
Abstract
Objective:
In animal models, sodium acetate has been shown to protect against acute kidney injury (AKI) via activation of the hypoxia-inducible factor pathway. We report our clinical experience with sodium acetate as an intraoperative renoprotective agent in patients undergoing robotic partial nephrectomy.
Patients and Methods:
Retrospective review of a single-surgeon experience using intraoperative sodium acetate infusion (SAI; 150 mEq at 200 mL/h) during partial nephrectomies. Primary outcomes included rates of AKI as defined by established standardized criteria (i.e., KDIGO [Kidney Disease: Improving Global Outcomes], RIFLE [Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease]). Propensity score matching without replacement was used to balance baseline characteristics between groups. Subsequent association between SAI and AKI events was assessed using logistic regression analysis in the matched cohort.
Results:
Overall, SAI did not impact postoperative renal function based on serum creatine level or glomerular filtration rate. On logistic regression analysis of the matched cohort, the administration of intraoperative SAI was associated with a 58% and 61% lower odds of AKI on postoperative day 1 based on the RIFLE (p = 0.06, CI 0.17–1.03) and KDIGO (p = 0.05, CI 0.15–1.01) criterion for AKI, respectively. In the subset of patients who had pre-existing chronic kidney disease (CKD), SAI was associated with significantly lower rates of AKI using both the RIFLE (p = 0.01) and KDIGO (p < 0.05) criteria.
Conclusion:
Perioperative SAI did not confer a statistically significant renoprotective effect for all patients undergoing partial nephrectomy. However, it may reduce the odds of postoperative AKI based on the RIFLE/KDIGO criterion, particularly in patients with pre-existing CKD. Further research is warranted to determine the clinical impact of sodium acetate as a renoprotective agent.
Introduction
Minimizing acute and chronic injury following robotic partial nephrectomy (RPN) remains a challenge. A decrease in renal function is the norm, although in most cases, the kidney will regain 80% to 90% of its preoperative function. 1 However, as much as 22% of these patients will go on to develop de novo chronic kidney disease (CKD) within a year, 2 and 25% of patients with preoperative CKD will be upstaged postoperatively. 3 Therefore, the optimization of modifiable intraoperative factors is critical. Most efforts have focused on surgical techniques and approaches aimed at limiting the extent of ischemic injury and the preservation of parenchyma. 1 Renoprotective agents are an alternative, but their use is less studied. Historically, mannitol was employed as a renoprotective agent but has been shown to not provide any clinical benefit. 4
Sodium acetate has unique properties as it can act as a buffer to stabilize serum pH and alkalinize urine. 5 In animal models, warm ischemia from renovascular clamping elicits an adaptive response to hypoxia.6,7 One of these pathways is modulated by the hypoxia-inducible factor, which can be activated by exogenous acetate, resulting in the increased expression of erythropoietin (EPO). 8 Clinically, EPO has been used as a renoprotective agent, particularly when given preoperatively. Two small randomized controlled trials involving patients undergoing elective cardiac surgery found a renoprotective effect by EPO that was given preoperatively and was associated with lower rates of acute kidney injury (AKI).9,10 In a mice model, pretreatment with EPO for 3 days prior to renovascular clamping attenuated renal dysfunction and injury compared with single EPO dose following reperfusion. 11 Using a similar approach, the use of acetate was explored in a porcine single renal unit model where an intraoperative acetate infusion showed a renoprotective benefit at 72 hours following 90 minutes of hilar clamping. 12 In this study, we report our clinical experience with intraoperative sodium acetate as a renoprotective agent in patients undergoing RPN.
Patients and Methods
This is a retrospective review (IRB: STU 20250867) of patients who underwent RPN for suspected malignancy by a single surgeon following a change in practice where sodium acetate infusion (SAI) became the preferred choice for intraoperative fluid management. Patients with low cardiopulmonary reserve were excluded at the discretion of the anesthesiologist. For comparison purposes, a historical cohort of consecutive patients that immediately preceded the SAI group was included. Patients in the comparison group received normal saline infusion during RPN (crystalloid group). The SAI infusion started upon anesthesia induction and transitioned to normal saline at 75 mL/h at the conclusion of the robotic portion of the case and maintained at this rate for both groups through the remainder of their hospital stay. Dosing of SAI was 150 mEq of sodium acetate in 1 liter of 5% dextrose or sterile water infused at 200 mL/h, which translates to 30 mM/h and is well below the toxic level of 200 mM/h as reported in the medical toxicology literature. 5 The SAI solution was compounded by the inpatient pharmacy and delivered to the OR ready to be used. Postoperative electrolyte imbalances for both groups were managed as clinically indicated based on institutional protocols.
