
Abstract
Objective:
Pyeloplasty is the gold standard procedure for treating ureteropelvic junction obstruction (UPJO), but the occurrence of postoperative complications is a major challenge. This study aimed to identify the predictors of postpyeloplasty complications, which are not well characterized in contemporary literature.
Study Design:
We retrospectively analyzed data of children who underwent pyeloplasty in our hospital from January 2011 to August 2022, with a minimum follow-up of 1 year. Furthermore, a systematic review and meta-analysis of studies published from 2000 to 2023 was performed to identify predictors of complications.
Results:
In cohort studies (n = 555), preoperative urinary tract infection (pre-UTI) (odds ratio [OR] = 5.65, 95% confidence interval [CI]: 2.96–10.78, p < 0.001), Double J-stent duration (OR = 1.005, 95% CI: 1.001–1.008, p = 0.005), renal cortical thickness (OR = 0.181, 95% CI: 0.071–0.461, p < 0.001), and collection system separation (OR = 1.170, 95% CI: 1.017–1.347, p = 0.028) were associated with total postoperative complications. Pre-UTI (OR = 4.87, 95% CI: 1.98–11.98, p = 0.001), Double J-stent duration (OR = 1.005, 95% CI: 1.001–1.009, p = 0.019), preoperative renal cortical thickness (OR = 0.197, 95% CI: 0.042–0.928, p = 0.040), and duration of operation (OR = 1.013, 95% CI: 1.003–1.022, p = 0.008) were associated with recurrence. Pre-UTI (OR = 5.33, 95% CI: 2.73–10.38, p < 0.001) and preoperative renal cortical thickness (OR = 0.351, 95% CI: 0.124–0.990, p = 0.048) were predictors of postoperative UTI. In the meta-analysis, sex (I2 = 0%, relative risk [RR] = 1.19, 95% CI: 1.01–1.40, p = 0.04), operation methods, and split renal function (I2 = 50%, RR = 0.76, 95% CI: 0.59–0.96, p = 0.02) were identified as predictors of postoperative complications.
Conclusions:
We identified the predictors of postpyeloplasty complications. Early identification and treatment can help us reduce the incidence of complications.
Introduction
Prenatal ultrasound can help detect most cases of fetal hydronephrosis during pregnancy. 1 Prenatally diagnosed hydronephrosis spontaneously resolves in many cases, 2 but surgical treatment is required in 15%–20% of cases. 3 Ureteropelvic junction obstruction (UPJO) is the most common cause of persistent postnatal hydronephrosis, 1 accounting for approximately 10%–30% of children with hydronephrosis. 4 The estimated incidence of congenital UPJO is 1 per 1000–2000 live births, with a male-to-female ratio of approximately 2–3:1; the left side accounts for about two-third of all cases.2,5 Without timely treatment, these children may suffer renal impairment, 6 and pyeloplasty is considered the gold standard for relieving the obstruction. 7 Surgical options include open operation, laparoscopy, and robot-assisted procedures. Minimally invasive pyeloplasty is a widely used surgical approach, and both laparoscopy and robot-assisted surgeries have success rates of over 90%, similar to open operation. 6
Although currently used surgical approaches have satisfactory success rates, postoperative complications are still inevitable. The incidence of postoperative complications is up to 20% or more. 3 The main postoperative complications include recurrence, urine leak, ileus, infection, obstruction secondary to clot or stent displacement, and blood transfusion. 8 Postoperative complications may necessitate readmission or even reoperation. Therefore, identifying the factors that affect postoperative complications can help inform interventions to prevent the occurrence of complications.
Currently, there is no clear consensus regarding the specific factors contributing to postoperative complications. However, surgical methods, 9 surgical access, 10 and drainage technique 3 likely play a role. We conducted a retrospective cohort study and meta-analysis of previously published studies to contribute to this ongoing discussion. The objective of this study was to illustrate the factors that may influence postpyeloplasty complications in patients with UPJO. Our findings may provide valuable insights for preventing postoperative complications of pyeloplasty.
Materials and Methods
Retrospective cohort study
This study was approved by the Ethics Committee of Qilu Hospital of Shandong University (Approval No. KYLL-202312-030). No additional patient-informed consent specific to this study was required, given its retrospective nature. The present study followed the Strengthening The Report Of Cohort Studies in Surgery (STROCSS) criterion. 11
Study population and design
Our retrospective cohort study included patients aged <18 years who underwent pyeloplasty for UPJO at our hospital between January 2011 and August 2022 and were followed up for a minimum of 1 year after operation. Patients with a previous history of pyeloplasty, other urological malformations, and nephrostomy were excluded, as they may have been more complex cases and could have influenced the outcomes. All patients included in the study underwent the same surgical procedure, pyeloplasty, which involves the reconstruction of the narrowed or UPJO. Additionally, a Double J-stent (DJ) was inserted in all patients.
Exposure and outcomes
Data regarding the following variables were extracted: sex, involved side, weight, age, presence of bilateral hydronephrosis, prenatal detection, calculus, vascular crossing, comorbidities, and urinary tract infection (UTI). Surgical and clinical variables included the surgical approach, operative time, estimated intraoperative blood loss, duration of DJ stent, drainage days, hospital days, and postoperative hospital stay. Preoperative and postoperative laboratory indices and radiological variables included pelvis anterior–posterior diameter, renal cortical thickness, split renal function (SRF), estimated glomerular filtration rate, blood urea nitrogen, serum creatinine, cystatin C, white blood cell count, C-reactive protein, and urine white blood cell.
Outcomes
Complications occurring during follow-up, including recurrence, UTI, urine leak, ileus, incision infection, obstruction secondary to clot or displaced stent, and blood transfusion.
Statistical analysis
Continuous variables were first tested for normality; those conforming to a normal distribution were presented as mean ± standard deviation, with between-group differences assessed by the t-test, while skewed distributed variables were expressed as quartiles (median [interquartile range]) and analyzed using the rank-sum test. Categorical variables were expressed as frequency (percentage), and between-group differences were assessed using the chi-square test. Binary logistic regression models were applied for covariate adjustment. All statistical analyses were conducted using SPSS 26.0 (IBM SPSS Statistics). A p-value of <0.05 was considered indicative of statistical significance.
