
Abstract
Purpose:
This study aimed to directly compare the Imamura, De Nunzio, and Zhang nomograms for predicting stone-free outcomes following ureterolithotripsy (ULT) with semi-rigid ureteroscopy for distal ureteral stones.
Methods:
A retrospective analysis was conducted on 397 consecutive patients who underwent ULT using semi-rigid ureteroscopy for distal ureteral stones between 2017 and 2024. Stone-free status was defined as the complete absence of residual fragments on postoperative non-contrast computed tomography. The predictive performance of each nomogram was evaluated using receiver operating characteristic curves, with internal validation performed using 1000 bootstrap resamples. Calibration was assessed using calibration-in-the-large, calibration slope, and Brier scores. The clinical utility was examined using decision curve analysis (DCA). Independent predictors of stone-free status were identified using multivariable logistic regression analysis.
Results:
The overall stone-free rate was 90.7%. The independent predictors of non-stone-free status included a stone diameter of ≥10 mm, multiple stones, pyuria, and stone impaction. The Imamura nomogram exhibited the highest discriminative ability (area under the curve [AUC]: 0.853), followed by the De Nunzio (AUC: 0.759) and Zhang (AUC: 0.689) nomograms. The bootstrap AUCs were nearly identical to the apparent AUCs. Additionally, the Imamura nomogram demonstrated the most favorable calibration profiles. DCA indicated that the Imamura nomogram provided the greatest net clinical benefit.
Conclusion:
Among the evaluated nomograms, the Imamura model exhibited superior discrimination, calibration, and clinical utility in predicting stone-free outcomes following ULT with semi-rigid ureteroscopy for distal ureteral stones. Integrating this tool into preoperative assessments may enhance risk stratification and improve individualized patient counseling. Prospective multicenter validation is warranted.
Introduction
Ureterolithiasis is a prevalent urological condition, with distal ureteral stones representing a significant proportion of cases necessitating surgical intervention. Ureterolithotripsy (ULT) with semi-rigid ureteroscopy (URS) continues to be the primary treatment modality for these stones, offering high stone-free rates (SFR) with acceptable morbidity.1,2 However, operative outcomes vary considerably based on patient- and stone-related characteristics, including stone size, impaction, anatomical factors, and preoperative inflammatory status. 3 Consequently, predicting the likelihood of achieving a stone-free outcome prior to a surgical procedure has become increasingly important for optimizing patient counseling, resource allocation, and individualized treatment planning.
In response to this requirement, several predictive nomograms have been developed using preoperative clinical and radiological variables. Notably, the Imamura, De Nunzio, and Zhang nomograms are the most frequently referenced and extensively employed tools for estimating the likelihood of postoperative stone clearance.4–6 Each model incorporates a unique set of predictors that reflect variations in patient populations and methodological approaches.
Despite the increasing interest in predictive modeling, the external applicability and comparative performance of these nomograms remain uncertain, particularly in homogeneous cohorts undergoing ULT with semi-rigid URS for distal ureteral stones. Previous studies have predominantly evaluated each nomogram in isolation, thereby limiting clinicians’ ability to determine which tool performs optimally in practical settings. 7 Furthermore, the generalizability of these models may be affected by variations in regional practice patterns, stone epidemiology, and institutional experiences.
These factors highlight the need for a direct head-to-head comparison of established nomograms in a well-defined clinical scenario. Evaluating these models in the same patient cohort offers the opportunity to compare their discriminative abilities and assess their clinical usefulness for preoperative decision-making. Given the increasing emphasis on individualized care, identifying the most reliable and practical predictive tool may help clinicians select appropriate treatment strategies, anticipate procedural challenges, and improve patient counseling.
This study aimed to evaluate the performance of the Imamura, De Nunzio, and Zhang nomograms in predicting stone-free outcomes following ULT with semi-rigid URS for distal ureteral stones. Using a large, contemporary patient cohort, we assessed the discriminative ability of each model and examined its potential role in guiding preoperative risk stratification.
Materials and Methods
This retrospective study included 397 consecutive patients who underwent ULT with semi-rigid URS for distal ureteral stones between January 2017 and January 2024 at our institution. A total of 198 patients were excluded because of incomplete follow-up imaging or missing data. The study adhered to the ethical guidelines delineated in the World Medical Association Helsinki Declaration’s “Ethical Principles for Medical Research Involving Human Subjects.” Ethical approval was secured from the Ethics Committee of Basaksehir Cam and Sakura City Hospital (approval number: 05.03.2025.84). Assuming an alpha level of 0.05 and statistical power of 80%, the minimum required sample size was determined to be 299 patients.
The exclusion criteria were age <18 years and incomplete preoperative data or insufficient radiological follow-up. A thorough preoperative evaluation was conducted for all patients, including urinalysis, urine culture, complete blood count, and serum creatinine measurements. Patients diagnosed with urinary tract infections received appropriate antibiotic treatment, and sterile urine cultures were obtained before surgical intervention.
Preoperative demographic and clinical data, including age, gender, body mass index (BMI), and comorbidities, were documented. Stone characteristics, such as size, location, and presence of hydronephrosis, were assessed using non-contrast computed tomography (NCCT). The maximum stone length and maximum transverse diameter were recorded. All radiological measurements were performed by an experienced radiologist (M.S.Ö.). Pyuria was defined as the presence of ≥5 white blood cells (WBC) per high-power field on urinalysis. Stone impaction was noted when there was an intraoperative inability to pass the guidewire beyond the stone.
