
Abstract
Introduction:
Holmium:yttrium-aluminum-garnet (Ho:YAG) laser is the gold standard for ureteroscopic lithotripsy, but faces challenges such as stone retropulsion. The emerging thulium fiber laser (TFL) offers advantages, including higher efficiency, smaller fiber size, and reduced retropulsion. Our study aims to compare the stone ablation efficiency of TFL and Ho:YAG laser.
Method:
This study is a prospective, single-center, randomized controlled trial comparing TFL and Ho:YAG laser for ureteral stone lithotripsy in 35 patients. The primary outcome is stone ablation efficiency, with secondary outcomes including total operation time and laser time, the degree of retropulsion, clarity of endoscopic view, hospital stay, 30-day complications, 3-month stone-free rate, and requirement for auxiliary procedure. The stone-free rate is defined as the absence of detectable stones on a post-operative noncontrast CT scan conducted 3 months after the procedure.
Result:
Sixteen patients and 19 patients were randomized in the Ho:YAG group and TFL group, respectively. Patient demographics were comparable except for more men in the TFL group (81.3% vs 68.4%). The stone ablation rate (the volume of stone ablated per minute of laser time) was comparable between both groups (1.12 mm³/s for the TFL group and 1.33 mm³/s for the Ho:YAG group, p = 0.772). TFL had shorter laser time (3.02 vs 5.78 minutes, p = 0.013), less retropulsion (p = 0.048), and a higher stone-free rate (100% vs 78.9%, p = 0.0015).
Conclusions:
Lithotripsy using a thulium fiber laser achieves a stone ablation rate comparable to that of the holmium:YAG laser. The thulium fiber laser results in a higher stone-free rate while keeping complication rates similar.
Introduction
Ureteral stones are often treated with ureteroscopic lithotripsy (URSL). The holmium:yttrium-aluminum-garnet (Ho:YAG) laser represents the gold standard for intracorporeal lithotripsy during URSL, as it can be used with instruments with small working channels and flexible instruments.
However, Ho:YAG laser lithotripsy has potential drawbacks. First, it causes more stone retropulsion, which leads to residual stones and increases treatment costs. Moreover, the maximum pulse rate of Ho:YAG laser machines limits the power delivery. Recently, high-power machines have provided options for higher pulse rates, but this comes at the cost of a bulkier and noisier design, as these machines require additional laser cavities and a more complex cooling system. Consequently, they are also more susceptible to damage from shocks. 1
The thulium fiber laser (TFL) has been introduced for lithotripsy in endourology.2,3 When operated in pulsed mode, the high-power TFL can effectively fragment various types of urinary stones. This capability makes it a versatile laser system suitable for multiple applications in urology, including the ablation of both soft and hard stones and tissues. 3
The TFL offers potential advantages: First, its wavelength aligns closer with the water absorption peak than that of the Ho:YAG laser, and this difference enhances stone ablation efficiency, as demonstrated in laboratory studies. 4 Additionally, TFL exhibits less retropulsion compared to the Ho:YAG laser. 4 Moreover, TFL fibers can be as small as 150 µm, while Ho:YAG fibers are typically 200 µm or larger. The smaller size of TFL fibers occupies less space in the working channel of endoscopes, facilitating better irrigation flow and improving the endoscopic view. Last, the TFL operates using a standard electrical outlet while delivering a power output comparable to that of a high-power Ho:YAG laser machine, but with a significantly higher pulse rate of up to 2000 Hz.
Several clinical studies investigating the efficacy of TFL and Ho:YAG laser have been published with conflicting results, while most of them included both renal and ureteral stones. Ulvik et al. showed that TFL provides a shorter operation time, higher stone-free rates, and less intraoperative bleeding when compared to a 30 W single pulse Ho:YAG laser machine 5 ; Haas et al., using a high-power 120 W pulse modulated (Moses) Ho:YAG laser machine, showed equivalent stone-free rates and laser times, but showed less energy required for the Ho:YAG laser group. 6
Regarding ureteral stones alone, only two randomized clinical trials are available to compare efficacy between TFL and Ho:YAG laser.7,8 Both studies have notable limitations: one did not include data on stone ablation efficiency, measured in terms of volume per laser time used, 7 and the other lacked standardization, as different sizes of endoscopes were utilized. 8 The current study compares TFL and Ho:YAG laser regarding stone ablation efficiency when treating ureteral stones.
