
Abstract
Introduction:
Sarcopenia, the generalized loss of muscle mass, has been linked to outcomes across various medical specialties, but remains understudied in Endourology. This study aimed to evaluate whether sarcopenia serves as a prognostic indicator in elderly patients undergoing percutaneous nephrolithotomy (PCNL).
Patients and Methods:
Patients ≥70 years who underwent PCNL between January 2021 and December 2022 were identified retrospectively. Sarcopenia was determined using preoperative CT. Postoperative outcomes were compared between sarcopenic patients and non-sarcopenic controls.
Results:
A total of 234 patients were included, with 148 (63%) meeting criterion for sarcopenia. There was no difference in mean age, co-morbidities, or cumulative linear stone burden (18.8 mm vs. 20.5 mm, p = 0.21) between the groups; however, sarcopenia was significantly more prevalent among men compared to women (77% vs 47.2%, p < .001). Patients with sarcopenia experienced higher rates of Clavien–Dindo grade ≥2 complications (20% vs 8%, p = 0.02) compared to controls and trended toward higher rates of perioperative transfusions (7% vs 1%, p = 0.06). Unanticipated ED visits were higher among patients with sarcopenia (24% vs 9%; p = 0.01). On multivariate analysis, patients with sarcopenia were 2.8 times more likely to experience complications (odds ratio = 2.78, p = 0.024) and had a 43% longer hospital stay (time ratio = 1.43, p = 0.01).
Conclusions:
Sarcopenia is associated with less favorable perioperative outcomes in elderly patients undergoing PCNL, with higher complication rates, increased emergency room visits, and prolonged hospital stays. We present a novel risk-stratification tool to help identify patients at increased risk of adverse events after PCNL, which may serve as a valuable adjunct in perioperative risk estimation and preoperative counseling in this high-risk population.
Keywords
Introduction
Kidney stones affect approximately 10% of the US population and are estimated to cost the health care system over $5 billion in annual expenses. 1 The prevalence of nephrolithiasis increases steadily with age, rising to 20% among men over age 80. 2 Percutaneous nephrolithotomy (PCNL) is the treatment of choice for large and complex kidney stones with stone-free rates ranging from 80 to 90%. 3 Advancements in surgical technique and superior stone-free rates justify its use in smaller stones over ureteroscopy. 4 A limitation of PCNL is the potential for serious complications such as transfusion, pseudoaneurysm formation, and visceral/pleural injury.
Elderly patients pose unique perioperative challenges. These patients have diminished cardiac reserve and limited ability to respond to hemodynamic changes during surgical procedure. 5 Age-related cognitive decline also predisposes to postoperative delirium and may prolong recovery. Age is an independent risk factor for all-cause mortality after surgical procedure. 6 Specific to kidney stone disease, prior groups have reported that PCNL is safe in elderly patients with similar complication rates to a matched younger cohorts.7,8 These studies, however, may have selection bias in the elderly patients who were recommended surgery.
When selecting patients for PCNL, the importance of achieving stone-free status must be weighed against a patient’s competing co-morbidities and the relatively higher invasiveness of PCNL. Accurate perioperative assessment relies on multiple factors including a patient’s functional status and co-morbidities, collectively termed frailty. 9 Assessing frailty often requires a multidisciplinary approach, which may not be practical within the workflow of many surgical practices. This has prompted several investigators to explore alternative objective and reliable methods for assessing a patient’s risk of adverse outcomes at the point of care.
Sarcopenia is defined as the loss of skeletal muscle mass and can be easily measured using software algorithms and cross-sectional imaging. 10 The presence of sarcopenia has been established as a predictor of outcomes in many other disease states, such as bladder cancer, 11 prostate cancer, 12 colorectal surgery, 13 and others. 14 It has also been correlated with risk for complications after neoadjuvant chemotherapy in bladder cancer. 15 Sarcopenia may serve as a practical tool to estimate perioperative risk in kidney stone surgery because nearly all patients have recent cross-sectional imaging available. Yet, no groups have determined if the presence of sarcopenia is associated with adverse outcomes after kidney stone surgery. Here, we compared outcomes in sarcopenic and non-sarcopenic patients over 70 years old undergoing PCNL.