Meta-analysis
The meta-analysis was conducted after the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions and complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 12 statement and A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR2). 13
Inclusion and exclusion criteria
Inclusion criterion: (1) Original research articles or graduation theses published in English and Chinese core journals; (2) reporting of at least one factor related to complications.
Exclusion criterion: (1) Literature reviews, meta-analyses, or animal experiments; (2) duplicate publications; (3) redo operation for recurrent patients.
Data sources
Three researchers searched the Cochrane Library, PubMed, Embase, Web of Science, CNKI, China Science and Technology Journal Database (VIP), Wanfang database, and Chinese Biomedical Literature Database (SinoMed) for relevant studies published until August 2023. The details of the search strategy are shown in Supplementary Data.
Study selection
Three authors independently selected the studies for inclusion in the meta-analysis. In case of any inconsistencies, the final decision was reached by consensus.
Data extraction and quality assessment
Data from the included studies were independently extracted by three researchers. The extracted contents included the first author’s name, location of study, year of publication, journal of publication, type of study, the number of total cases, and cases with complications.
The quality of the cohort studies was assessed using the Newcastle–Ottawa Scale with a total score of 9. 14 A minimum score of 6 was required for inclusion. The Cochrane risk of bias tool was used for the quality assessment of randomized controlled trials (RCTs). 15
Statistical analysis
RevMan 5.4 (Review Manager) was used to calculate effect sizes, graph forest plots, and assess the quality of RCTs. The chi-square test was used to assess statistical heterogeneity among studies. Q-test was used to assess whether this heterogeneity affected the results. According to the Cochrane review guidelines, in case of small heterogeneity (I2 < 50%), a fixed-effects model was used. Otherwise, a random-effects model was used for the meta-analysis. The extracted original data were analyzed using dichotomous methods, and the results were reported as relative risk (RR) with 95% confidence intervals (CIs), calculated by the M-H method (fixed- or random-effects model). Sensitivity analyses and publication bias analyses were performed using Stata 16.0 (Stata Corp LP, College Station, TX, USA). Publication bias was analyzed by Egger’s test and funnel plots. A p-value of <0.05 was considered statistically significant.
Results
Cohort study
Patient characteristics
A total of 555 patients were included in the final analysis; of these, 90 (16.2%) patients developed complications. Thirty (5.4%) patients developed recurrence, and 57 (10.3%) patients developed post-UTI. Patient characteristics, surgical information, and examination results are summarized in Table 1.
Baseline Characteristics of Included Patients Stratified by Complication, Recurrence, and Post Urinary Tract Infection
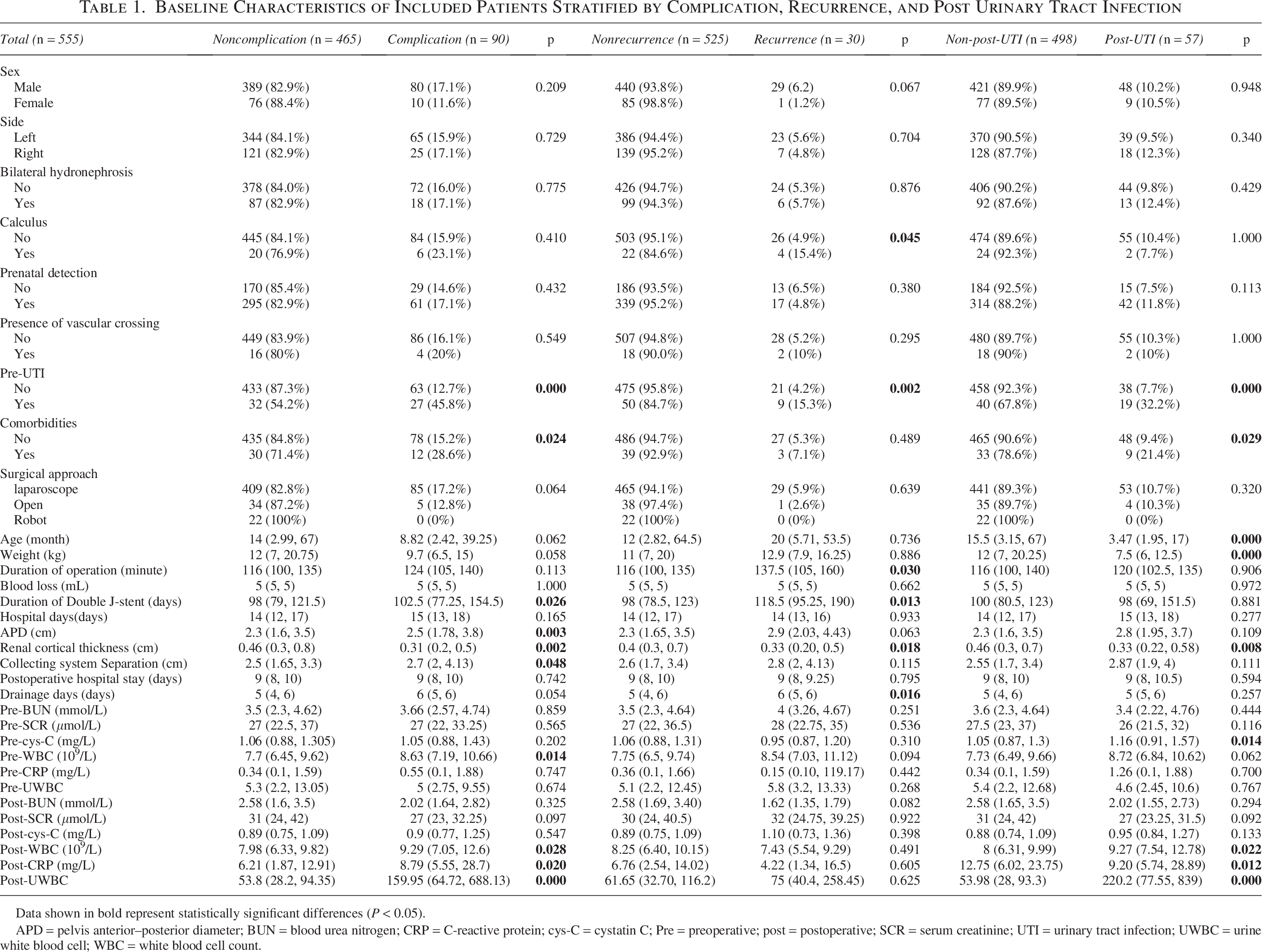
Data shown in bold represent statistically significant differences (P < 0.05).