Renal function was evaluated within the context of the surgeon practice, which included a basic metabolic panel within 2 weeks of surgery, immediately following surgery, night on postoperative day (POD) 0, the morning of POD1, and again at 2 to 4 weeks after surgery. The glomerular filtration rate (GFR) was estimated using the 2021 CKD-EPI equation. 13 The complexity of tumors was determined using the RENAL (Radius, Exophytic/Endophytic, Nearness to collecting system, Anterior/posterior, Location relative to polar line) Nephrometry Score. 14 The rates of AKI were calculated using the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 guidelines 15 and the RIFLE (Risk, Injury, Failure, Loss of Kidney function, and End-stage kidney disease) criterion. 16 To the best of our knowledge, this is the first study to report rates of AKI following RPN using the KDIGO criterion. The KDIGO criterion is a continuation and/or updated version of RIFLE. Within the urology literature, the definition of AKI is largely limited to the RIFLE criterion. Whereas, in other fields, there has been a shift toward using KDIGO. For example, a recent study evaluated the use of a perioperative infusion of amino acids in patients undergoing elective cardiac surgery that was found to be beneficial in decreasing rates of AKI in the postoperative setting. 17 This study used the KDIGO criterion to define AKI. We believe that reporting AKI rates using both definitions would allow for more accurate reporting but also allow for comparison to prior studies using the RIFLE criterion. See Supplementary Table S1 for direct comparison between the KDIGO and RIFLE criteria.
Baseline characteristics between patients who received SAI and the historical comparison group were calculated using the Kruskal–Wallis test and chi-square for continuous and categorical, respectively. Primary outcomes of the study included the occurrence of AKI on POD1 in patients undergoing RPN. Secondary outcomes included the overall change in postoperative renal function based on GFR and serum creatinine (SCr). To reduce potential confounding in this observation study, we performed 1:1 nearest neighbor propensity score matching without replacement. The propensity score represents the probability of receiving acetate infusion, estimated for each patient using a logistic regression model based on the following baseline covariates: age, estimated blood loss (EBL), body mass index (BMI), preoperative GFR, RENAL Nephrometry Score, and ischemia time. In the 1:1 nearest neighbor matching approach, each patient in the treatment group was matched to a single patient in the control group based on the closest estimated propensity score. After matching, balance diagnostics were conducted to assess the adequacy of covariate balance between groups. In addition, rates of AKI events were calculated in the matched cohort and in a subset of patients with CKD stage 2 or higher (GFR < 90 mL/min/1.73 m2) in the nonmatched cohort. Data analyses were performed using Stata (StataCorp LLC, College Station, TX, USA). Illustrations were completed using Microsoft 365 (© Microsoft 2025, Redmond, WA, USA).
Results
A total of 190 patients underwent RPN between January 2023 and September 2024, of which 96 had intraoperative SAI and 94 received routine maintenance fluid management with crystalloid fluids (Table 1). A total of 20 patients were excluded from SAI infusion, most of which 14 were due to nonclinical reasons (i.e., communication gaps and shortage of IV fluids). The median volume of SAI was 537 mL (IQR 472–600). In the SAI group, 59 patients received SAI in D5W and 37 in sterile water. Electrolyte imbalances (hyperglycemia and hyperkalemia) were more common in the SAI group during the immediate postoperative period (Table 2) and similar between the groups by POD1 (Table 3). Electrolyte imbalances appeared to be less frequent once SAI in sterile water was instituted, but differences were not statistically significant (Table 3).
