
Abstract
Objectives:
To compare the efficacy of traditional double-layer suturing techniques vs an improved “cross-stitch” suturing technique (CST) in robot-assisted partial nephrectomy (RAPN) for localized renal cell carcinoma.
Patients and Methods:
We retrospectively analyzed clinical data from patients who underwent RAPN at our center between August 2022 and January 2025. A total of 89 patients were ultimately included, including 58 in the double-layer suture group and 31 in the “cross-stitch” suturing technique group. To minimize selection bias, 1:1 propensity score matching (PSM) was performed to balance baseline characteristics between groups (matched covariates: age, body mass index, RENAL score, tumor size, tumor location, and growth pattern). In the matched cohort, a double robust estimation strategy was applied. Multivariate regression models were used to adjust for residual confounders, enabling comparison of perioperative indicators, early renal function changes, and postoperative complications between the two groups.
Results:
After PSM, 52 patients (26 in each group) were analyzed, and the clinical baseline characteristics of both patient groups achieved favorable matching, with significantly reduced differences in the distribution of covariates such as age, BMI, tumor size, radius, exophytic/endophytic, nearness to collecting system, anterior/posterior, location score, tumor location, and growth pattern (standardized mean difference <0.1). Compared with the double-layer suturing group, the “cross-stitch” suturing technique group had a significantly shorter operative time (111.1 vs 133.4 minutes, p = 0.002) and warm ischemia time (WIT) (15.4 vs 20.5 minutes, p < 0.001). However, no statistically significant differences were observed between groups in estimated blood loss (p = 0.362), postoperative hospital stay (p = 0.349), positive margin rate (p = 0.932), postoperative complications (p = 0.315), or trifecta achievement rate (p = 0.07).
Conclusion:
The modified CST was associated with shorter WIT and operative time and may be particularly suitable for localized renal tumors of moderate complexity. However, no significant differences were observed in postoperative renal function or trifecta after matching, and these findings should be interpreted with caution and require further validation.
Keywords
Introduction
With the advancement of imaging technologies and increased public health awareness, the detection rate of localized renal cell carcinoma has steadily increased. 1 Nephron-sparing surgical procedure, particularly robot-assisted partial nephrectomy (RAPN), is now the standard treatment for such tumors.2,3 The primary goal of RAPN is to achieve complete tumor resection while maximizing renal function preservation and minimizing complications. 4
During RAPN, the suturing and reconstruction of the renal collecting system and parenchyma are critical steps, directly impacting the risk of postoperative complications such as bleeding and urinary leakage. 5 Furthermore, suturing efficiency is closely associated with warm ischemia time (WIT), and prolonged WIT is a well-established risk factor for postoperative renal dysfunction.6,7 Therefore, minimizing WIT remains a key objective in RAPN to optimize renal functional outcomes.8,9
The traditional double-layer suturing technique (DST), a widely adopted mature method, sequentially closes the collecting system/deep vascular structures and the superficial renal parenchyma, offering good safety and reliability. However, it requires two suturing layers, which may increase operative time and WIT. 10 Moreover, the deep suturing step in double-layer techniques has been associated with an increased risk of renal artery pseudoaneurysm. 11 In contrast, single-layer suturing simplifies the procedure and reduces WIT but may be less reliable for closure of deep collecting systems and vessels, raising concerns about increased risks of postoperative bleeding and urinary leakage.12,13
Sutureless techniques, such as lipocortical reconstruction, fibrin sealants, or coverage with hemostatic materials (e.g., oxidized regenerated cellulose), have demonstrated promising outcomes in selected cases, particularly for superficial, exophytic small tumors.4,14,15 However, their reliability in managing deeper tumors or those adjacent to collecting systems remains controversial, limiting their widespread adoption. 16
In this context, we propose a modified “cross-stitch” suturing technique (CST) to address the practical trade-off between operative efficiency and closure reliability during renorrhaphy. Traditional double-layer suturing is reliable but requires two layers of reconstruction, which may prolong WIT. In contrast, standard single-layer suturing is simpler and faster but may provide less secure closure of the deep collecting system and vascular structures. The “cross-stitch” configuration was therefore designed to improve the efficiency of renorrhaphy while maintaining effective closure of both deep and superficial components of the defect.
This retrospective study compares the clinical outcomes of the modified “cross-stitch” technique with traditional double-layer suturing in RAPN for localized renal cell carcinoma. We focused on operative time, WIT, postoperative renal function, and perioperative outcomes to provide evidence to guide surgical decision-making.
