
Abstract
Background:
Bladder outlet obstruction (BOO) and urinary retention were recognized contributing factors to bladder cancer (BCa) recurrence and progression due to prolonged urothelial exposure to carcinogens, chronic inflammation, and incomplete bladder emptying. Holmium laser enucleation of prostate (HoLEP) is a minimally invasive and highly effective procedure that completely removes obstructive prostatic tissue, thus resolving BOO. To explore the HoLEP impact on BCa recurrence and progression by improving voiding dynamics and reducing post-void residual (PVR).
Materials and Methods:
We carried out a retrospective case-control study, based on a multicenter prospectively maintained database, on 100 consecutive male patients (cases) with a first diagnosis of non-muscle-invasive bladder cancer, with BOO and urinary retention and treated with HoLEP (in case of at least 3-months of timor-free status). The cases were compared with 200 patients (controls) with same baseline characteristics but not treated with HoLEP. We evaluated PVR, International Prostatic Symptoms Score—IPSS, BCa recurrence and progression rates. The t-Test, χ2-test, logistic correlations, multivariate analysis were applied to evaluate the association between the BOO resolution and urinary retention by HoLEP and BCa recurrence and progression.
Results:
Patients treated with HoLEP showed a significant PVR reduction compared with controls (p < 0.01). The HoLEP group demonstrated statistically significant improvements in IPSS scores, indicating better urinary symptom control. The rates of recurrence and progression were significantly lower in the HoLEP-treated group (p < 0.01). Multivariate analysis identified the BOO resolution by HoLEP as an independent predictor of reduced BCa recurrence (odds ratio 0.65, 95% CI 0.45–0.85, p < 0.001). The control group exhibited persistently elevated PVR and higher rates of BCa recurrence and progression.
Conclusions:
Urinary retention could represent a prognostic factor of treatment response, and its active treatment by HoLEP should be considered as an important therapeutic step in the clinical management of patients with BCa.
Keywords
Introduction
Bladder cancer (BCa) is among the most common malignancies affecting the urinary tract, with non-muscle-invasive bladder cancer (NMIBC) comprising the majority of cases. Despite advances in diagnostic and therapeutic strategies, NMIBC remains a disease with high recurrence rates. 1
Bladder outlet obstruction (BOO) and urinary retention have been recognized as contributing factors to BCa recurrence and progression due to prolonged urothelial exposure to carcinogens, chronic inflammation, and incomplete bladder emptying.2,3
Urinary retention is recognized as a promoting factor for BCa, but its role as a prognostic factor for therapeutic response has not yet been widely considered. There is growing evidence that bladder outlet characteristics, particularly postvoid residual (PVR), may correlate with short- and long-term response to treatment in NMIBC.4,5
Holmium laser enucleation of the prostate (HoLEP) is a minimally invasive and highly effective procedure that completely removes obstructive prostatic tissue, thus resolving BOO and optimizing urinary flow. 6
This article explores the impact of HoLEP on BCa recurrence and progression, particularly by improving voiding dynamics and reducing PVR volume, a recognized prognostic factor for treatment response in non-muscle-invasive bladder cancer (NMIBC).
Materials and Methods
We carried out a retrospective case-control study based on a multicenter prospectively maintained database. The study was approved by the Institutional Review Board (ID number 174/2025).
We evaluated 100 consecutive male patients (cases) with diagnosis of NMIBC, with BOO and urinary retention, and therefore treated with HoLEP (after at least 3 months of tumor-free status after standard treatment). The cases were compared with 200 patients (controls) with the same baseline characteristics with BOO and urinary retention but not treated with HoLEP.
A detailed flow-chart of the patient selection and exclusion process is presented in Figure 1.
We evaluated baseline and bladder-outlet characteristics [“functional parameters”: PVR volume, International Prostatic Symptoms Score (IPSS), 7 perceived quality of bladder outlet], the rate of recurrence, and progression of BCa.
Patients were selected according to their outcome (disease status after standard treatment for NMIBC). Patients and controls who fulfilled the inclusion and exclusion criterion were enrolled. Controls were extracted from the same population base so as to be representative of the population from which the cases were obtained. Two control groups were enrolled for every case (ratio of 2:1).
The inclusion criterion were as follows: patients who were treated for the first diagnosis of NMIBC with standard treatment and with proven tumor-free status after at least 3 months from the last treatment, cancer management according to international guidelines, pure urothelial cancer, detrusor muscle included in resection specimen, patients who did not receive BOO-surgical therapeutic indications before, complete follow-up, and signed consent.
The exclusion criteria were as follows: patients undergoing BOO treatment at the time of transurethral resection of bladder tumor (TURB-T); patients with residual/recurrent disease at the second resection (patients considered with the highest risk of short-term recurrence/progression); BCa involving the urethra or upper urinary tract; patients not treated according to international guidelines or treated with off-label agents; previous pelvic radiotherapy; previous systemic chemotherapy; known immune deficiency; active/uncontrolled urinary infections; liver, kidney, or hematological function disorders; coexistence of other primary tumors; and inability to participate.
Disease-free status was defined as the absence of any histologically/clinically proven neoplastic recurrence or progression, including voiding/washing of urinary cytology negative for high-grade urothelial carcinoma and negative radiological imaging of the upper urinary tract.
Patients were categorized into three risk categories according to neoplastic characteristics: low, intermediate, and high risk. 1 The 2009 TNM classification 8 and 2004 World Health Organization grading system 9 were used.
