
Abstract
This study uses the Structurational Model of Identification (SMI) to investigate how resident primary care physicians (PCPs) manage multi-level identity conflicts during the routine activity of the medical office visit. Drawing from interviews with 27 physicians and more than 47 hours of office visit observations, the data build a Structurational Model of Identity Conflict. The model depicts how physicians encounter a taxonomy of identity-centered constraints, including financial (e.g., insurance availability), material (e.g., computer-use), and temporal (e.g., waiting times), among others, that disrupt their identification during office visits, creating multi-level (e.g., relational vs professional) identity conflicts. PCPs created and shared care appropriations (i.e., workarounds) to reposition their identities and re-engage with important social contexts of work (i.e., compassionate, patient-centered care). The model also depicts how the micro-level strategies that PCPs employed to manage their identity tensions during office visits were shared, routinized, and reified, generating structurational change. This study offers practical implications for professions beyond medicine, such as education, social work, and legal aid, where practitioners must balance competing structural demands with relationship-oriented goals through creatively appropriating identity and work tasks.
Keywords
Introduction
Notions of being a “good worker” are often examined within organizational communication and identity research (Long & Buzzanell, 2022, 2024). These studies show how discursive constructions of being a “good worker” are shaped by professional structures that reward constant availability, despite illnesses or family events, and discourage accommodation requests (Long & Buzzanell, 2024). Identifying as a “good worker,” then, often prioritizes professional and organizational identities over personal ones, reflecting both compliance with and resistance to intersecting workplace identity structures (Long & Buzzanell, 2022). The “good worker” illustrates identity as performative and multidimensional, showing how multiple identities are negotiated and conflict within organizational life (Tracy & Trethewey, 2005).
Yet the term “good worker” need not always prioritize professional identity. Consider the term “good doctor.” Professional physician identity—i.e., the internalization of physician values and norms—has been widely studied in medical and management research with an acute focus on residency (e.g., Barnhoorn et al., 2022; Pratt et al., 2006; Santivasti et al., 2022; Sawatsky et al., 2023, 2024). Residency is a formative period of professional and organizational socialization, in which residents learn not only the values and norms of the physician profession, but also the material routines, power structures, and communicative practices of specific clinical organizations (Van & Schein, 1977). The harsh realities (e.g., intense workloads; high-stakes decisions) and normative behaviors of medical practice learned during residency can clash with residents’ preconceived notions of being a “good doctor” (Sawatsky et al., 2023, 2024), which are often shaped by humanistic values that call physicians into medicine.
For physicians, medical residency represents a critical period for navigating identity conflicts. Identity conflicts arise when organizational actors encounter incompatible or competing identities at work, creating tension in their enactment (Williams & Connaughton, 2012) and often producing stress, frustration, anxiety, and discomfort that requires positive reframing (Ashforth et al., 2008; Woo et al., 2017). Unlike role conflict—defined as incompatible work roles (Katz & Kahn, 1978; Nicotera, 2015)—identity conflict is rooted in systems of self-meaning that shape how individuals understand and present who they are to others (Vough et al., 2024). Such conflicts require reconciling competing facets of the self and may generate significant dissonance (Larson & Pepper, 2003). Research has explored healthcare professionals’ role conflicts (Apker et al., 2005) and identity tensions (Kyratsis et al., 2017). Yet primary care physician (PCP) identity construction during residency remains understudied (Barnhoorn et al., 2022; Pratt et al., 2006). This gap is important, given PCPs encounter short patient visits, fragmented assessments, and high needs for rapport building, creating added constraints to patient care (Porter et al., 2023).
Guided by the Structurational Model of Identification (SMI; Scott et al., 1998), this paper demonstrates how resident PCPs fluidly draw upon and distance themselves from multiple identity sources to manage competing goals during the highly turbulent time of residency (see Kuhn & Nelson, 2002; Woo et al., 2017). Given identity is situational, I focus on how resident PCPs manage multiple salient identities during medical office visits—a fundamental PCP activity. Results contribute to organizational identity/identification research by building a theoretical model that (a) offers an identity-centered taxonomy of constraints that produce multi-level identity conflicts within situated clinical activity, (b) connects multi-level identity conflicts with care appropriations, and (c) shows how appropriations become shared and result in structurational change. Data also show how fundamental activities structure identity through temporality. Below, I begin by explaining Scott et al.’s (1998) SMI framework, followed by an explanation of the constraints that providers encounter in underserved patient care. I then pose the study’s research questions, report the findings, and explain the study contributions.
Literature Review
The Structurational Model of Identification
The Structurational Model of Identification (SMI; Scott et al., 1998) offers a framework for theorizing the reciprocal relationship between identity and identifications. Identities are the larger social structures—i.e., the rules and resources—that anchor the self, while identifications are the social acts and discourse that (re)produce those identities in everyday life. The SMI has been largely under-utilized in its ability to capture (a) identification with multiple identity targets and (b) how enacted identity dynamically (re)shapes and disrupts workplace practice (see Ault, 2018). Below, I detail how the SMI borrows from three foundational concepts in structuration theory (Giddens, 1984): duality of structure, regionalization, and situated activity. I then use the SMI to consider the multiple identities that PCPs navigate as they care for underserved patients during the office visits.
Duality of Structure: Physician Identity and Identification
Giddens (1984) coined the term duality of structure to explain the relationships between social structures and human agency. Social structures are comprised of rules and resources. Rules represent the routines, shared norms, and interpretive schemas that order human operation and that actors use to understand situations and appropriate behavior. Resources are the capabilities or assets that actors formally draw upon (e.g., money, technology, space, hierarchical authority, physical space) to exercise power and accomplish action within social systems. Human agency refers to the capacity of human beings to act independently, to consciously shape their own lives, and to create new social practices. For Giddens (1984), social life is constituted through a recursive relationship between structures (rules and resources) and human agency.
Within the SMI, identities function as structures that regulate notions of self, while identification is their situated communicative enactment (Scott et al., 1998). Unlike psychological approaches that frame identification as cognitive or emotional attachment operated through internalization (Schuster et al., 2024), the SMI theorizes identification as communicatively constituted in everyday work practices. It emphasizes how individuals discursively draw upon identity structures embedded in relational, organizational, and professional contexts. Thus, physician identification targets are not limited to emotionally valued persons or groups, but include institutionalized rules, clinic policies, EHR-use mandates, etc.—that structure physician identity in practice. Cheney and Tompkins (1987) similarly portray identification as inherently communicative and rhetorical, claiming employees use discourse to (dis)connect with various identity structures. Scott and Stephens (2009) demonstrate how identification, visible through language and interaction, can be fleeting, and mutable, contingent upon the activity at hand. Together, this scholarship attests to the ways that identity sets the groundwork for identification and identification iteratively evolves identity over time.
Identity Regionalization and Physicians’ Multiple Targets of Identification
“Place” functions as a discursive resource for identity in that it significantly frames and organizes identity construction (Larson & Pearson, 2012). Giddens (1984) argued that space and time provide unique contexts that shape expectations, behavioral patterns, and communication. His notion of regionalization suggests that social space is differentiated into regions—settings in which distinct configurations of rules, norms, and resources structure action.
Building on this foundation, the SMI theorizes that identity has regions (Scott et al., 1998). Identity regions consist of grouped identity structures (rules/resources) that are temporally and spatially differentiated where identity is constituted (e.g., in my child’s room when my child is home, my identity as “mom” is activated). Identity regionalization reflects the ongoing (re)structuring of social relations and negotiation of identity boundaries. Regions can encompass different types of identity social discourse, include identification with multiple targets, and vary in size, tenure, position, front/back stage positioning, and degree of overlap (Endacott & Leonardi, 2020; Scott et al., 1998), all of which may intensify or constrain identity conflict.
Description of Identities Relevant to Organizational Life
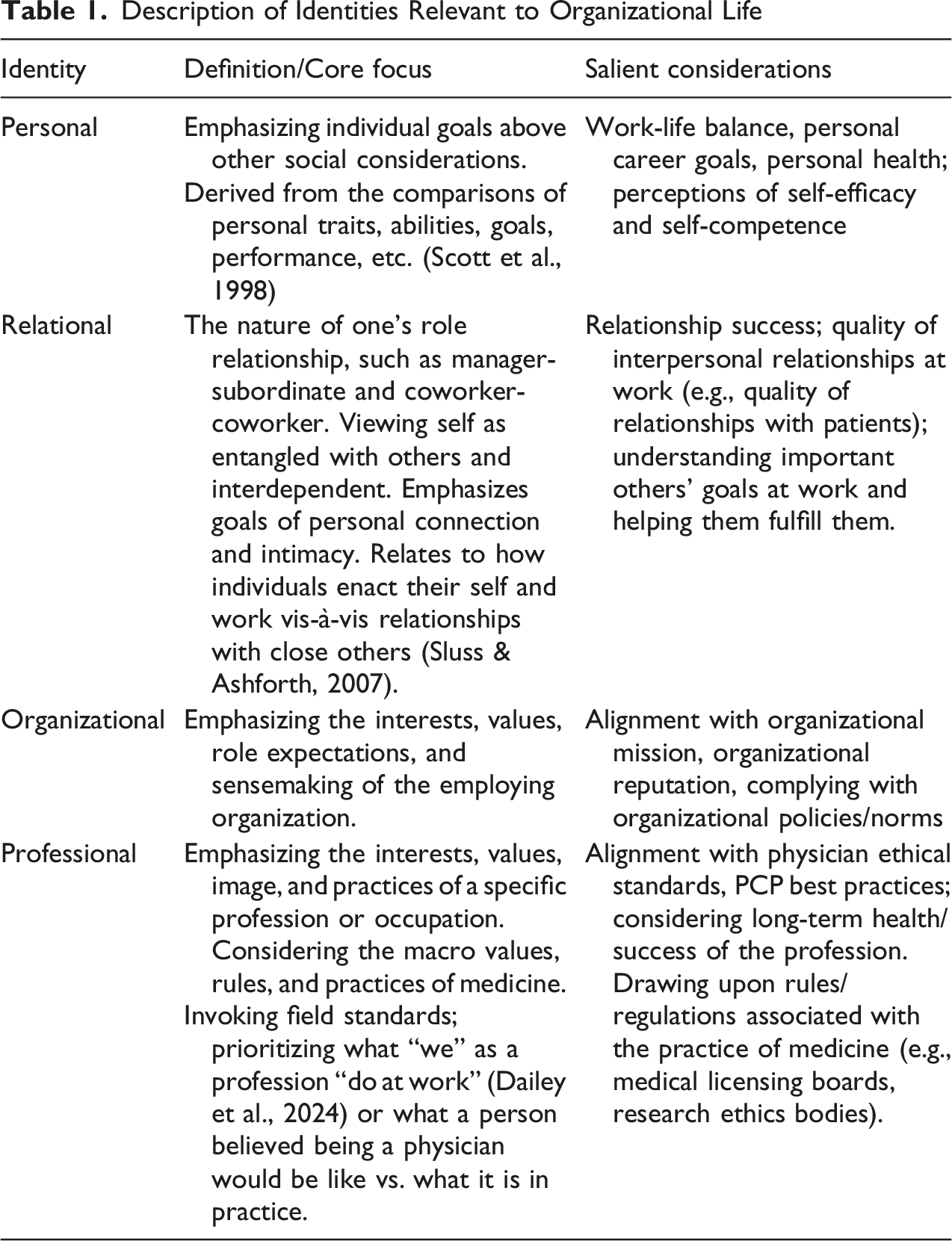
Thus, the ongoing practice of identity regionalization is particularly active for resident PCPs in the clinic office. Within exam rooms, PCPs report pursuing the roles of parent, friend, and advocate (Pratt et al., 2006), interweaving the identity rules and resources that they draw upon and reflecting partially compatible and conflicting identities (Cheney & Tompkins, 1987). Professional PCP identity is grounded in both the science and art of care. PCPs must follow technical policies and use advanced technologies to improve care and reduce medical errors (Soriano et al., 2017), reflecting the “science” of care, while many enter healthcare because they associate the profession with compassion and helping others—the “art” of care (Cochrane et al., 2019; Latimer, 2020). A physician's relational identity in practice can overlap or be embedded within the art of care, and thus their professional PCP identity. However, tensions can arise when professional physician structures privilege technical efficiency over relational connection with patients, creating (a) intra-professional identity tensions and (b) difficulty for PCPs to simultaneously enact their professional and relational identity. In some cases, strong relational commitments may lead physicians to disidentify with institutionalized forms of practice (Elsbach, 2001; Kreiner & Ashforth, 2004). Furthermore, these tensions may be intensified when caring for underserved patients, as their diverse social and cultural needs can add complexity to office visits (Chan et al., 2019).