All procedures were performed by seven experienced endourologists, each with more than 5 years of experience in uULT and performing high annual case volumes (>100 cases/year). All procedures were conducted under general or spinal anesthesia using a 6/7.5F semi-rigid URS (Richard Wolf, Knittlingen, Germany). Following the initial placement of a guidewire (Boston Scientific, Marlborough, Massachusetts, USA), lithotripsy was performed using a Holmium:YAG laser (Sphinx, Katlenburg-Lindau, Germany) in all patients. Flexible URS was not routinely utilized in this cohort, as only distal ureteral stones treated with semi-rigid URS were included to ensure procedural standardization. The decision to place a postoperative Double-J stent was made at the discretion of the operating surgeons. Stone-free status was assessed at 1 month postoperatively using NCCT to ensure consistent follow-up and minimize missing data inherent to retrospective analyses. Complete clearance on imaging was defined as stone-free status, whereas patients with residual fragments were managed according to clinical indications.
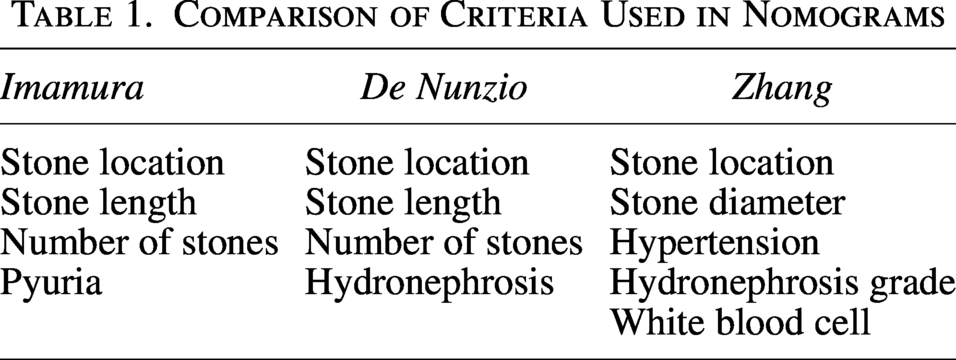
The nomogram scores were calculated as outlined in the original publications without any alterations. The criteria employed for scoring each nomogram are detailed in (Table 1). Nomogram scores were calculated retrospectively and were not available to the operating surgeons; therefore, surgeons were blinded to nomogram predictions. Each nomogram score was categorized according to the predefined SFR thresholds of 70%, 80%, and 90%. Subsequently, the predictive performances of the nomograms were compared.
Comparison of Criteria Used in Nomograms
Statistical analyses were conducted using the Statistical Package for the Social Sciences version 27 (SPSS IBM Corp.; Armonk, NY, USA) and Python version 3.12, incorporating scikit-learn and matplotlib libraries. Categorical variables were assessed using the chi-square test, whereas continuous variables were evaluated using either the independent sample t-test or the Mann–Whitney U test, depending on the data distribution. Variables deemed significant in the univariate analysis were further investigated using multivariate logistic regression. Receiver operating characteristic (ROC) curves were used to evaluate the discriminative performance of each nomogram in predicting stone-free status after ULT.
Bootstrap resampling (n = 1000) was employed to internally validate the model’s performance and mitigate optimism bias. In each iteration, random samples were drawn with replacement from the original dataset, and the area under the curve (AUC) values were recalculated. The calibration performance was evaluated using calibration plots, calibration-in-the-large (CITL), and calibration slope. The Brier score was computed to measure the overall predictive accuracy. The clinical utility was assessed using decision curve analysis (DCA) across threshold probabilities ranging from 0.10 to 0.50. Net benefit curves were compared with “treat-all” and “treat-none” strategies to ascertain whether each nomogram provided an incremental value in clinical decision-making. Statistical significance was set at p < 0.05, and all analyses were conducted with 95% confidence intervals.
Results
We analyzed a cohort of 397 patients who underwent semi-rigid URS for the treatment of distal ureteral stones. The overall SFR was 90.7%. The baseline characteristics stratified by stone-free status are shown in Table 2 (Table 2). No statistically significant differences were identified in terms of age (p = 0.566), gender (p = 0.273), BMI (p = 0.172), stone laterality (p = 0.865), or Hounsfield Unit (p = 0.179). Notably, hypertension (HT) was significantly more prevalent in the group that did not achieve stone-free status (37.8% vs 22.8%, p = 0.037).
