
Abstract
Introduction:
Accurate estimation of nephrostomy tract length is crucial for planning percutaneous nephrolithotomy (PCNL) access site and required tools, yet data are limited for supine PCNL. This study compared real-time intraoperative tract lengths with preoperative CT-based estimations using two techniques: a novel CT-anatomical technique and the S.T.O.N.E. nephrolithometry-based technique.
Methods:
In a prospective single-surgeon cohort, patients undergoing supine PCNL between March and June 2025 were included. Preoperative CT-based tract lengths were measured using the CT-anatomical and S.T.O.N.E. techniques and were compared to real-time intraoperative measurements in a blinded manner. Paired comparisons used the Wilcoxon signed-rank test, while mean squared error (MSE) and intraclass correlation coefficients (ICC) assessed accuracy and reliability. Correlation analyses and multivariable regression identified predictive factors and generated a model for improved tract length estimation.
Results:
Of 47 eligible cases, 33 met the inclusion criterion. Both CT-based methods significantly overestimated the real-time intraoperative tract length (mean intraoperative: 9 ± 2.5 cm vs CT-anatomical: 11.2 ± 2.7 cm and S.T.O.N.E.: 11.4 ± 2.2 cm). The CT-anatomical method showed better agreement with intraoperative values (MSE = 10.42, ICC = 0.42) than S.T.O.N.E. (MSE = 11.18, ICC = 0.35). A multivariable linear model incorporating body mass index, access site level, CT positioning, and CT-anatomical length was used to develop an easy-to-use calculator that accurately predicts the actual intraoperative tract length from the preoperative CT measurement (MSE = 3.64, ICC = 0.58; p < 0.001).
Conclusion:
CT-based tract lengths often overestimate actual intraoperative values in supine PCNL, suggesting that true tract lengths in the supine position are shorter than previously believed. Preoperative accuracy can be enhanced using our newly developed predictive formula.
Introduction
Nephrostomy tract length is an important consideration prior to percutaneous nephrolithotomy (PCNL) and can be affected by the amount of subcutaneous fat, retroperitoneal fat, and back musculature. 1 The point at which an access sheath enters the renal parenchyma serves as a fulcrum, which later enables maneuverability within the collecting system; a longer tract length, therefore, may make nephroscopy more challenging to perform and may influence PCNL treatment success, including stone clearance rates. 2 The S.T.O.N.E. nephrolithometry score, first proposed by Okhunov et al., incorporates five variables, including tract length, to predict both stone-free rates and the risk of perioperative complications. In their study, the authors found the S.T.O.N.E. score correlated with operative times, procedural blood loss, length of hospital stay, and postoperative stone-free status. A tract length >10 cm was considered to negatively impact the outcomes. 2 This scoring system was later externally validated in a separate cohort of PCNLs. 3 These studies have been validated primarily for prone PCNL, but no robust comparative studies have evaluated the impact of tract length on supine PCNL outcomes.
Over the years, various techniques have been proposed for CT-based preoperative tract length measurement, including: the distance between the skin and the lateral edge of the calyx at a 25°–30° angle from a vertical line extending from the anterior abdomen to the spinous process, 1 the vertical average distance from the center of the stone to the skin measured at 0°, 45°, and 90° angles (used for tract length in the S.T.O.N.E. nephrolithometry score), 2 and the distance from the skin to the most lateral midpole calyx. 4 Given that at our institution most PCNL procedures are performed in the supine position using an ultrasound-guided approach, we developed a novel CT-based measurement technique (CT-anatomical length) more aligned with the anatomical trajectory of this access.
Several factors were found to influence preoperative tract lengths. CT positioning had a significant impact, with the prone position yielding the shortest tract length, followed by the supine oblique and then the straight supine position.5,6 Additionally, a well-established association between higher body mass index (BMI) and longer tract lengths is attributed to increased subcutaneous adipose tissue. 7 Body wall compliance has also been touted as a contributor to tract length differences, with the anterior abdominal wall believed to be more pliable as compared with the more muscular posterior body wall. 2 All these factors may affect the prediction accuracy and reliability of the preoperative measurements.
To our knowledge, no previous study has examined the association between preoperative CT-based and real-time intraoperative PCNL tract lengths. The primary objective of this study was to compare intraoperative tract lengths with preoperative measurement techniques in supine PCNLs and to evaluate whether preoperative measurements consistently over- or underestimate true intraoperative values.
Methods
Study design
The study is a single-center prospective observational cohort (IRB# STUDY-14–00879) of patients undergoing US-guided supine PCNL between March 13, 2025, and June 6, 2025, by a single surgeon (M.G.). Exclusion criteria were defined to minimize measurement bias and included: prone position, fluoroscopy-guided access, lack of appropriate CT images for accurate measurements, surrounding organs interposition on CT scan interrupting with the measurements, significant abnormal anatomy (e.g., duplication, malrotation, horseshoe kidney, scoliosis), and imaging-to-surgery intervals exceeding 6 months. These criteria were selected to minimize measurement bias that may have influenced the results. We decided that patients with interposing organs, primarily referring to the colon, will be excluded, as it is impossible to simulate on CT the medial movement of the colon seen on ultrasound in the supine PCNL position.
In this study, we utilized two distinct CT-based techniques to estimate preoperative tract lengths: CT-anatomical tract length based on coronal CT images and a technique based on the S.T.O.N.E. nephrolithometry score (S.T.O.N.E. tract length). These were compared to a real-time intraoperative measurement, conducted in a blind manner. During PCNL, the intraoperative tract length was measured by the operating surgeon (M.G.) immediately after access was obtained with the sheath, blinded to any informal preoperative estimates to minimize bias. The intraoperative selected calyx and relativeness to ribs were documented and communicated to a single independent investigator (Z.S.) at the conclusion of the surgical procedure. The CT-based measurements were subsequently measured on the preoperative imaging based on this information by the single independent investigator, who was blinded to the intraoperative tract length at all times. Therefore, the preoperative tract length was measured retrospectively after the surgical procedure to simulate the actual calyx used during the surgical procedure.