Situated Activity: The 15-min PCP Office Visit
For Giddens (1984), regions reflect differentiated parts of space/time where routine activities and social practices are instantiated and reproduced. Activities—tasks, routines, and forms of day-to-day social life—are the central characteristics of regions, as they define and demonstrate how particular resources are drawn upon and displayed. Similarly, Scott et al. (1998) suggest that identification within regions is situational; it occurs “in the moment” and comes alive through communicative interaction and routine/fundamental activities. It is dependent upon both communication interactants and the communication situation (Stephens & Dailey, 2012). Thus, workers’ identification could vary based on the work room they are in (and the activities associated with that room), who they are engaging with, the history of that relationship, etc.
PCPs are patients’ first point-of-care to receive preventative and general healthcare (Shi & Singh, 2015), which often includes annual checkups, acute care, and continuous care within clinic offices. Thus, the clinic office visit is a fundamental PCP activity that offers a dynamic context in which to analyze the reciprocal nature of identity and identification. As evidenced, PCPs operate under larger rules that set formal parameters for visits, yet, they also iteratively integrate their own personality, (non)verbal communication style, and decision-making into patient visits, reflecting their agentic power to form emergent identity (Gilpin & Miller, 2013).
Importantly, the context surrounding the PCP office visit has shifted (Matulis et al., 2019; Young et al., 2018). Medicare and private insurance companies have changed reimbursements from a fee-for-service payment scheme to one that essentially pays physicians by number of patients seen (Zelman et al., 2014), prompting healthcare systems to increase the number of patients that physicians must see per day and reduce visit time to a goal of 15-min (Byyny, 2023; Linzer et al., 2000). Simultaneously, advances in medicine have increased the complexity of clinical issues addressed during office visits (Linzer et al., 2000). Thus, the office visit represents a situated activity that is both routine and ripe for PCP identity conflict, particularly when caring for underserved patient populations who often require more time (see Fiscella & Epstein, 2008).
Constraints to Caring for Underserved Patients
As previously noted, underserved patients experience heightened healthcare constraints and complex needs (Berkman et al., 2010). They are more likely to be uninsured, have limited English proficiency, face restricted access to healthcare services, and have lower income and/or education (Bradley et al., 2007). Literacy and health literacy challenges are also disproportionately concentrated within this population (Hahn & Cella, 2003), making it more difficult to grasp provider instructions and comprehend complex care routines (Rothman et al., 2009). Additionally, underserved patients may harbor a general distrust toward healthcare systems (LaViest et al., 2009). Despite these challenges, underserved patients often require greater relational engagement—such as clear, step-by-step explanations, careful attention to nonverbal cues, and nonjudgmental clinical spaces (Raja et al., 2015). Thus, caring for underserved patients during time-limited office visits can carry unique constraints that intensify PCP identity conflicts. Previous research has yet to reveal how the enactment of PCPs’ identities during residency (a) is a response to underserved patients’ unique communication needs, and (b) involves fluid identifications with multiple, competing identity structures. Thus, the first two RQs ask:
Repositioning and Reprioritizing Identity
Examining identity-centered constraints also raises questions as to how resident PCPs respond to incompatible identities in practice. Individuals may manage incompatible identities by buffering or separating identities, suppressing one or more identities, redefining identity expectations, and/or deferring to the most salient identity (Ashforth et al., 2008). Organizational communication scholars also highlight how workers may engage in disidentifications, or efforts to discursively distance themselves from identities in organizational life that source dissonance (Elsbach, 2001; Ploeger & Bisel, 2013). From a structurational perspective, workers may reposition identity—or reshape how an identity is understood and/or reprioritize identities to more productively align with specific contextual goals (Scott et al., 1998). How workers (re)position their identities determines the rules and resources they draw upon, shapes their work perspectives, and enables different levels of adaptability in completing work tasks (Endacott & Leonardi, 2020).
Relatedly, Pratt et al. (2006) show how physicians experiencing work-identity integrity violations during residency responded by actively engaging in identity customization processes to better align their identity with task demands. Building on this, physicians may also employ work customization processes—or work appropriation—to reconcile identity tension. Appropriation entails workers autonomously interpreting and engaging with organizational structures (e.g., rules and resources) and then embedding those decisions into ongoing organizational practice (Poole & DeSanctis, 1990). Management scholars have similarly studied how job crafting and role innovation can resolve identity conflicts and sustain valued identities (Horton & Wanderley, 2023; Wrzesniewski & Dutton, 2001). Although prior research suggests appropriation reflects problem-solving behaviors that can encourage positive deviance (Ashforth et al., 2008), we still lack a richer, more granular understanding of how and why people appropriate their work and reposition identities to manage specific, multi-level identity conflicts.
Context also matters. Integrative identity research reviews emphasize how identity conflict is shaped by situational demands, yet context is largely understudied in interdisciplinary identity research (Horton et al., 2014). Recurring work activities—such as the PCP office visits—are the “central characteristics of contexts” in which situated identity is expressed (Scott et al., 1998, p. 322). Examining such activities can reveal how workers manage identity conflicts through identity (re)positioning and work appropriations. Thus, the last question guiding this study is posed:
Methods
Research Site and Design
This research was conducted at a Federally Qualified Health Center (FQHC) serving the residents of a county in Southwest Texas that live at or below 200% of Federal Poverty Guidelines. This FQHC, hereafter referred to as First-Rate Care, has a residency program that is ranked in the top 5% in the U.S. The average income of First-Rate Care patients was $9,000. Most patients fall into one or more underserved categories (Bradley et al., 2007). I completed 10 hours of training to become a formal research associate at First-Rate Care.
I interviewed resident PCPs and observed both residents and First-Rate Care patients during medical visits. Semi-structured interviews captured resident PCPs’ reflections on identity conflicts, while video observations revealed how identity was enacted in physician–patient interaction. Resident PCP interviews were conducted first to generate a codebook that would later inform observation analyses. Observing PCP-patient communication provided insight into additional physician identity conflict examples not described in PCP interviews.
Resident PCP Interviews
Research Participants
Of the 37 residents recruited at First-Rate Care, 27 participated in interviews, including 12 women (44%) and 15 men (56%) whose ages ranged from 27 to 40 years (M = 32.1). Participants identified as White (51.9%, n = 14), Hispanic/Latino/a (18.5%, n = 5), Asian (14.8%, n = 4), South Asian (7.4%, n = 2), Black (3.7%, n = 1), and American Indian/Alaska Native (3.7%, n = 1). Interviews, conducted via Zoom, ranged from 25.8 to 61.1 minutes long (M = 48.23), totaling 21.7 hours of data. Questions addressed work conflicts, work-home balance, and challenges and successes in caring for underserved patients (e.g., “Does who you are, or want to be, as a physician ever conflict with formal physician standards or rules. If so, how, and what do you do?”; “What are some challenges you have experienced caring for underserved patients?”). All interviews were audio-recorded, transcribed, and assigned pseudonyms to protect participant identity. Field notes were recorded during interviews to record key observations. The interview protocol and additional data materials are available in the Harvard Dataverse (https://doi.org/10.7910/DVN/BUSX28).
Data Collection Procedures for PCP Residents
First-Rate Care primary care residents were recruited through a purposive sampling method operated through referrals. I partnered with the First-Rate Care’s residency program director, research director, and faculty leaders to generate a recruitment plan for its 37 residents. Efforts were made to recruit residents across different years in their three-year residency and with varied backgrounds to strengthen study findings. The chief resident pitched the study at the annual resident meeting and collected interview and observation consent forms. The residency program director provided names of residents absent from the meeting, and I emailed them directly to solicit participation. Interviews occurred via Zoom during residents' lunch breaks, off-days, or after-work hours. I was assigned a First-Rate Care office and granted credentials to access video recordings on its servers. All video data were analyzed on site to uphold HIPAA regulations. Residents received a $50 gift card for interviews and a $50 gift card for observation participation. They were assured that their (non)participation would not affect their residency.