Materials and Methods
This retrospective study included clinical data and surgical videos from 125 patients who underwent RAPN at our center between August 2022 and January 2025. The exclusion criteria were as follows: (1) Bilateral or ipsilateral multifocal renal tumors (4); (2) Conversion to radical nephrectomy during the surgical procedure (4); (3) Use of non-blocking sutures or single-layer suturing (23); and (4) Missing clinical data or surgical video (5). A total of 89 patients were ultimately included in the analysis (Fig. 1).
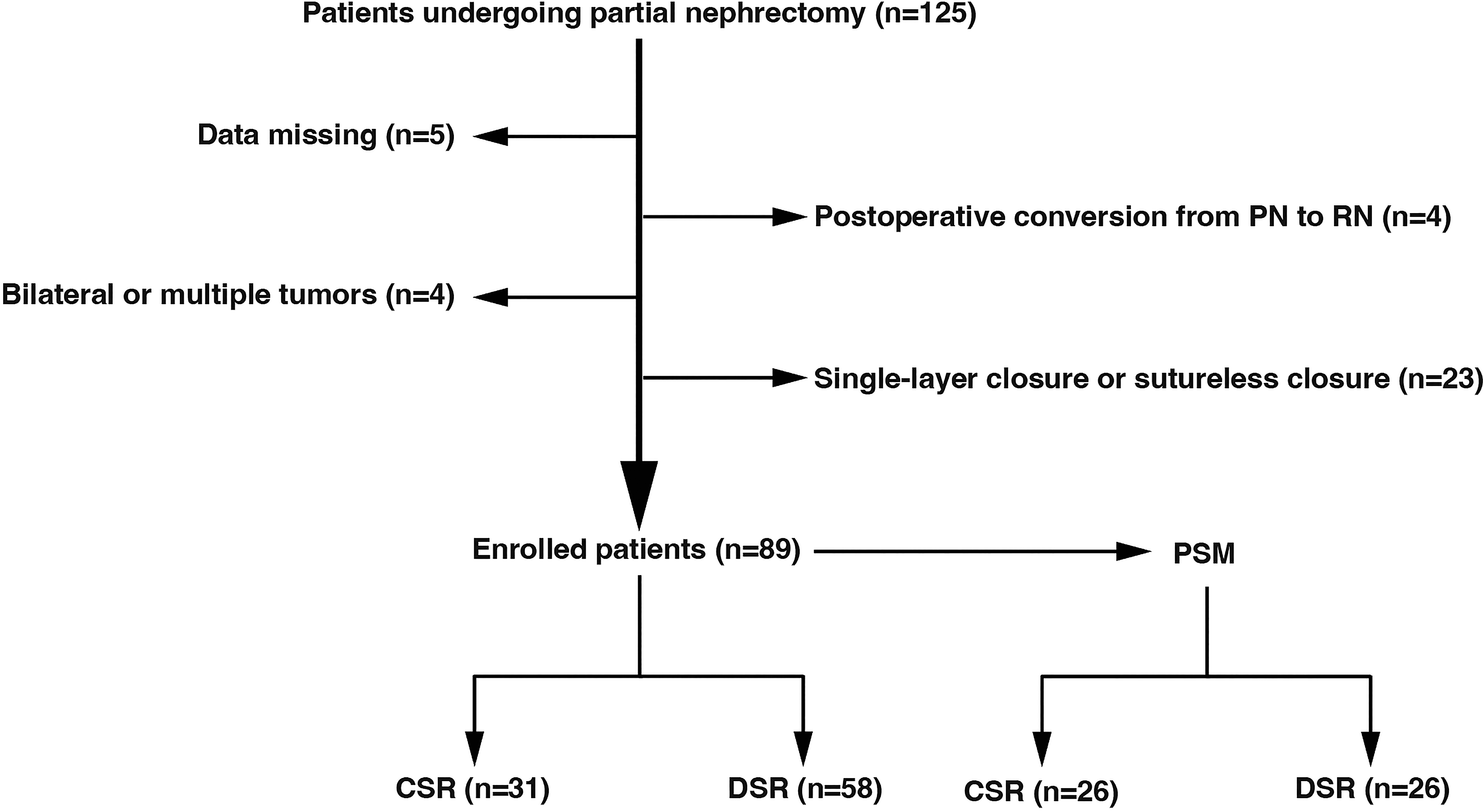
Study flow diagram showing patient enrollment, exclusions, and final grouping.