APD = pelvis anterior–posterior diameter; BUN = blood urea nitrogen; CRP = C-reactive protein; cys-C = cystatin C; Pre = preoperative; post = postoperative; SCR = serum creatinine; UTI = urinary tract infection; UWBC = urine white blood cell; WBC = white blood cell count.
Predictive factors
Univariate results
The univariate analysis identified 11 predictors associated with complications, 6 factors associated with recurrence, and 9 factors associated with post-UTI (Table 1).
Multivariate results
On multivariate analysis, pre-UTI showed a significant association with total postoperative complications (odds ratio [OR] = 5.65, 95% CI: 2.96–10.78, p < 0.001), recurrence (OR = 4.87, 95% CI: 1.98–11.98, p = 0.001), and post-UTI (OR = 5.33, 95% CI: 2.73–10.38, p < 0.001). The incidence of total complications (OR = 1.005, 95% CI: 1.001–1.008, p = 0.005) and recurrences (OR = 1.005, 95% CI: 1.001–1.009, p = 0.019) increased with the increase in the duration of the DJ stent. Patients with a thinner renal cortical thickness prior to operation were more likely to have complications (OR = 0.181, 95% CI: 0.071–0.461, p < 0.001), recurrences (OR = 0.197, 95% CI: 0.042–0.928, p = 0.040), and post-UTI (OR = 0.351, 95% CI: 0.124–0.990, p = 0.048). Compared to the group without