All patients underwent TURB-T and a second resection for high-grade pTa and pT1 tumors.
Patients underwent disease management according to European Association of Urology guideline recommendations: low-risk patients underwent one immediate instillation of intravesical chemotherapy (mitomycin C [MMC]) after TURB-T; intermediate-risk patients underwent one immediate instillation of intravesical chemotherapy (MMC) after TURB-T, followed by an induction course with intravesical chemotherapy (MMC); and high-risk patients underwent an intravesical induction course with Bacillus Calmette-Guérin (BCG).
The chemotherapy induction course consisted of 8 weeks of MMC instillations (40 mg diluted in 40 mL of sterile water), and the immunotherapy induction course consisted of 6 weeks of BCG instillations. MMC and BCG were introduced into the bladder via a 10 F to 12 F urethral catheter, and patients were instructed to not pass urine for 2 hours.
The first follow-up visit was performed 3 months after TURB-T in low-risk patients and at least 45 days after the induction of intravesical therapy in intermediate- and high-risk patients.
We recorded the following baseline characteristics: age, sex, American Society of Anesthesiologists Classification, Charlson Comorbidity Index, Eastern Cooperative Oncology Group Performance Status, and body mass index.
We recorded bladder-outlet characteristics (defined as “functional”): PVR and IPSS.
Postvoid residual was calculated twice by ultrasonography performed on two different days before TURB-T; the final value was calculated as the mean between the two values. The IPSS was applied and recorded before TURB-T.
We compared patients according to baseline and functional characteristics. The primary end point consisted of the correlation between the non-tumor-free status and PVR in the two groups at the first follow-up visit. Secondary endpoints were the correlation between PVR and risk categories and the correlation of other functional parameters (IPSS) with no tumor-free status.
As no definitive definition of pathological PVR was stated in literature, we based it on previous experience 4 and we assumed a PVR >50 cc as a reference to consider and screen patients for the study.
The patients underwent surgery and/or follow-up at Veneto Institute of Oncology-Department of Urology, Policlinico Abano Terme-Department of Urology, Abano terme, Italy; Humanitas University-Department of Urology, Bergamo, Italy, and the contribution of the centers was almost identical.