Baseline Characteristics
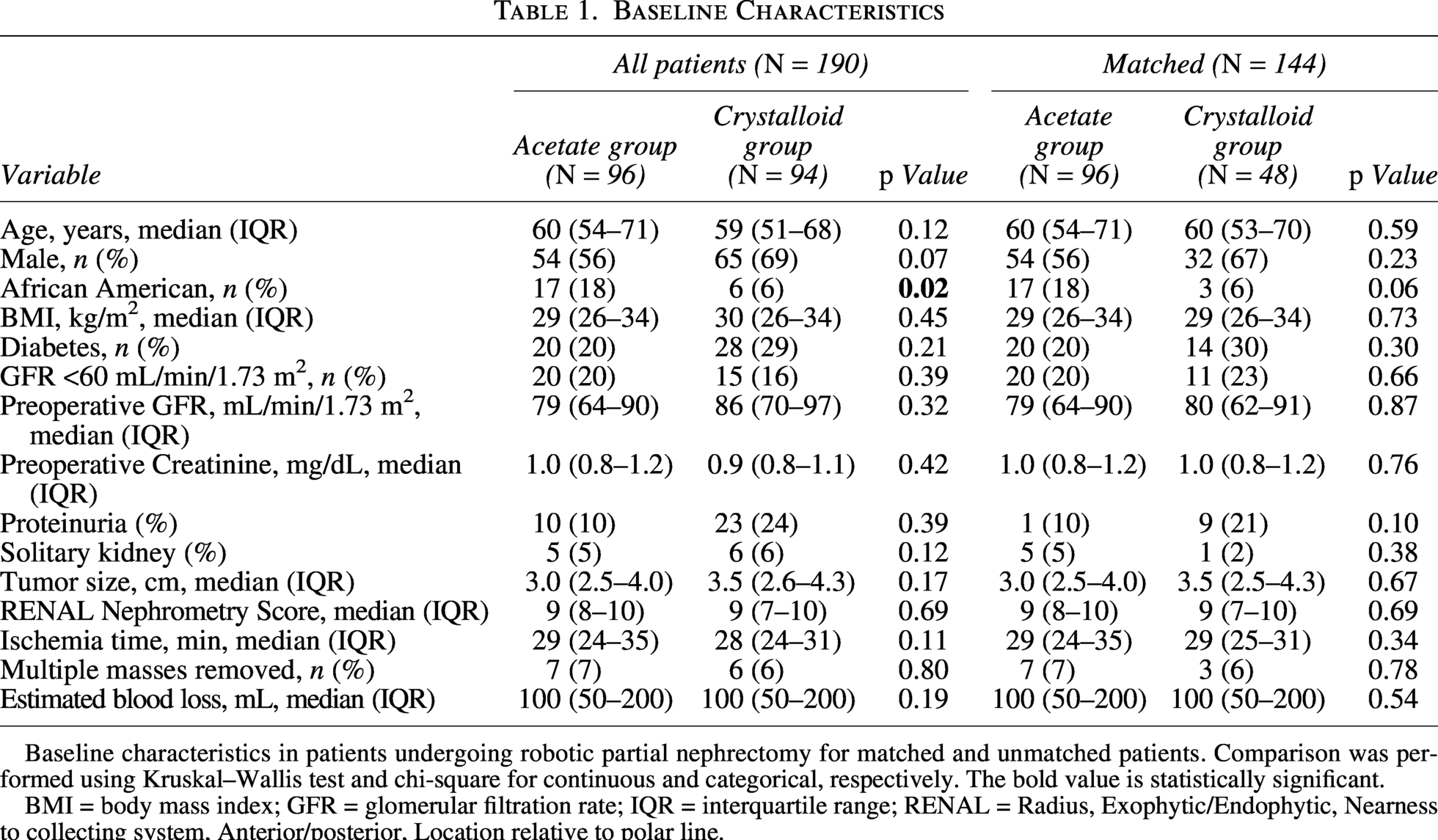
Baseline characteristics in patients undergoing robotic partial nephrectomy for matched and unmatched patients. Comparison was performed using Kruskal–Wallis test and chi-square for continuous and categorical, respectively. The bold value is statistically significant.
BMI = body mass index; GFR = glomerular filtration rate; IQR = interquartile range; RENAL = Radius, Exophytic/Endophytic, Nearness to collecting system, Anterior/posterior, Location relative to polar line.