For the sample size calculation, we set a statistical power of 80% and a significance level (α) of 0.05. Based on prior studies reporting a mean preoperative tract length of 9 cm with a standard deviation of 1.3 cm, 8 we selected a minimum detectable difference of 1 cm. Under these assumptions, the required sample size was estimated to be at least 22 paired comparisons. After achieving this sample size and collecting all tract length data, statistical analyses were conducted.
Measurement techniques
Intraoperative real-time tract length (Fig. 1)
Intraoperative tract length was measured using a ruler and the access sheath (Nephromax, BSC). After performing balloon dilatation of the nephrostomy tract and following entry into the collecting system with the sheath, the shorter side of the beveled tip of the sheath was positioned at the cutting edge, and the external portion of the sheath remaining outside the body was measured. This external length was subtracted from the total 16.5 cm sheath length to determine the true intrabody tract length.
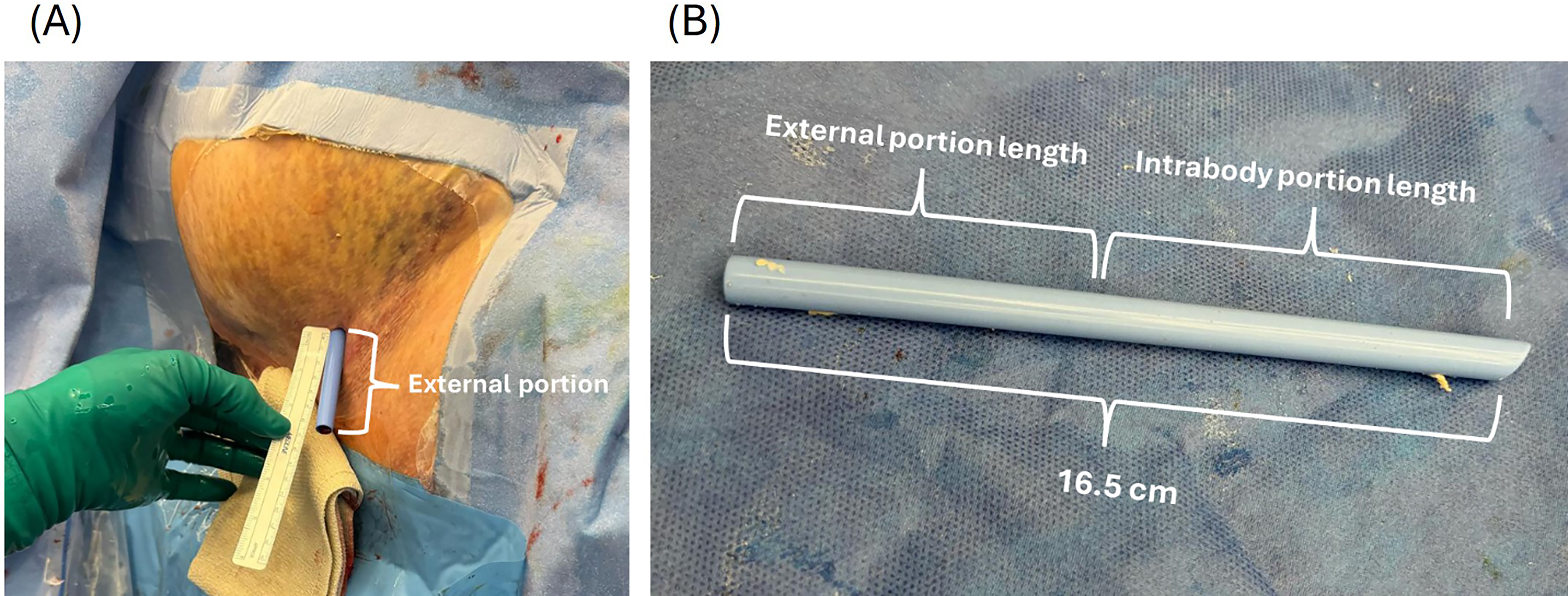
Intraoperative real-time tract length measurement.
Preoperative CT-anatomical tract length technique (Fig. 2)
To provide a more anatomically aligned measurement in the supine position, we used coronal CT sections, which better reflect the trajectory of the ultrasound-guided access tract (Fig. 2A). The tract length for lower pole calyces was measured from the skin surface to the edge of the papilla as a straight line passing through the calyceal infundibulum. For interpolar and upper calyces, tract length was measured from the skin surface to the edge of the papilla, along a straight perpendicular line, with adjustments made for any interposed organs as needed (Fig. 2B). The calyx used for preoperative measurements was selected based on the actual access site achieved during the procedure.