Methods
Study design
This is a prospective, single-center, randomized trial comparing the effectiveness of TFL and Ho:YAG laser for URSL in patients with ureteral stones. The research is conducted in accordance with the Declaration of Helsinki, has been approved by the local ethics committee, and is registered on ClinicalTrials.gov (ID: NCT05218057).
Patients
Patients were recruited between July 2022 and September 2023. We screened all consecutive patients diagnosed with ureteral stones through noncontrast computed tomography (NCCT) for eligibility in this study. We included patients who are older than 18 years with informed consent. The following exclusion criteria were applied:
Patients on anticoagulant therapy Patients with conditions that increase the risk of urolithiasis (e.g., cystinuria, hyperparathyroidism, prior intestinal resection) Patients with abnormal urinary tracts (e.g., ileal conduit, neobladder, ureteral stricture) Patients with stones larger than 15 mm Patients with multiple ureteral stones Patients on Double-J stents
Informed consent was obtained from all eligible study subjects before their scheduled operations.
Randomization, allocation concealment, and blinding
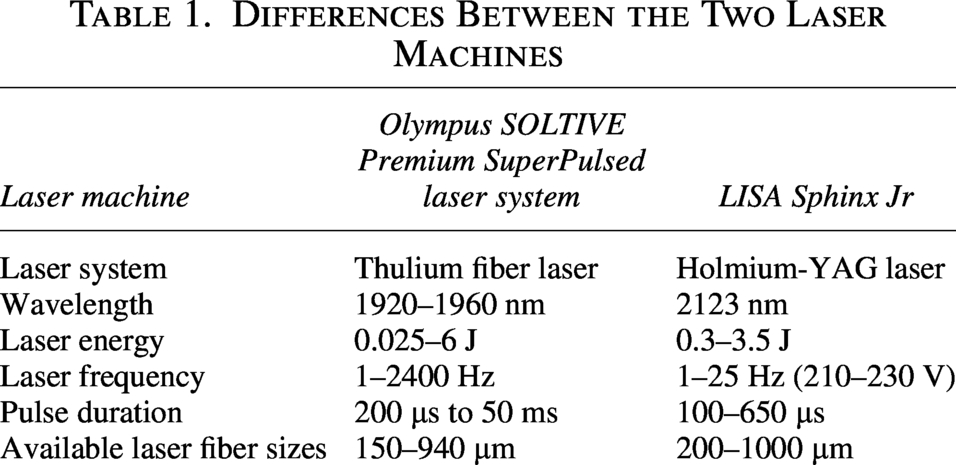
Patients were randomly assigned to receive URSL using either a TFL in Group 1 or a Ho:YAG laser in Group 2, with an allocation ratio of 1:1. Randomization was conducted using a computer-generated sequence of random numbers arranged in permuted blocks of varying sizes. Although the urologist performing the surgery could not be blinded because of the nature of the intervention, the patients receiving treatment and the investigators evaluating the outcomes were blinded to the allocated treatment arm. In Group 1, the TFL utilized was the Olympus SOLTIVE Premium SuperPulsed laser system, equipped with a 365-µm laser fiber. The laser pulse settings could be set to any combination up to 10 W, while the only limitation is that the combination has to be available in the Ho:YAG laser machine. In Group 2, the Ho:YAG laser used was the LISA Sphinx Jr laser system, featuring a 365-µm laser fiber. The pulse settings for this laser were adjusted to any combination up to 10 W (with the shortest pulse duration available on the machine). The differences between the two laser systems are summarized in Table 1.