complications, the separation of the collecting system (OR = 1.170, 95% CI: 1.017–1.347, p = 0.028) was more severe in the group with complications. The duration of operation (OR = 1.013, 95% CI: 1.003–1.022, p = 0.008) in the recurrent group was longer than that in the nonrecurrent group (Supplementary Fig. S1).
Meta-analysis
Study characteristics and quality assessment
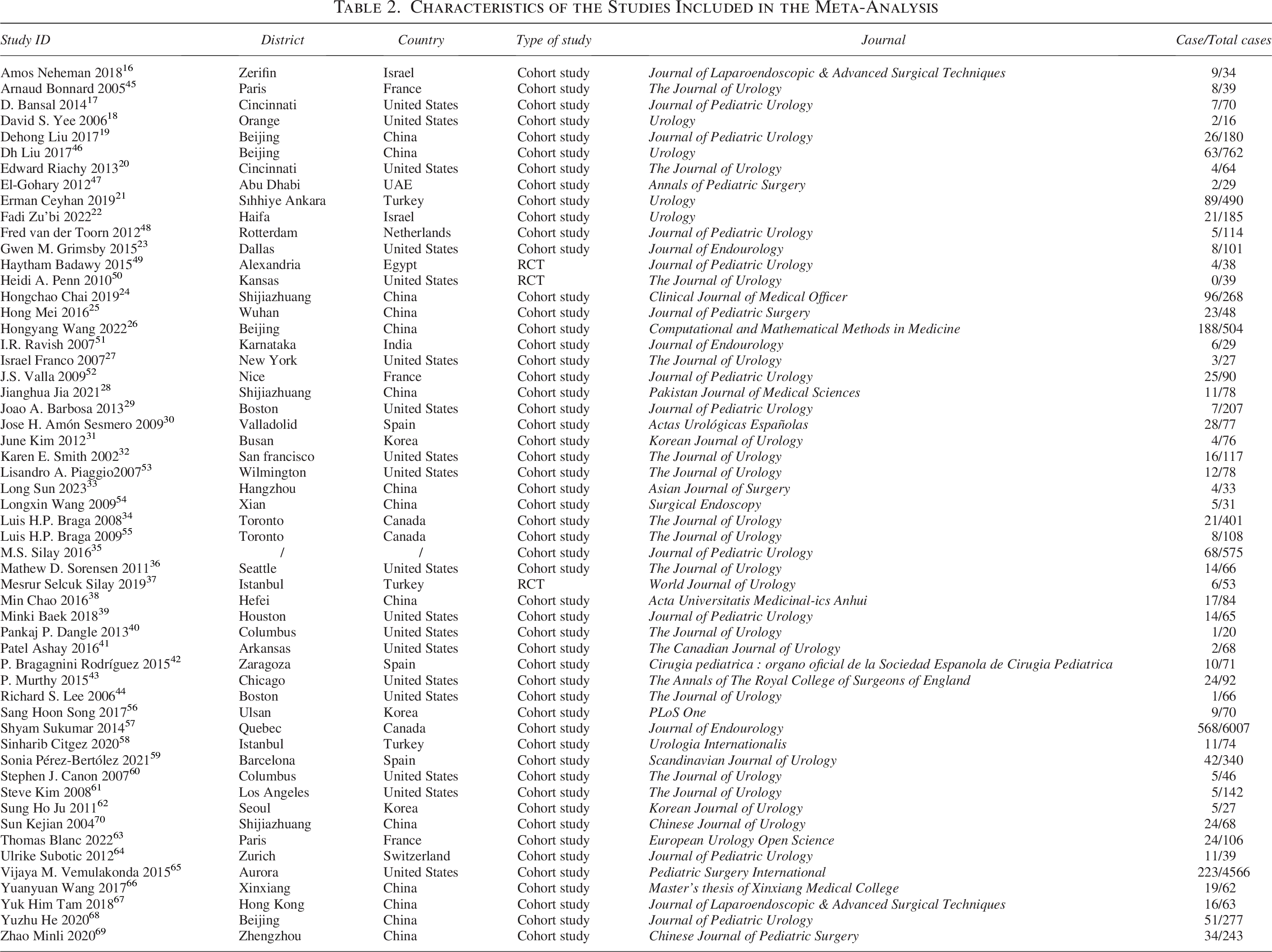
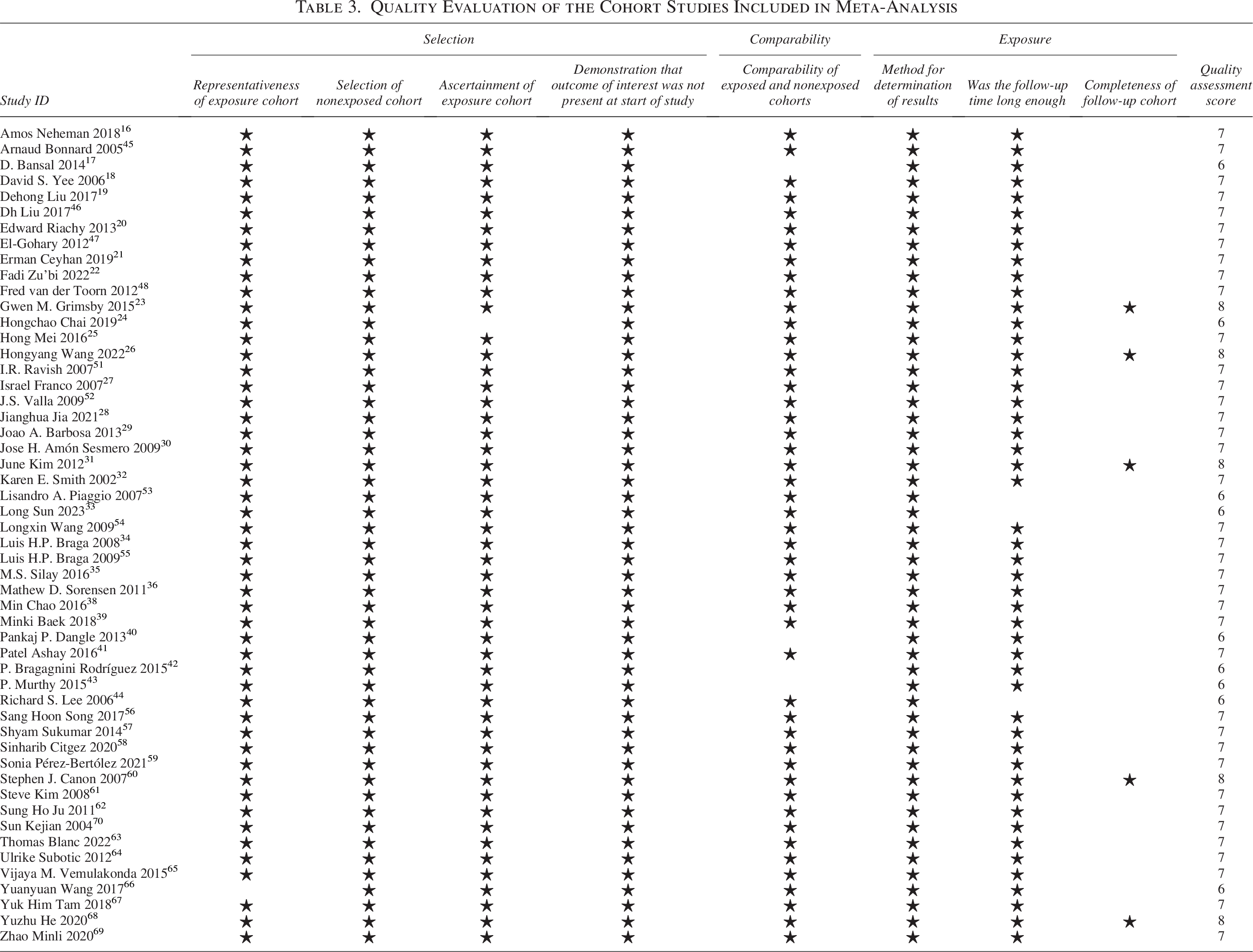
A total of 5899 articles were retrieved, of which 55 studies (3 RCTs and 52 cohort studies) were included in the meta-analysis.16–70 The total number of patients undergoing pyeloplasty in the 55 studies was 17,623, of which 1909 developed complications. A schematic illustration of the literature screening process is shown in Figure 1. The characteristics of the included studies are shown in Table 2. The NOS score of nine studies was 6, five studies received a score of 8, and the remaining studies received a score of 7 (Table 3). The risk of bias and summary of the RCTs are shown in Supplementary Figure S1.
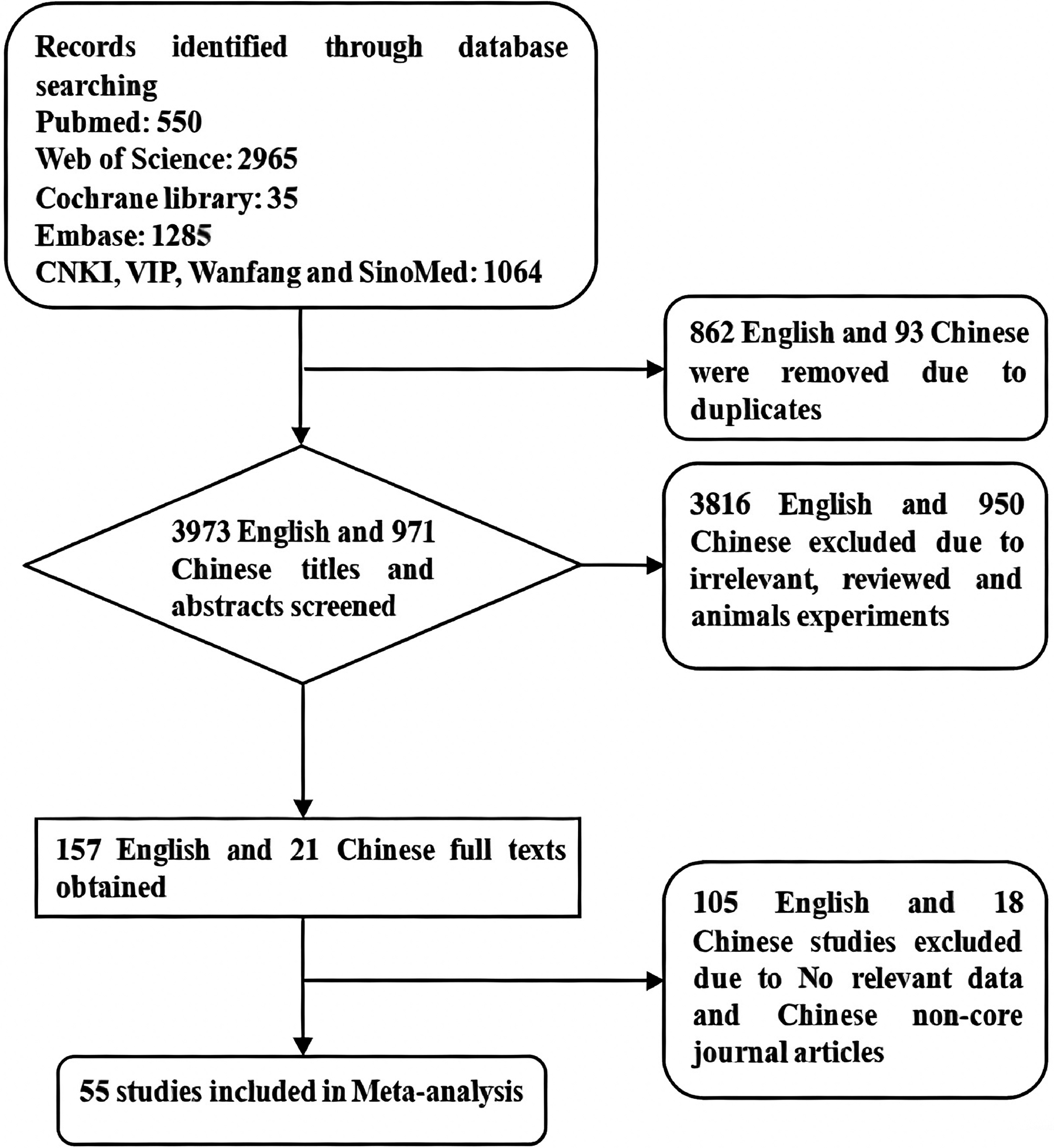
Flowchart of predictors of complications after pyeloplasty study search and screening.
Characteristics of the Studies Included in the Meta-Analysis