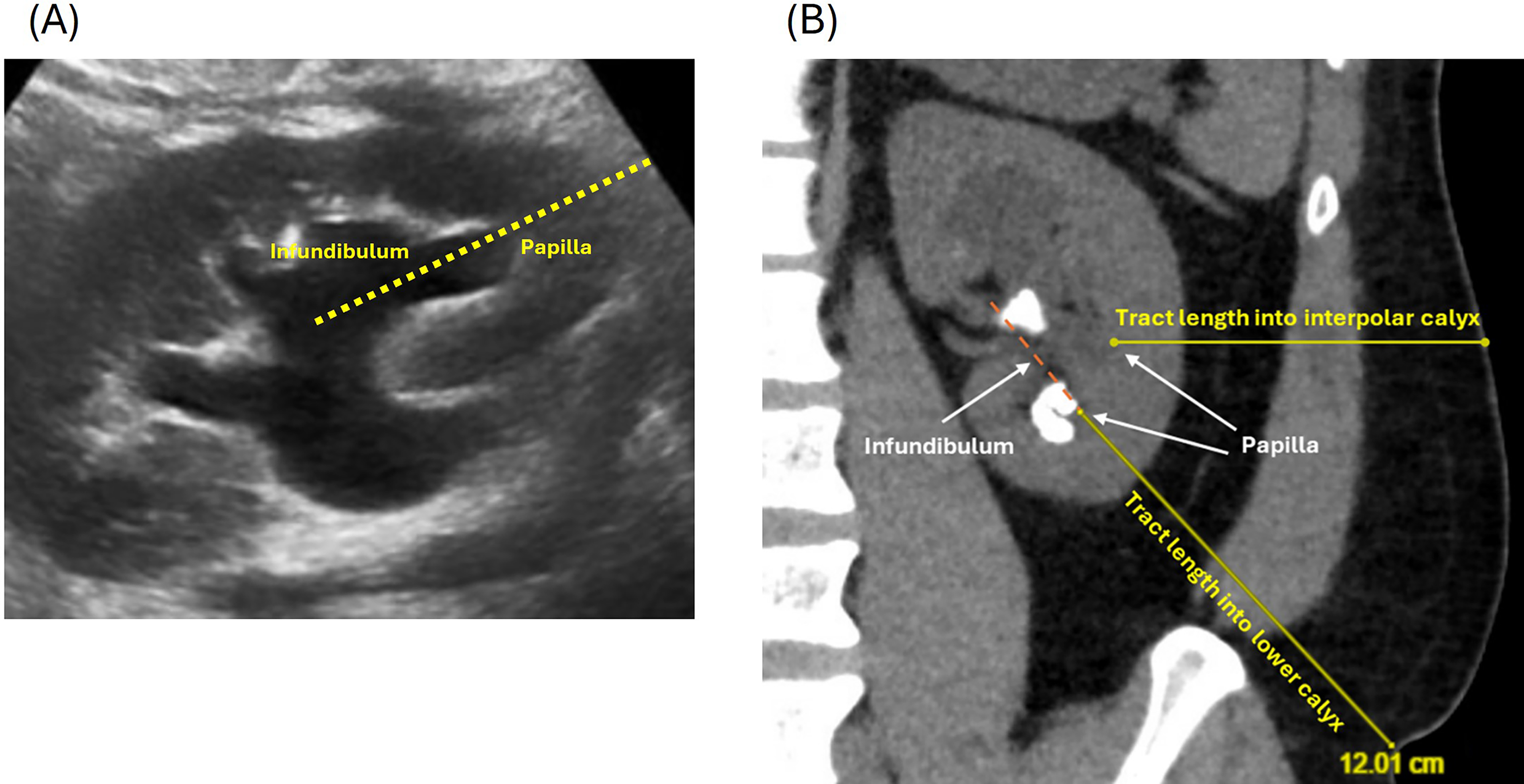
Preoperative CT-anatomical tract length technique.
Preoperative S.T.O.N.E. tract length technique (Fig. 3)
According to Okhunov et al., the tract length measurement in the S.T.O.N.E. nephrolithometry tool is defined as the average vertical distance from the center of the stone to the skin, measured at 0°, 45°, and 90° angles on the axial section. 2
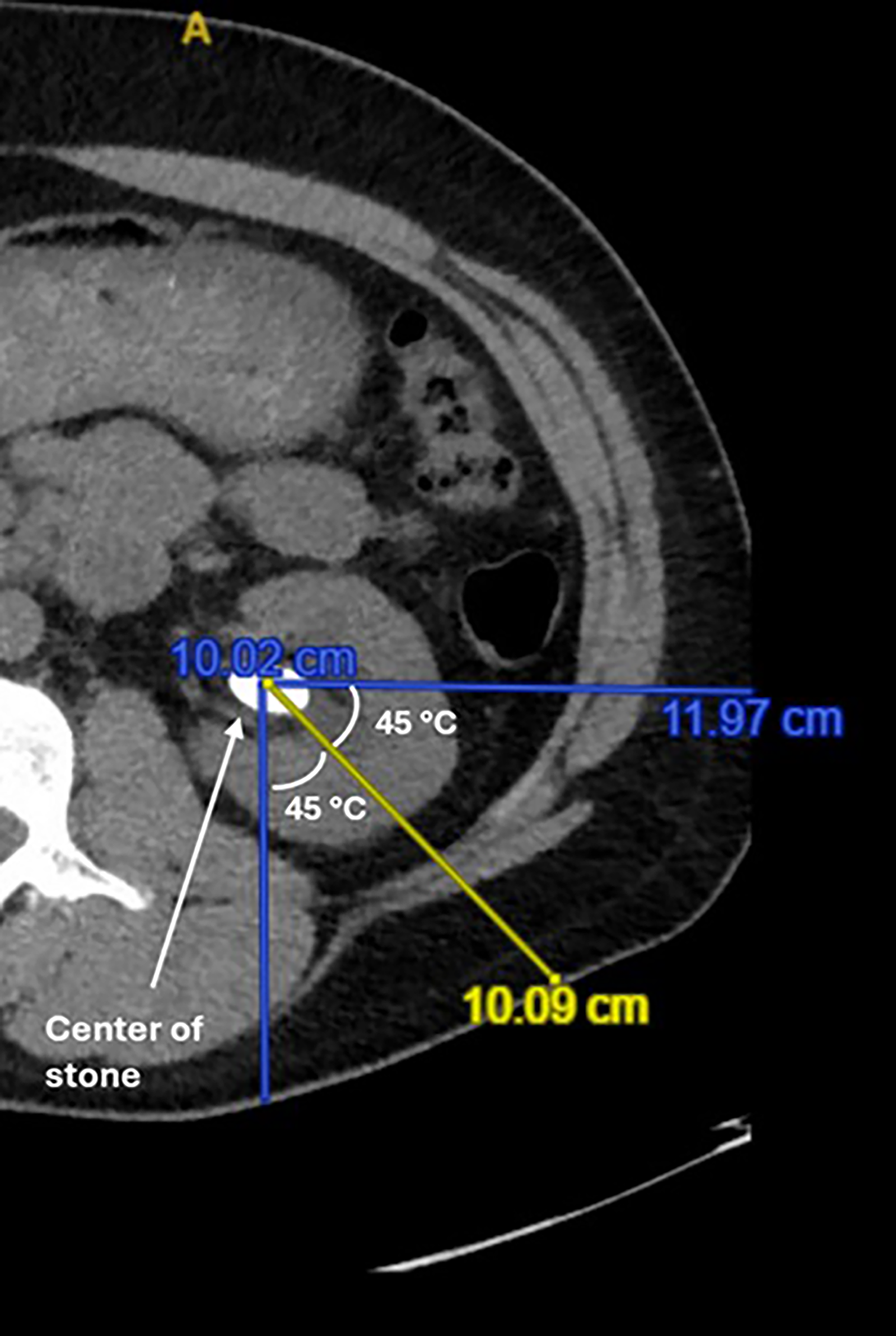
Preoperative S.T.O.N.E tract length technique.