Electrolyte Imbalances Following Robotic Partial Nephrectomy
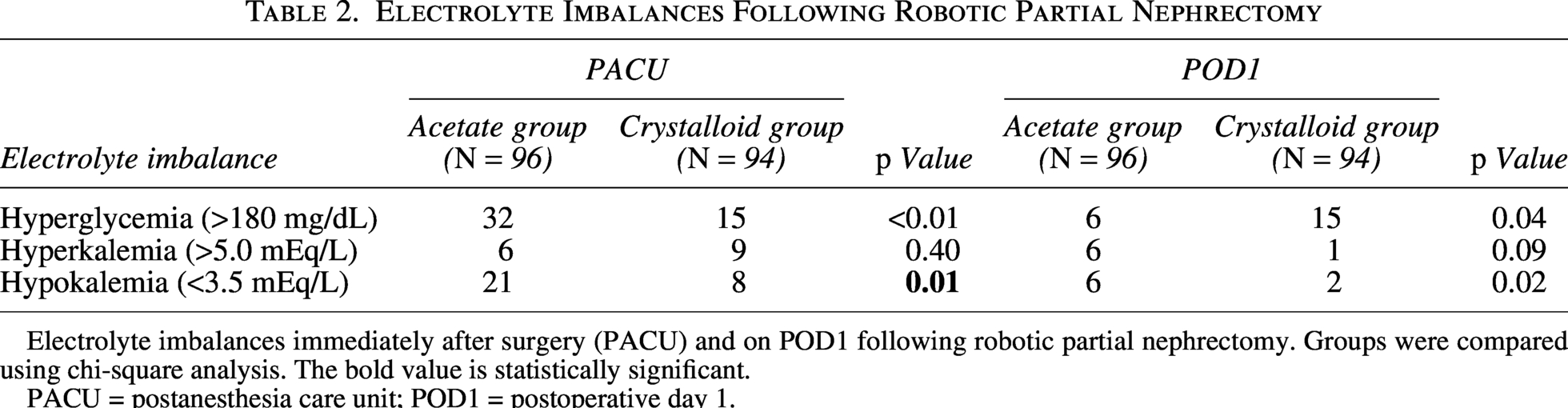
Electrolyte imbalances immediately after surgery (PACU) and on POD1 following robotic partial nephrectomy. Groups were compared using chi-square analysis. The bold value is statistically significant.
PACU = postanesthesia care unit; POD1 = postoperative day 1.
Electrolyte Imbalances with Sodium Acetate Infusion During Robotic Partial Nephrectomy
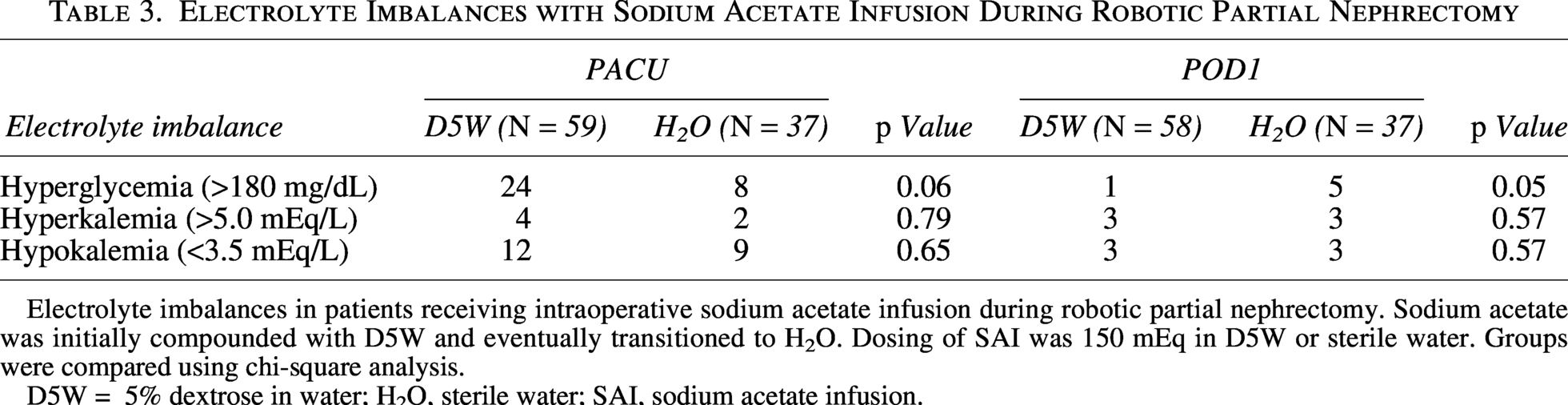
Electrolyte imbalances in patients receiving intraoperative sodium acetate infusion during robotic partial nephrectomy. Sodium acetate was initially compounded with D5W and eventually transitioned to H2O. Dosing of SAI was 150 mEq in D5W or sterile water. Groups were compared using chi-square analysis.