Comparison of the Characteristics of the Patients Who Were Stone Free and Not Stone Free After Ureterolithotripsy
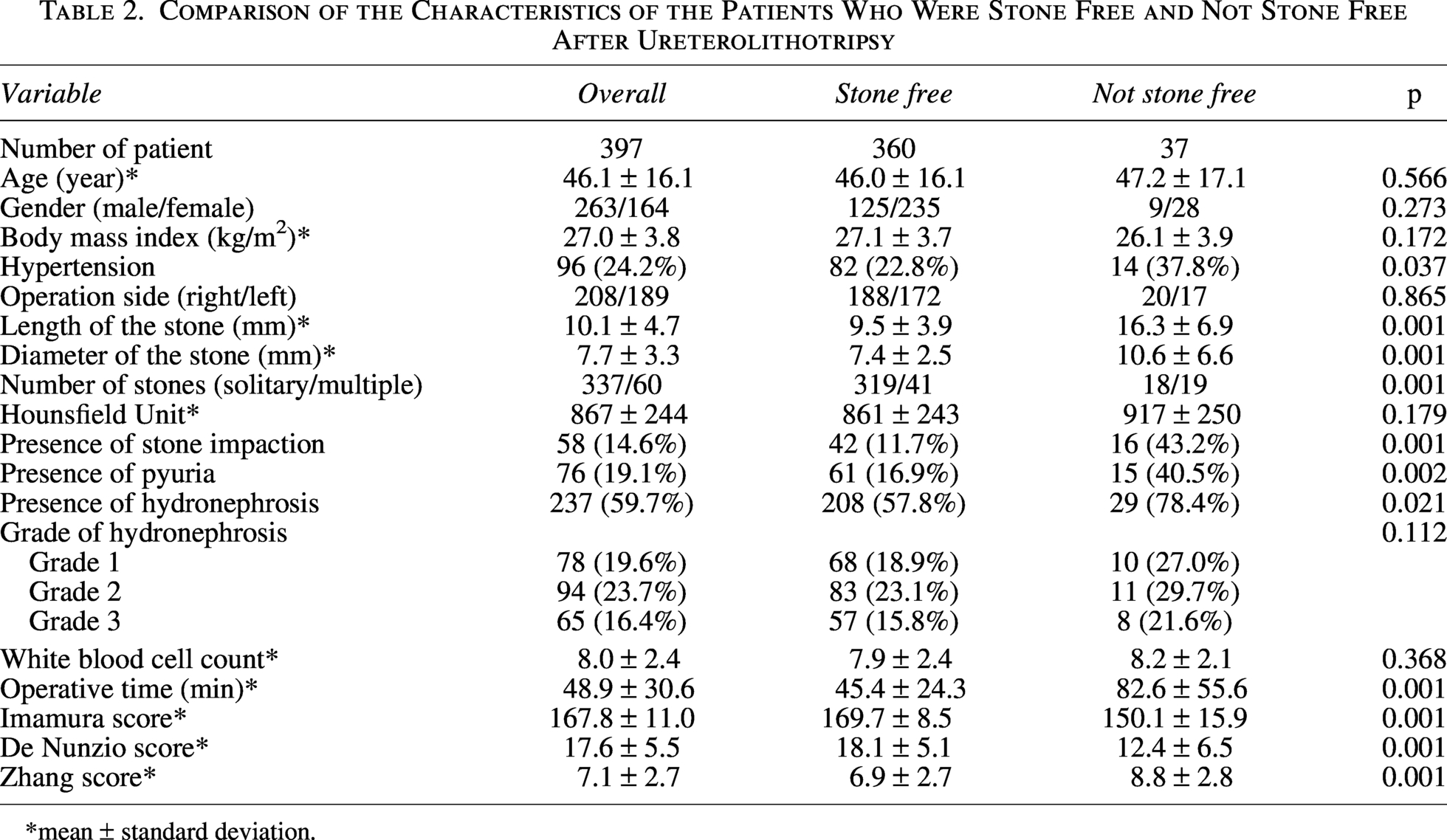
*mean ± standard deviation.
Among patients who were not stone-free (n = 37), the stones were significantly larger in both maximum length (16.3 vs 9.5 mm, p < 0.001) and diameter (10.6 vs 7.4 mm, p < 0.001). Additionally, there was a higher incidence of multiple stones (51.4% vs 11.4%, p < 0.001), more frequent stone impaction (43.2% vs 11.7%, p < 0.001), a greater prevalence of pyuria (40.5% vs 16.9%, p = 0.002), and an increased occurrence of hydronephrosis (78.4% vs 57.8%, p = 0.021). The operative time was notably longer in the non-stone-free group (82.6 minutes vs 45.4 minutes, p < 0.001). No significant differences were observed in hydronephrosis grade (p = 0.112) or WBC count (p = 0.368).