Statistical analysis
Tract lengths were normally distributed and reported as averages with standard deviations. Paired comparisons of tract lengths were performed using the Wilcoxon signed-rank test. To assess the accuracy and reliability of preoperative measurement techniques in predicting intraoperative tract lengths, mean squared error (MSE) and intraclass correlation coefficient (ICC) were calculated, respectively. Lower MSE values reflect better accuracy, and higher ICC values better reliability. Correlation analyses using Pearson and Spearman’s methods, as well as linear regression models, were used to evaluate associations between preoperative factors and intraoperative tract lengths. All statistical tests were two-sided, with a significance threshold of p < 0.05. Analyses were performed using SPSS Statistics (version 28; IBM Corp., Armonk, NY, USA) and Microsoft Excel (Microsoft Corp., Redmond, WA, USA, 2016).
Results
Cohort’s characteristics
During the study period, 47 supine ultrasound-guided PCNL procedures were performed by M.G. using the described surgical technique. Based on the exclusion criterion, 14 cases were excluded: 6 because of inadequate preoperative CT images, 5 because of colonic interposition, 1 for renal malrotation, and 2 with imaging-to-surgery intervals exceeding 6 months. This resulted in a final cohort of 33 cases for analysis (Fig. 4). The average age of the cohort was 58 years (±21) with an average BMI of 30.4 kg/m2 (±6.8). The average imaging-to-surgery interval was 48 days (±82), and 70% (23 cases) of the CT scans were performed in the supine position. Most access tracts were placed into the lower pole (73%), predominantly into anterior calyces (82%) and below the 12th rib (85%). Table 1 summarizes the cohort’s characteristics.
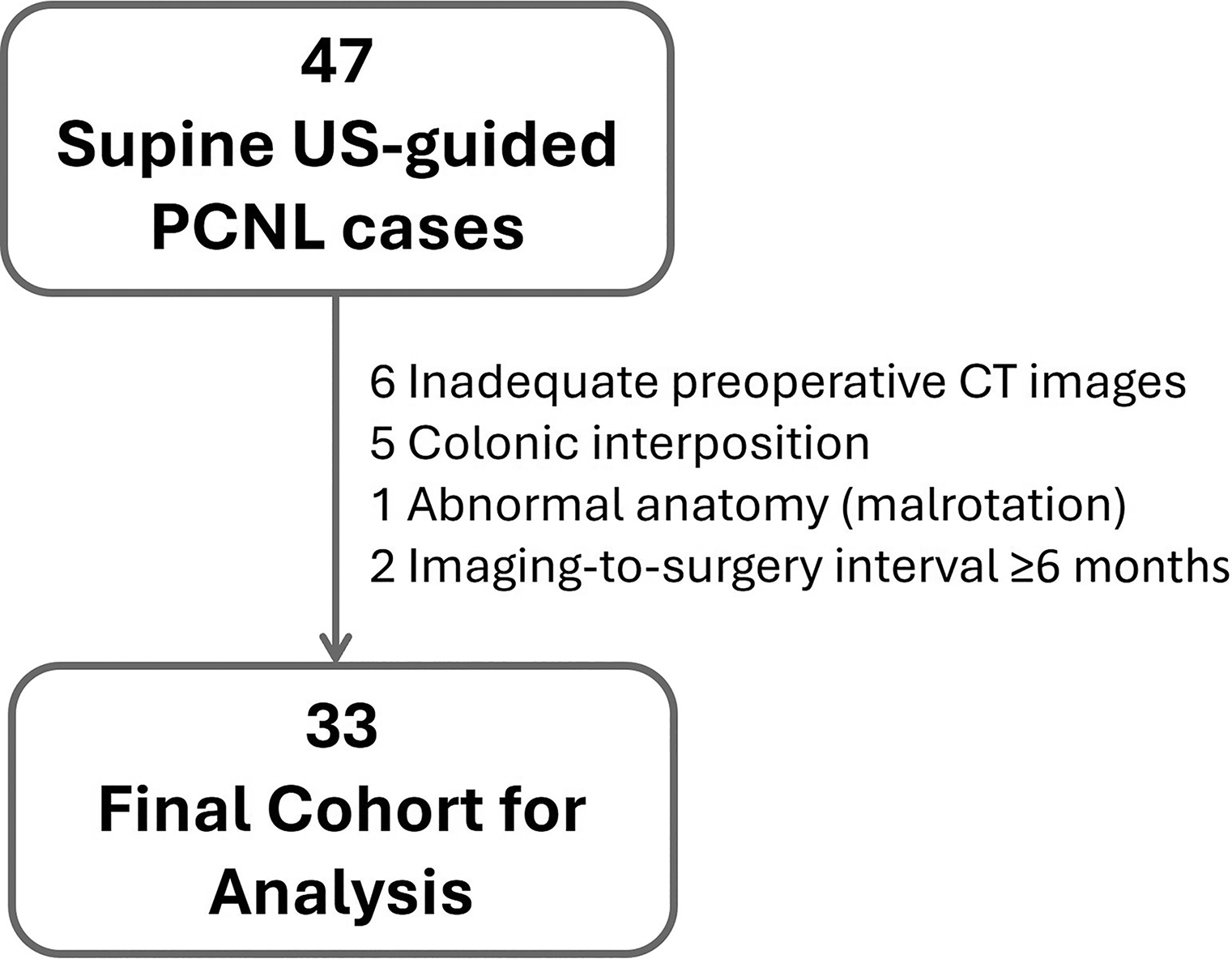
Study diagram. CT = computed tomography; PCNL = percutaneous nephrolithotomy; US = ultrasound.