Patients and Methods
We retrospectively identified patients aged ≥70 years who underwent PCNL at our high-volume, multi-site institution between 2021 and 2022. Inclusion required an abdominal CT scan performed within 1 year prior to surgical procedure. A chart review was performed to collect demographic variables, comorbidities, operative characteristics, and perioperative complications. PCNL was performed in the prone position, and percutaneous renal access was obtained using either fluoroscopy alone or in combination with ultrasound guidance. Tracts were dilated to either 16F/18F (mini-PCNL) using co-axial sheaths or balloon dilated to 24F/30F (conventional PCNL). In cases of mini-PCNL, laser lithotripsy was performed using either Ho:YAG or thulium fiber laser, and ultrasonic lithotripsy was utilized for conventional PCNL. The decision to perform mini or conventional PCNL was determined by surgeon preference.
As described in prior studies, total skeletal muscle area was calculated from preoperative axial CT images at the mid-L3 vertebral level using Aquarius Intuition software (TeraRecon Inc, Durham, NC, USA). 15 Thresholds of −29 to 150 Hounsfield units were used to define skeletal muscle. Boundaries between skeletal muscles were generated automatically by the software and subsequently verified and corrected as required by 2 trained observers (H.Y. and V.C.) using an established protocol. 15 Skeletal Muscle Index (SMI) was calculated by dividing the L3 skeletal muscle area by height squared (cm2/m2) (Fig. 1). Sarcopenia was defined using preestablished gender-specific thresholds (male: SMI < 52 cm2/m2; female: SMI < 39 cm2/m2). 16
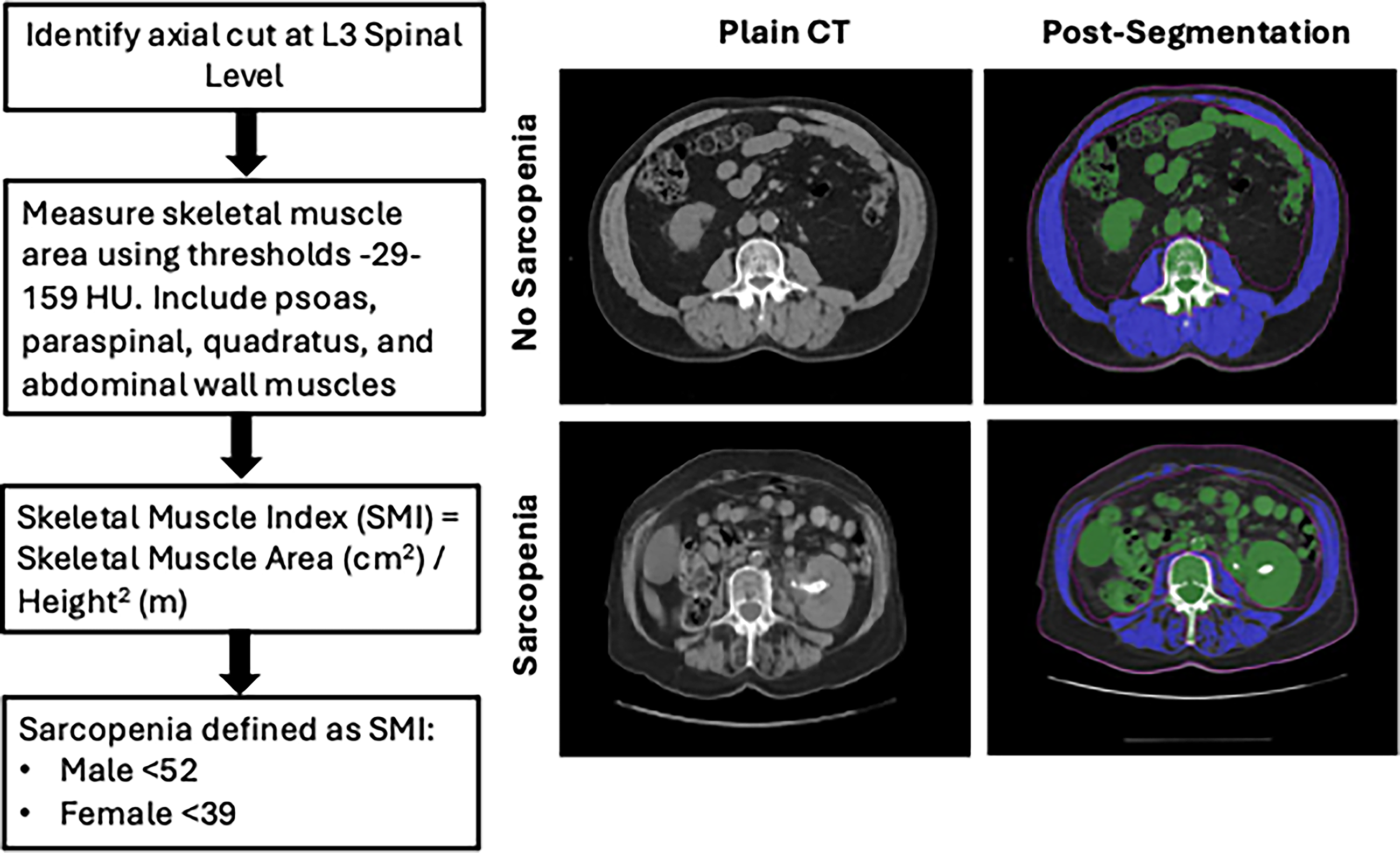