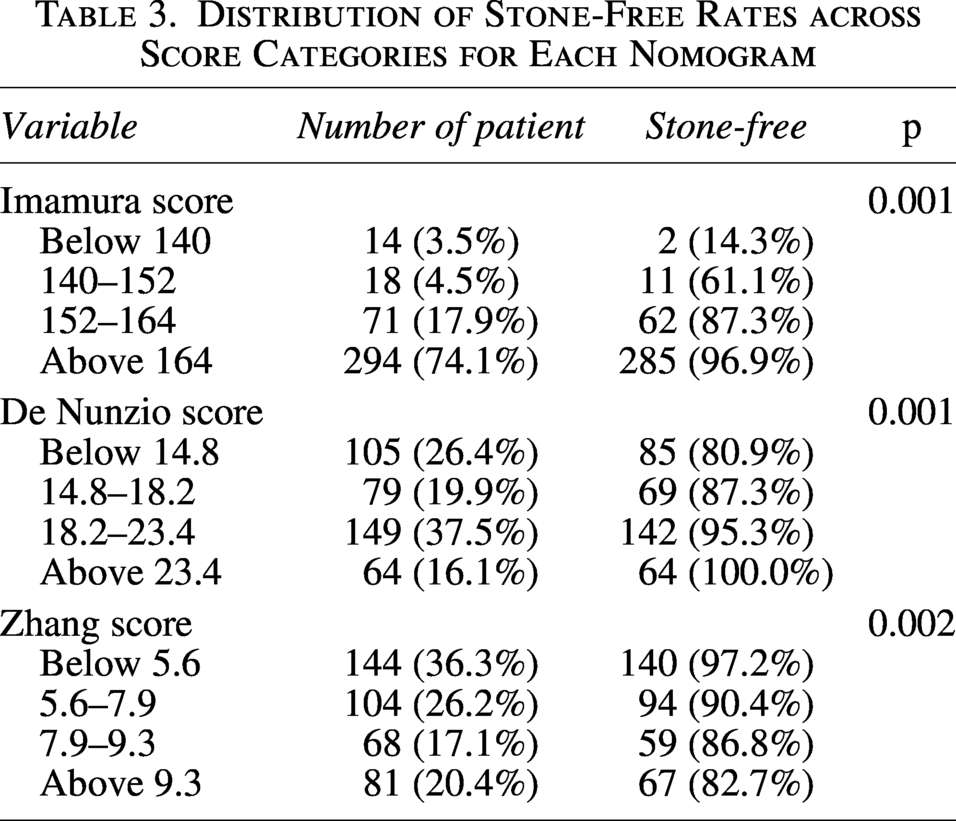
The mean scores of the Imamura, De Nunzio, and Zhang nomograms were significantly different between the stone-free and non-stone-free groups (all p < 0.001). When stratified into score-based categories, all three nomograms effectively demonstrated a statistically significant stratification of SFRs (Table 3).
Distribution of Stone-Free Rates across Score Categories for Each Nomogram
In the multivariate analysis detailed in Table 4, several factors emerged as independent predictors of achieving stone-free status (Table 4). The factors included a stone diameter of ≥10 mm (OR: 2.70, 95% CI: 1.12–6.53; p = 0.027), presence of multiple stones (odds ratio [OR]: 8.25, 95% confidence interval [CI]: 3.21–21.20; p < 0.001), presence of pyuria (OR: 2.87, 95% CI: 1.15–7.15; p = 0.024), and presence of stone impaction (OR: 5.23, 95% CI: 2.04–13.44; p < 0.001).
Multivariate Analysis for Stone-Free Rate
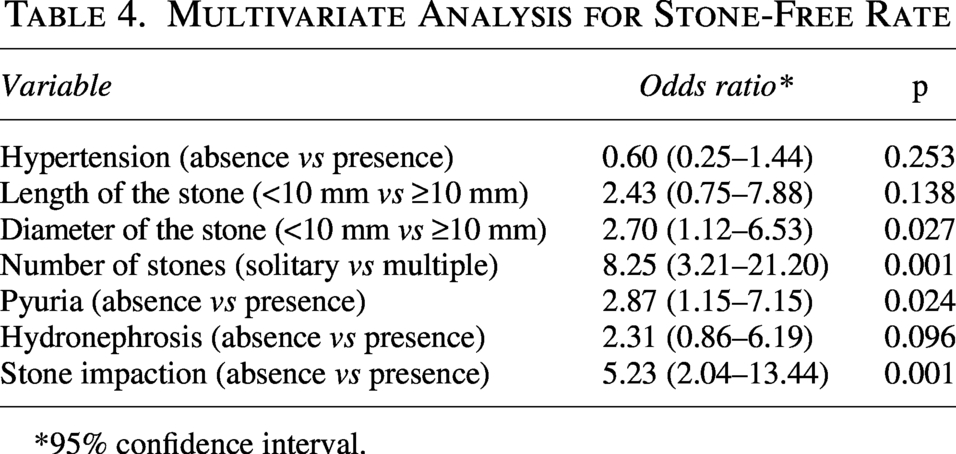
*95% confidence interval.
A ROC curve analysis was employed to evaluate the predictive efficacy of each nomogram. The Imamura nomogram demonstrated the highest discriminative capability, with an AUC of 0.853, followed by the De Nunzio (AUC: 0.759) and Zhang (AUC: 0.689) models. The ROC curves are shown in Figure 1 (Fig. 1). Bootstrap-corrected mean ROC curves, accompanied by 95% confidence bands, are shown in Figure 2 (Fig. 2). The bootstrap AUC values closely approximated the apparent AUCs, suggesting minimal optimism and no overfitting.