Cohort’s characteristics. Categorical variables presented as n (%) and continuous variables as average (±SD).
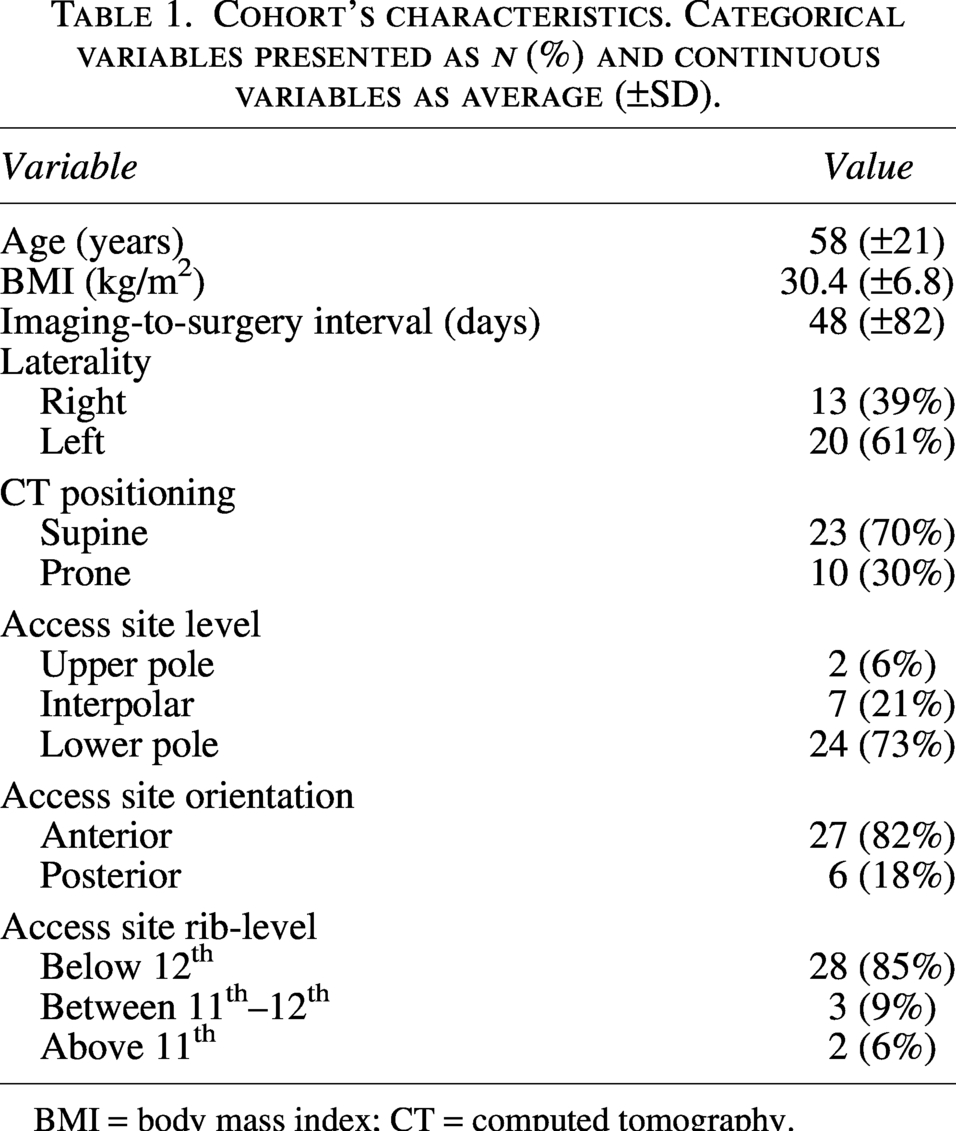
BMI = body mass index; CT = computed tomography.
Tract lengths
The intraoperative, CT-anatomical, and S.T.O.N.E. tract lengths were all normally distributed according to the Shapiro-Wilk test with average values of 9 cm (±2.5), 11.2 cm (±2.7), and 11.4 cm (±2.2), respectively. Both CT-anatomical and S.T.O.N.E. tract lengths were significantly higher than intraoperative lengths (Fig. 5a, p < 0.001), with no significant difference observed between the two preoperative techniques (p = 0.48). The majority of differences between preoperative and intraoperative measurements were positive (CT-anatomical: 85%, S.T.O.N.E.: 82%; Fig. 5b), indicating CT measurements were overestimated in most cases. CT-anatomical tract length technique demonstrated a lower MSE and higher ICC (MSE = 10.42; ICC = 0.42) compared to S.T.O.N.E. tract length technique (MSE = 11.18; ICC = 0.35), indicating greater accuracy and reliability in predicting the true intraoperative length.