Differences Between the Two Laser Machines
Procedures
Patients fasted for at least 6 hours before the procedure. Prophylactic intravenous antibiotics were administered prior to the intervention. All procedures were performed by urology specialists under general, spinal, or local anesthesia. Patients were placed in the lithotomy position. Under gravity, warmed (37°C) 0.9% normal saline was used to irrigate the patient, set at a 60 to 80 cm height above the patient. Pressure irrigation was applied as needed by the operating urologist. A 6/7.5F semi-rigid ureteroscope was utilized.
The choice of laser was based on the randomization results. The operating urologist decided to perform stone dusting or fragmentation with extraction. For dusting, laser lithotripsy was performed with a lower pulse energy until the operating urologists were satisfied with the size of the fragments (e.g., <3 mm). For fragmentation with extraction, the laser lithotripsy was performed with a higher pulse energy, and the fragments are retrieved with forceps or a basket. 9
A Double-J ureteral catheter was inserted in all patients and removed within 4 weeks, based on clinical necessity. The operative time was defined as the time between the ureteroscope insertion and the completion of Double-J stent insertion. NCCT of the abdomen and pelvis was performed 3 months after the procedure to assess stone clearance.
Outcome measures
The primary outcome is the efficiency of stone ablation in terms of the stone ablation speed (preoperative stone volume/laser time expressed in cubic millimeters per second) and laser energy consumption (total laser energy/preoperative stone volume expressed in Joule per cubic millimeter). 10 Secondary outcomes include total operation time and laser time, the degree of retropulsion, clarity of endoscopic view, hospital stay, 30-day complications, 3-month stone-free rate, and requirement of auxiliary procedure. The stone-free rate is defined as the absence of residual fragments on the postoperative NCCT scan conducted 3 months after the procedure.
Statistics and sample size analysis
The primary analysis included all randomized participants who fulfilled all eligibility criteria on central review (modified intention-to-treat population). To compare the baseline characteristics between the TFL and Ho:YAG groups, the independent-samples t test was used for parametric continuous variables, the Mann–Whitney U test for nonparametric continuous variables, and the chi-square test for categorical variables. The stone ablation speed was compared using the independent-samples t test. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using R version 4.1.1 or above.
For the sample size calculation, a previous clinical study by Martov et al. 7 reported a 47% reduction in laser time for the TFL group. The average stone size for both groups was not provided, making calculation of the stone ablation speed impossible. However, we can assume that the preoperative stone load is similar for both groups. Therefore, we estimate a 47% difference in the stone ablation speed. Using a significance level of 0.05, a power of 0.8, and an assumed standard deviation of 0.5, the required sample size is approximately 18.8 per group. Considering a 20% dropout rate, the required sample size increases to 23 per group.
Results
A total of 252 patients were assessed for eligibility, while we randomized 46 patients (23 patients in each group). However, seven and four patients did not receive the allocated intervention in the TFL and Ho:YAG groups, respectively (Fig. 1). Therefore, 16 and 19 patients from the TFL and Ho:YAG groups were included for the analysis. The age, mean body mass index (BMI), laterality, and position of the stones, stone density, and stone volume were comparable between the two groups. However, significantly more men were in the TFL group (81.25% vs 68.4%, p = 0.009). The patient demographics are presented in Table 2.