D5W = 5% dextrose in water; H2O, sterile water; SAI, sodium acetate infusion.
Baseline characteristics between the cohorts were not statistically different with the exception of the number of African American patients where they represented 18% in acetate group and 6% on the crystalloid group (p = 0.02). The study was largely limited to patients with small renal masses with 70% (crystalloid group) to 73% (acetate group) having T1a renal masses. Only one patient in either group had a T2 renal mass who had an imperative indication for nephron-sparing surgery (Supplementary Table S3).
After performing 1:1 nearest neighbor matching, 48 controls were well matched to 96 patients undergoing SAI and were kept for analysis. Differences in the clinical characteristics of the matched patient cohort were not statistically significant. The median preoperative GFR before and after matching remained less than 90 mL/min/1.73 m2. Compared with the matched cohort (N = 48), the 46 control patients that were nonmatched were younger, had greater EBL, and had lower ischemia times (Supplementary Table S3).
Differences in perioperative renal function based on SCr and GFR were not statistically significant, overall or in the matched cohort (Table 4). The rates of AKI in the nonmatched and matched cohorts were not significantly different (Table 5). In the matched group, rates of AKI in the acetate group ranged from 8% to 9% depending on the AKI criterion compared with 12% to 14% in the crystalloid group that did not receive SAI. In the matched analysis and when adjusted for confounding variables, the administration of SAI was associated with a 58% and 61% lower odds of AKI on POD1 based on the RIFLE (p = 0.06, CI 0.17–1.03) and KDIGO (p = 0.05, CI 0.15–1.01) and criterion for AKI, respectively (Table 6). In a subset of patients with pre-existing CKD Stage 2 or higher, SAI was associated with a lower rate of AKI events using both the KDIGO (p < 0.05) and RIFLE (p = 0.01) criteria.
Perioperative Renal Function (Matched Patients)
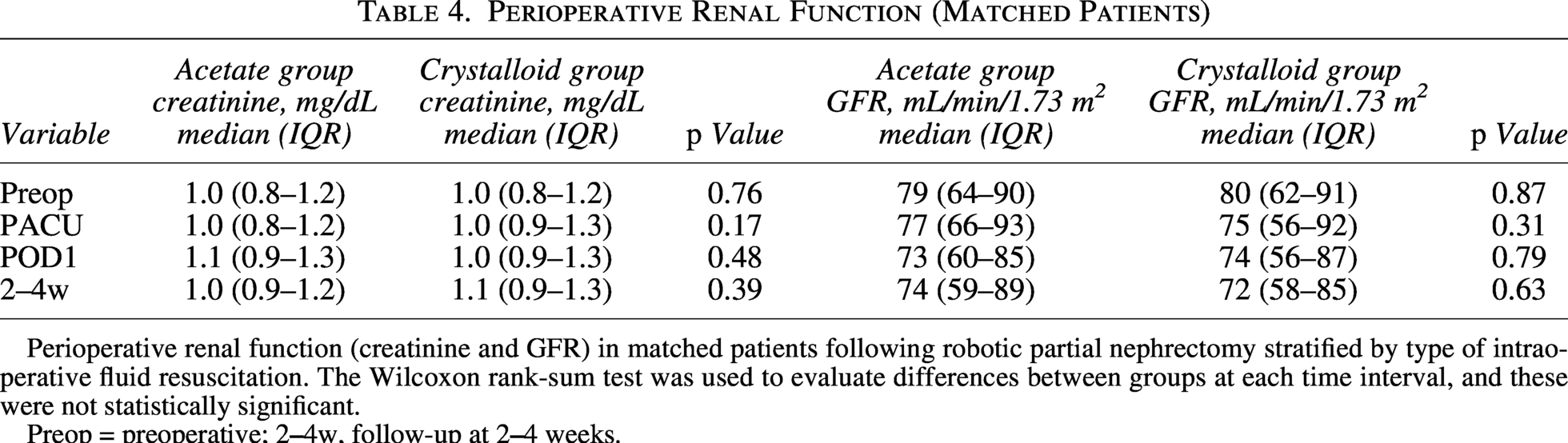
Perioperative renal function (creatinine and GFR) in matched patients following robotic partial nephrectomy stratified by type of intraoperative fluid resuscitation. The Wilcoxon rank-sum test was used to evaluate differences between groups at each time interval, and these were not statistically significant.