Categorical variables were summarized using actual counts and percentages, and continuous variables were summarized using median ± standard deviation. Parametric and nonparametric variables were evaluated using t-tests and χ2 tests. The correlation between the individual factors and the non-tumor-free status after therapy at the first follow-up was evaluated by univariate analysis (Pearson χ2 test). 10 A multivariate logistic regression analysis was performed for factors associated with no tumor-free status in the univariate analysis. Statistical significance was set at p < 0.05.
By assuming that the HoLEP procedure should lead to a reduction of at least 10% in the rate of bladder tumor recurrence, as reported by Kamat et al., 11 and that almost 50% of patients with BCa experience a recurrence after 36 months of follow-up, by using an alpha cutoff of 5% (0.05) and a beta cutoff of 20% (0.2), the minimum number of subjects for adequate study power was 69 in group 1 (cases) and 138 in group 2 (controls).12,13
In a post hoc power calculation, it was 100% according to the complete response rate for carcinoma in situ or recurrence-free rate for papillary tumors of at least 25% at 18 months as recommended by the International Bladder Cancer Group. 11
Results
Patients’ characteristics were summarized in Table 1.
Baseline Characteristics
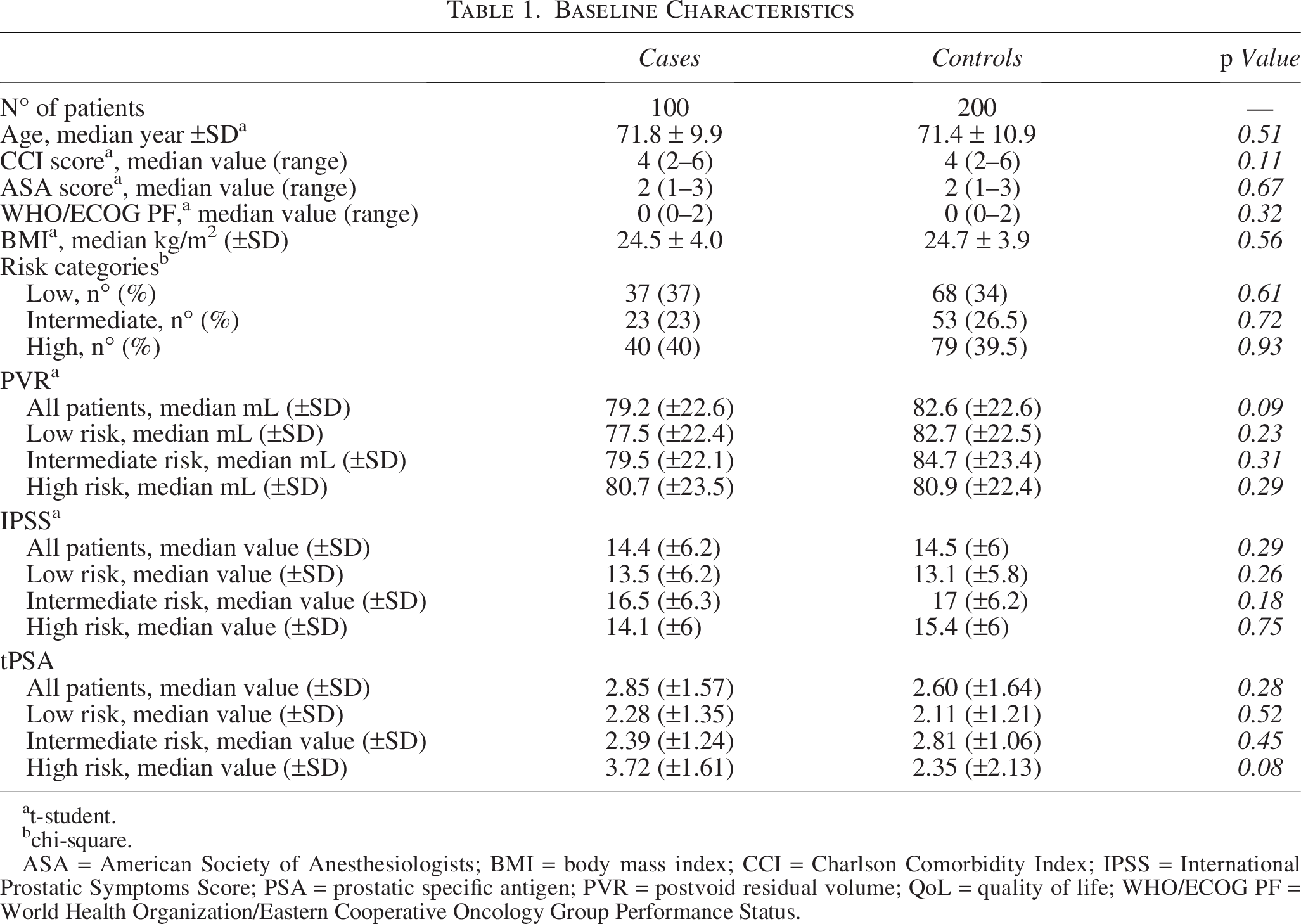
t-student.
chi-square.
ASA = American Society of Anesthesiologists; BMI = body mass index; CCI = Charlson Comorbidity Index; IPSS = International Prostatic Symptoms Score; PSA = prostatic specific antigen; PVR = postvoid residual volume; QoL = quality of life; WHO/ECOG PF = World Health Organization/Eastern Cooperative Oncology Group Performance Status.
Patients who underwent HoLEP experienced a significant improvement in bladder emptying parameters compared with those who did not receive surgical intervention for BOO. The mean PVR volume in the HoLEP-treated group was significantly lower than that in the control group (p < 0.01). In addition, the IPSS showed marked improvement in patients who underwent HoLEP, with a significant reduction in lower urinary tract symptoms (p < 0.01) (Table 2, Figs. 2–4).
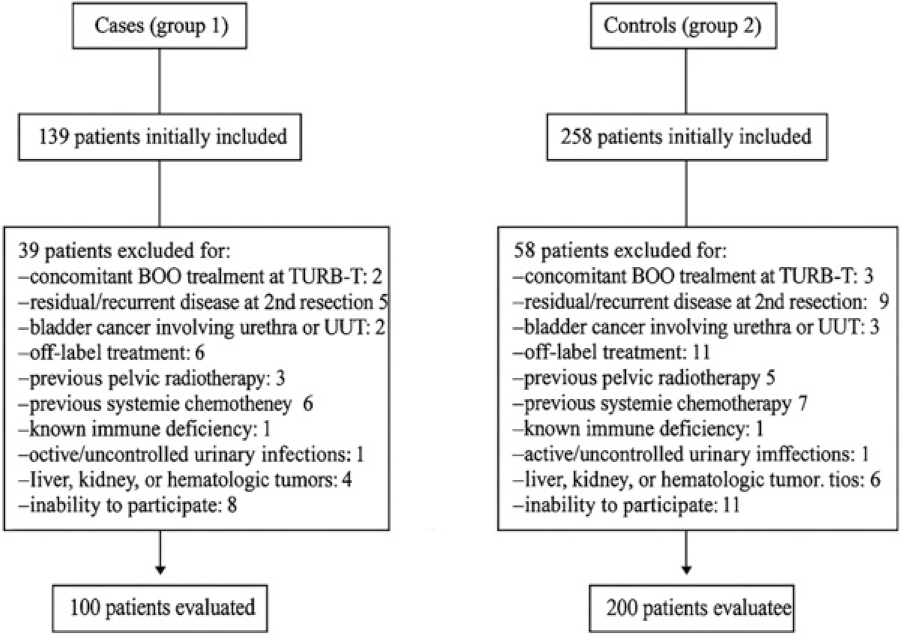
Flow-chart.