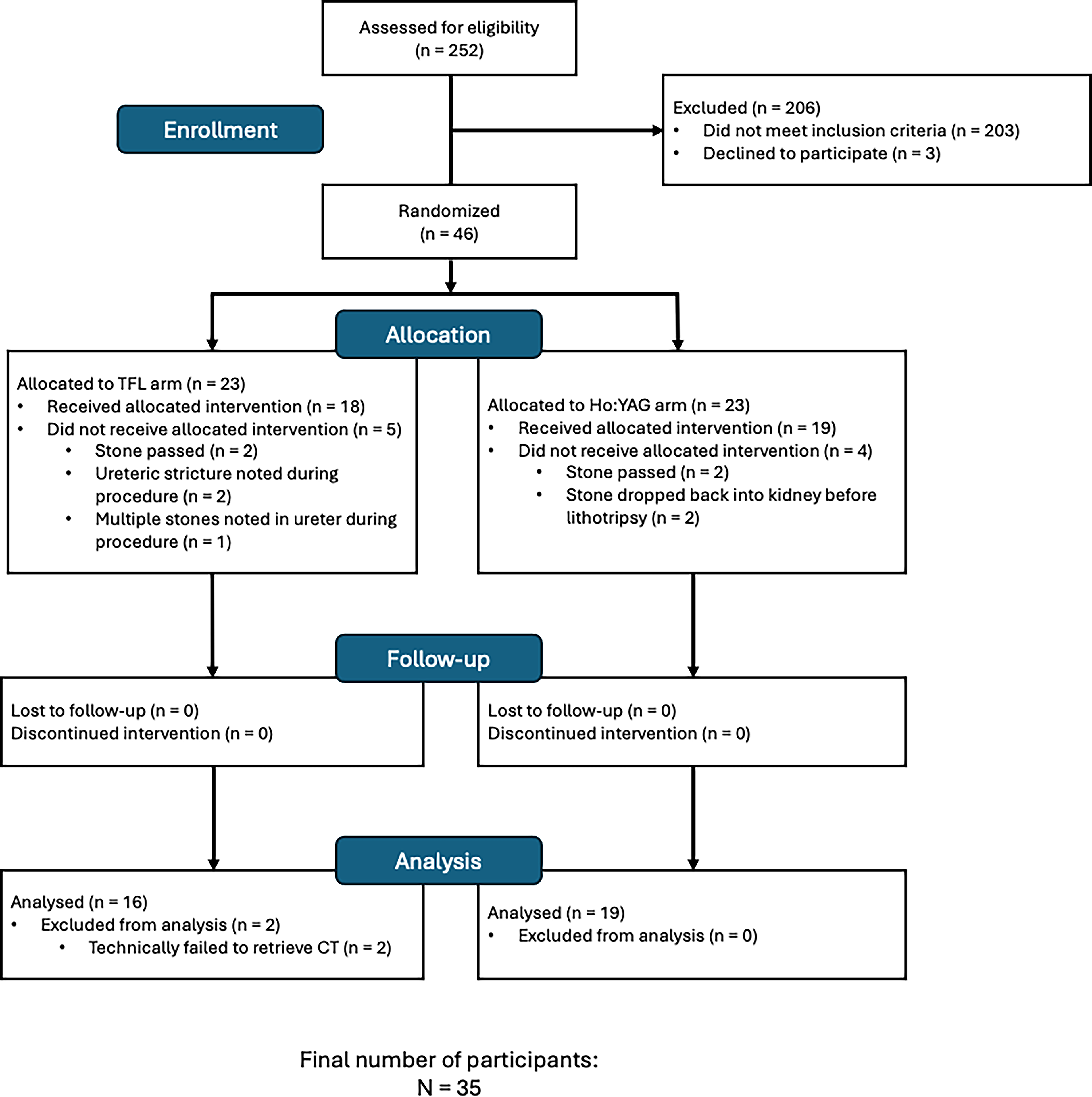
Consolidated Standards of Reporting Trials diagram of case flow through the study phases. Ho:YAG = holmium:yttrium-aluminum-garnet laser; TFL = thulium-fiber laser.