Quality Evaluation of the Cohort Studies Included in Meta-Analysis
Quantitative synthesis
Analysis of data from 1279 robotic and 1405 laparoscopic surgeries from 12 cohort studies and 1 RCT revealed that compared to laparoscopic operation, robotic operation16,20,27,33,35,37,41,56,57,61,64,67 (I2 = 8%, RR = 0.70, 95% CI: 0.54–0.90, p = 0.007) (Fig. 2) was a protective factor for complications. Analysis of data from 10 cohort studies with 6378 patients (597 complications) revealed that open operation17,18,29,36,40,43,44,56,57 was a protective factor compared to robotic operation (I2 = 15%, RR = 1.28, 95% CI: 1.05–1.57, p = 0.01) (Fig. 3). Analysis of data from 50 cohort studies and 1 RCT (7553 patients, 916 complications) revealed no significant difference between laparoscopy22,26,28,31,45,48,50–57,59 (I2 = 37%, RR = 1.15, 95% CI: 0.99–1.35, p = 0.08) and open operation; however, the complication rate of laparoscopic surgery was higher than that of open operation. A larger sample size may have provided a significant result. There was no significant difference in complications between the trans-flank (I2 = 33%, RR = 1.30, 95% CI: 0.92–1.86, p = 0.14) and trans-dorsal procedures.
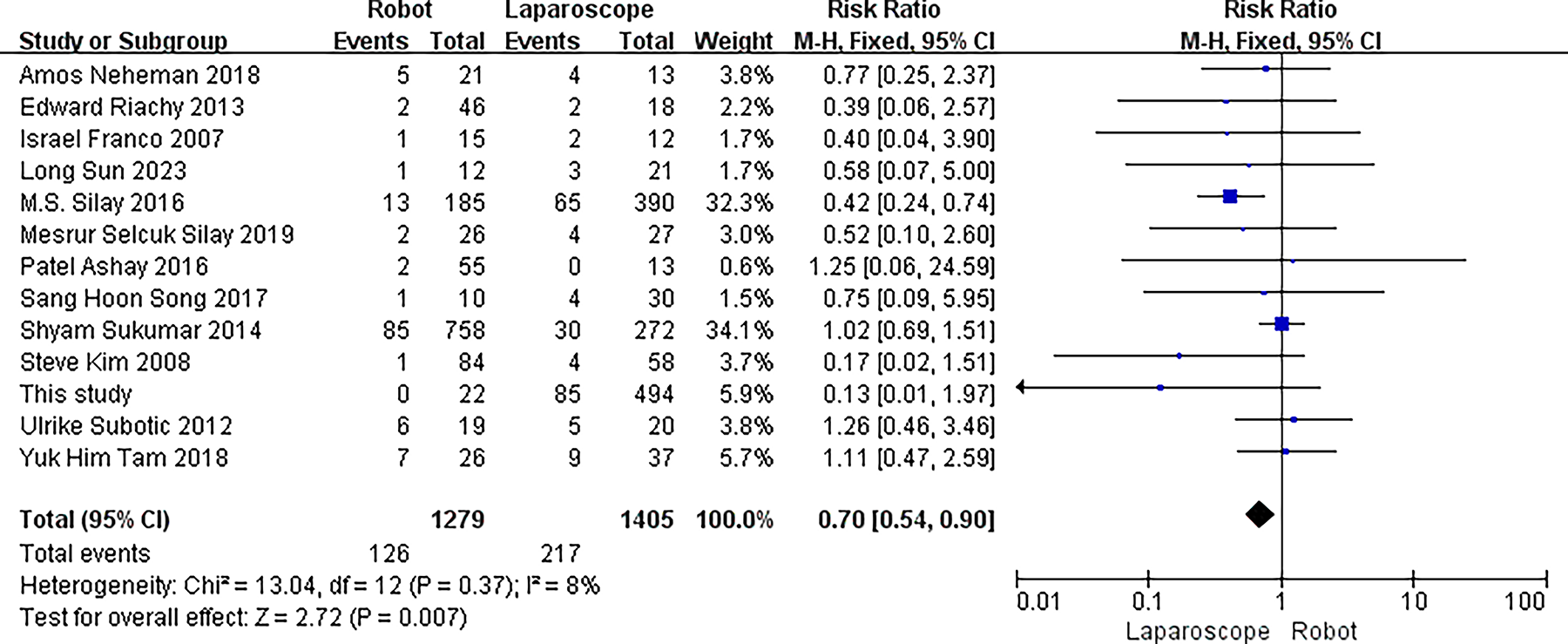
Forest plot of robot vs laparoscope for complications after pyeloplasty.