Preop = preoperative; 2
Postoperative Acute Kidney Injury
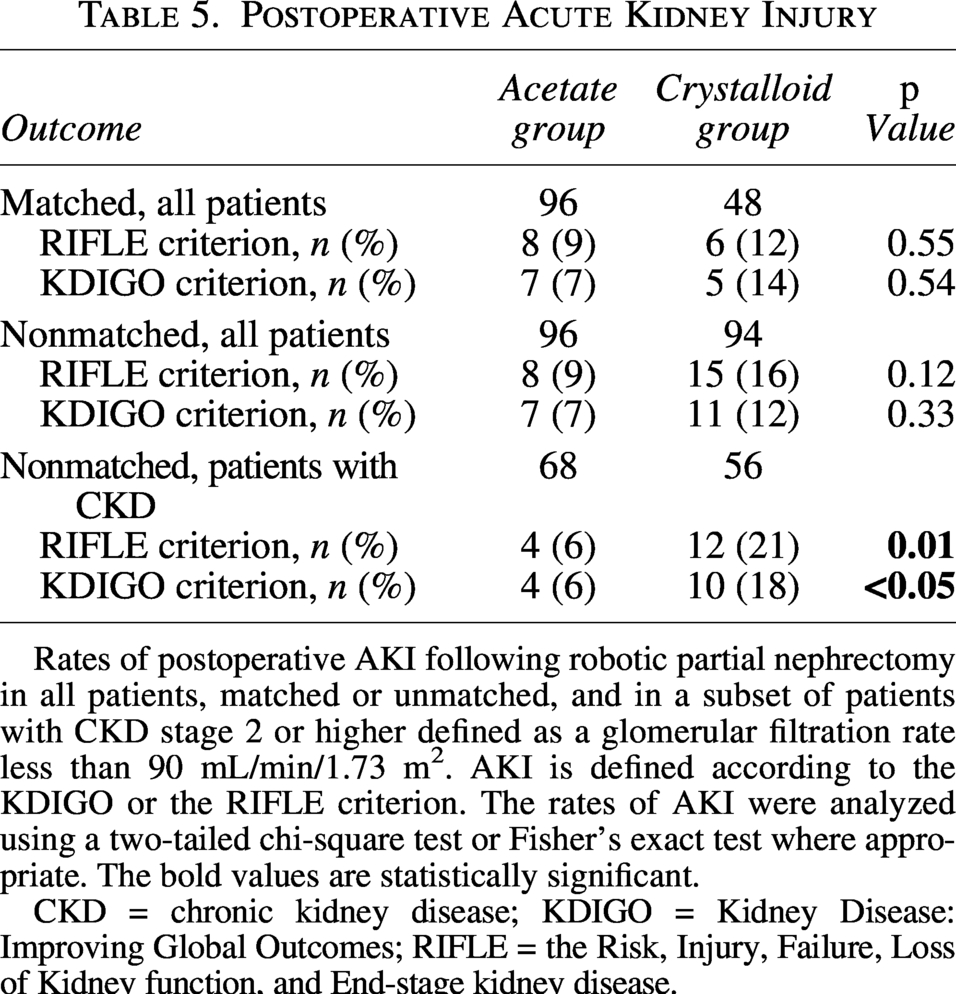
Rates of postoperative AKI following robotic partial nephrectomy in all patients, matched or unmatched, and in a subset of patients with CKD stage 2 or higher defined as a glomerular filtration rate less than 90 mL/min/1.73 m2. AKI is defined according to the KDIGO or the RIFLE criterion. The rates of AKI were analyzed using a two-tailed chi-square test or Fisher’s exact test where appropriate. The bold values are statistically significant.
CKD = chronic kidney disease; KDIGO = Kidney Disease: Improving Global Outcomes; RIFLE = the Risk, Injury, Failure, Loss of Kidney function, and End-stage kidney disease.