Clinical variables collected included age, gender, body mass index (BMI), and comorbidities such as hypertension and diabetes, as well as tumor size. Tumor parameters were assessed using the radius, exophytic/endophytic, nearness to collecting system, anterior/posterior, location (R.E.N.A.L.) score based on preoperative computed tomograpy (CT) or magnetic resonance imaging (MRI). 17
Perioperative variables included operative time, WIT, estimated blood loss, and length of hospital stay. Renal function was assessed using estimated glomerular filtration rate (eGFR) measured preoperatively and postoperatively. 18 The Trifecta was defined as a negative surgical margin, zero perioperative complications, and warm ischemia ≤25 minutes. 19
This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University in accordance with the principles of the Declaration of Helsinki (revised in 2013). Informed consent was not required as this study was retrospective in nature.
Preoperative preparation
Imaging preparation
All patients underwent standardized preoperative evaluation and preparation. Contrast-enhanced CT or MRI was performed to assess tumor anatomy and calculate the R.E.N.A.L. nephrometry score (Fig. 2A). For deep-seated or complex tumors located near the renal hilum, three-dimensional reconstruction or 3D-printed models were used to facilitate surgical planning (Fig. 2B). In addition, preoperative renal dynamic imaging was performed to evaluate split renal function and ensure adequate compensatory function of the contralateral kidney. Prior to the surgical procedure, a multidisciplinary team conducted case discussions to preliminarily determine the surgical approach and suturing strategy based on tumor-specific characteristics (e.g., size, location, relationship with the collecting system). All procedures were performed by a single surgeon with experience of over 500 RAPN cases. The CST was introduced in 2021 and used in parallel with double-layer suturing during the study period, without a systematic difference in case sequence.
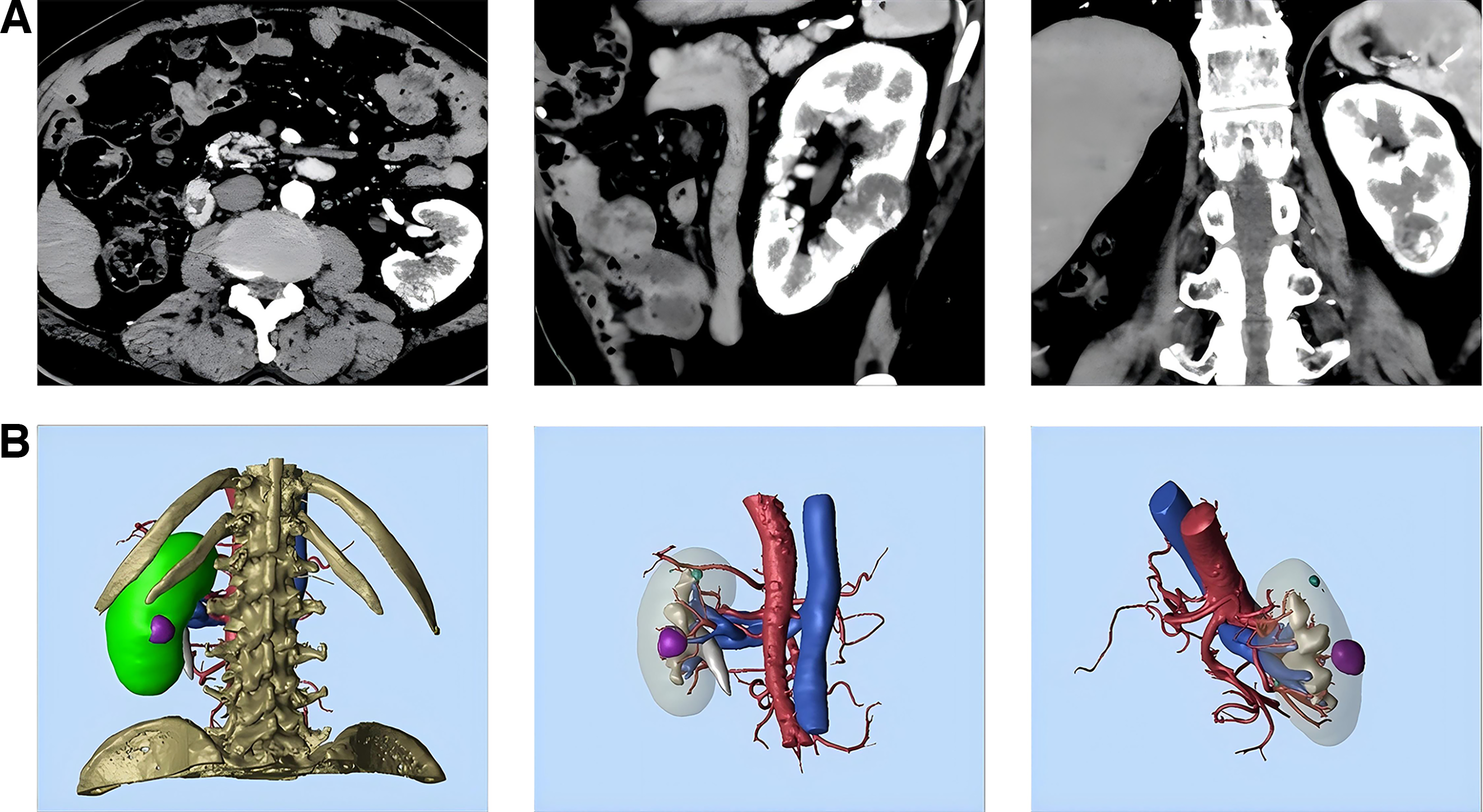
Preoperative imaging.