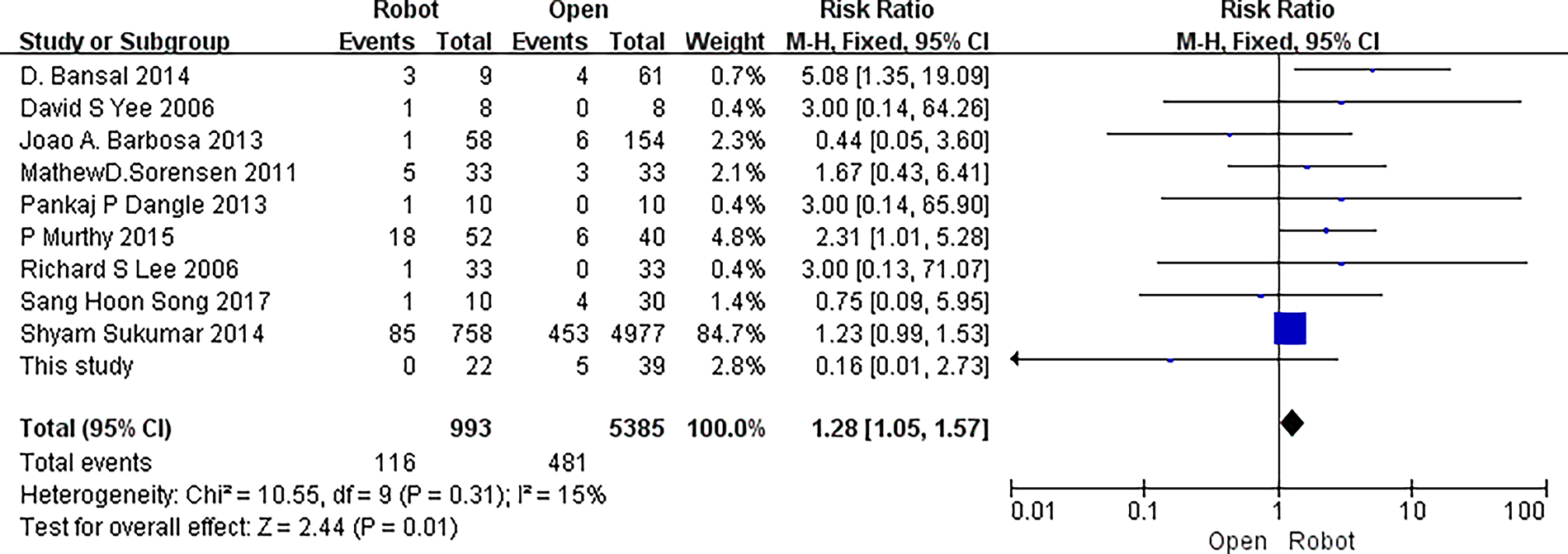
Forest plot of open vs robot for complications after pyeloplasty.
Sex
Analysis of data from eight cohort studies (7395 patients, 764 complications) identified male sex21,22,26,35,65,68,69 (I2 = 0%, RR = 1.19, 95% CI: 1.01–1.40, p = 0.04) (Fig. 4) as a risk factor for complications.
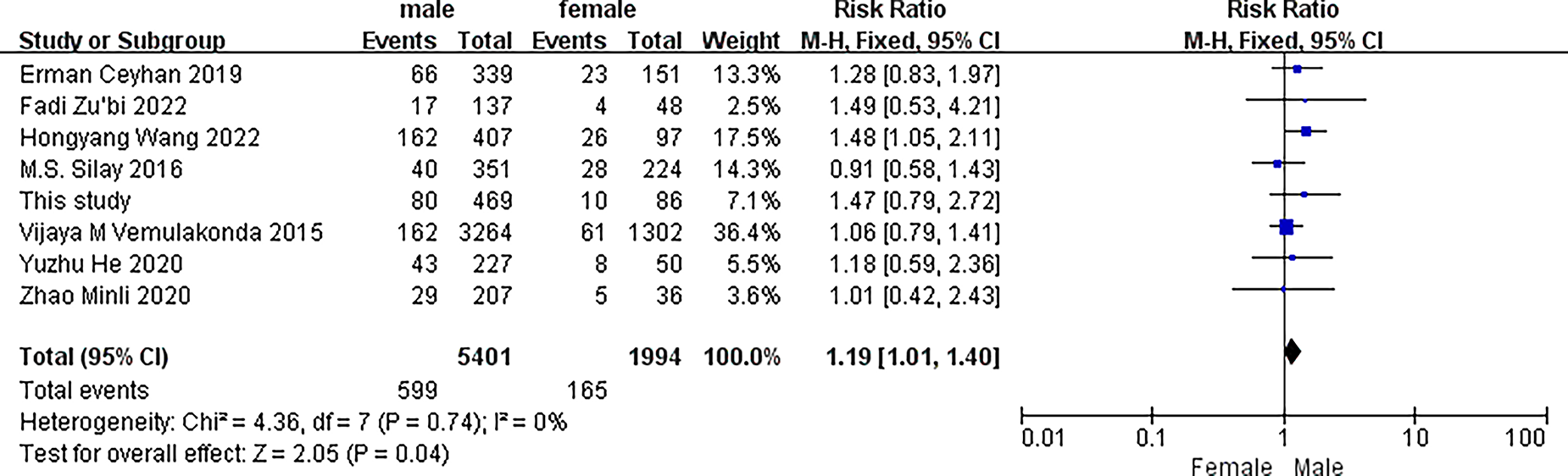
Forest plot of gender for complications after pyeloplasty.
Split renal function
Analysis of data from six cohort studies showed that SRF <4023,24,34,35,69 (I2 = 50%, RR = 0.76, 95% CI: 0.59–0.96, p = 0.02) (Fig. 5) was a protective factor for complications.