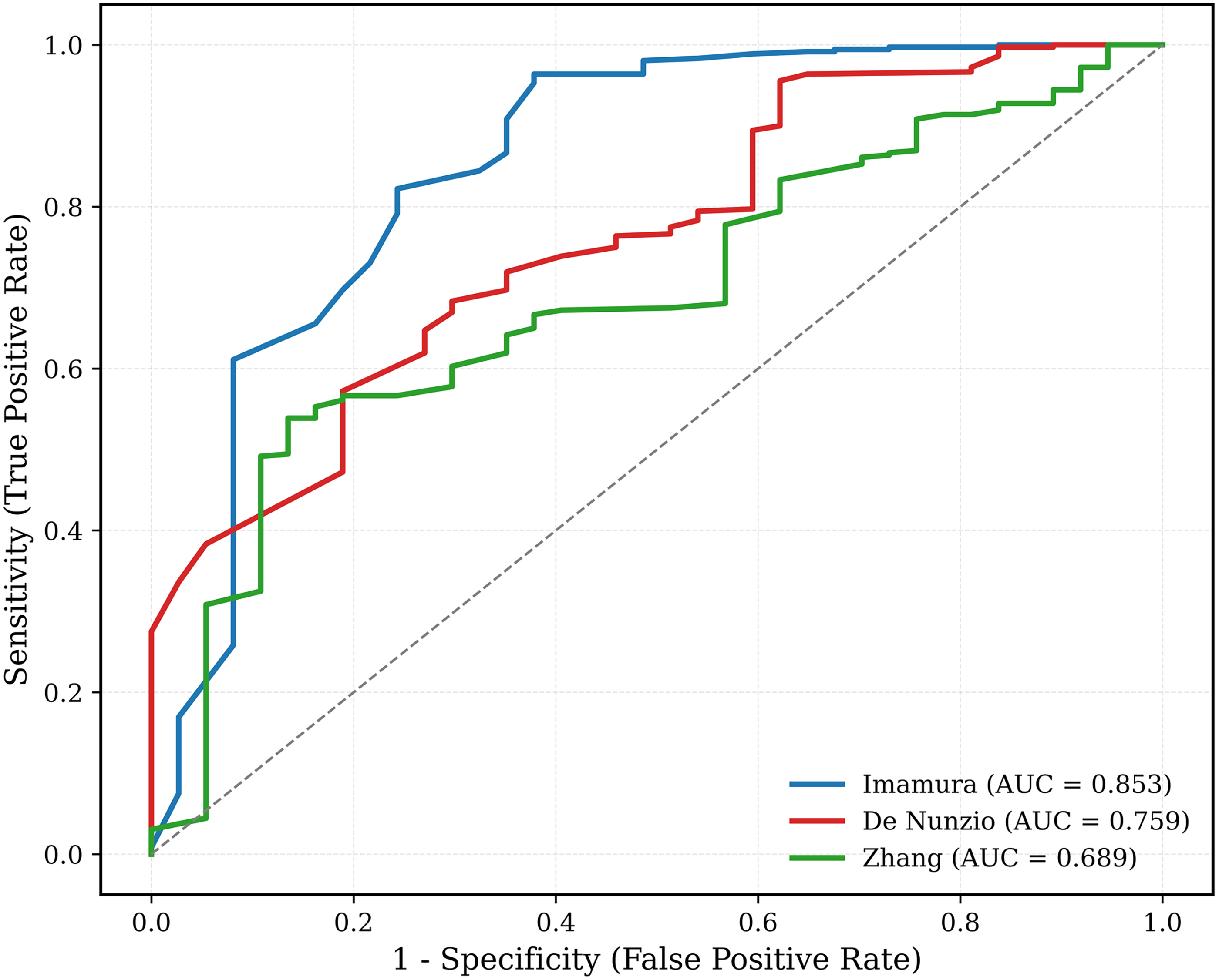
Combined receiver operating characteristic (ROC) curves comparing the discriminative performance of the Imamura, De Nunzio, and Zhang nomograms for predicting stone-free status after ureteroscopic lithotripsy. The Imamura model demonstrated the highest AUC (0.853), followed by De Nunzio (0.759) and Zhang (0.689).
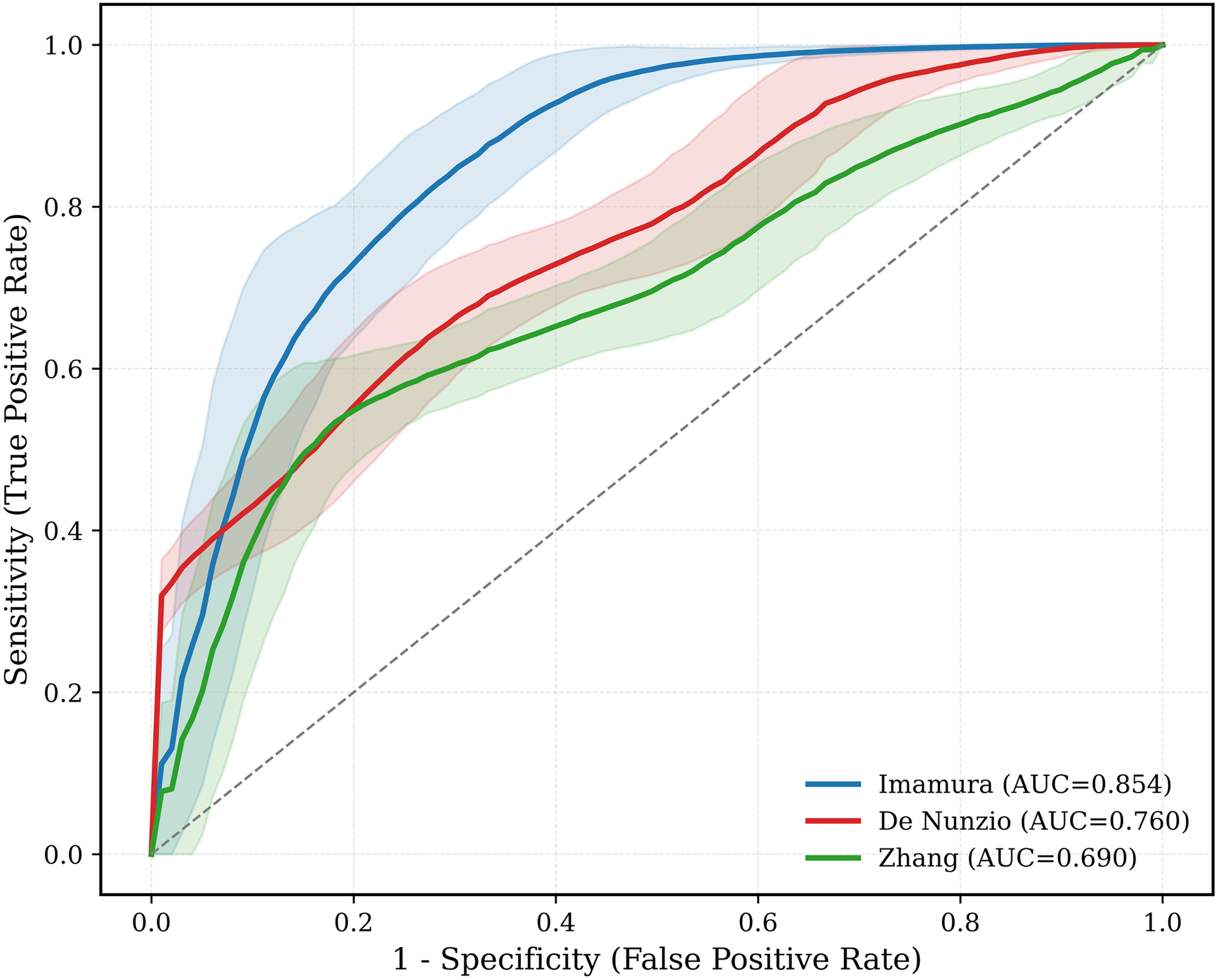
Bootstrapped mean ROC curves (1000 re-samples) with 95% confidence bands for the three nomograms. Bootstrap-corrected AUC values remained nearly identical to apparent AUCs, indicating minimal optimism and no evidence of overfitting.
Bias-corrected calibration plots for all nomograms are presented in Figure 3 (Fig. 3). In addition to discrimination, the overall performance metrics confirmed the robustness of the nomograms. The Imamura model demonstrated