Step-by-Step Procedures of Interview Data Analysis
Interview data were analyzed using an iterative approach guided by Braun and Clarke’s (2006) six phases of thematic analysis. First, I transcribed interviews into written texts. I read each text multiple times to heighten familiarity with the data and then began open coding by broadly naming the data. Second, I adopted first cycle “initial” coding to create emic codes related to PCP barriers to caring for underserved patients and collapsed and condensed these codes (Saldaña, 2016, p. 100). For example, the comment “underserved patients…there’s a lot more trouble shooting… as far as like, finding them the resources. Maybe they can’t afford a medication,” was coded into the category “financial barrier.” A second round of initial coding produced formal, etic codes associated with SMI concepts (e.g., identity, (dis)identification, identity conflicts, professional identity). In later stages, I refined and collapsed SMI codes to create broader categories. For example, statements about EHR being “a really hard part of the job for me” were coded as “identity conflict” and categorized under “personal vs. professional identity”.
Third, I used a second-cycle, pattern coding (Saldaña, 2016) to identify emerging interactive relationships between resident PCP identity conflicts and how they then responded to these conflicts through identity repositioning and/or work appropriations. For example, the quote, “just like any other physician, I’m subject to compassion fatigue at work. I struggle with that… [so] we adopt a dark sense of humor…that’s just how we deal with it here” illustrates how a resident PCP navigated a personal vs. professional identity tension by repositioning identity. He downplayed and recast problematic aspects of his professional identity (compassion fatigue) by prioritizing his organizational identity (i.e., using dark humor is “how we deal with it here”).
Fourth, I reviewed the codes and themes. Interview data reached saturation during the 25th interview, meaning (a) no new identity-centered constraints emerged in the text, (b) no new types of conflict-appropriation relationships emerging during second-cycle coding; and (c) the codebook stabilized, indicated by an absence of new code applications or substantive revisions to code definition. This reflected previous research suggesting data saturation and redundancy for in-depth interview studies starts to manifest around 25 to 30 interviews (Dworkin, 2012).
Fifth, I refined and defined each code and theme. To enhance thoroughness and transparency, I collaborated with a research associate to evolve the codebook. After training the associate, we reviewed five interviews per week, meeting regularly to compare coding, resolve discrepancies through direct reference to the transcripts, and revise the codebook accordingly. We then independently coded the final 12 interviews, achieving 89% agreement on initial codes. The final codebook included 105 open codes, which were collapsed into 39 initial codes, 14 broader categories, and five pattern codes/themes. In Braun and Clarke’s (2006) sixth phase, I selected vivid examples of each theme and linked the findings back to the research questions in the final report.
Video Observations of Office Visits
Research Participants
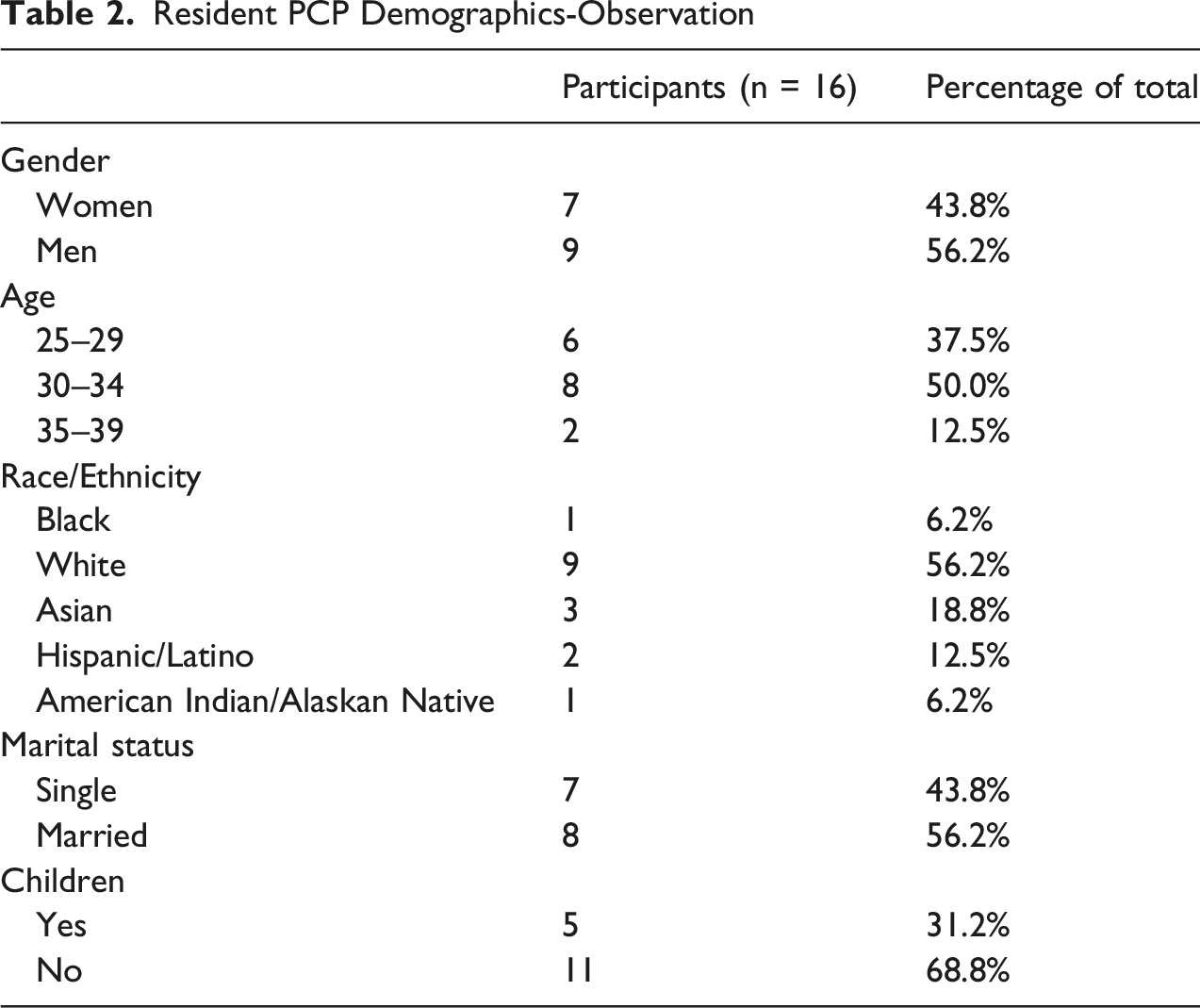
Resident PCP Demographics-Observation
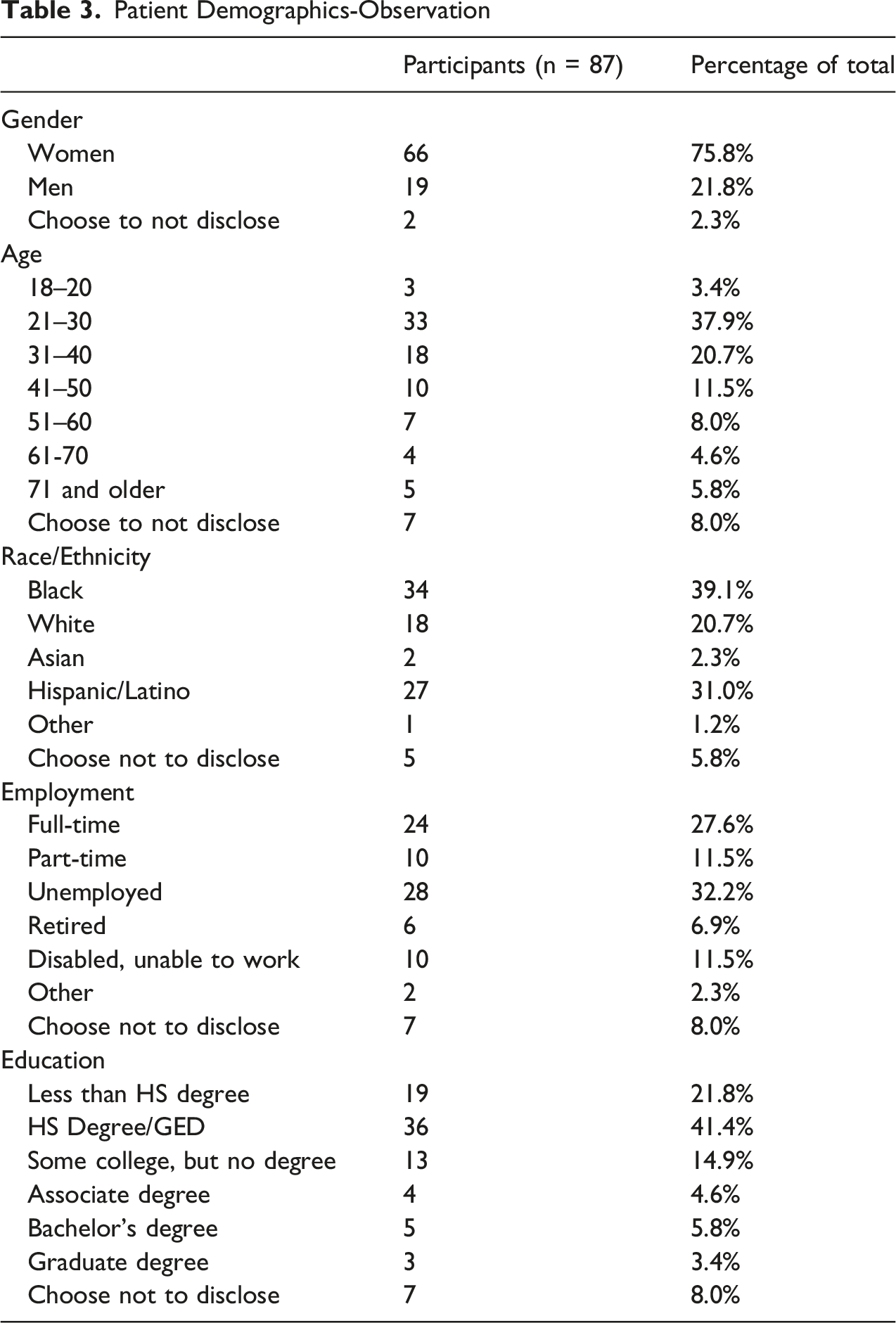
Patient Demographics-Observation
Data Collection Procedures
First-Rate Care resident PCPs were recruited for interviews and observations through the same methods. Thus, residents were recruited through a purposive sampling method operated through referrals, in which I partnered with the First-Rate Care’s residency program director, research director, and faculty leaders to generate a recruitment plan for its 37 residents.