Patient Demographics
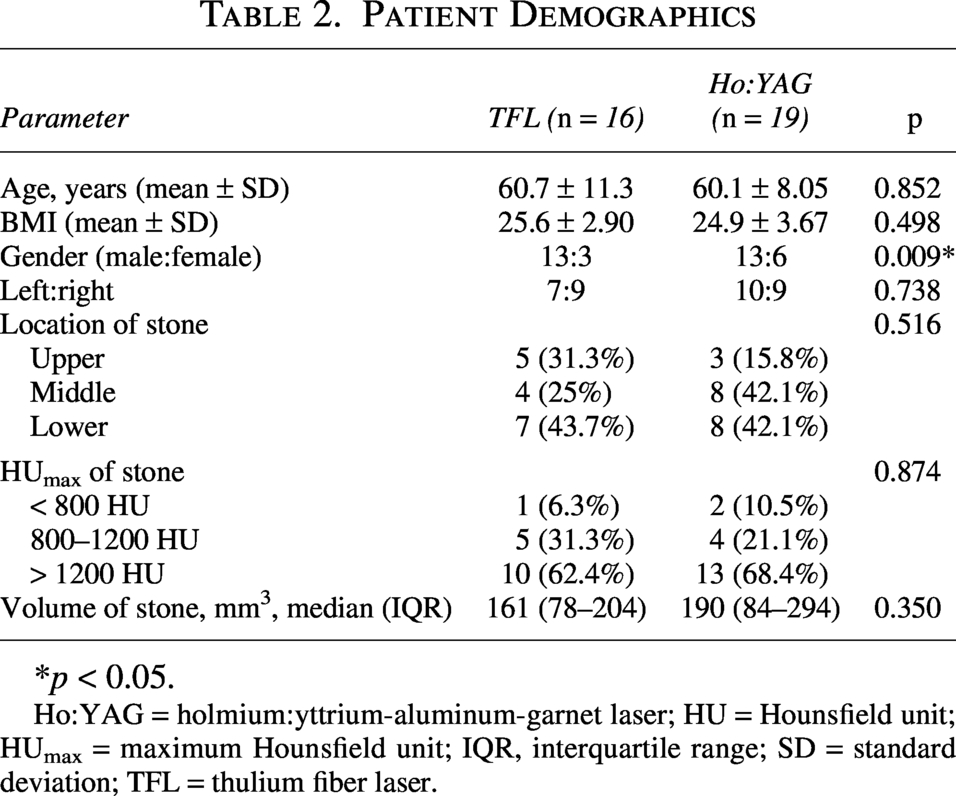
*p < 0.05.
Ho:YAG = holmium:yttrium-aluminum-garnet laser; HU = Hounsfield unit; HUmax = maximum Hounsfield unit; IQR, interquartile range; SD = standard deviation; TFL = thulium fiber laser.
The primary outcome, which consisted of efficiency measures, is presented in Table 3. The stone ablation speed (the volume of stone ablated per second of laser time) was comparable between groups (1.12 mm³/s for the TFL group and 1.33 mm³/s for the Ho:YAG group, p = 0.772).
Laser Efficiency Measures
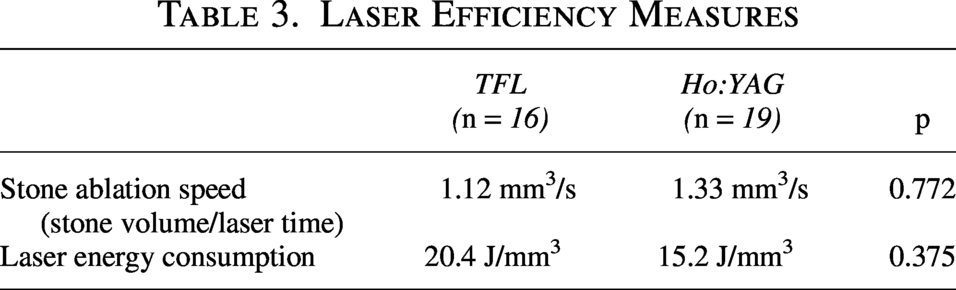
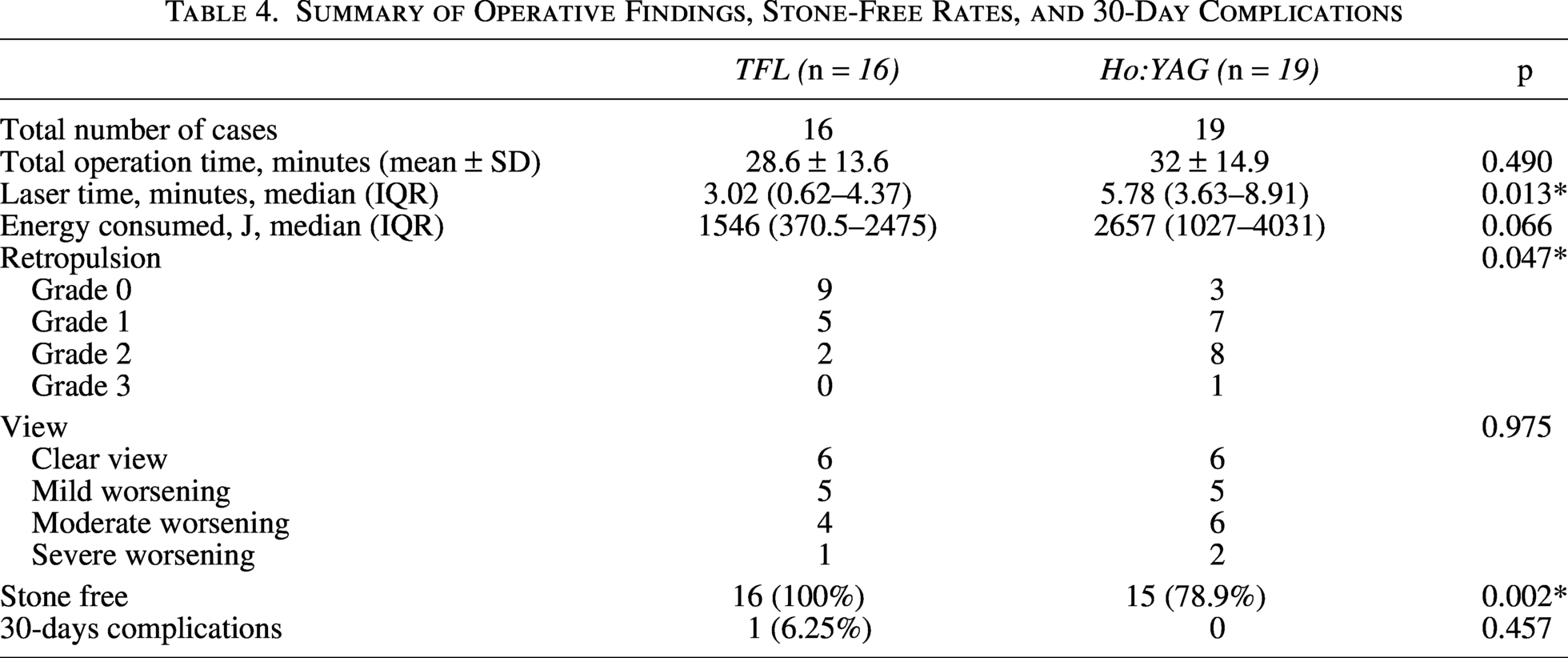
The laser energy consumption was 20.4 J/mm³ for the TFL group and 15.2 J/mm³ for the Ho:YAG group. There was no statistically significant difference between the two groups in these measures (p = 0.375). The laser time was significantly longer in the Ho:YAG group (5.78 minutes vs 3.02 minutes, p = 0.013). Otherwise, the total operation time and median energy consumed were similar between the groups. The Ho:YAG group exhibited significantly higher retropulsion, as assessed by the operating surgeon on a Likert scale (p = 0.047), while the clarity of endoscopic views remained similar (p = 0.9752). While all 35 patients had undergone the 3-month NCCT, the TFL group had a significantly higher stone-free rate than the Ho:YAG group (100% vs 78.9%, p = 0.002). The TFL group experienced one complication: the distal coil of the Double-J stent migrated proximally, requiring a ureteroscope to retrieve the stent. Otherwise, the complication rates were similar (p = 0.457). The secondary outcomes are summarized in Table 4.