Approach used to measure sarcopenia using non-contrast CT scans of the abdomen. Representative axial CT images at mid-L3 are displayed above for male patients with and without sarcopenia. CT = computed tomography.
Baseline patient characteristics, operative variables, and outcomes are reported as frequencies (%) or mean (± standard deviation) according to sarcopenia status. Comparisons between groups for continuous and categorical variables were performed using the Wilcoxon rank-sum test and the chi-squared test, respectively. Fisher’s exact test was applied when categorical variables had low cell counts. Multivariable logistic regression was used to evaluate the association between sarcopenia status and perioperative complications, with odds ratios (ORs) and 95% confidence intervals (CIs) estimated, adjusting for potential risk factors. A multivariable Cox proportional hazards model was used to compare the length of stay between patients with or without sarcopenia. The proportional hazards assumption was assessed using the Schoenfeld residual test. Restricted mean time ratios (TRs) were estimated via 1000 bootstrap resamples, adjusting for covariates. Variables included in the multivariable models were selected based on univariate models of preoperative demographic and perioperative variables using the Bayesian Information Criteria, with sarcopenia included a priori. Both 95% confidence intervals and p values for TRs were estimated using bootstrapping. A p value < 0.05 was considered statistically significant. All tests were two-sided. Statistical analysis and figures were generated using R (version 4.5.0; R Foundation for Statistical Computing, Vienna, Austria; www.R-project.org).