Patients were recruited through convenience sampling based on clinic data collection days. Each morning, the research team—comprised of myself and a group of undergraduate and graduate students—discussed the research and consent processes with the First-Rate Care nurses working in the clinic’s four waiting areas. I kept and maintained a master list of residents who had previously consented to observations and worked with the consenting PCPs to identify patients eligible for recruitment (e.g., serious mental health patients or female patients undergoing sensitive physical exams were excluded).
Afterwards, the research team recruited patients in the clinic waiting areas. Nurses provided us with an official patient schedule (including patient names and visit times) so we could identify the patients the residents had screened for recruitment. In total, 116 patient names were on the recruitment list throughout the duration of the study. The research team then actively recruited these patients each day. Researchers gave a pink piece of paper to consenting patients, indicating to nurses that the patient should be placed in a video-enabled room. I partnered with First-Rate Care to ensure the consent forms read at a 5th grade reading level and clearly understood by patients. Patients were assured that their (non)participation would not affect their medical care. A University Institutional Review Board and the First-Rate Care’s Research Ethics Committee approved this study. Patients received a $15 gift card for participation in observations.
Step-by-Step Procedures of Observation Data Analysis
After I coded interviews, I began observation analysis. Integrating both data analysis sources allowed me to (a) visualize identity struggles not articulated in interviews, and (b) use interview findings to guide focused observations (Pomerantz et al., 1997). For instance, because many interviewees described identity struggles as situated within the material set up of the exam room, I observed how room configuration (e.g., computer or chair placement) shaped resident PCPs’ verbal and nonverbal communication with patients. After observing five patient visits, I developed a structured coding worksheet to guide subsequent analysis. This worksheet included columns for (a) physician and patient demographics and (b) the frequency, type, and content of disclosures and questions by both parties, along with transcribed segments of video related to PCP identity. Depending on the frequency and complexity of disclosures and questions documented, coding for a single observed visit could range from one to one-and-a-half worksheet pages. This process produced 96 worksheet pages and 78 pages of transcribed video data.
Identity Conflict Codebook
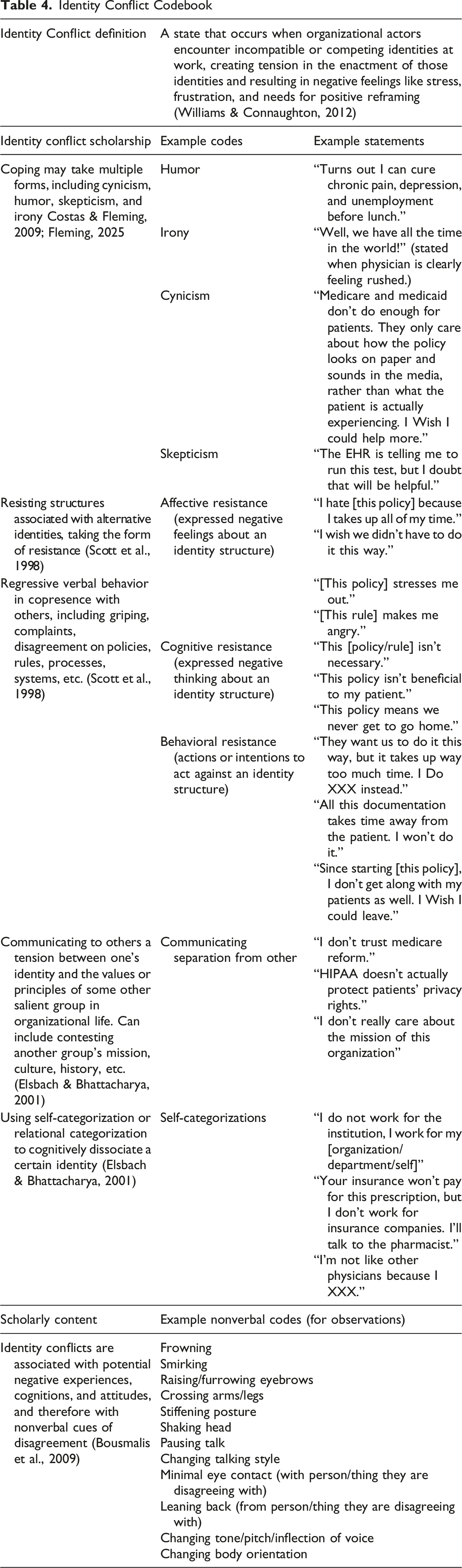
During second-cycle, pattern coding (Saldaña, 2016), I linked (a) PCP identity conflicts and care challenges with (b) work/identity appropriations. Continuing the example, when a PCP noticed a patient’s attention was negatively affected by indirect nonverbal communication, the PCP may adjust the room’s materiality to re-engage the patient. Data saturation occurred around the 83rd and 84th unique patient visit, as identity themes became redundant, yielding no new insights (Saunders et al., 2018). Because video observation is labor intensive and cognitively demanding (Asan & Montague, 2014), I stopped data collection at 87 unique medical visits.
Findings
Findings show how resident PCPs’ everyday responses to identity tensions do more than resolve momentary conflicts—they gradually reshape how care is organized and practiced. Care appropriations were a routine, generative feature of office visits. Figure 1 synthesizes interview and observational evidence to depict how the constraints identified in RQ1 precipitate identity conflicts (RQ2) The structurational model of identity conflicts Evidencing the Identity Conflict Model Through a Personal vs. Professional Identity Conflict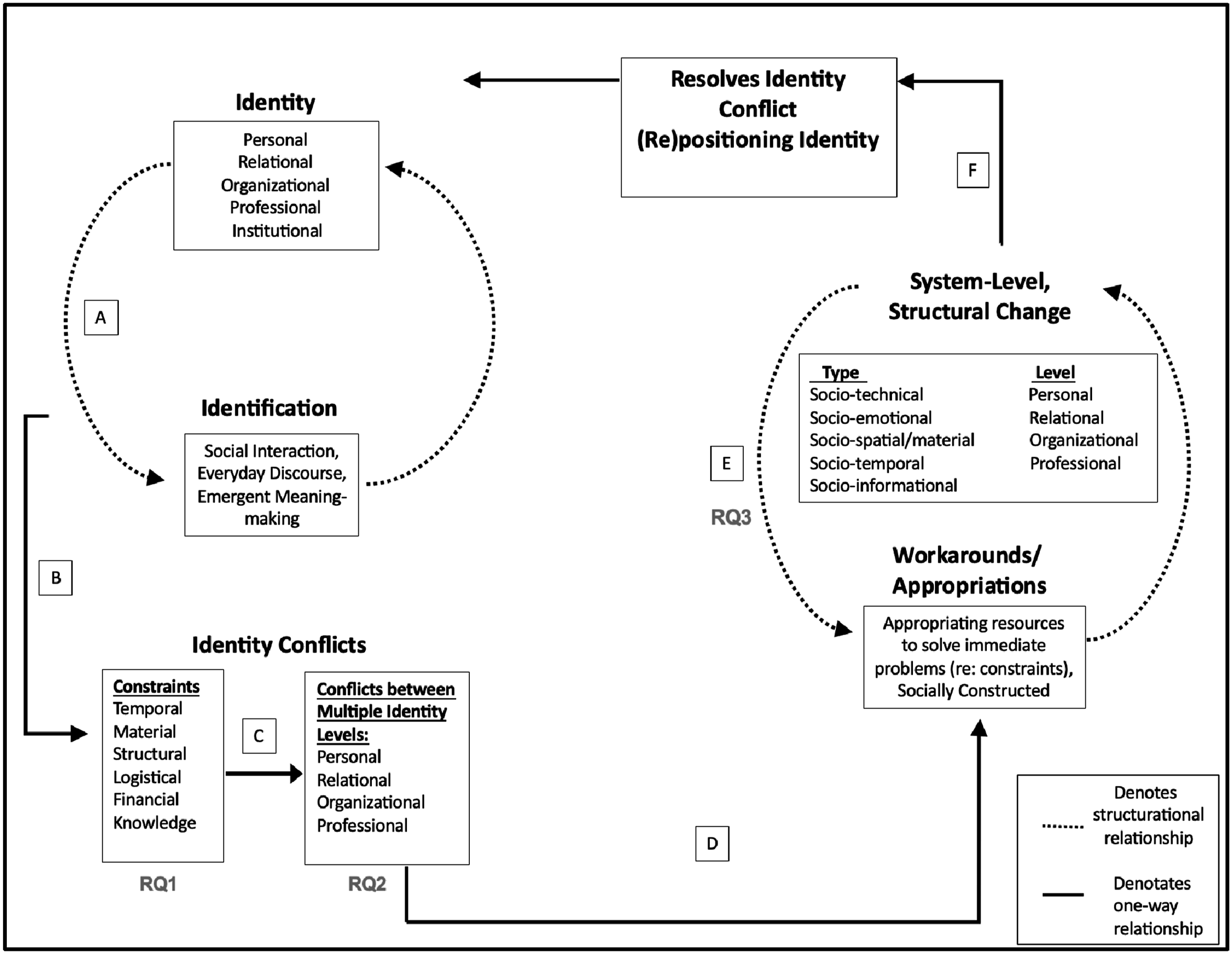
RQ1: Constraints to Caring for Underserved Patients During Office Visits
RQ1 Results: Taxonomy of Physician Identity Constraints When Caring for Underserved Patients
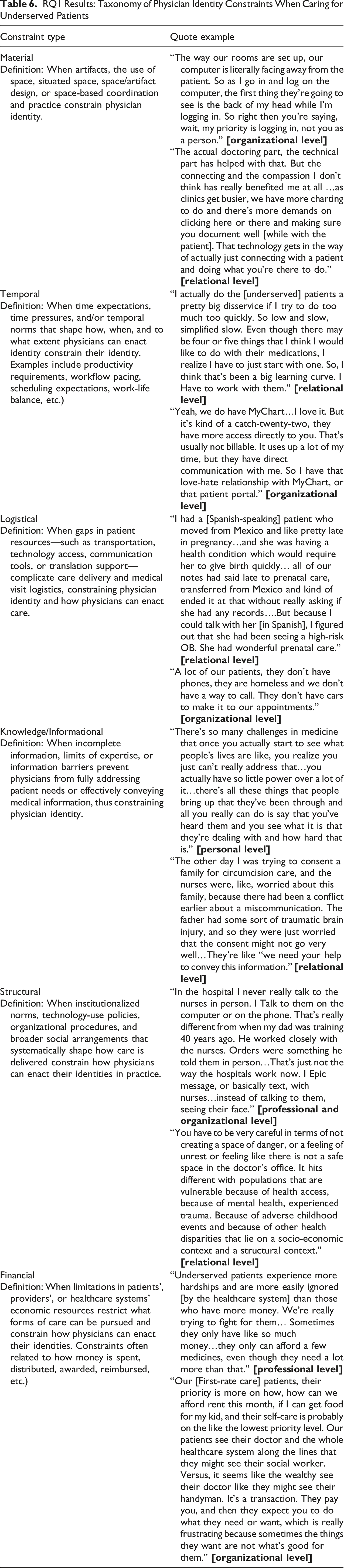
Constraints were not mutually exclusive. For example, time-intensive electronic health record (EHR) templates reflected both temporal and structural constraints. Identity levels were also not mutually exclusive. EHR use mandates interfering with unique patient connections exemplified a structural constraint operating at the relational and professional levels, leading to a relational vs. professional identity conflict. Because this paper centers on resident PCPs’ identity-centered constraints when caring for underserved patients, analyses largely focus on identity incompatibility, though identity compatibility also emerged in the study findings.