Operative preparation
All procedures were performed using the da Vinci robotic surgical system. A nasogastric tube and a urinary catheter were placed prior to the surgical procedure. After induction of general anesthesia, patients were positioned in a contralateral lateral decubitus position at approximately 60°.
Following routine disinfection and draping, pneumoperitoneum was established. Three robotic ports and two to three assistant ports were placed in the abdominal wall. The robotic ports consisted of one 12-mm camera port (with a 30° downward-viewing lens) and two 8-mm working ports, while the assistant ports included two 12-mm trocars. For right-sided tumors, an additional 5-mm assistant trocar was placed in the subxiphoid region.
Surgical techniques
Traditional double-layer suturing
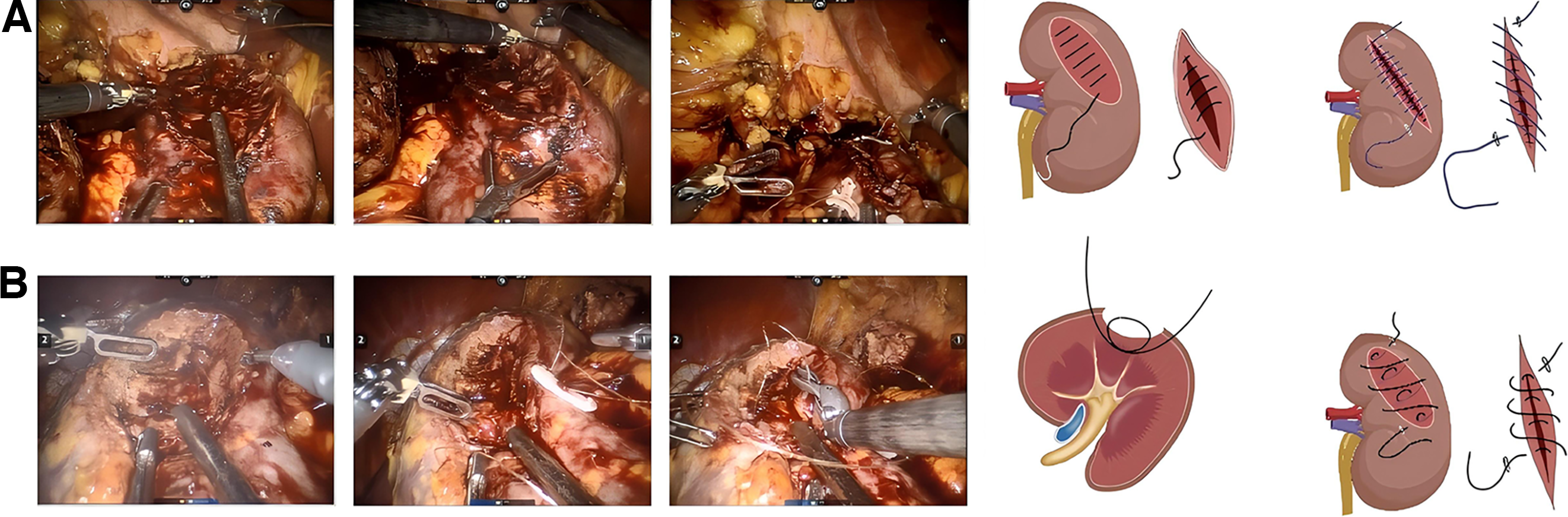
A continuous inner layer suture was first performed using 3-0 barbed sutures to repair deep vascular and collecting systems within the renal parenchyma. Subsequently, an outer layer suture was performed using 0 barbed sutures to close the renal capsule and superficial renal parenchyma with a continuous running technique, providing final contouring and reinforcement of the renal wound. All sutures were secured with Hem-o-Lok clips (Fig. 3A). The arterial clamp was then released after the completion of the entire suturing process.
Preoperative imaging.