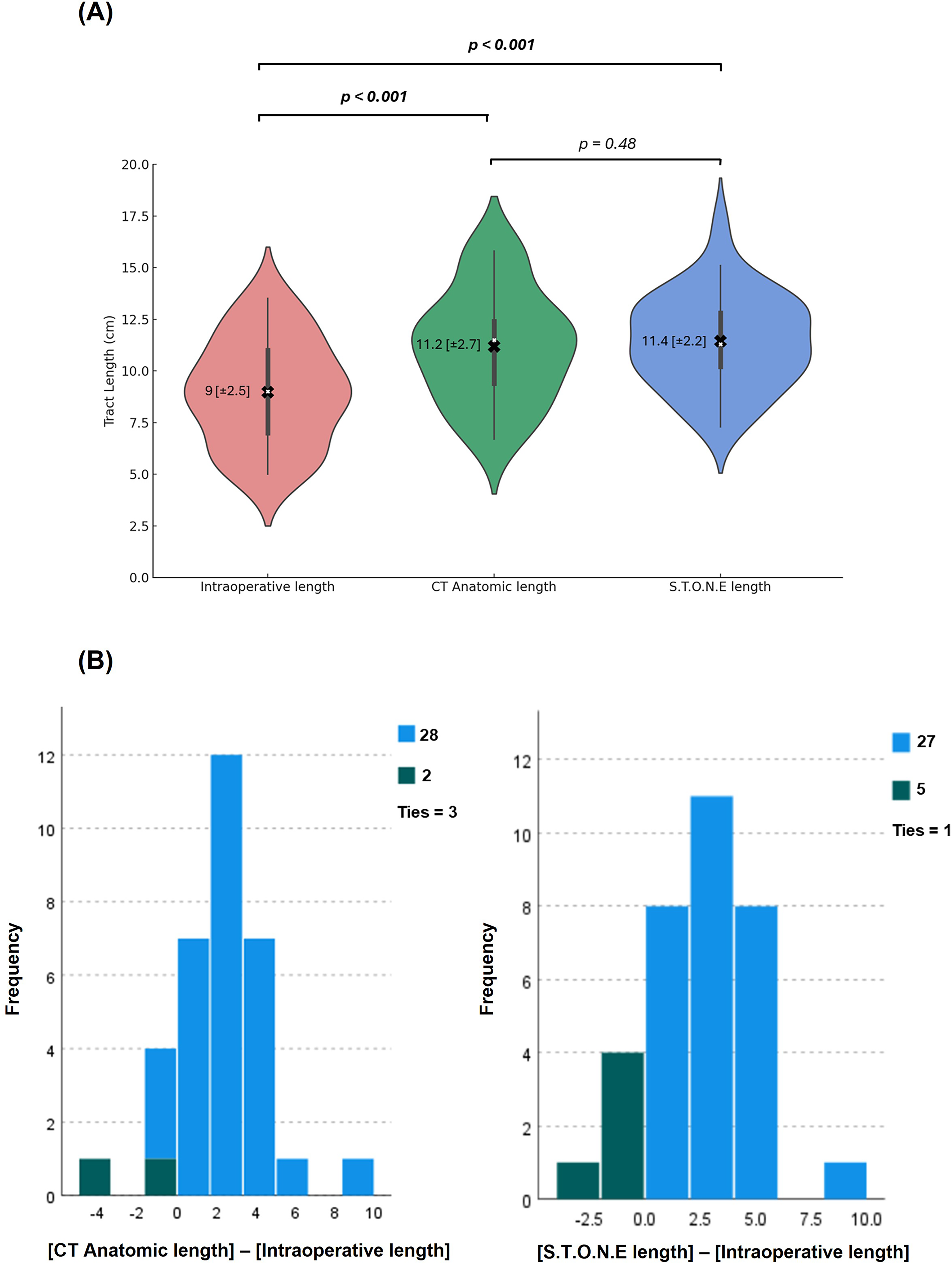
Comparison of preoperative CT-based and intraoperative tract lengths.
When patients were stratified according to their preoperative CT positioning (23 supine and 10 prone), the trend of overestimation persisted across subgroups and measurement techniques. In the prone position, CT-anatomical lengths overestimated intraoperative tract lengths by an average of 2.4 cm (±2.7), while in the supine position, by 2.1 cm (±2.7). Similarly, S.T.O.N.E.-derived lengths exceeded intraoperative measurements by 1.9 cm (±1.9) in the prone group and 2.7 cm (±2.4) in the supine group.
Predictive model for improved intraoperative tract length estimation
Pearson and Spearman correlation analyses revealed that, in addition to CT-anatomical tract length, BMI, access site level (lower/interpolar/upper), and CT positioning (supine/prone) were the most strongly associated with intraoperative tract length (Supplementary Table S1). These factors were subsequently included in a multivariable linear regression model (Table 2), which yielded the following predictive formula for intraoperative tract length:
Multivariable linear regression model for evaluating associations with intraoperative tract lengths.
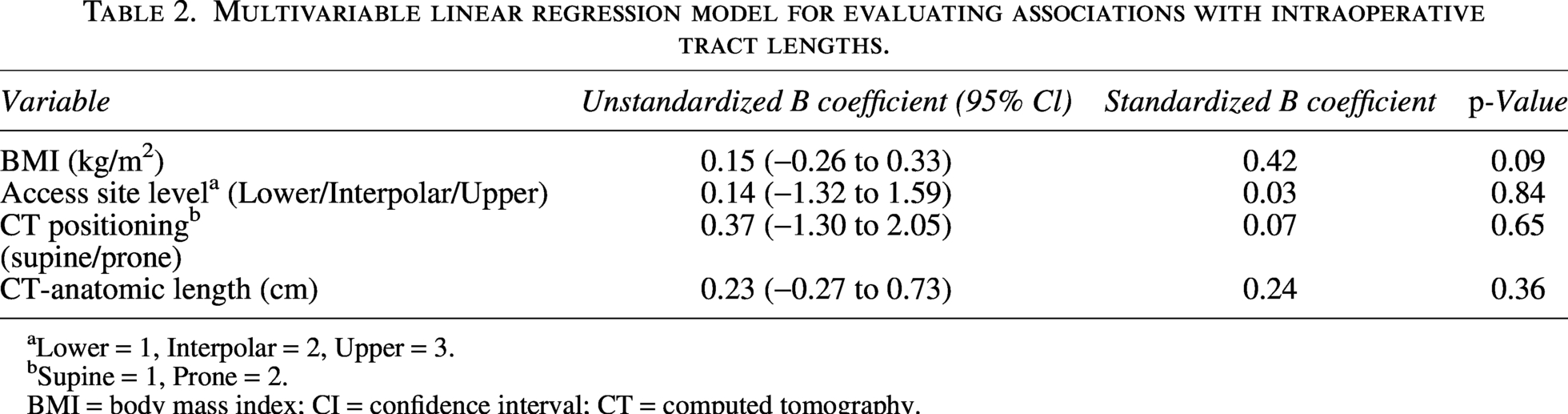
Lower = 1, Interpolar = 2, Upper = 3.
Supine = 1, Prone = 2.
BMI = body mass index; CI = confidence interval; CT = computed tomography.