Results
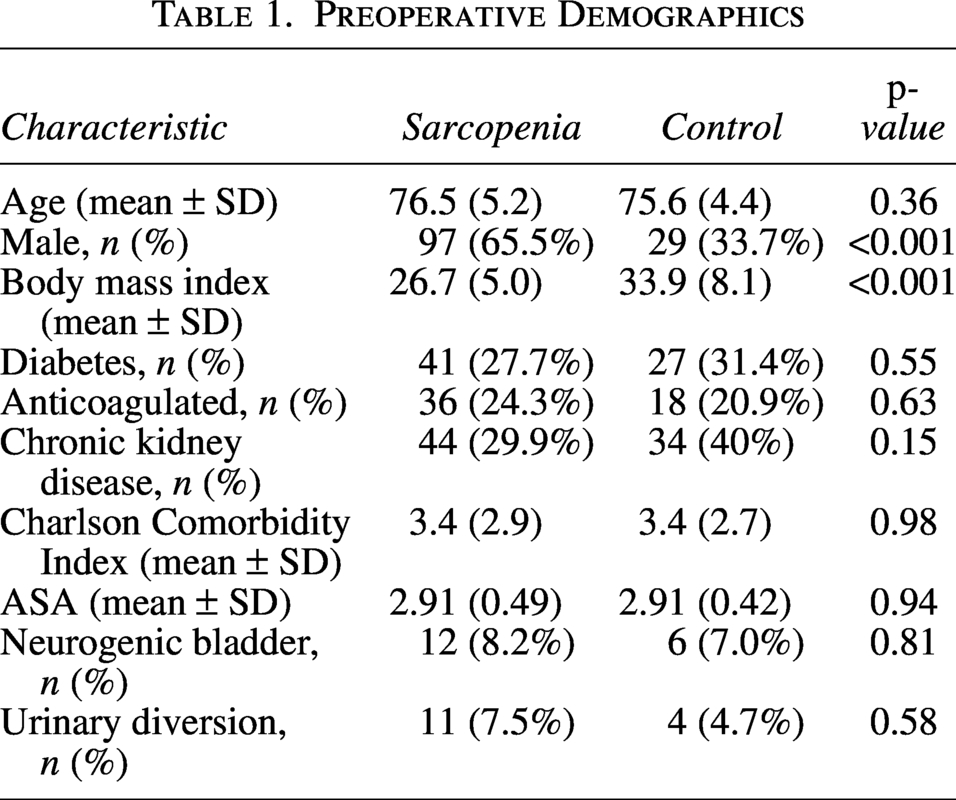
Our study cohort consisted of 234 patients above age 70 who underwent PCNL, of which 63% met criteria for sarcopenia. The mean SMI was 45.7 for males vs 39.3 for females. Male patients were more likely to be sarcopenic (77% vs 47.2%, p < 0.001). Otherwise, there were no differences in age or preoperative comorbidities (Table 1). Mean American Society of Anesthesiologists (ASA) score and Charlson Co-morbidity Index were also similar between groups. Mean linear stone burden was 18.8 mm vs 20.5 mm for sarcopenic and non-sarcopenic patients, respectively (p = 0.21; Table 2). Thirty-two percent of cases were performed using a miniaturized sheath (<20F) in the sarcopenia group compared to 21% in the control group (p = 0.1). The frequency of upper pole and multiple accesses was 26%–28% and 1% in both groups, respectively.
Preoperative Demographics
Intraoperative Variables