Importantly, residents often noted how constraints experienced during the 15-min visit were a result of the intensified challenges experienced by their underserved patients (e.g., illiteracy, racial and language disparities, domestic abuse). Dr. Jones exemplifies below: Meeting the patient where they are because of their education level in context of exposure to the healthcare system… are big points of compassion. If patients don't know what's going on or don't understand how to communicate like how people who had a middle-class upbringing can communicate… [it] can lead to very dangerous things that are happening to their child… or not treating very manageable things. But they just haven't had that contact with the healthcare system to know how to journey with your physician to address this… it requires more cognitive effort on my part as a physician, more time, and more patient education. And it's hard because you have less frequent contact for underserved patients and so you're doing the work of… multiple visits in one visit and in a 15- minute slot.
As Dr. Jones notes, caring for underserved patients often required residents to compress the work of multiple visits into a single 15-min encounter, intensifying tensions between efficiency demands and compassionate, patient-centered care.
RQ2: Competing Identity Structures and Identifications During Office Visits
When resident PCPs’ reciprocal process of drawing on identity structures to enact identity (path A, Figure 1) encountered constraints (path B), multi-level identity conflicts occurred (path C). Though space does not permit evidencing every type of multi-level identity conflict found in the data, below I exemplify the four most frequent tensions between PCPs’ salient workplace identities.
Professional vs. Organizational Identity Conflicts
Resident PCPs, like Dr. Stein below, often discursively constructed a distance between professional PCP identity goals and the routines that structured their organizational PCP identity: “Medicare's reimbursement policies are not patient-centric at all. They seem to not care or really even notice patients’ health outcomes. They care about some bill that was passed… which means that's going to affect what I do in the exam room… At [First-Rate Care], we [now] these Medicare wellness visits that are done with nurses that mean absolutely nothing… The patient thinks that they're an important thing, but they're not. Doctors, we never look at the notes… They have absolutely no bearing on our patient relationship or plan for the patient. We just do them to satisfy Medicare so that we can keep getting paid for seeing the patient… The structural problems [of Medicare]… are the bigger issue… it’s not what I imagined… my stethoscope in my ears, my hands on the patient for 30 minutes or something. That’s what I imagined doctoring would look like.”
Here, a structural constraint emerges as Dr. Stein describes how Medicare reimbursement policies constrain the PCP profession. Professional identity is shaped by profession-wide norms, expertise, ethics, and participation in a professional community (Lammers & Garcia, 2009). For Stein, PCP professional identity should be enacted through patient-centric policies and clinically meaningful visits. However, Medicare mandates—formalized through legislation and operating beyond any single organization—required visits that, in his view, did not enhance clinical quality. He explained that these visits “did not serve a diagnostic purpose,” often “left patients frustrated,” and consumed organizational resources without tangible patient benefit. Another physician similarly described them as “robotic,” noting, “you kind of feel more like you have to follow them.”
Although Medicare exists outside First-Rate’s direct control, it shapes organizational routines and identification (Lammers & Garcia, 2009). The clinic’s compliance with Medicare wellness visit requirements prioritized billing and visit metrics, signaling an organizational identity rooted in revenue and numbers. As Lammers and Garcia (2009) found in call centers, productivity mandates can conflict with professional standards for careful work. Similarly, Medicare-driven organizational practices clashed with PCPs’ patient-centered professional commitments, producing organizational vs. professional identity conflicts. In his quote Stein engages in disidentification (Costas & Fleming, 2009), discursively distancing himself from the organizational routines he believes undermine PCP professional ethics and quality care. Thus, Medicare is an extra-organizational institution that shapes routines and rewards in ways that can produce conflicts for physicians on the professional vs organizational level.
Professional/Organizational vs. Relational Identity Conflicts
Identity conflicts were also sourced from EHR protocols embedded within resident PCPs’ professional identity conflicting with the enactment of their relational identity. Dr. Jen explains: I have struggled in the past when I'm in the room with the patient, how much time do I spend looking at the screen, cause it can be helpful, right? Like sending in the patients’ medications, putting in orders, pulling up past history… In other situations, it just distracts from the connection that you're trying to make with the patient. Sometimes I get the sense that they think I'm ignoring what they're saying… I hate that…that can be very difficult… it interrupts the flow of the conversation. And I just struggle with the direction of the computer, where the patient is sitting, how much time I am spending with my back to them, especially if they’re underserved and already feel like they’re not heard.
Dr. Jen is encountering a structural and material constraint operating at professional and relational identity levels. EHR use during patient visits has become standardized practice, reshaping physicians’ work and patient communication and, in turn, reconfiguring professional identity (Boonstra et al., 2022). Professionals incorporate rules and resources into their identities when legitimized by the professional community (Lammers & Garcia, 2009). Today, EHRs are embedded in medical education, certification and quality metrics, professional association standards, and everyday clinical routines (Fife et al., 2013; Hong et al., 2022). Thus, EHRs have become a legitimate component of the medical profession’s knowledge and practice.
Although Jen acknowledges EHR use benefits and accepts them as a professional norm, she describes how EHR routines constrain her relational physician identity by limiting interdependence and personal connection with patients. EHR use requires sustained screen attention, reducing the verbal and nonverbal immediacy (e.g., eye contact, conversational flow) that constitutes attentive care and is especially important for underserved patients. She highlights the EHR’s materiality, noting how the physical exam-room setup shapes how she enacts relational care. Statements such as “I hate that” index identity tension, as EHR materials restrict her ability to orient her body and gestures toward patients. The resulting spatial arrangement increases perceptions of interpersonal distance and limits direct engagement. Thus, the EHR operates not as a neutral tool but as a socio-spatial norm that constrains Dr. Jen’s relational physician identity.
Importantly, this constraint is contingent upon organizational environment and built space, signaling both professional- and organizational–relational identity conflicts. Exam rooms vary widely, and some clinics use mobile workstations that allow clinicians to reposition computers during visits. At First-Rate Care, however, the workstation was fixed on a wall opposite the exam table. This material arrangement organized space, body orientation, eye contact, and gestures in ways that hindered relational connection. EHR use, then, emerged as both a professional and organizational constraint on Dr. Jen’s relational physician identity.
Observing five of Dr. Jen’s patient visits quickly revealed her relational physician identity was highly important. She intently used open-hand gestures, casual posture, body orientation, validating statements and positive reinforcement to elicit sensitive disclosures from her patients, including household abuse, possible HIV diagnoses, absent fathers, and post-partum depression.
Similarly, Dr. Bracken also navigated professional vs. relational identity conflicts at work, yet they were sourced from temporal barriers to offering underserved patients care: I took care of a young single mom yesterday who was in an abusive relationship for four years and moved to get away from this guy. She was raising a one-year-old. She has severe depression now and anxiety… [in this profession], I have to address those things… with medication and counseling. But I'm like, I'm pretty confident if you were good friends with my wife and her girlfriends when you had this baby, you'd be in a whole different place… Really good care for you means you need community and friends and, I can't really offer that to you in a 15-minute office visit. That's probably what I feel the most with our [underserved] patient population. Just feeling I wish we could be their friend, especially when I meet younger patients and I'm starting to see the trajectory of their lives.
For Dr. Bracken, the rules and resources structuring his professional PCP identity constrained his time to 15-min visits and the resources he could formally draw upon to medication and counseling. As Lammers & Barbour (2006) argue, institutions formalize rational practices (e.g., time-limits, documented procedures) that guide and constrain professional identity. In contrast, Bracken’s relational PCP identity centered on community and unique “patient-specific” relationships. He noted, “the most beautiful level of care is seeing each moment as a moment to listen… to be attuned to what else could be going on… seeing each patient as an opportunity to connect.” His relational PCP identification was evidenced during a visit with a Hispanic woman in her 60s. Dr. Bracken eagerly asked to see a picture the patient’s granddaughter drew for her, exclaiming, “I love it!” They shared many laughs. While listening to her heart, he joked “this is serious business…no laughing…that’s always what I say to make my kids laugh!” Yet, his patient-specific connections often generated a desire to offer support beyond clinical boundaries, as reflected in his block quote. His desire to further enact relational connection was impeded by professional logics.