Modified “cross-stitch” suturing technique
A single-layer closure was performed using 0 barbed sutures. The needle was inserted from the outer edge of the resection bed capsule, passed through the base of the incision, and exited after crossing 2/3 to 3/4 of the transverse diameter of the resection bed. Subsequently, a second back-and-forth suture was performed. The needle was inserted on the same side as the first entry point, near the midline of the incision. It again traversed 2/3 to 3/4 of the transverse diameter of the incision and exited at the outer edge of the capsule on the opposite side of the incision. This unique needle pathway formed a precise “cross-stitch” structure within the renal parenchymal incision. This “cross-stitch” simultaneously applied tension to both the deep collecting system/vascular structures and the superficial renal parenchyma within the incision. Consequently, a single-layer suture could achieve a closure effect comparable to that of traditional DSTs (Fig. 3B). The incision was closed using this continuous suturing technique and secured with Hem-o-Lok clips. Similar to the traditional group, arterial unclamping was performed only after the full completion of the renorrhaphy.
Statistical analysis
All statistical analyses were performed using R and SPSS software. Continuous variables with a normal distribution were expressed as mean ± standard deviation and compared between groups using the independent-samples t tests. Continuous variables that were not normally distributed (e.g., operative time, maximum tumor diameter) were expressed as median (interquartile range, IQR) and compared using the Mann–Whitney U test. Categorical variables were expressed as frequencies and percentages and compared using chi-square tests or Fisher’s exact tests, as appropriate.
To reduce baseline differences between groups, PSM was performed using 1:1 nearest-neighbor matching with a caliper of 0.2. The matching covariates included age, BMI, RENAL score, tumor size, tumor location, and growth pattern. Given minor residual imbalance in some matched covariates after matching (e.g., tumor growth pattern, standardized mean difference [SMD] > 0.1) and the low incidence of certain binary outcomes, a double robust estimation strategy was further applied. Specifically, multivariate linear regression models were used for continuous outcome measures. For sparse binary outcomes, Firth’s penalized logistic regression was applied, and Fisher’s exact test results were primarily referenced when appropriate to account for residual confounding and improve robustness. A two-sided p < 0.05 was considered statistically significant.