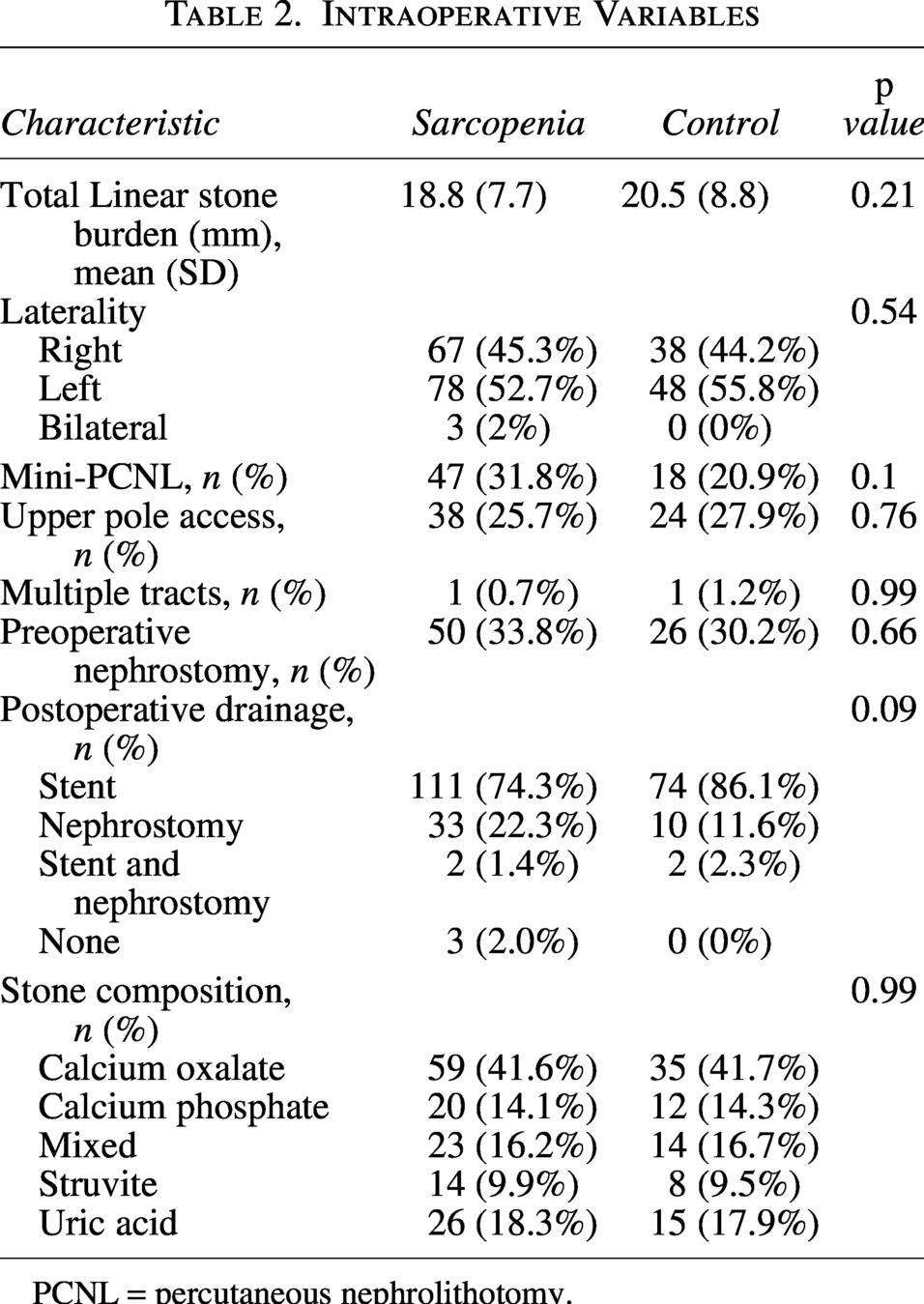
PCNL = percutaneous nephrolithotomy.
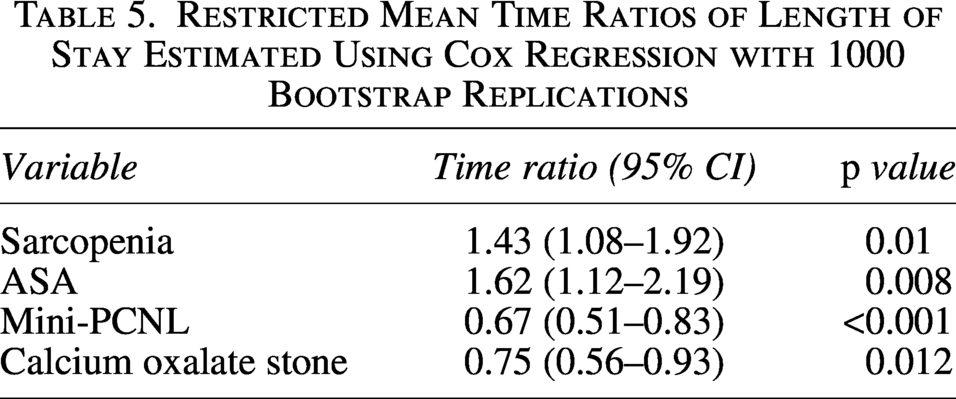
The presence of sarcopenia was associated with a significantly higher risk for Clavien–Dindo ≥ 2 complications (20% vs 8%; p = 0.02; Table 3). Bayesian Information Criteria was used to identify other pre- and intraoperative variables that were associated with complications in this population. Of the variables collected, only anticoagulation status and sarcopenia were associated with risk for complications and were used to build a multivariate model. According to this model, sarcopenia independently conferred a 2.8-times higher risk for Clavien–Dindo ≥ 2 complications (OR = 2.78, 95% CI: 1.2–7.21, p = 0.024; Table 4). Patients with sarcopenia also trended toward longer length of hospital stay (2.4 vs 1.6 days). However, after adjusting for preoperative disease severity, operative procedures, and stone composition, sarcopenia