Summary of Operative Findings, Stone-Free Rates, and 30-Day Complications
Discussion
Stone ablation speed
Andreeva et al. 4 demonstrated that, under the same laser energy and repetition rates, TFL produces two to three times higher ablation rates than Ho:YAG in laboratory settings. During laser lithotripsy, water in the pores of the stone expands and vaporizes as it absorbs the laser energy (photomechanical mechanism). Because of a higher water absorption coefficient, water absorbs TFL energy better than the Ho:YAG laser energy, showing better stone ablation speed.
However, our trial did not observe this increased ablation rate. Our findings align with a recently published study by Gupta et al., 8 which also reported no differences in ablation rates between the two groups. In contrast to laboratory conditions, where the goal is to produce dust that can pass through a 250-µm sieve, urologists typically aim to fragment stones into pieces measuring 2 to 3 mm in diameter in the ureter, allowing them to pass spontaneously. Since Ho: YAG produces more fragments >2 mm than TFL, 11 while TFL produces fragments <0.2 mm even with high pulse energy, 12 this could negate the efficiency advantages of TFL regarding higher ablation speed.
Laser efficiency may involve more factors other than only water absorption. Katta et al. 13 suggested that photons need to reach the stone to exert the ablation effect. When photons delivered from TFL have been absorbed by water between the laser fiber tip and the stone, no additional photons can reach the stone.
Our results did not show the benefits of TFL with shorter operative times as did Ulvik et al. 5 Our results are more consistent with those shown in Haas et al., who also showed a higher ablation speed and lower ablation efficiency (i.e., laser energy consumption in this article). 6 This could be because of the higher proportion of patients with ureteral stones in the Haas et al. group and similar laser power used (0.8 J and 8 Hz for fragmentation).
Stone-free rate and retropulsion
Andreeva et al. showed a higher peak power of Ho:YAG as the pulse energy increases. In contrast, the peak power of TFL is fixed, even when the pulse energy increases, which is similar to the peak power produced by a 0.2 J long pulse Ho:YAG. Higher peak power leads to greater force caused by the momentum of ablated stone fragments and axial water pressure, thus resulting in a higher retropulsion effect. 4
In our analysis of retropulsion, the Likert scale indicates that the TFL group exhibited significantly less movement of the stone, which aligns with findings from laboratory 4 and clinical studies.7,8 In contrast, the Ho:YAG group demonstrated a significantly higher retropulsion rate, which may contribute to a lower stone-free rate and a higher health care cost. Two patients had their stones dropped back into the kidney, and we changed to a flexible ureterorenoscopy to complete the procedure. This increases the overall treatment cost because of the use of flexible ureterorenoscopy (single-use or reusable ones) and the accessories (e.g., ureteral access sheath or baskets), lengthening the operation time and the anesthetic time. These two cases were excluded from the analysis as we focused on the ureteral stones’ ablation efficiency.
Furthermore, the Ho:YAG group had four patients with small residual fragments in the kidney that were not present preoperatively. Auxiliary procedures were arranged for these patients to render them stone free. However, the four patients preferred conservative management. This leads to the need for surveillance and a higher chance of stone growth or recurrence, as there is now a niche for the stone to grow. Whether or not we treat the residual fragments still requires an additional cost.
Laser time
We found the laser time for the Ho:YAG group was significantly longer than for the TFL group, corroborating the results of Martov and colleagues, 7 which showed a similar 47% difference. Their study showed that the operative time between the groups was statistically different. Their total operation time, less laser time, was similar in both groups; hence, the shorter operation time in TFL is attributed to the shorter laser time. Our study showed similar findings, albeit statistically insignificant, likely because of the small sample size.
Why our results opposes that in laboratory findings?