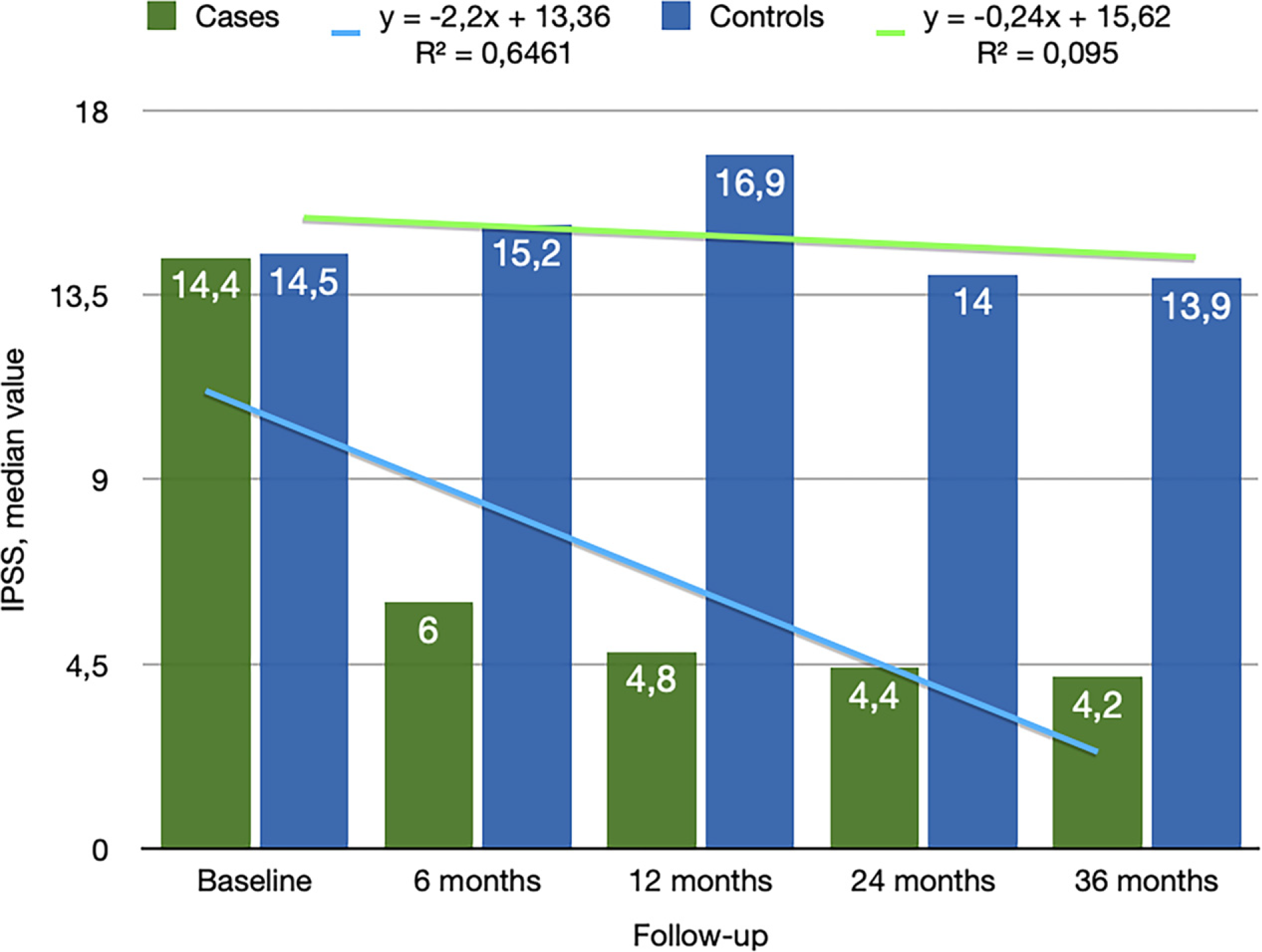
IPSS trend by considering all patients. IPSS = International Prostatic Symptoms Score.
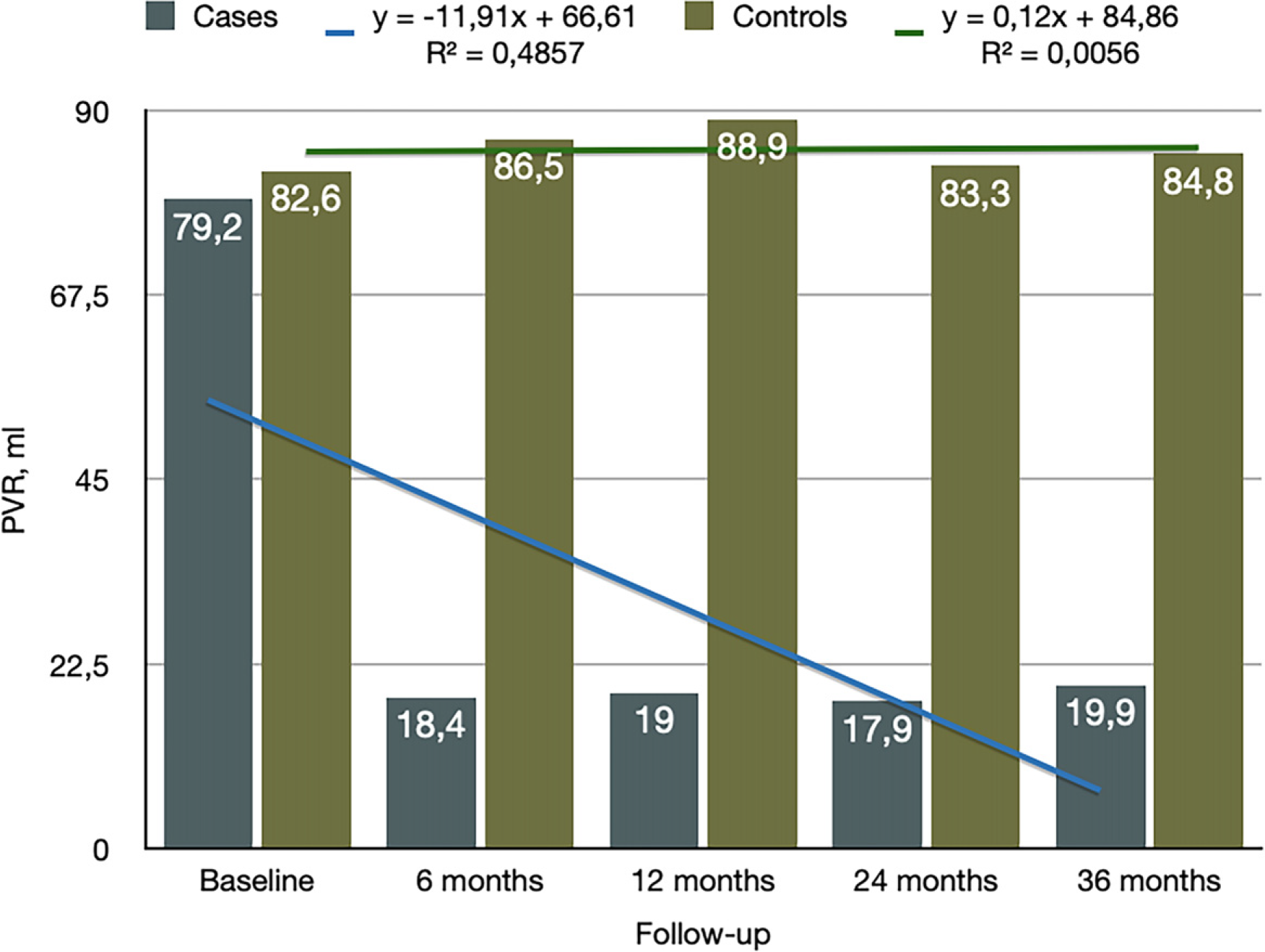
PVR trend by considering all patients. PVR = post-void residual.