was significantly associated with 43% longer hospital stay (TR = 1.43, 95% CI: 1.06–1.92, p = 0.01; Table 5). Other variables that were associated with shorter length of stay included lower ASA score and use of a miniaturized sheath. Sarcopenic patients had a sevenfold higher risk of needing a blood transfusion (7% vs 1%, p = 0.06) and were significantly more likely to have a 30-day emergency department (ED) visit (24% vs 9%, p = 0.01). The most common complication was urinary tract infection (n = 19, 8%). Six patients needed postoperative admission to the intensive care unit (2.6% overall), 5 of whom met criteria for sarcopenia. Pleural effusions and pseudoaneurysms occurred in 2% and <1% of cases, respectively. No patients experienced mortality within 30 days of surgical procedure.
Postoperative Outcomes
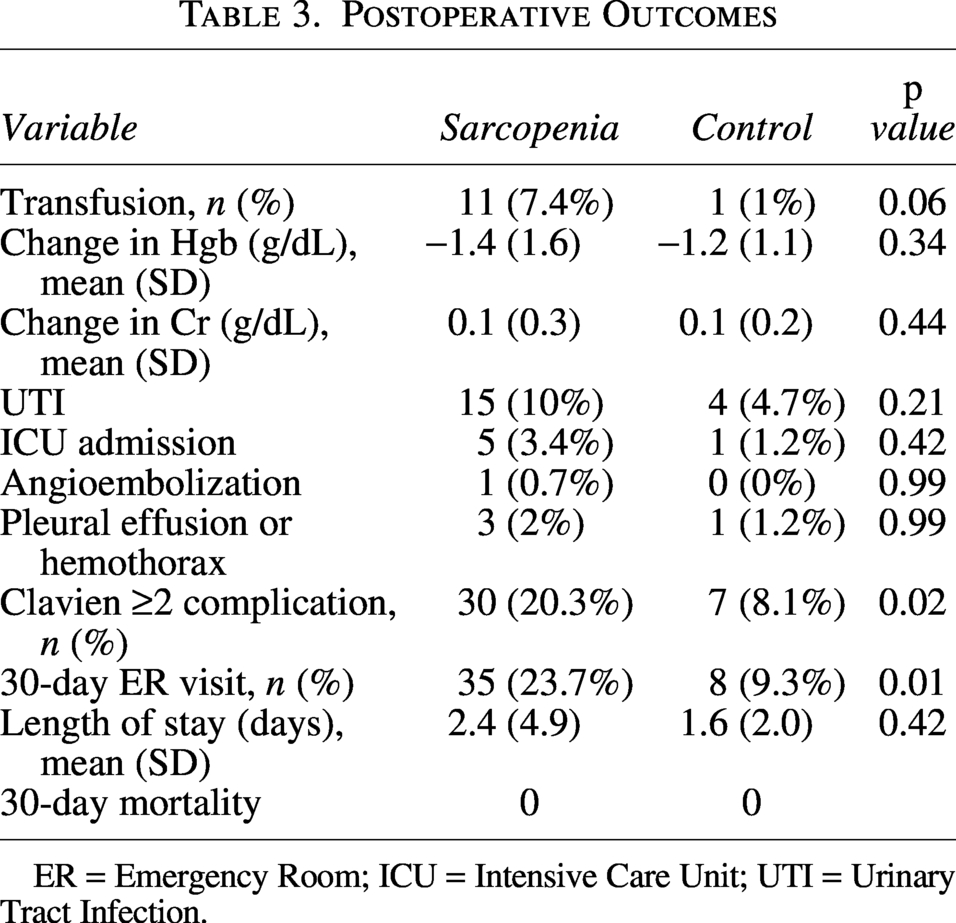
ER = Emergency Room; ICU = Intensive Care Unit; UTI = Urinary Tract Infection.