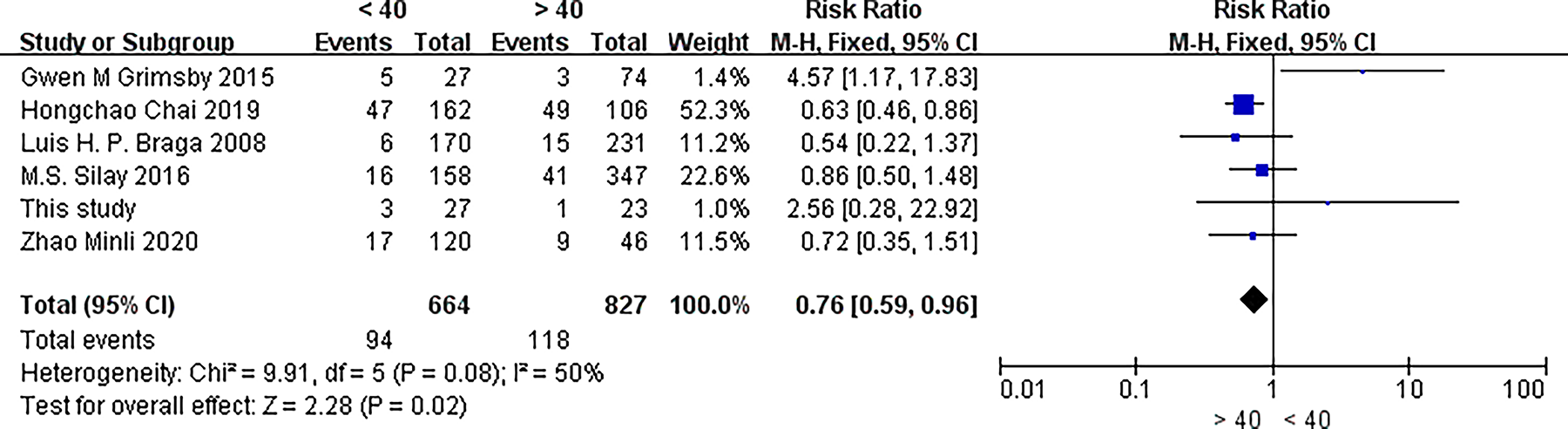
Forest plot of split renal function <40 for complications after pyeloplasty.
Other factors
We analyzed several other potentially relevant factors, but none was found to be statistically significant (Table 4).
Risk Factors for Postoperative Complications of Pyeloplasty
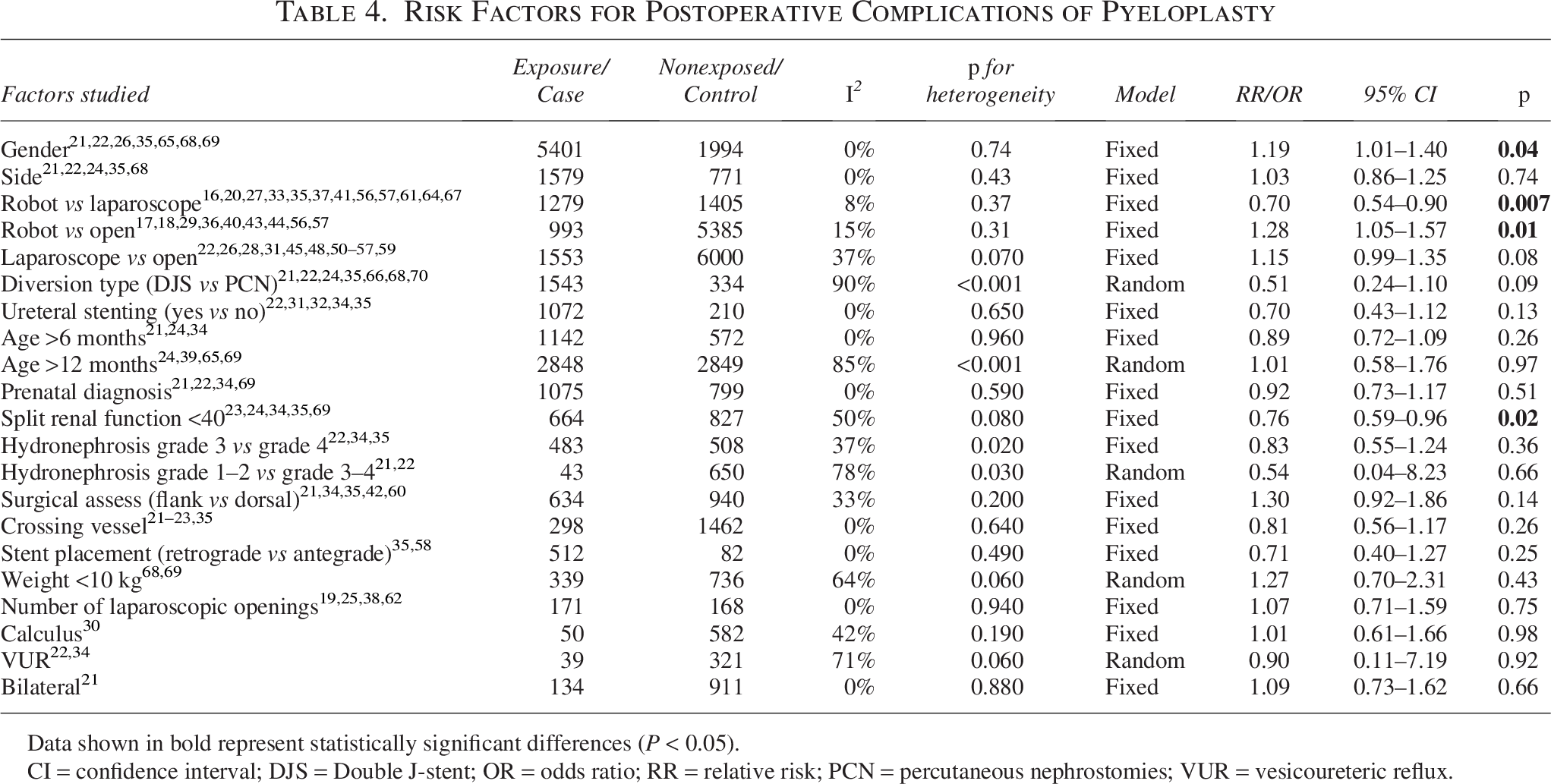
Data shown in bold represent statistically significant differences (P < 0.05).