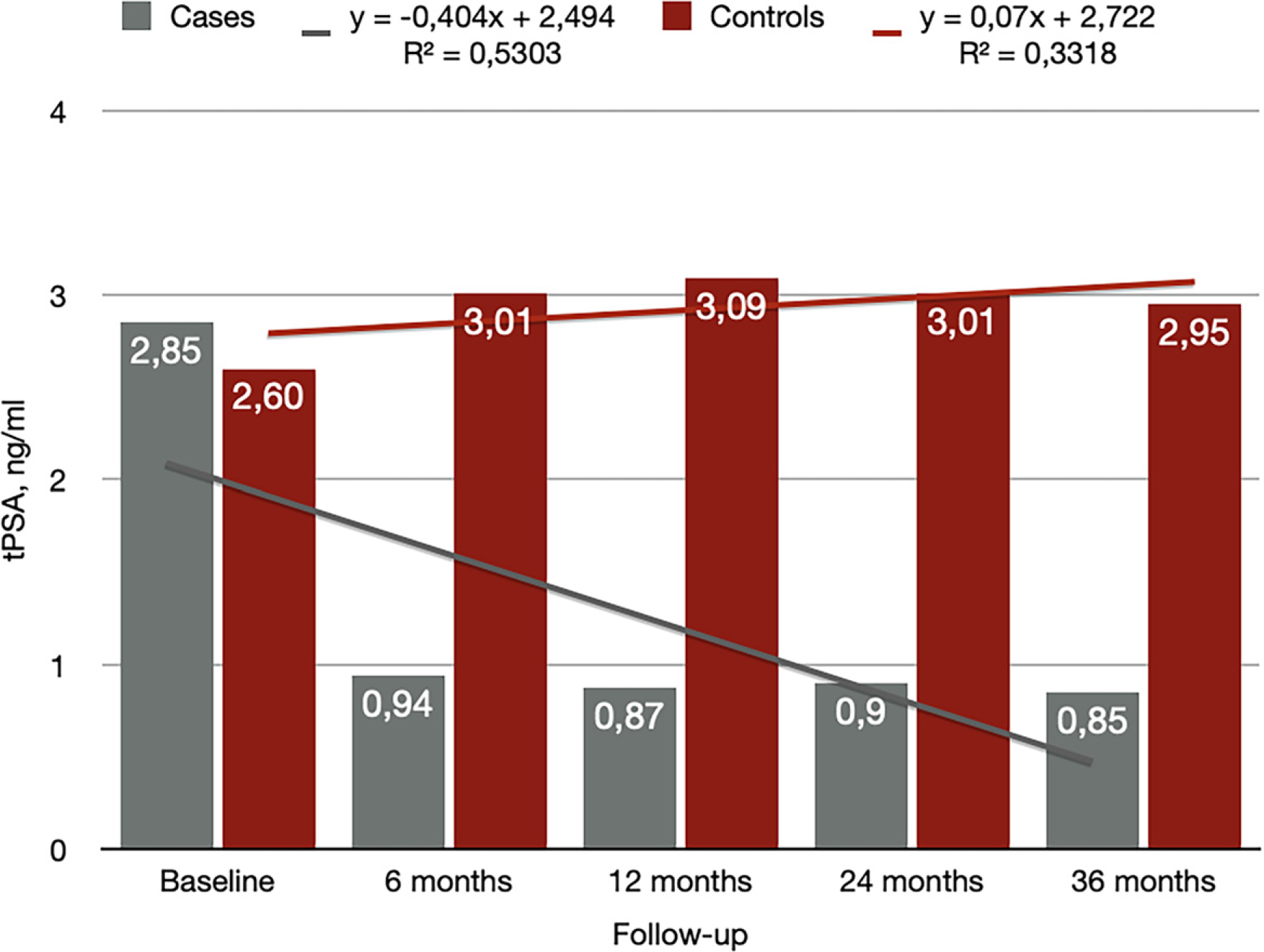
PSA trend by considering all patients. PSA = prostatic specific antigen.