Estimated Intraoperative Length = 1.06 + [0.15 × BMI] + [0.14 × Access Site Level] + [0.37 × CT Positioning] + [0.23 × CT-Anatomical Length] (Access site level: lower = 1, interpolar = 2, upper = 3; CT position: supine = 1, prone = 2) (Tract Length Calculator). BMI and CT-anatomical length were found to be the most impactful covariates (standardized B: 0.42 and 0.24, respectively).
The estimated tract lengths calculated by the formula were significantly closer to the real-time intraoperative values than the corresponding CT-anatomical values (p < 0.001), with an average difference of 1 mm (±19) compared to 22 mm (±24) (Fig. 6, Supplementary Table S2). The MSE and ICC of the formula-based tract lengths were 3.64 and 0.58, respectively, demonstrating improvement in accuracy and reliability over the corresponding values derived from the CT-anatomical measurements (MSE = 10.42; ICC = 0.42).
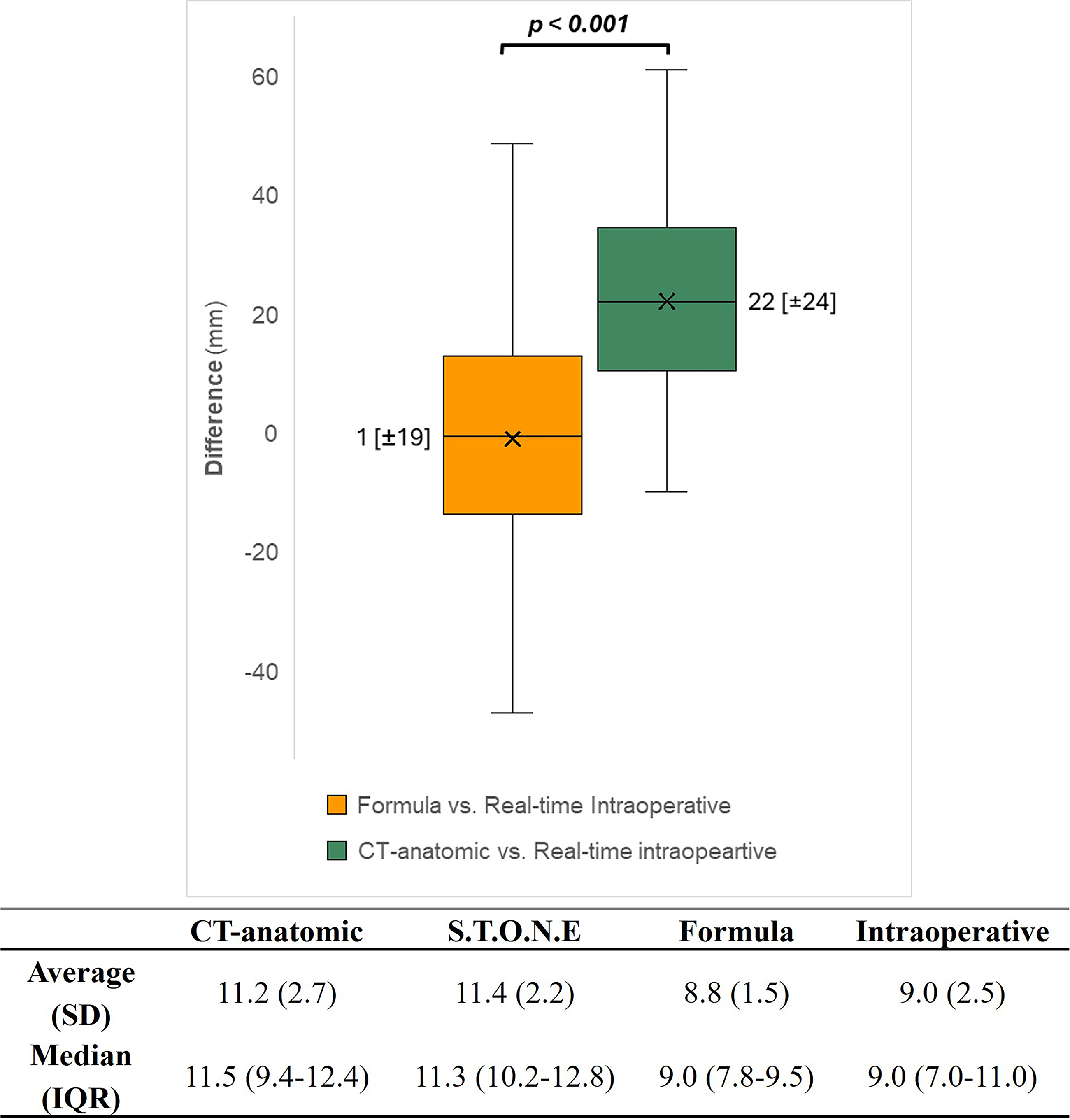
Box-plot and table comparing preoperative tract length estimation methods relative to real-time intraoperative measurements. Crossmark represents the mean [±SD], while boxes indicate the medians and IQR. CT = computed tomography; IQR = interquartile range; SD = standard deviation.
Discussion
PCNL is the gold standard in the treatment of large and/or complex renal calculi. However, the success and safety of the procedure depend heavily on careful preoperative planning. 9 Key considerations include the stone burden, renal anatomy, and the course and depth of the planned percutaneous tract.8,10 Among these, tract length has emerged as an important technical variable influencing both surgical difficulty and complication rates. Longer tract lengths reduce the maneuverability of the nephroscope by increasing the distance between the skin and the kidney. 11 This limited mobility can lead to lower stone-free rates, longer operative times, and increased risk of bleeding because of excessive torque on the renal parenchyma. In contrast, a shorter tract length improves nephroscope control. Supporting this, Okhunov et al. reported a 100% success rate when the tract length was under 8 cm, compared with only a 50% success rate when the tract length exceeded 12 cm.2,7,11 Obesity, which often correlates with longer tract lengths, is linked to a higher incidence of complications, longer surgical times, and higher re-intervention rates 2 .