the lowest Brier score, indicating superior global accuracy (Brier score, 0.055), followed by the De Nunzio (0.075) and Zhang (0.081) models. Logistic re-calibration analyses revealed that CITL was effectively neutral (intercept ≈ 0), and calibration slopes were nearly 1.0 for all three models, consistent with the bias-corrected calibration plots derived from the bootstrap resampling. Collectively, these findings suggest that the Imamura nomogram offers superior discrimination and provides more accurate absolute risk estimates than the other two models.
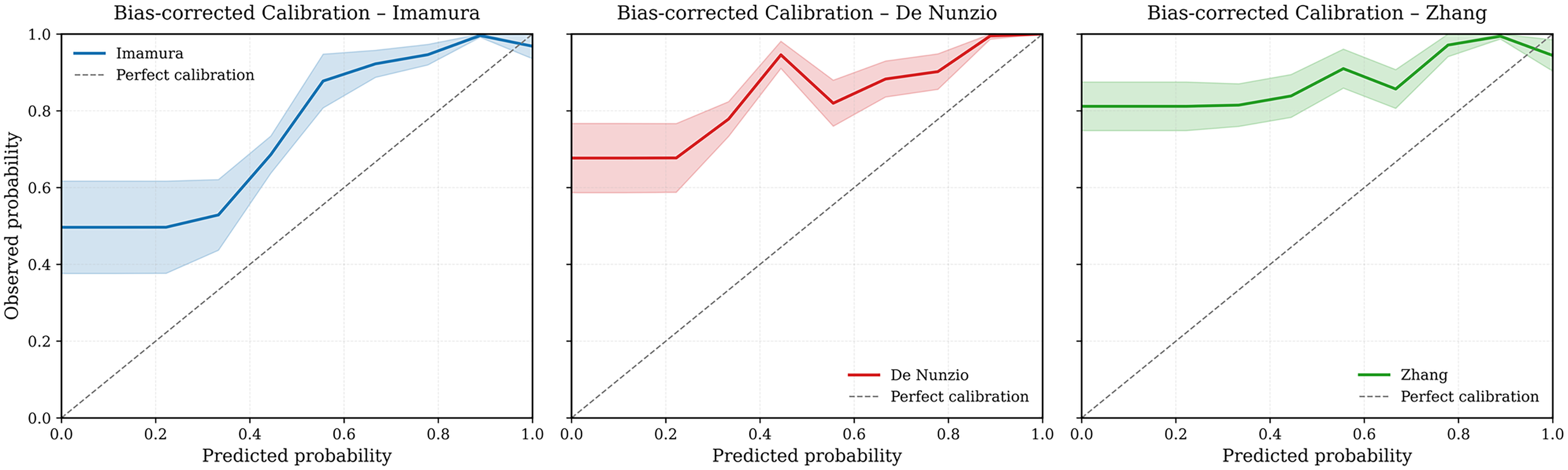
Bias-corrected calibration curves for the Imamura, De Nunzio, and Zhang nomograms based on 1000 bootstrap re-samples. The Imamura model showed the closest alignment between predicted and observed probabilities, demonstrating superior calibration.