Logistic Regression Analysis Odds of AKI by Acetate Infusion
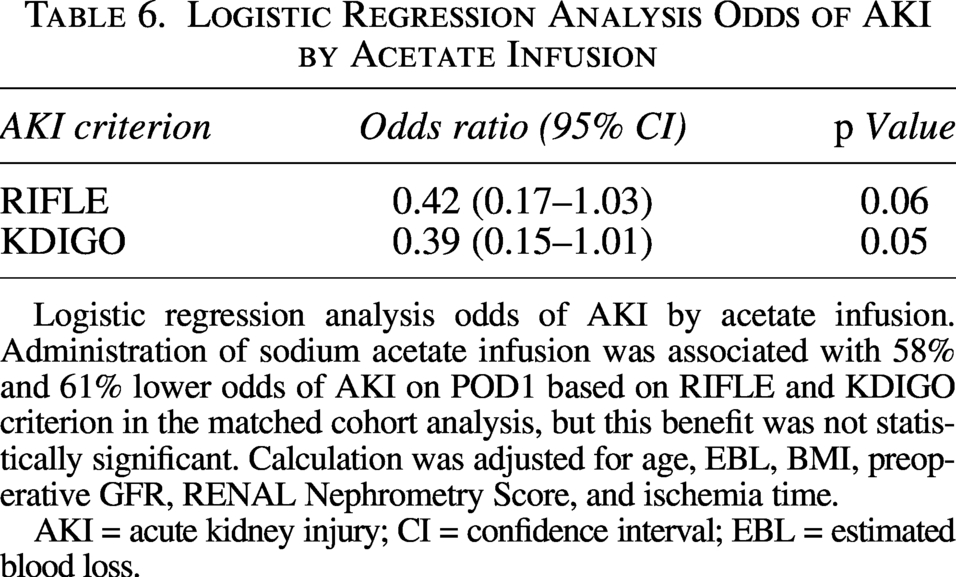
Logistic regression analysis odds of AKI by acetate infusion. Administration of sodium acetate infusion was associated with 58% and 61% lower odds of AKI on POD1 based on RIFLE and KDIGO criterion in the matched cohort analysis, but this benefit was not statistically significant. Calculation was adjusted for age, EBL, BMI, preoperative GFR, RENAL Nephrometry Score, and ischemia time.
AKI = acute kidney injury; CI = confidence interval; EBL = estimated blood loss.
Among patients in the nonmatched cohort, patients with a solitary kidney amounted to 5 and 6 in the SAI and crystalloid group, respectively. One of these patients in the SAI group developed AKI (KDIGO and RIFLE) compared with three in the crystalloid group. All of these patients met the AKI criterion using both the KDIGO and RIFLE criteria. All of these patients had their renal function evaluated at 1 month after surgery, with four out of five patients in the SAI group regaining at least 90% of their preoperative GFR compared with two out of six patients in the crystalloid group.
Discussion
This study evaluated the clinical use of SAI as a renoprotective agent during RPN and found evidence of reduced odds of AKI based on KDIGO criterion in patients receiving SAI, although such benefit (p = 0.05) did not meet the conventional level of statistical significance. However, it may reduce the odds of postoperative AKI based on the RIFLE/KDIGO criterion, particularly in patients with pre-existing CKD. These retrospective results should be interpreted as hypothesis-generating, and further study is needed.
In the post-PN setting, AKI is often reported according to the RIFLE criterion that was originally published in 2004 and updated in 2012 (redefined as KDIGO). 18 Despite standardized reporting, contemporary rates of AKI in the post-RPN have ranged between 10% and 56%.19,20 This is noteworthy as our low rates of AKI (7–14% depending on diagnosing criterion) could have been influenced by lead-time bias as the majority of patients were discharged the day after surgery before their SCr might have peaked. For this reason, we included the KDIGO criterion as it has the ability to diagnose AKI earlier given the lower threshold for a significant increase in SCr in the acute setting (≥0.3 mg/dL within 48 hours). Despite these efforts, the aforementioned AKI definitions are at least partly based on SCr, which is prone to diurnal variations that make the clinical significance of mild cases of AKI difficult to identify.