Professional vs. Personal Identity Conflicts
Other resident PCPs’ identity conflicts were grounded in how institutional rules that governed their professional identities impeded their personal desires and calls to help underserved patients. Dr. Chen felt personally constrained as a PCP by U.S. healthcare insurance policies: Underserved patients experience more hardships and are more easily ignored than those who have more money… One patient, who is in his 20s, it’s a really sad case… he was basically normal up until he was in his teens when he got a viral infection and then a really bad autoimmune response [that left him] paralyzed from his waist down… His paralysis has been going up towards his arms [and] his mouth… He is an undocumented immigrant… That prevented him from being qualified for various insurance… that illustrates the financial difficulties of wanting to feel like you are compassionate, you personally want to do the good things for your deserving patients. But sometimes, the resources aren't available… And his poor mom, it's not the life that he expected… or that she expected for her child. I couldn’t help them… and that was hard for me personally.
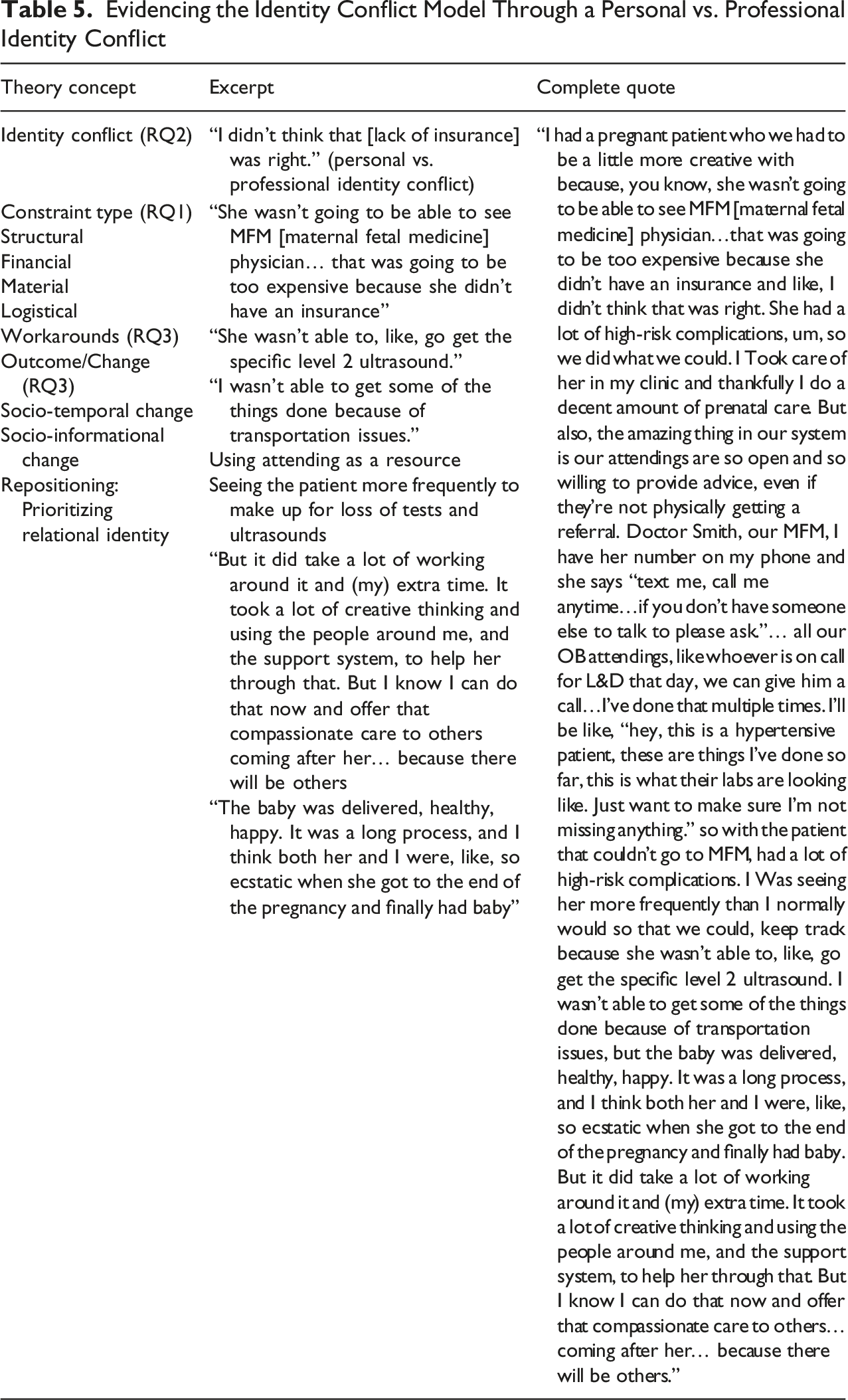
Dr. Chen describes a structural and financial constraint shaping care for underserved patients at both the professional and personal levels. She explains that her self-efficacy as a PCP is constrained by external regulatory agencies and professional bodies (i.e., insurance) that govern her profession, yet further disadvantage underserved patients (Lammers & Garcia, 2009). These same institutional structures grant medicine its professional authority, illustrating how professions both empower and restrict practitioners (Lammers & Garcia, 2009). PCPs operate within a constellation of field-level rules that influence their daily choices and abilities, constraining their enactment of work (Lammers & Barbour, 2006). Chen personally identifies with this patient and his mother and desires autonomy from enacting insurance policies that obstruct her ability to show compassion to them. However, her personal PCP identity is complicated by insurance policies, which generate a multi-level identity conflict. Table 5 offers another example of a resident PCP experiencing a personal vs. professional identity conflict centered on insurance policies.
Personal vs. Relational Identity Conflicts
Personal and relational identity are inherently tied to one another. Ricoeur (1992) argued personal identity is inextricably bound to the concept of the other and the relation between the self and others, which may suggest that resident PCPs’ personal and relational identities are compatible. However, identity tensions of this nature often surfaced in the current data, in that resident PCPs’ concept of self conflicted with their ability to enact relational depth and intimacy with patients. Below, Dr. Jones explains how her identity as a PCP is entrenched in the construction of compassionate and empowering patient relationships: I’m always thinking about understanding the narrative from a patient standpoint, understanding the unique challenges and unique strengths of each patient when it comes to facing their unique [health] obstacles… being able to partner with patients… to come alongside them, understand them, to move forward in their healthcare.
Given Dr. Jones was also the only Black resident at First-Rate Care, she felt uniquely equipped to care for patients of color (POC). Yet, this personal identity anchor did not always reinforce her PCP relational identity with POC: I'm repeating word-for-word what they [POC] were saying, and I thought I understood their experience and was communicating that… [but] they thought they weren't being heard or listened to. And that was really frustrating for me because especially as a physician of color, part of the ways that I use, show compassion is to use personal experience with a lot of my patients of color… And with this patient, it was a patient who was African American, and being a Black person myself… there’s a lot of aspects of culture that I consider that this is my people… [but] I had a breakdown in communication… There was a breakdown in experienced compassion… [but] I was using all my tricks in the toolbox to connect.
Dr. Jones is experiencing a knowledge constraint to caring for POC that is operating on the personal and relational levels. The overlap between Dr. Jones’ personal (e.g., racial/cultural) and relational identity regions in her exam room ordinarily gives her access to a rich set of identity resources—shared cultural knowledge, experiential understanding, and moral commitments—that she routinely draws upon to care for POC. Yet, in this case, she expresses not having enough or the right type of information. She personally identifies with POC, claiming, “this is my people” and “being a Black person myself,” which should lead to positive relational identifications/enacted connections with POC; yet her patient’s response resulted in a disrupted identification episode, generating a personal (e.g., racial/cultural) vs. relational PCP identity tension. The rules and resources she drew upon on a personal identity level (e.g., using personal experiences to show understanding) did not empower or develop trust with this POC—a type of relational identification important to Dr. Jones in her workplace. Jones responds, “that was really frustrating for me.”
During observations, Jones routinely demonstrated her ability to relationally connect with POC. For example, A 38-year-old Black female patient, complaining of chest pains, explained: I’ve been through a lot… my house has been shot up three times. They was trying to kill my son… I’m worried about people finding out where I stay and doing it again… I’ve had to move into another house that I can’t afford… I won’t ever be able to get the fear out of my head, no matter the counselors or medications they put me on.
Dr. Jones completely stopped what she was doing to look directly into the patient’s eyes and say: You know, there are many people in this community struggling with different things, so I want you to feel like you’re not alone with what you are going through here. The reason why we check up on you and call you or offering counseling is for you to find places of safety and to make sure we can work through some of these symptoms… so, I am very, very appreciative of you sharing things that can be hard or bring shame.
The patient responded, “I really like you… I really wanted a woman doctor to begin with, a black woman doctor… that’s important to me.” Dr. Jones smiled and nodded. The patient continued, “I always wanted someone who could understand me. These [White] men, they’re OK [but] they don’t have kids. They don’t understand… They don’t know what we go through.” On the word “we,” the patient motioned with her hand between her and Jones’ chest. Jones responded, “We are a team.” Given Jones’s consistent (non)verbal efforts to empathize with POC and their community challenges, it is clear why identity conflict emerged when her personal, cultural identity did not strengthen her relationships with POC during the medical visit.
RQ3: Identity Conflicts Lead to Care Appropriations and Structurational Change
Types of Structurational Change
Professional and Organizational Identity Constraints Lead to Appropriating Technology
As mentioned, EHR use during patient visits has become a standardized, macro-level PCP practice that has considerably (re)shaped PCP professional identity (Boonstra et al., 2022). In RQ1, PCPs explained how new routines and demands linked to in-visit EHR use constrained their ability to uniquely care for underserved patients. Building on this, RQ2 results then show how PCPs appropriated EHR-use rules to prioritize their relational identity. Dr. Begay elucidates: I really, really don't like the EHR. I think it is a waste of the doctor's time, and I think it gets in the way of… good, compassionate patient care… Honestly, most of our charts have nothing at all to do with patient care… it is to try not to get sued, which is a big bummer… Our attendings all the time are like, “if a lawyer sees that you put this patient on this medicine, but didn't write this down, you could lose your license”… So the reason I don't do it [EHR documentation] in the room is because most of the stuff I put in there is not relevant… to my relationship with the patient… it’s about the depersonalization of medicine… The reason I went into family medicine is that I like people, and a whole lot of my job right now is computers, instead of people… We [first-year residents] only see six or seven patients a day. Next year when we see 10, we may have to do it differently.