Multivariable Logistic Regression Analysis of Clavien–Dindo Grade II–IV Complications
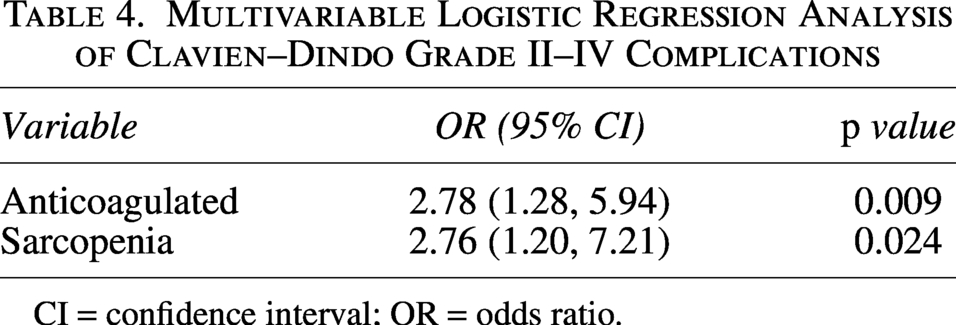
CI = confidence interval; OR = odds ratio.
Restricted Mean Time Ratios of Length of Stay Estimated Using Cox Regression with 1000 Bootstrap Replications
Discussion
Older patients are undergoing an increasing number of surgical procedures, and surgeons will more frequently find themselves having to weigh the risks and benefits of procedures in patients with complex co-morbidities and frailty. 17 Sarcopenia is becoming recognized as an important predictor of outcomes in geriatric patients across several disease states. In this study, we demonstrate an association between sarcopenia and adverse postoperative outcomes in elderly patients undergoing PCNL. Patients with sarcopenia were more likely to experience serious postoperative complications, prolonged hospital stays, and increased emergency department visits. Prior groups have examined the outcomes of geriatric patients undergoing PCNL. Abedali et al. concluded that while octogenarians were more likely to experience a perioperative complication (over twofold) compared with a matched younger cohort, the safety profile was acceptable. 7 The majority of these complications were bleeding-related and similar in frequency to that observed in our cohort (5–10%). A similar study found no differences in complication rates among extremely elderly patients (mean age 88 years), despite a higher prevalence of comorbidities and preoperative sepsis. 18
Surgical management of large renal stones in geriatric patients is important for preserving renal function, alleviating pain, and eliminating a potential source of infection. In this population, the decision to proceed with surgical procedure requires careful consideration of surgical risks relative to comorbidities and functional status. Geriatric assessments and frailty indices can provide a comprehensive picture of a patient’s functional status; however, these are often time-consuming and may not be practical in the clinical setting. Bhatia and colleagues prospectively screened patients undergoing PCNL for frailty using the Hopkins Frailty Index. 19 They found that patients meeting criteria for frailty were more likely to develop Systemic Inflammatory Response Syndrome, require ICU admission, and have a longer hospitalization. Unique to this study, one-half of frail patients were discharged to a higher level of care (i.e., rehab, skilled nursing facility). A limitation of their study is the use of a frailty index that relies on measurements not routinely obtained in the Urology clinic, such as grip strength.
The presence of sarcopenia may help simplify patient assessment by acting as an objective, point-of-care index to estimate perioperative risk in elderly kidney stone patients. Prospective studies have linked sarcopenia with overall mortality and the need for hospitalization. 20 Although there is debate on the optimal method to define sarcopenia, cross-sectional imaging is regarded as one of the gold standards. 21 In Oncology, sarcopenia identified on CT has been consistently correlated with outcomes in bladder, kidney, and colorectal cancer.