Clinico-Pathological Characteristics
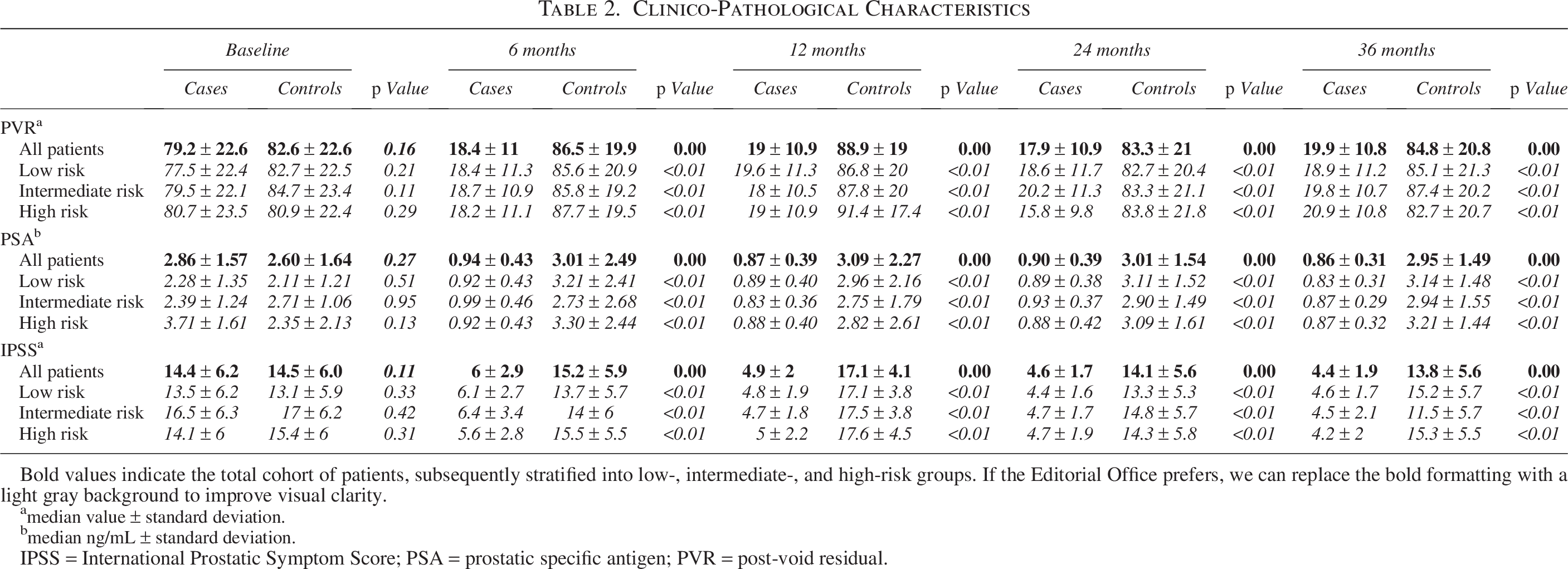
Bold values indicate the total cohort of patients, subsequently stratified into low-, intermediate-, and high-risk groups. If the Editorial Office prefers, we can replace the bold formatting with a light gray background to improve visual clarity.
median value ± standard deviation.
median ng/mL ± standard deviation.
IPSS = International Prostatic Symptom Score; PSA = prostatic specific antigen; PVR = post-void residual.
In terms of BCa, the recurrence free survival and the progression free survival rates at 3-year follow-up were significantly higher in the HoLEP-treated group than in the control group (75% vs. 44%, p < 0,05 log-rank >3.84, Fig. 5c, and 97.9% vs 91.5%, p < 0,05 log-rank >3.84, Fig. 5d, respectively).
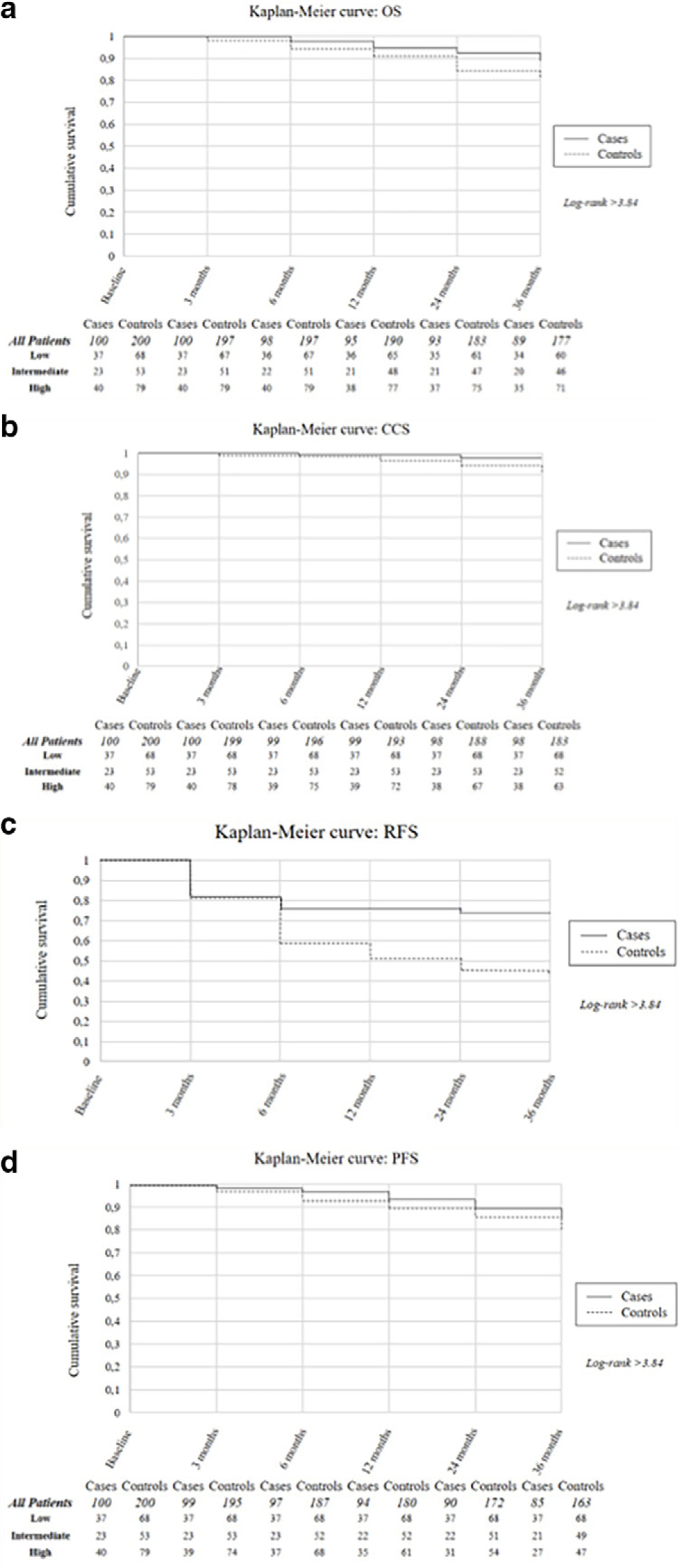
Kaplan Maier survival curves:
In terms of overall survival and cancer specific survival, we reported rates of 89% vs 88,5%, p < 0,05 log-rank >3.8, Figure 5a, and 98% vs 91,5%, p < 0,05 log-rank >3.8, Figure 5b, respectively.
Multivariate analysis identified the resolution of BOO via HoLEP as an independent predictor of reduced BCa recurrence (odds ratio 0.65, 95% CI 0.45–0.85, p < 0.001).
Discussion
The findings of this study aimed to highlight the potential therapeutic role of HoLEP in patients with NMIBC with concomitant BOO. BOO has long been associated with an increased risk of BCa recurrence due to its impact on chronic urinary stasis, urothelial exposure to carcinogens, and persistent bladder inflammation. Our study supports the hypothesis that resolving BOO through HoLEP may mitigate these risk factors and contribute to better oncologic outcomes in patients with NMIBC.
Several previous studies have established the detrimental effects of urinary retention and BOO on BCa outcomes. Suzuka et al. reported that high PVR volumes were strongly associated with increased NMIBC recurrence rates, corroborating our findings. 14
Existing studies have explored the relationship between BOO, its treatment, and BCa outcomes. A study investigated the effect of BOO on BCa recurrence and progression. The findings indicated that BOO did not significantly affect disease recurrence or progression, nor did it influence the pathological features of the tumor at diagnosis. However, increased bladder trabeculation resulting from BOO was associated with higher-grade tumors at initial diagnosis. 