the bladder neck in the case of more proximal stenoses.
In 2023, a video was published demonstrating the performance of endoscopic urethroplasty using buccal mucosal graft for male membranous urethral stricture disease. The patient had an 8 mm stricture at the membranous urethra; this was dilated and an approximately 1 cm wide strip of superficial mucosa was resected from the bladder neck past the area of stricture to create a graft bed. A buccal mucosal graft was harvested and sutured in place proximally and distally, as well as with endoscopic secure straps. The patient was discharged with a Foley catheter that was removed after 1 month. At the 3-month mark, the urethra was able to easily accommodate a flexible cystoscope. 26 As the ease of endoscopic suturing improves, buccal graft harvesting and endoscopic urethroplasty will be a part of advancing minimally invasive treatments for BNS and VUAS.
Strengths and limitations
The review evaluated literature from 2014 to 2024 but includes references to historical papers that provide a foundation to place current studies within their appropriate context. Outcome data of gold standard and more novel treatments of BNS and VUAS have been compared in a concise format. The review also provides insight into the impact of future studies by identifying where long-term data are lacking so as to better counsel patients in the clinic. Though our intention was to be inclusive and capture all literature referencing BNS, VUAS, and posterior urethral stenosis, we narrowed the focus of the review to predominantly exclude stenosis of the membranous urethra. In our analysis of the literature, we do not break down subjects along racial or ethnic lines. Most of the literature reviewed comes from Australian, American, European, and Asian patients, which may limit generalizability to posterior urethral disease in different clinical contexts.
Conclusion
The review evaluates the evolution and outcomes of minimally invasive treatment options for posterior urethral stenosis, focusing specifically on BNS and VUAS. The current gold standard for treatment of VUAS/BNS continues to be transurethral incision; however, success rates vary widely. DCB dilation and transurethral membrane realignment will likely be offered more frequently, and long-term data may show more prolonged time until recurrence with these therapies. Development of novel alternative treatments is beneficial, as open and robotic repairs of the VUAS and BNS can be technically challenging and pose greater morbidity to the patients. More data are necessary to determine long-term success, but there is great potential for improvement over standard methods of stenosis treatment in the coming years.
Footnotes
Authors’ Contributions
C.N.H.: Data curation (equal), project administration (equal), resources (equal), writing—original draft (equal), and review and editing (equal). T.D.: Data curation (equal), project administration (equal), resources (equal), writing—original draft (equal), and review and editing (equal). M.F.M.: Conceptualization (lead), writing—review and editing (equal), and supervision (lead).
Author Disclosure Statement
The authors of this article have nothing to disclose.
Funding Information
No funding was received for this article.