Accurately estimating perioperative risk is important in elderly patients with complex kidney stones. According to American Urological Association guidelines, PCNL is the treatment of choice for stones greater than 2 cm3. It also affords superior stone-free rates compared to ureteroscopy for stones 1–2 cm. Maximizing the stone-free rate is important in elderly patients to alleviate symptoms and reduce the risk of infection and stone-related events. However, this goal must be balanced against the realities of limited life expectancy, competing comorbidities, and increased perioperative risk in this population. In our dataset, sarcopenia emerged as one of the few preoperative variables associated with adverse outcomes, conferring an approximately 2.5-fold increased risk of serious complications on both univariate and multivariate analysis. Sarcopenia may serve as a useful marker to guide counseling of comorbid elderly patients when choosing between PCNL and alternative management strategies such as observation or ureteroscopy. Given the routine use of cross-sectional imaging in stone patients, sarcopenia offers a practical and accessible tool for estimating perioperative risk. Several image analysis software programs such as Aquarius and Fuji Synapse are integrated in hospital film libraries. Some groups have also started to develop artificial intelligence algorithms for the measurement of skeletal muscle mass and this may help further simplify and expand the use of sarcopenia. 22 As Endourology advances toward automated imaging tools for metrics like stone volume, sarcopenia measurements could be integrated into point-of-care software to provide rapid, accurate estimate of an elderly patient’s risk for adverse outcomes after PCNL. Further studies are needed to validate the accuracy of such software and its predictive value for perioperative complications in a prospective cohorts.
The prevalence of sarcopenia was notable in our cohort, with over 60% of patients fulfilling criteria for sarcopenia. Other studies estimate that sarcopenia affects 10%–15% of the elderly population but can approach 70% in series with cancer patients. 16 Zhang et al. compared the likelihood of kidney stones in patients with and without sarcopenia on dual-energy X-ray absorptiometry scan who were enrolled in the National Health and Nutrition Examination Survey (NHANES). 23 After propensity score matching, they report a significant association between sarcopenia and the development of kidney stones patients. Whether there is a direct causal link between muscle wasting and kidney stone formation remains to be determined and could provide insight into the increasing incidence of nephrolithiasis with age. Elderly patients also tend to form larger stones with atypical compositions, a finding which could be related to changes in musculoskeletal metabolism. 2 Despite this, we did not identify any associations between stone composition and sarcopenia in our cohort.
This study is limited by its retrospective design. As with most surgical series in elderly patients, our cohort includes only those deemed fit for surgical procedure and may not represent the broader elderly population with kidney stones. It is possible that the frailest—and thus, most sarcopenic—patients were not offered PCNL, and therefore not captured in our study, potentially underestimating the predictive value of sarcopenia. Additionally, we are unable to compare sarcopenia with other established measures of perioperative risk, such as frailty indices, in this population. Lastly, we were unable to accurately capture stone-free rates because of heterogeneity in postoperative imaging protocols. However, the efficacy of PCNL in elderly patients has been previously published 7 and its superiority compared to other kidney stone treatments has been established in prospective randomized controlled trials. 4 Nonetheless, this does not limit the applicability of findings in this study, given that the objective was to evaluate sarcopenia as a predictor of perioperative complications in elderly patients undergoing PCNL.
Conclusions
Preoperative sarcopenia is associated with increased complication rates, prolonged hospital stay, and higher emergency department utilization in geriatric patients undergoing PCNL. Quantifying skeletal muscle mass on preoperative CT offers a practical, point-of-care tool for perioperative risk assessment and may enhance shared decision-making in this vulnerable population. Prospective validation and incorporation into automated imaging platforms could further establish sarcopenia as a cornerstone of precision risk assessment in Endourology.
Authors’ Contributions
Article writing: C.C., J.L., and S.S. Data collection and analysis: C.C., H.Y., V.C., A.T., L.H., J.L., and S.S. Critical review of article: J.G.-A., A.Z., and S.D. Study Conception: C.C., L.H., J.G.-A., A.Z., S.D., and S.S.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no external funding.