Dr. Begay is experiencing structural and temporal constraints to care, creating a conflict between his professional and relational PCP identities. He explains how EHR documentation requirements center on legal liabilities and structurally discourage time spent with patients, reflecting his weakened professional identification. Dr. Stein, who also stopped EHR documentation during patient visits, showed similar weakened professional identifications, such as “I feel like I’m an electronic paper pusher in the hospital instead of a caring physician.” To manage this multi-level identity conflict, Begay has started to routinely work around EHR use during office visits altogether (i.e., professional physician targets) so that he can prioritize compassion and connection time with his patients (i.e., relational physician targets). Dr. Begay is therefore reprioritizing relational PCP identification targets, and distancing himself from professional identity structures (i.e., EHR norms) (Larson & Pepper, 2003). Moreover, this appropriation has become reproduced to the extent that it has created structural change at the relational level (path E). According to Dr. Begay, most first-year PCP residents are not engaging in EHR documentation during visits.
Dr. Henry also notes how EHR structures created obstacles for his relational PCP identification. Yet, for him, EHR use structured activity at the organizational level, resulting in an organizational vs. relational identity conflict: I deviate a little bit from standard template stuff because it drives me bonkers… they are curated from a central site, the central work team at First-Rate Care… I’m about as far polar opposite from a notes style from the folks who make the templates. I hate everything about that note… so I’ll just make my own [templates]… Mine are pretty sparse in terms of the content that’s required… It helps me give more of my time to my [underserved] patients who have many needs… they don’t want to see the person they talk to typing on a computer… you have to sit with them in the midst of whatever it is that they’re going through… I don’t know if you can sit with somebody in something and actually be with them if you don’t actually want to have a relationship, which is impeded by the pace of medical practice, which has changed a lot with EHRs. It’s [now] far more common that… you don’t feel like you have time to sit and be with someone.
For Dr. Henry, the EHR use structures (i.e., templates) creating tension operated at the organization level in that the templates were created by the central work team at First-Rate Care. Thus, Henry’s quote, which expresses his “hate” for the standardized note, reflects organizational disidentification (Kreiner & Ashforth, 2004). He appropriates patient care by creating his own templates that are not as “cumbersome” (path D in Figure 1). Notably, First-Rate Care housed an applied clinical informatics fellowship in which fellows met regularly with residents to discuss EHR concerns and translate these conversations into customized EHR modifications. As a result, agentic actions like Dr. Henry’s generated socio-technical and socio-informational changes at both relational (patient–provider) and organizational levels (path E), reshaping how PCPs understood their identities and enabling them to better meet contextual demands (path F; Scott et al., 1998).
Professional Identity Constraints Lead to Appropriating Time
PCPs’ ability to care for patients with emotional needs was often constrained by the 15-min office visit norm, reflecting a temporal constraint that created identity conflict. More experienced PCPs learned to appropriate temporal workplace structures to provide compassion, thus managing multiple identities. Dr. Gonzalez exemplifies: If it's a busy clinic day… that means that patients are waiting… but if it's important enough to spend the extra time, like with someone who just had a miscarriage, I'll take the time. This is something I developed as I got more comfortable… probably six months into intern year… I learned it from my attending… Say there's three patients waiting after I just spent an extra 20 minutes in a room… I’ll pop in [to the waiting room] and be like… “hey, it's going to be 30 minutes. Is that OK?” So, they’re not waiting for an hour, like, is the doctor ever going to come see me?… It really works out when you have quicker visits, like if I have a well-child check afterward. I can better serve all my patients.
This workaround enabled Dr. Gonzalez to create time to connect with patients in need, while upholding professional norms of honesty and time efficiency. She used this strategy across patients and first learned it from her attending, showing how appropriation enacted socio-temporal change at the relational and organizational levels (path E).
Similarly, Dr. Win described how she strived to pray with patients and make them feel loved. To achieve this, she was working to “get faster,” reflecting her efforts to appropriate time: A lot of patients have really appreciated prayer, especially end of life things… or just scary things. Doctor Che [her attending] really surprised me because she is different. She has a commitment to herself to pray with every patient… And I remember watching her, and there was one patient with high blood pressure. And I'm like… this person's just a routine high blood visit, but… it just meant so much to the patient… She was a really good role model for me… as I get faster, hopefully I will have more time and space to do that [prayer].
When asked what it meant to “get faster,” Dr. Win explained: If we have like 15 patients and half a day then that can be kind of a juggling act… part of getting faster is learning how to help the patient share what's most important for them to talk about and then partnering with them so that we agree on what we're going to do in the next 15 minutes so that they still feel heard and loved.
Dr. Win’s quotes reveal how triaging patients’ health needs and encouraging patients to quickly prioritize their most pressing concerns enabled her to work around temporal constraints generating professional vs. relational identity conflicts. During residency, PCPs learn to “get faster” reflecting a shared time appropriation that is reproduced to enact socio-temporal change. Win, like all PCP residents—regardless of organization, rework the temporal enactment of patient visits during residency. Likewise, her desired efforts to integrate prayer into patient visits reflects a shared appropriation that, if reified, produces socio-emotional structuration in patient-provider practice.
During observations, Dr. Chen navigated temporal and structural constraints that caused professional vs. relational identity tension by making time to attentively listen to her patient. Tessa, a 42-year-old Black female patient, explained excruciating eye pain that had forced her to stop driving. She recounted a prior visit for the same issue, but “the nurse was very rude” and the physician “rushed.” Dr. Chen turns from the computer and looks directly at her, saying, “I’m sorry about that,” with her full attention and eyebrows furrowed. She inquires further to understand Tessa’s symptoms. She then intermittently faced the screen for extended periods—typing, reviewing information, and sitting with her back to Tessa—creating stretches of silence. After several pauses, Chen asked, “I need my attending to come see us, if that’s OK?” It became clear that her silence reflected careful use of the EHR as a search engine, listening to Tessa, inputting symptoms, and asking clarification questions to ultimately diagnose Tessa with Graves’ disease.
Tessa is relieved. She exclaims, “I haven’t had a doctor that actually listens to me… I know y’all only have a certain amount of time… so I get it, [but] I appreciate it. I really, really do.” Dr. Chen reassures her, saying “you are easy to care for.” Tessa proceeds to her insurance paperwork problems. Chen swivels her chair towards her and completes the forms with her in that moment. She spends 8 minutes translating medical terminology to ensure Tessa understands. Chen then smiles ear-to-ear as she accepts Tessa’s hug. She was in the room with Tessa for 33 minutes.
Dr. Chen’s identifications suggested conflict. Verbally, she apologized for other providers’ behaviors, signaling divergent values. Nonverbally, she paused, redirected her body orientation, and furrowed her brows. She worked around temporal constraints embedded within professional norms to problem solve with Tessa in the moment (path E). She prioritized her relational identity region as evidenced through her cheerful smile when Tessa embraced her before her exit (path F).
Relational Identity Constraints Lead to Appropriating Knowledge Tasks
Resident PCPs often encountered knowledge constraints during office visits (e.g., underserved patients’ low literacy levels) that conflicted with the enactment of their relational PCP identity. PCPs appropriated care in inventive ways to work around these constraints, which sourced relational PCP identity conflicts (paths D). They then shared these appropriations, thus reshaping workplace structures (path E). Dr. Mao exemplifies: It’s just thinking creatively to serve them and doing the best I can. I have a patient who I see very regularly who's illiterate, and there are challenges with him just being able to take his medicine properly… and he doesn’t have any family to help either… So, even just drawing pictures, “This is the sun for morning, and this is the moon for night. And this little circle is your pill, and you're supposed to take it here.” Things like that… sometimes you have to literally take a sheet of paper from the printer and draw.”
Moreover, Mao discovered Amazon PillPack as a workaround to meet her patient’s literacy needs: Amazon PillPack is really wonderful because instead of having to open prescription bottles and understand, like, oh, this is for this and you take it at this time, PillPack sends you every pill you need in a pouch… you don't have to actually sort it… You have to have an e-mail account to set it up… So I had to personally… create an e-mail for him… It's a little complicated if you can't read… It was just taking the time to go do that for him because otherwise, how is he going to get his medicine?… Before that he was not taking any meds and now, he is taking his meds correctly 80% of the time.
Dr. Mao shared this work appropriation with her resident colleagues and enacted this change moving forward with all her patients who encountered significant literacy challenges (path E).
Somewhat against her medical training, Mao explains she has started to approach the patient-provider relationship through a “teammates” philosophy: Doing this extends far beyond how you do it in the textbook because if they can't access whatever you're trying to do or make that happen, then it's not effective, no matter what you do… The history of medicine has been a little paternalistic at times, to say the least… [but] the newer generations of doctors, we think a little bit more like, “Hey, let's take into account the patients’ opinion and social state… I’m like, “I want to be your teammate.” [One time] my older attending looked at me like, “hmm,” [laughs] because it was a foreign concept… But I very much care about that, and now I always emphasize that to my patients… other residents my age are doing that, too.
Dr. Mao’s actions reflect socio-emotional change on both the relational and professional levels (path E). She is confronting the paternalistic traditions institutionalized within medicine (i.e., professional structures) and asserts that her generation of doctors are instituting similar changes. Thus, they are repositioning their PCP identities in ways that prioritize relational identity (path F).