Tract length estimation is typically performed using CT-based methods, yet no standardization has been made. The S.T.O.N.E. score includes tract length as one of five parameters measured as the average distance from the center of the stone to the skin at 0°, 45°, and 90° angles on a supine CT. Its cutoff of 10 cm is based on typical distances observed in patients with a BMI ≥30 kg/m2. 2 Abouelleil et al., defined tract length as the linear distance from the skin to the medial lower calyx. 7 Duty et al. used a more detailed approach of measuring tract length as the distance from a posterior calyx to the skin along an infundibulum, with separate assessments for the upper, middle, and lower poles of the kidney. 11 However, all of these methods rely on static CT images acquired in the prone or supine position, which may not accurately reflect the patient’s real-time intraoperative positioning. This mismatch can contribute to discrepancies in tract length measurements.
Our study addresses this limitation by comparing preoperative measurements to actual intraoperative measurements and proposing a predictive model that incorporates key modifying factors. Multiple patient- and procedure-related factors affect nephrostomy tract length and should be considered during preoperative planning. BMI appears to be an influential factor with a strong positive correlation (ρ = 0.69, p < 0.001),1,7 with subcutaneous fat thick being the primary driver. 9 Patient positioning during imaging and during surgical procedure has a notable impact on tract length. Tract lengths were found significantly longer in the supine position, particularly while obtaining lower pole access, because of subcutaneous tissue displacement by gravity. 9 This finding was supported in patients with BMI ≥ 30, with average tract lengths measuring 11.3 cm in the supine position versus 9.3 cm in the prone position. 7 Access site location also contributes to variations in tract lengths. Astroza et al. found that lower pole access resulted in longer tracts (median 9.3 cm) compared to upper pole access (8.6 cm), reflecting anatomical variability within the kidney. 1 These findings may support criticism of the supine PCNL approach (which also typically uses lower pole access), claiming it is associated with a longer access tract length compared to the prone position, as suggested by preoperative CT-based trajectories.
In our study, we compared preoperative nephrostomy tract length estimates from two CT-based methods: the S.T.O.N.E. score and a CT-anatomical measurement, with intraoperative lengths measured during supine PCNL. Both methods significantly overestimated the actual tract length (mean intraoperative: 9.0 cm; CT-anatomical: 11.2 cm; S.T.O.N.E.: 11.4 cm). The study was designed to mirror real-world practice, where tract length is estimated from CT-based 2D scans and access is performed without adjusting for CT imaging parameters. The observed overestimation likely stems from differences in positioning, kidney mobility, and 2D–3D projection discrepancies. These findings challenge the commonly held belief, derived from preoperative imaging, that the kidney lies deeper in the supine position, resulting in longer tract lengths compared with the prone position. 12 Although our study did not directly compare supine and prone PCNL tract lengths, the marked overestimation (∼2–3 cm) of CT-based tract lengths in the supine position may suggest that the real intraoperative tracts are shorter than those in the prone position. This directly contradicts claims made by proponents of the prone approach. Future studies directly comparing intraoperative tract lengths between positions are warranted to confirm this assumption.
Inaccuracies between preoperative and intraoperative tract lengths can affect preprocedural planning, including inappropriate sheath selection (standard vs extra-long), choosing an extra-long nephroscope when a standard will suffice, misestimation of operative time, and suboptimal access site decision for selection of a shorter tract. Since our study shows that real-time tracts are approximately ∼2 cm shorter than CT estimates, surgeons may safely retain their preferred access site most of the times even when preoperative imaging suggests a longer tract. Additionally, needle length is particularly important in ultrasound-guided procedures that employ a needle guide, where a longer external length of needle may be necessary. These considerations are especially critical in patients with extreme morbid obesity, where accessing the targeted calyx can be technically challenging and may seem impossible based on CT-assessed tract lengths, but in reality, is quite doable. To address this, we developed a predictive formula using BMI, access level, CT position, and CT length that outperformed CT-based methods alone with a high accuracy (mean error of 1 mm) and improved reliability. These findings highlight that integrating patient- and procedure-specific variables significantly enhances preoperative tract length estimation and offers more precise guidance, especially for technically complex cases involving obese patients or those requiring lower pole access.
This study has several limitations. First, it was conducted at a single institution, which may affect generalizability. Second, while the sample size was adequate for the primary outcome, it was insufficient for meaningful subgroup analyses. Third, while we demonstrated improved accuracy in tract length prediction, we did not directly assess clinical outcomes. Fourth, our predictive formula was not externally validated on an independent cohort. Lastly, it is important to note that 10 patients underwent preoperative CT imaging in the prone position. This is likely the most significant source of measurement bias, as kidney position has been demonstrated to vary on CT imaging based on supine or prone positioning. 12 And yet, even in the prone position, tract lengths were overestimated by approximately 2 cm, and we addressed the CT position in our formula. An ideal study would actually conduct CT imaging in the modified supine position for the most accurate comparison. However, this was a real-world study where radiologists may modify imaging protocols and patient positioning despite the urologists’ preoperative planning. Future research should focus on validating this predictive model in larger, multicenter cohorts and to compare intraoperative tract lengths between supine and prone position. It should also assess whether improved tract length estimation translates into tangible clinical benefits, such as reduced operative time, fewer access-related complications, and improved stone-free rates.
Conclusion
Conventional preoperative CT-based measurements frequently overestimate the true access length in supine PCNL. Our predictive model, incorporating both patient- and imaging-related factors, offers improved accuracy for operative planning. Future studies are needed to assess if integrating this tool into preoperative planning may support better surgical outcomes and decision-making.
Authors’ Contributions
Conception and design—Z.S. and M.G. Acquisition of data—Z.S., S.K., K.G., E.F., V.D., and J.S.S. Analysis and interpretation—Z.S., R.G., and B.G. Drafting of the article—Z.S., R.G., and S.K. Critical revision of the article—K.G., W.M.A., and M.G. Statistical analysis—Z.S. Administrative, technical, or material support—B.G. Supervision—M.G.
Footnotes
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because of ethical issues and the privacy of the participants.
Ethics of Approval Statement
Ethical approval to report this study was obtained from our institutional review board (Icahn School of Medicine at Mount Sinai; STUDY-14–00879; 1/22/25).
Authors’ Disclosure Statement
No competing financial interests exist.
Supplemental Material
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.