While the Ho:YAG group showed a numerically faster ablation rate (although statistically insignificant), and the TFL group showed shorter laser time could be contradictory, it could be a result that the TFL group has less retropulsion. Less retropulsion results in steady stone, leading to a shorter laser time in the TFL group. Nonetheless, our results are in keeping with that reported by Haas et al., 6 where the Ho:YAG group showed better stone ablation speed.
Besides, the stone ablation speed also depends on the composition of the stones. Our patients had a majority of stones with Hounsfield units >1200 (more than 60% in both groups), which implies harder stones like calcium oxalate monohydrate or calcium phosphate stones. Katta et al. 13 have shown that photons need to reach the stone to exert the lithotripsy effect, and TFL works best when it is in contact with the stone. As it is difficult for TFL to stay in contact with the stone, the photons will be absorbed by water while traveling away from the fiber tip and do not reach the stone, resulting in less efficient lithotripsy. In contrast, the Ho:YAG laser performs better in partitioning fluid between the fiber tip and stone, allowing more photons to reach the stone for lithotripsy. This could be the reason the Ho:YAG group was more efficient in our result.
Strengths
One of the strengths of our study is that we maintained a well-controlled environment to compare the two types of lasers, using the same set of instruments and the same group of surgeons. The only variable between the two groups was the laser machine used. Besides, we only included ureteral stones with a strict inclusion criterion to provide a homogeneous population to compare the two laser machines. Additionally, we utilized NCCT scans both before and after the procedure to assess stone volume and determine the stone-free status. This type of imaging allowed us to calculate the ablation rate of the stone accurately.
Limitations
Our study has several limitations. First, the dropout rate was higher than anticipated. We initially considered a 20% dropout rate; however, the stone passage rate exceeded our expectations because of prolonged operation waiting times caused by cancellations of operating theatres during the COVID-19 era. This brings us to another point: stones may spontaneously pass even after 8 weeks, which warrants further investigation. Second, while there is a guideline for laser settings (maximum of 10 W), it is not a fixed standard. This flexibility for the operating urologist (to choose the laser setting and whether to fragment and basket or purely dust the stone) can affect the primary outcome of this study, which means that direct comparisons between the two lasers could introduce bias. However, different surgeons have varying preferences for laser settings, 14 making it more realistic to compare laser performance based on surgeon preferences. Besides, as TFL and Ho:YAG lasers are two different technologies, using the same setting may restrain TFL from performing at its best, therefore putting TFL at a disadvantage. 6 Third, our study is single-blinded, meaning only the patients were blinded to the treatment they received. A multicenter, double-blind, randomized controlled trial is necessary to determine which laser is more effective for treating ureteral stones in a clinical setting. Last, the group’s unexpected smaller difference in stone ablation speed led to an inaccurate sample size estimation. With the current data, the power of the study is calculated to be only 9.5%. This low number of participants may not have enough power to find subtle differences, which includes secondary outcomes like the total operative time or complication rates. Nonetheless, our study provided a basis for future studies on the difference in stone ablation speed.
Conclusion
Lithotripsy using a TFL achieves a stone ablation speed comparable to that of the Ho:YAG laser. However, the TFL results in a higher stone-free rate while keeping complication rates similar. This evidence indicates that TFL lithotripsy could provide a more effective option for managing urinary stones without increasing the risk of adverse outcomes.
Authors’ Contributions
J.L.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing—original draft. I.K.: Visualization, writing—review & editing. S.C.: Investigation. F.W.: Investigation. S.Y.: Investigation. W.C.: Investigation. C.N.: Conceptualization, methodology, project administration, supervision, writing—review & editing.
Footnotes
Funding Information
This study was supported by Olympus Corporation of Asia Pacific Ltd., which provided equipment for the trial. Olympus had no involvement in the study’s design, data collection, analysis, or article preparation. All opinions expressed in this work are solely those of the authors.
Author Disclosure Statement
No competing financial interests exist.