DCA further demonstrated the clinical utility of the three nomograms across a spectrum of threshold probabilities ranging from 0.10 to 0.80 (Fig. 4). All models exhibited a superior net benefit compared to the “treat none” strategy throughout this range. The Imamura nomogram consistently provided the highest net benefit and slightly surpassed the “treat all” approach across clinically relevant thresholds. The De Nunzio model yielded moderate benefit, while the Zhang nomogram performed poorly, remaining below the “treat all” strategy for low thresholds. These findings indicate that among the three tools, the Imamura nomogram is most likely to offer a significant advantage in guiding preoperative decision-making beyond standard clinical judgment alone.
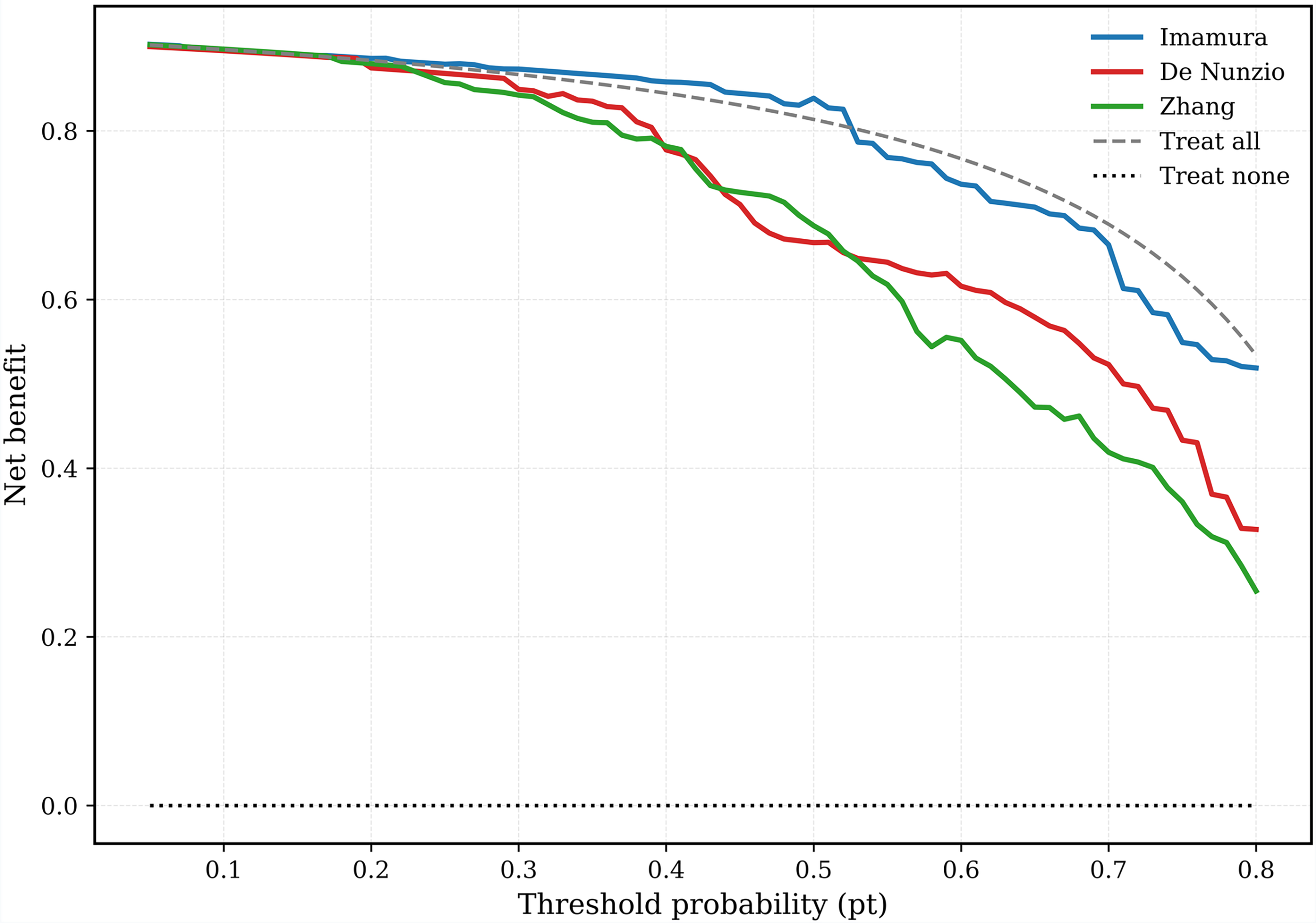
Decision curve analysis (DCA) for the Imamura, De Nunzio, and Zhang nomograms across threshold probabilities ranging from 0.10 to 0.80. The Imamura model demonstrated the greatest net clinical benefit throughout the entire threshold range, consistently outperforming both the “treat-all” and “treat-none” strategies, while the De Nunzio and Zhang nomograms showed limited incremental benefit.
Discussion
An ideal nomogram for patients undergoing stone surgical procedure should be simple, reproducible, and based on easily accessible clinical and radiological parameters. Accurate preoperative predictions of stone-free status should be made to facilitate treatment planning and patient counseling.
The SFR observed in our sample (90.7%) is consistent with the current outcomes of ULT documented in the literature. Several factors contribute to the success of ULT, with the location, size, and number of stones being the most critical determinants. Notably, stone location was a common predictor across all three nomograms. According to the Clinical Research Office of the Endourological Society (CROES) Ureteroscopy Global Study, proximal stones are associated with higher rates of failure and the need for re-treatment, particularly when semi-rigid URS is used. 8 Given that flexible URS is routinely employed for proximal stones at our institution, only distal stones treated with semi-rigid URS were included in this study to ensure procedural consistency.