Results
Patient baseline characteristics
A total of 89 patients were included in this study, including 58 in the double-layer suture group (DST) and 31 in the “cross-stitch” suturing technique group. Table 1 summarizes the baseline demographic and tumor characteristics of the two groups before and after PSM. Although no statistically significant differences were observed in baseline variables before PSM, SMDs indicated some imbalance in variables relevant to surgical outcomes, particularly tumor size and tumor growth pattern (SMD > 0.1). After PSM, the SMDs of most key variables were reduced to < 0.1, indicating improved comparability between groups. For variables with residual imbalance after matching (e.g., tumor growth pattern), a double robust estimation strategy was further applied to reduce residual confounding.
Comparison of Demographic Characteristics Between Double—Layer Suturing and “Cross-Stitch” Suturing Technique
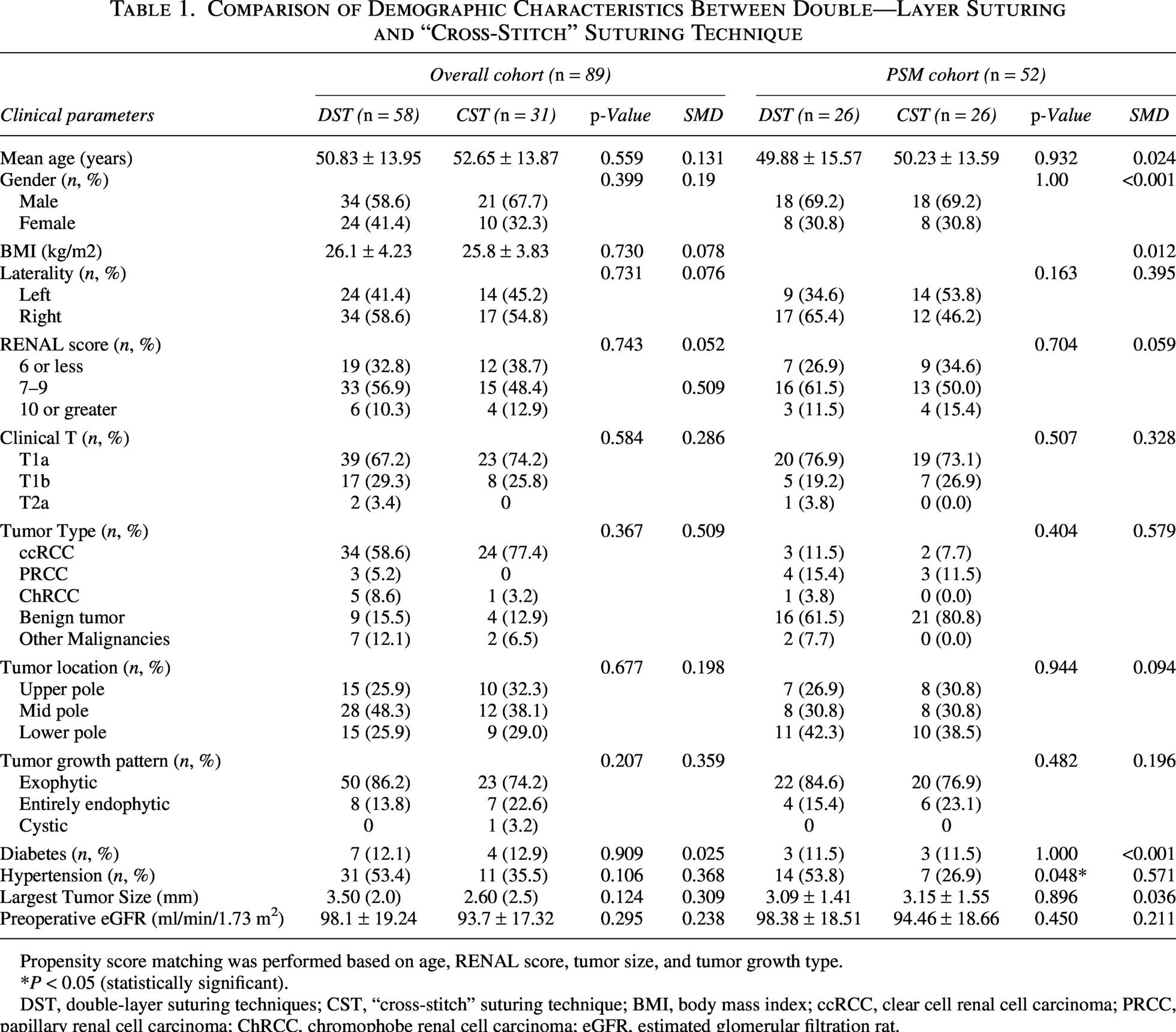
Propensity score matching was performed based on age, RENAL score, tumor size, and tumor growth type.
P < 0.05 (statistically significant).
DST, double-layer suturing techniques; CST, “cross-stitch” suturing technique; BMI, body mass index; ccRCC, clear cell renal cell carcinoma; PRCC, papillary renal cell carcinoma; ChRCC, chromophobe renal cell carcinoma; eGFR, estimated glomerular filtration rat.
Perioperative and postoperative outcomes
Table 2 summarizes the perioperative and postoperative outcomes in the unmatched and matched cohorts. In the unmatched cohort, the CST group had a significantly shorter mean WIT (15.2 ± 4.0 minutes vs 21.4 ± 5.2 minutes, p < 0.001) and operative time (109.0 minutes vs 134.0 minutes, p < 0.001) than the DST group. In addition, the decline in eGFR within 24 hours after surgical procedure was significantly smaller in the CST group than in the DST group (–9.45 ± 12.5 vs –14.62 ± 11.0 mL/min/1.73 m2, p = 0.049). No statistically significant differences were observed between groups in estimated blood loss, length of postoperative hospital stay, positive surgical margin rate (DST: 3.4% vs CST: 0%, p = 0.296), or overall complication rate (p = 0.602). According to the trifecta criterion, 20 the trifecta achievement rate was significantly higher in the CST group than in the DST group (83.8% vs 60.3%, p = 0.023).