CI = confidence interval; DJS = Double J-stent; OR = odds ratio; RR = relative risk; PCN = percutaneous nephrostomies; VUR = vesicoureteric reflux.
Sensitivity analysis and publication bias
On sensitivity analyses, the results of the meta-analysis remained largely stable after the exclusion of any individual study. Funnel plots showed no significant asymmetries. In addition, Egger’s test showed no evidence of any significant publication bias (p > 0.05).
Discussion
In our cohort study, four factors were found to be associated with the development of complications, four with recurrence, and two with post-UTI. The presence of pre-UTI was found to increase the incidence of total complications, recurrences, and UTI after operation. Thus, it seems that the effect of pre-UTI may be underestimated and that a complete resolution of the pre-UTI is necessary before operation. Decreased renal cortical thickness has been shown to be associated with an increased incidence of total complications, recurrences, and post-UTI. The results of previous studies are consistent with our analysis that the reduction of renal cortical thickness increases the risk of postoperative complications, UTI, and recurrence.26,71 This may be attributable to the fact that the reduced thickness of the renal cortex implies a more severe degree of hydronephrosis and impaired renal function. This can also be verified in collection systems. The rate of complications becomes higher with more severe collection system separations in our cohort, and the mean pyelocalix area was found to be associated with postoperative complications in a long-term follow-up. 30 DJ stent duration was found to correlate with recurrence, which may be attributable to local inflammation induced by prolonged physical irritation, resulting in scar formation. Obviously, removing the DJ tubes is not as early as possible. Therefore, the appropriate time of removal still needs to be further discussed. Duration of operation is significantly associated with recurrence. The duration of operation is related to the difficulty of the operation, and factors such as severe adhesions may prolong operation time. This may be attributed to higher local leakage and the formation of aseptic inflammation, which aggravates scar formation.
In addition, a meta-analysis of predictors identified four factors associated with the development of complications. Male sex was identified as a risk factor for complications. Previous studies have found a higher incidence of UTI in males than in females,26,72 but there are also studies that show a higher incidence of UTI in females. 73 In conclusion, the point about the association between gender and complications is controversial, which was the motivation for our meta-analysis, and we ultimately concluded that being male is a risk factor for postoperative complications. This may be because of the differences in microbiological profile and antibiotic susceptibility between males and females. The urinary tract pathogens isolated from male patients are more resistant to antibiotics than those from females. 74 Open operation was associated with the lowest complication rate of all surgical modalities, and laparoscopic operation had the highest complication rate among all surgical approaches. However, this result was obtained by analyzing data from the published literature. Although we screened through the literature, we could not completely exclude the effect of confounding factors such as age. Notably, children with SRF <40% had fewer postoperative complications. This is contrary to our findings for renal cortical thickness. This may be attributable to the fact that patients without loss of renal function tend to present with more severe clinical symptoms or recurrent UTI, which motivates them to undergo operation. Further studies are required to explain this phenomenon.
The cohort study revealed that the causes of each complication are different. Therefore, the risk factors of different complications should be analyzed separately. However, in the meta-analysis, we were unable to analyze the risk factors separately, as most of the studies investigated the risk factors for total complications. Therefore, we could only analyze the predictors of total complications. This may be because of the small sample size in most of the studies, resulting in an insufficient number of various complications. Besides these factors that were included in the meta-analysis, duration of DJ stent, 75 delayed operation, 76 and premature delivery 22 have also been reported to be potentially associated with the development of complications.
In contrast to similar studies, two systematic reviews and meta-analyses of pyeloplasty outcomes by Valentina Cascini 77 and Riccardo Autorino 9 et al. found no significant differences in the complication and failure rates between minimally invasive procedures and open procedures. We included more studies and obtained a different conclusion. A meta-analysis by Liu et al. found no significant difference between DJ, external stented, and stent-less procedures in terms of total complications, but DJ-stented cases had the lowest incidence of urine leakage. 3 This is consistent with our study.
This study has many strengths. This is the first meta-analysis of predictors of postoperative complications of pyeloplasty involving a large sample. And we have identified a number of risk factors for complications. However, some limitations of our study should be acknowledged. Our clinical data cover a longer period and include a wide age range of patients, because we considered all of these surgeries to be performed using a uniform surgical approach. Therefore, we consider that the heterogeneity with respect to surgical approaches is small. Some indicators such as differential renal function were not included in our retrospective study because of a large amount of missing data. Technologies such as robotics and laparoscopy were only analyzed as a factor rather than a subgroup. Because of data limitations of previously published studies, we were unable to analyze many factors that we were concerned with in our meta-analysis such as UTI. In addition, we included patients across a wide range of ages, leading to the possibility of some confounding factors in this. This made our cohort study less comparable with the results of the meta-analysis.
Conclusions
This study identified several predictors of total postoperative complications, recurrence, and UTI after pyeloplasty. Therefore, adequate resolution of UTIs prior to operation is necessary, and closer follow-up is required in children who are male and have reduced renal cortical thickness.
Authors’ Contributions
X.Z.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, validation, writing—original draft, and visualization. Y.Z.: Conceptualization, formal analysis, methodology, project administration, resources, supervision, and writing—review and editing. C.M.: Formal analysis and writing—review and editing. W.W.: Data curation, formal analysis, and investigation. D.S. and Q.X.: Data curation, formal analysis, methodology, and visualization. Y.L., J.H., X.R., and L.Z.: Formal analysis and investigation. G.S. and X.L.: Formal analysis, investigation, and methodology. Z.S., G.M. and Y.J.: Methodology and writing–—review and editing. Z.Z.: Methodology and formal analysis. A.L.: Conceptualization, formal analysis, funding acquisition, methodology, project administration, resources, supervision, and writing–—review and editing.
Footnotes
Author Disclosure Statement
The author states that there are no conflicts of interest.
Funding Information
Financial support was provided by the Qilu Medical Development Fund of Shandong University (34641390220001).
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.