5 Another study evaluated the association between PVR, a common consequence of BOO, and response to standard therapy in patients with NMIBC. The study found that higher PVR was associated with a reduced response to standard therapy, suggesting that managing BOO to reduce PVR might improve treatment outcomes. 4 While direct evidence linking surgical intervention for BOO to reduced NMIBC progression is limited, these studies highlight the potential impact of BOO and its management on BCa outcomes.
The mechanism by which HoLEP influences BCa recurrence is multifactorial. First, HoLEP effectively eliminates BOO, thereby reducing urinary stasis and enhancing the clearance of carcinogens from the bladder. Second, improved bladder emptying may reduce chronic inflammation, which has been implicated in the carcinogenic process and tumor microenvironment of NMIBC.2–6 Finally, by optimizing voiding dynamics, HoLEP enhances the effectiveness of intravesical therapies such as MMC and Bacillus Calmette-Guérin (BCG), which rely on adequate drug distribution and retention within the bladder.
BCa and its treatments, particularly intravesical therapy, have a well-documented impact on urinary function. The interplay between the disease, treatment-induced inflammation, and underlying bladder dysfunction significantly affects lower urinary tract symptoms (LUTS) and overall quality of life in patients.
BCa itself contributes to LUTS due to tumor-related inflammation, urothelial irritation, and, in some cases, obstruction of the bladder outlet. Common symptoms include: Increased urinary frequency and urgency, 15 Dysuria (painful urination), 16 Hematuria (blood in urine), often a primary presenting symptom, 17 Nocturia and incomplete bladder emptying due to bladder wall changes. 18 Patients with NMIBC frequently report these symptoms before diagnosis, and they often persist or worsen after treatment.
Intravesical Bacillus Calmette-Guérin (BCG) is the gold-standard immunotherapy for intermediate- and high-risk NMIBC. 17 However, BCG induces a robust immune response, leading to significant urinary toxicity, including urinary frequency and urgency in up to 80% of patients, 19 dysuria and hematuria in 50% of cases, 20 BCG-related cystitis, which can persist after treatment 21 ; and rarely, systemic BCG infection leading to granulomatous prostatitis or orchitis. 22 These symptoms typically peak during the induction phase and may persist in patients undergoing maintenance therapy.