Comparison of Perioperative Outcomes and Follow-up Characteristics Between Double—Layer Suturing and “Cross-Stitch” Suturing Technique
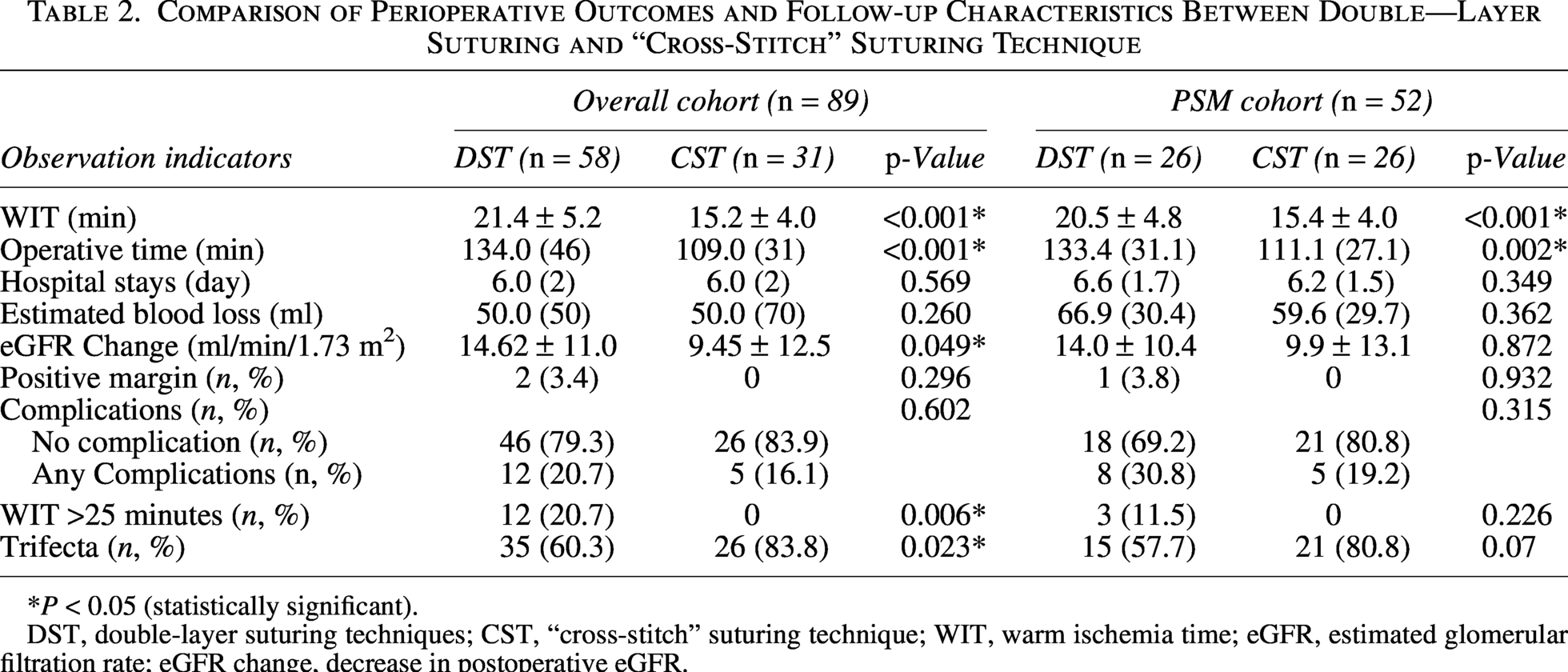
P < 0.05 (statistically significant).
DST, double-layer suturing techniques; CST, “cross-stitch” suturing technique; WIT, warm ischemia time; eGFR, estimated glomerular filtration rate; eGFR change, decrease in postoperative eGFR.
In the matched cohort (26 patients per group), the CST group still had a significantly shorter WIT (15.4 ± 4.0 minutes vs 20.5 ± 4.8 minutes, p < 0.001) and operative time (111.1 minutes vs 133.4 minutes, p = 0.002) than the DST group. However, postoperative changes in eGFR were no longer significantly different between groups (p = 0.872). The remaining outcomes, including estimated blood loss, postoperative hospital stay, positive margin rate (DST: 3.8% vs CST: 0%, p = 0.932), overall complication rate (p = 0.315), and trifecta achievement rate (80.8% vs 57.7%, p = 0.070), also showed no statistically significant differences. With regard to complications, the most common event was postoperative hematuria (Clavien grade I), which occurred in 11 patients in the DST group and 5 patients in the CST group; all cases resolved spontaneously without specific intervention. One patient in the DST group required blood transfusion because of postoperative bleeding (Clavien grade II). No Clavien grade III or higher complications were observed. At the end of follow-up, no tumor recurrence or metastasis was observed in either group.
Discussion
Ideal renal reconstruction following partial nephrectomy aims to minimize WIT while preserving functional renal parenchyma and ensuring complete hemostasis and secure closure of the collecting system. 21 In this study, PSM analysis showed that, compared with traditional double-layer suturing, the modified CST was associated with significantly shorter WIT (15.4 ± 4.0 vs 20.5 ± 4.8, p < 0.001) and operative time (111.1 [27.1] vs 133.4 [31.1], p = 0.002).