In the nomograms developed by Imamura and De Nunzio, stone length and number were utilized as predictive factors, whereas the Zhang nomogram employed the stone diameter. It has been established that larger and multiple stones negatively impact the success of ULT, frequently requiring multiple treatment sessions. 9 A recent meta-analysis emphasized that stone area may offer the most accurate prediction of SFR. 10 Consistent with these findings, stone diameter and number emerged as significant predictors of SFR in our cohort.
In our cohort, pyuria emerged as a particularly strong predictor, aligning with the hypothesis that preoperative inflammation may indicate occult infection, epithelial edema, or underlying impaction that could impede effective fragmentation or clearance. Recent studies have similarly highlighted that sterile pyuria may function as a surrogate marker for impacted stones or increased intraluminal pressure, corroborating our finding that pyuria significantly exacerbates surgical outcomes.4,11,12
Stone impaction emerged as a significant independent predictor of non-stone-free status in our cohort. This observation aligns with the well-documented effects of chronic obstruction, mucosal edema, and diminished ureteral compliance on ureteroscopic maneuverability and stone fragment clearance.13,14 Notably, none of the evaluated nomograms incorporated stone impaction as a parameter, despite its evident clinical significance. This omission may partially account for the limited efficacy of certain models in practical applications and underscores the necessity for future predictive tools to integrate impaction or related markers of obstruction when assessing ureteroscopic success.
Hydronephrosis is a variable considered in the De Nunzio and Zhang models and has been associated with decreased success rates, likely because of inflammation and ureteral dilatation, which hinder access and effective stone fragmentation.5,6 While hydronephrosis was linked to lower SFR in the univariable analysis, it did not maintain significance in the multivariate analysis. This pattern likely indicates collinearity between hydronephrosis and the true obstructive burden; once more specific markers of obstruction (e.g., impaction, pyuria) are considered, hydronephrosis contributes limited additional value.
Zhang et al. incorporated HT and WBC counts into their model, suggesting that HT may be linked to residual fragments through systemic inflammatory and oxidative mechanisms. 6 While HT was associated with SFR in the univariate analysis, it did not achieve significance in the multivariate analysis. Similarly, the WBC count was not a significant predictor in our cohort. Additionally, the surgeon’s experience and consistency of the technique are critical factors influencing surgical outcomes. 15 In our study, all procedures were performed by experienced surgeons using a standardized approach that included the placement of a safety guidewire and Holmium:YAG laser lithotripsy.
From a clinical standpoint, the integration of the Imamura nomogram into practice may facilitate several key areas: identifying patients most likely to benefit from a single-session URS, recognizing high-risk individuals who may necessitate staged procedures, and informing discussions regarding alternative options, such as extracorporeal shock wave lithotripsy or delayed intervention. Although no predictive model can supplant surgical judgment, tools that enhance risk stratification are increasingly valuable as precision-based management continues to advance in endourology.
This study has several limitations that should be acknowledged. First, its retrospective, single-center design may introduce selection bias and limit generalizability. Second, certain perioperative factors were not standardized, including postoperative stent placement and duration, which were determined at surgeon discretion and may have introduced variability compared with nomogram development cohorts using standardized protocols. Additionally, stone composition was not systematically incorporated, although it may influence fragmentation efficiency and treatment outcomes. Third, stone-free status was assessed using NCCT at 1 month, which differs from the 3-month end point used in the original Imamura nomogram and may limit direct comparability. Finally, adjunctive flexible ureteroscopy was not routinely utilized, which may affect comparisons with studies incorporating flexible instruments for retropulsion or concomitant stones. Despite these limitations, the use of a homogeneous cohort and robust internal validation strengthens the reliability of our findings, which warrant confirmation in prospective, multicenter studies.
Conclusion
The present study offers a comprehensive evaluation of three nomograms designed to predict stone-free outcomes following ULT with semi-rigid URS for the treatment of distal ureteral stones. Our findings indicate that the Imamura nomogram exhibits superior discriminative performance, accurate calibration, and enhanced clinical utility compared with the other two tools. Key factors such as stone diameter, impaction, multiplicity, and pyuria significantly influenced surgical outcomes. Future multicenter prospective studies with external validation are necessary to further assess the generalizability of these findings.
Authors’ Contributions
M.S.: Protocol development, data analysis, article writing. E.A.: Data collection and data analysis. Y.N.A.: Data collection and data analysis. M.Ş.Ö.: Data collection and data analysis. Y.C.F.: Data analysis and article editing. H.L.C.: Article editing.
Ethical Approval
The research was conducted according to the principles of the World Medical Association Declaration of Helsinki “Ethical Principles for Medical Research Involving Human Subjects.” Ethics committee approval was obtained from the Basaksehir Cam and Sakura City Hospital Ethics Committee (approval number: 05.03.2025.84).
Footnotes
Data Availability
The data that support the findings of this study are not openly available because ofto the reasons of sensitivity and are available from the corresponding author upon reasonable request.
Author Disclosure Statements
The authors declare that they have no conflicts of interest.
Funding Information
The authors did not receive support from any organization for the submitted work.