Intravesical chemotherapy (e.g., MMC, epirubicin) has a direct cytotoxic effect on BCa cells but also causes significant urothelial irritation. 23 Chemical cystitis is a common side effect, leading to increased frequency, urgency, and bladder pain. 24 In some patients, prolonged inflammation results in detrusor overactivity and urgency incontinence. 25 Urinary symptoms may persist for several weeks posttreatment due to urothelial damage. 26
Persistent LUTS after intravesical therapy represent a significant concern, as they may lead to long-term complications such as reduced bladder compliance and fibrosis due to chronic inflammation, an increased risk of bladder dysfunction resulting in secondary incontinence, and progressive deterioration of voiding function in patients with preexisting BOO. 19
For patients with NMIBC with concurrent BOO, treatment-related LUTS can be further exacerbated. HoLEP, a minimally invasive approach to resolving BOO, may provide substantial benefits by: Reducing PVR volume, thereby decreasing urinary stasis and inflammation, 27 Improving bladder emptying, which may lower the risk of persistent LUTS after intravesical therapy, 28 Potentially reducing NMIBC recurrence by minimizing chronic urothelial irritation and exposure to carcinogens. 29
The relationship between BCa, intravesical therapy, and urinary symptoms is complex, with significant implications for patient management. While intravesical therapy remains essential in NMIBC treatment, its impact on bladder function must be carefully monitored. In patients with concomitant BOO, HoLEP represents a promising intervention to alleviate LUTS, improve treatment tolerance, and potentially contribute to better oncological outcomes by reducing chronic inflammation and urinary stasis.
In addition to oncologic benefits, HoLEP offers several advantages over other surgical treatments for BOO, such as transurethral resection of the prostate. Multiple studies demonstrated that HoLEP provides superior long-term outcomes in terms of symptom relief, urinary flow improvement, and reduced risk of reoperation. 30
While this study underscored the promising role of HoLEP in improving functional and oncologic outcomes in patients with NMIBC with concomitant BOO, it is crucial to recognize that the observed benefits likely stem from the relief of obstruction itself, rather than the specific laser technique employed. Evidence from comparative urodynamic studies suggests that more complete anatomical deobstruction—regardless of the method—correlates strongly with symptomatic improvement and enhanced lower urinary tract function. For example, HoLEP demonstrated the most robust improvements in bladder outlet obstruction index (BOOI) among surgical interventions, but other forms of anatomical endoscopic adenomectomy such as ThuLEP, GreenLEP, or BipolEP have shown similar deobstructive efficacy when performed thoroughly. 31
The variability in treatment outcomes among different modalities is often attributed to differences in the degree of obstruction relief, baseline bladder dysfunction, and patient selection. As supported by a recent systematic review, the magnitude of BOO relief is a primary determinant of clinical improvement, rather than the specific energy source or surgical platform used. This is further corroborated by findings that even medical therapies such as α-blockers improve LUTS to a lesser extent and with less durable BOOI reduction, highlighting the unique impact of anatomical deobstruction on voiding efficiency.
Therefore, in the context of NMIBC, where chronic urinary retention and incomplete bladder emptying are increasingly recognized as contributors to recurrence and intravesical therapy failure, any intervention capable of achieving substantial relief of BOO may offer similar oncological benefits. Future studies should focus not only on laser type but also on the completeness of obstruction relief and its impact on intravesical therapy tolerance, recurrence rates, and bladder function recovery.
While our study provides compelling evidence supporting the role of HoLEP in improving NMIBC outcomes, certain limitations should be acknowledged. The nature of this multicentric study was retrospective; the study was conducted with a relatively short follow-up period, and long-term recurrence and progression rates require further evaluation. In addition, while we accounted for major confounding factors, prospective randomized trials would be necessary to establish a definitive causal relationship between HoLEP and improved NMIBC prognosis.
Conclusion
Urinary retention could represent a prognostic factor of treatment response in BCa, and its active treatment should be considered an important therapeutic step in clinical management.
HoLEP, by definitively resolving BOO and urinary retention, presents a promising therapeutic approach to reducing BCa recurrence and progression. By optimizing voiding parameters, decreasing chronic urothelial irritation, and mitigating inflammatory pathways, HoLEP may contribute to better oncological outcomes in patients with NMIBC. Given the strong association between urinary retention and tumor recurrence, integrating HoLEP into the comprehensive management of patients with NMIBC with BOO may lead to improved oncologic and functional outcomes. Further prospective multicentric studies and randomized controlled trials are warranted to establish a direct link between HoLEP and reduced BCa recurrence, but current evidence strongly supports the role of BOO treatment in comprehensive BCa management.
Authors’ Contributions
Conceptualization: D.L. and M.F.; methodology: D.L. and M.F.; validation: B.G.M.; formal analysis: D.L. and M.F.; investigation: D.L., C.F., S.F., D.D., and G.M.; resources: D.L.; data curation: S.F., C.F., and D.D.; writing—original draft preparation: D.L. and M.F.; writing—review and editing: S.F., D.D., and G.M.; visualization: D.D. and A.A.; supervision: P.A., B.G.M., C.A., and A.A.; project administration: P.A. All authors have read and agreed to the published version of the article.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research did not receive any funding to cover publication costs.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Humanitas Gavazzeni e Castelli for studies involving humans (ID number 174/2025).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.