Whether reducing suture layers increases the risk of postoperative bleeding or urinary leakage is an important concern. In the present study, no statistically significant differences were observed between groups in intraoperative blood loss (p = 0.362), postoperative hospital stay (p = 0.349), or overall complication rates (p = 0.315), and negative surgical margins were achieved in both groups. These findings suggest that the CST, while improving operative efficiency, does not appear to compromise fundamental requirements of suturing, including reliable hemostasis, complete closure of the collecting system, and integrity of tumor resection. However, given the relatively limited sample size of this study, the robustness of inferences regarding safety outcomes, including complications, positive surgical margins, and trifecta achievement, remains limited. Accordingly, the absence of significant differences in these endpoints should be interpreted with caution, and these findings require further validation in larger prospective studies.
For patients with normal contralateral renal function, a WIT <25 minutes is generally considered safe. However, in patients with compromised renal reserve, such as those with a solitary kidney or chronic kidney disease, minimizing ischemia time remains clinically important. 6 In this context, the approximately 5-minute reduction (about 25%) in WIT observed with the “cross-stitch” suturing technique group may be of potential relevance. Nevertheless, no significant difference in postoperative renal function was observed after matching, and no ipsilateral renal volumetric assessment was performed because appropriate imaging data for quantitative analysis were unavailable. Renal function in this study was primarily evaluated using eGFR, which may not fully reflect changes in preserved renal parenchymal volume. Therefore, these findings should be interpreted with caution, although the reduction in ischemia time may still be clinically relevant in patients with limited renal reserve. We also report a solitary kidney case with short ischemia time and favorable postoperative recovery, which, although not generalizable, may provide preliminary insight into the potential applicability of this technique in selected patients. Future studies incorporating CT-based volumetric assessment or 3D reconstruction may help to further clarify the relationship between ischemia time reduction and renal parenchymal preservation.
For elderly patients and those with severe comorbidities (such as cardiovascular disease), surgical risks are often influenced by the duration of anesthesia and overall operative time. Prolonged anesthetic exposure has been associated with an increased risk of postoperative complications, including postoperative delirium and hemodynamic instability.22,23 Furthermore, extended operative duration exhibits a linear correlation with the incidence of infectious and thromboembolic complications. 24 Consequently, minimizing operative duration may be particularly important for such patients. In this context, the reduction in operative time observed with the CST may be clinically relevant. However, as the present study did not specifically evaluate these systemic outcomes, any potential benefit in reducing such risks remains speculative.
To address potential selection bias inherent in retrospective studies, we used a PSM design to improve comparability between groups. Key confounding factors, including age, RENAL score, tumor size, and growth pattern, were included in the matching process. Given the possibility of residual imbalances in small-sample analyses (e.g., post-matching hypertension distribution difference p = 0.038, with some variables showing SMD > 0.1), we further implemented a double-robust estimation strategy. Specifically, in outcome analysis, we constructed a multivariable regression model (using Firth penalty regression for sparse data) incorporating all imbalanced baseline variables for adjustment. These methods were intended to reduce confounding and strengthen the robustness of the findings; however, residual bias cannot be completely excluded.
All procedures were performed by a highly experienced surgeon, and the learning curve associated with the CST was not formally evaluated. Therefore, the reproducibility of this technique among surgeons with varying levels of experience requires further investigation.
This study has several limitations. First, as a single-center retrospective study, the sample size was relatively limited, and residual selection bias cannot be entirely excluded despite the use of PSM. Second, the study primarily focused on perioperative indicators and lacked follow-up data on long-term renal function, precluding assessment of long-term functional benefits. No ipsilateral renal volumetric assessment was available, which limited direct quantification of preserved renal parenchyma. In addition, the evaluation of the modified “cross-stitch” suturing technique group was primarily concentrated on cases with small-to-medium tumor volumes and moderate complexity. The applicability of this technique to more complex tumors warrants further investigation.
Conclusion
In summary, the modified CST was associated with improved operative efficiency, with shorter WIT and operative duration, without an observed increase in perioperative complications. The technique may be particularly suitable for localized renal tumors of small-to-medium size and moderate complexity. However, given the retrospective design, limited sample size, and lack of volumetric assessment, these findings should be interpreted with caution and require further validation in prospective studies.
Authors’ Contributions
Y.L.: Data collection and article writing; A.G.: Data collection and article writing; Y.D.: Data collection and draft revision; J.W.: Data collection and draft revision; X.N.: Project development and draft revision; Z.J.: Project development and draft revision.
Footnotes
Human Ethics and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University.
Consent to Participate
Informed consent was waived by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University because of the retrospective nature of the study and the use of de-identified clinical data.
Author Disclosure Statement
The authors have no relevant financial or non-financial interests to disclose.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant No. 82302964) and the Henan Medical Researcher Overseas Training Program (Grant No. HNMOT2025066), both awarded to Xianghui Ning.