The natural history of renal function following AKI in the post-PN setting is also not well understood. It is suggested that AKI may trigger a maladaptive cellular response resulting in renal fibrosis that exacerbates kidney damage, putting patients at risk of progressive renal dysfunction.18,21 A large cohort study that evaluated 1-year outcomes in patients who underwent PN found that patients with AKI post-PN were less likely to regain 90% of their preoperative baseline function than their counterparts who did not experience AKI. 20 On the contrary, when adjusted for parenchymal volume, AKI did not significantly impact long-term renal function in patients with solitary kidneys after PN. 22 A follow-up study evaluated the extent to which modifiable risk factors account for the inherent decline in renal function post-PN and reported that the new baseline GFR was 70% attributable to parenchymal loss and 30% to perioperative factors such as AKI and ischemia time. 23 This being said, it is possible that reported rates of AKI in the post-PN setting are an overestimation where the decline in renal function is primarily due to the loss of renal parenchyma and not AKI.
The efficacy of renoprotective agents is not well defined in the PN population. Spaliviero et al. published on the intraoperative use of mannitol during PN and found that mannitol did not improve renal function outcomes at 6 months. 4 Study criticisms were related to generalizability concerns given that the reported dose of mannitol was lower than what was commonly used and the inclusion of mostly patients with normal baseline renal function who may be more resilient to AKI. Follow-up studies by other authors addressed some of the limitations of the trial and confirmed the lack of renoprotective benefit.24–27 Interestingly, all of these studies evaluated the effect of renoprotection in the context of SCr or estimated GFR, which differs from the dichotomous outcome of AKI. Whether one is more appropriate than the other is debatable as they provide different insights. The KDIGO criterion, and its prior iterations, standardized the definition of AKI in an attempt to identify patients with renal impairment earlier in their clinical course and allow for prompt intervention. Such definitions allow for the risk stratification of AKI by its severity and duration, which have been associated with adverse renal functional outcomes. 21 On the other hand, the assessment of renal function using a continuous variable as the primary end point (SCr/GFR) to evaluate the efficacy of a renoprotective agent is pragmatic and simple to interpret.
Patients tolerated SAI without major issues. No volume overload complications occurred, and none of the patients received renal replacement therapy. In instances where patients developed electrolyte imbalances, these were managed as clinically indicated without escalation of care and/or prolonged hospital stay. These occurrences prompted the change to sterile water with SAI as opposed to D5W. Electrolyte imbalances appeared to stabilize, but differences were not statistically different.
Limitations of this study include inherent biases related to its retrospective design. The presence of AKI was determined using SCr according to the KDIGO/RIFLE criteria, and not urine output (UO) or biomarkers suggestive of kidney damage such as serum cystatin C. As a result, rates of AKI could have been underestimated. The intraoperative and postoperative fluid status of patients could not reliably be evaluated as the documentation of fluid administration and UO were not completed in a controlled clinical setting. Third, there is the possibility that AKI events could have been overestimated as volumetric analysis to adjust for the loss of devascularized parenchymal volume was not possible. Fourth, the vast majority of patients included in this cohort had a contralateral kidney. The extent and timing of any compensatory renal function by the contralateral kidney is difficult to discern. As such, it is possible that AKI rates may have been underestimated.
This study has strengths worth mentioning. Sodium acetate is inexpensive, readily available, and commonly used in other medical settings. Such familiarity facilitated the implementation of SAI for intraoperative fluid management during RPN. Furthermore, this review included all patients with a median preoperative GFR consistent with CKD Stage II, which may be reflective of practices by high-volume surgeons and/or centers. In our unadjusted analysis of a nonmatched subset of patients with pre-existing CKD, rates of AKI in patients who received SAI were 6% compared with 18% (KDIGO, p < 0.05) and 21% (RIFLE, p = 0.01) in those who did not receive SAI. However, our small series did not allow for the analysis of CKD patients in our matched cohort. Nonetheless, our data support a possible beneficial role for the use of SAI in patients with suboptimal renal function.
In conclusion, SAI did not impact postoperative renal function based on SCr or GFR for all patients undergoing RPN. Administration of intraoperative SAI during RPN reduced the odds of postoperative AKI based on the KDIGO criterion, albeit this benefit did not meet conventional levels of statistical significance (p = 0.05). Further investigation, including prospective evaluation, randomization, and volumetric analysis, is necessary to determine the clinical impact of sodium acetate as a renoprotective agent.
Authors’ Contributions
I.P.-Z.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing—original draft preparation, and writing—review and editing. R.R.B.: Formal analysis and methodology. Z.-E.K.: Formal analysis and methodology. D.S.: Data curation, investigation, and project administration. R.B.: Investigation. K.A.: Investigation. J.C.: Conceptualization, investigation, supervision, methodology, writing—original draft preparation, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.