Discussion
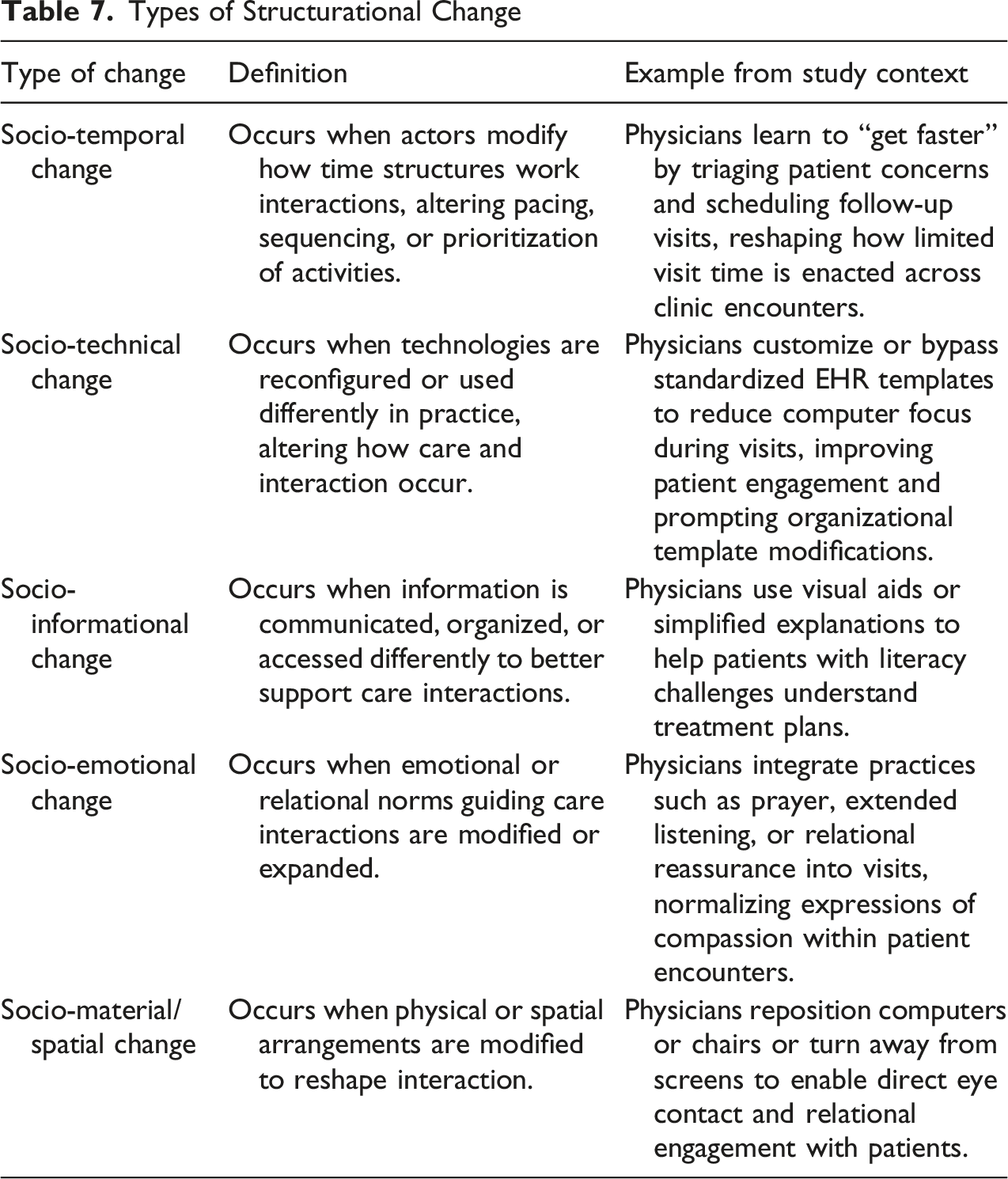
The findings from this study build the Structurational Model of Identity Conflicts (Figure 1), which depicts how resident PCPs encounter a taxonomy of identity-centered constraints, including financial (e.g., insurance), material (e.g., computer-use), and temporal (e.g., visit times) constraints that created multi-level identity conflicts (path C). The incompatibility of PCPs’ professional identity, which was often tethered to macro-level structures governing the institutionalized physician occupation, with identities that prioritized compassion and situated connection, prompted care appropriations (i.e., workarounds) that enabled PCPs to reengage with important social contexts of work (path D). Interview data revealed how appropriations became routinized, shared, and reified, enacting system-level changes that took many forms (i.e., socio-temporal, socio-technical, socio-informational, socio-material/spatial, and socio-emotional change; Table 7; path E). These system-level changes, and their associated affordances to situated care, were symbolic of how PCPs actively repositioned their work identities (path F).
Contributing to the Structurational Model of Identification
Results contribute to the Structurational Model of Identification (SMI) in four ways: foregrounding identity-centered constraints, expanding notions of appropriation, and emphasizing temporality and compassion in structuration.
Theorizing Identity Constraints and Expanding Appropriation
First, this study builds on the SMI by further theorizing how identity conflicts emerge within organizational activity and can generate structurational change. The SMI argues organizational members have multiple, regionalized identities that can partially overlap and conflict, and are triggered through activity and situated identifications (Scott et al., 1998). Yet it does not explicate how material, temporal, logistical, financial, structural, and knowledge constraints function as identity-disrupting structures in practice. By developing an identity-centered taxonomy of constraints, this study demonstrates how structural conditions systematically produce multi-level identity conflicts within a core professional activity. In doing so, it shifts the SMI from a framework primarily concerned with attachment to situational identity targets and salience to one focused on explaining identity destabilization and generative repair.
Second, this study reconceptualizes appropriation within SMI. Scott et al. (1998) acknowledge that identities are appropriated in interaction. Appropriation refers to how actors draw upon, invoke, or use identity structures in situated activity. When actors draw upon identity structures in ways that foreground incompatible identity regions, identity conflict can emerge. In contrast, the Structurational Model of Identity Conflict theorizes identity conflict as a generative mechanism that catalyzes appropriation, while portraying appropriation as both identity- and work-centered. Contradictory structures create identity tension, which then prompted employees to creatively reinterpret and modify work tasks and identity positioning. These micro-level appropriations, when shared and routinized, then recursively reshaped work norms and identity expectations. Thus, identity conflict is not merely a byproduct of situational identity appropriation, but a structurational engine through which professional identities, work tasks, organizational routines, and potentially institutionalized care practices evolve over time. In this way, the Structurational Model of Identity Conflict extends the SMI beyond activation and attachment modalities by illustrating how recurring situated identity conflicts can recursively generate organizational and institutional change through shared work appropriations. Further, this research produced an a priori identity conflict codebook that can help future scholars code for both verbal and nonverbal identifications connected to identity conflicts (See Table 4).
Interconnected Structurational Processes Within the Structurational Model of Identity Conflict
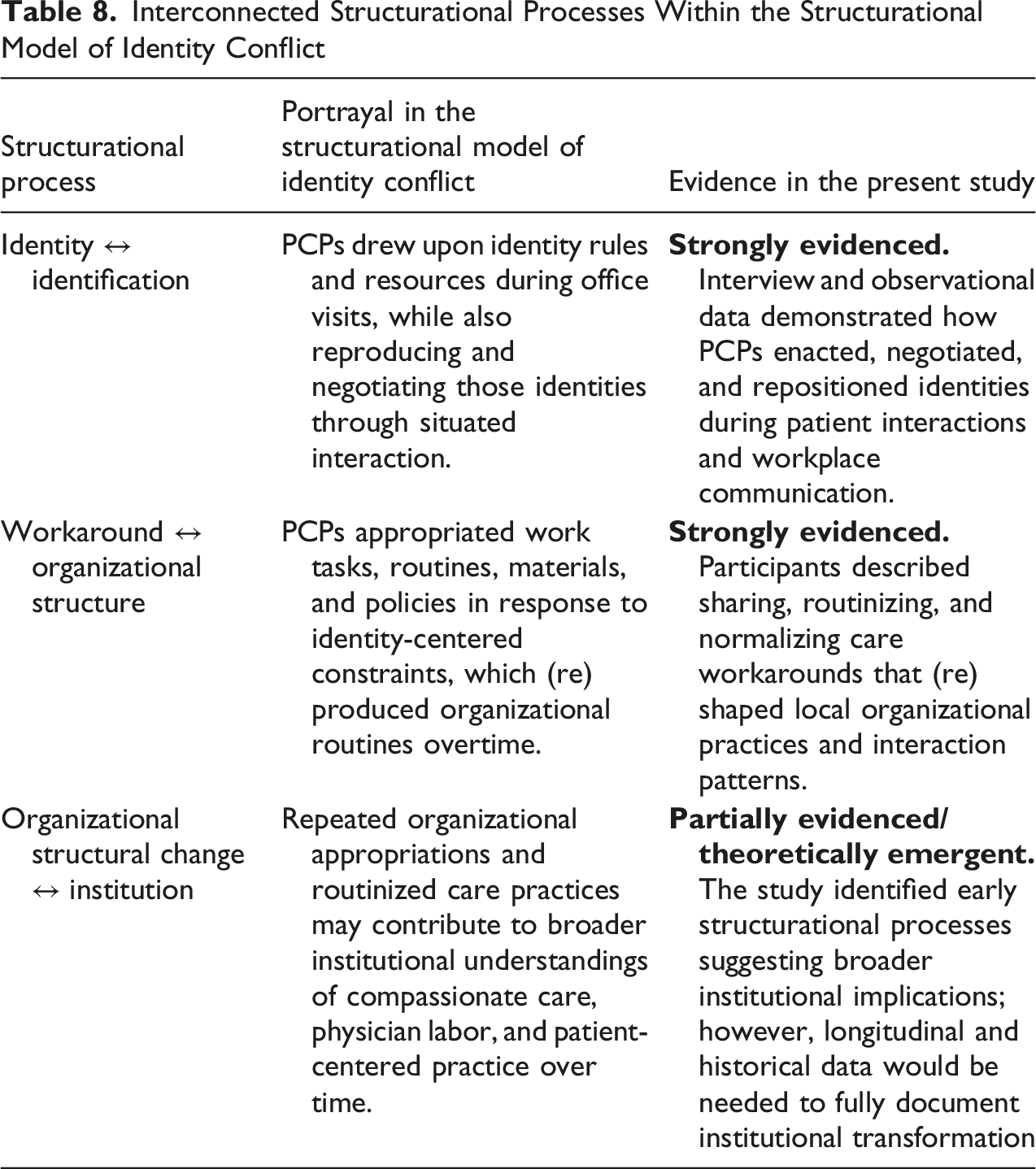
Activities Structure Identity Through Temporality
Third, this study introduces temporality as a key factor in the relationship between activity and identity. Scott and colleagues (1998) called for SMI research to examine specific activities vital to organizations and professions, rather than general work activities, to more sophisticatedly understand identity salience. Accordingly, this study analyzed a specific identity activity—the PCP visit within residency—a unique time-space and transformative identity event wherein resident PCPs confront the demanding realities and profound responsibilities of in-situ medical practice. Results nuance our understanding of how professional activities shape and are shaped by situated identity expression. The 15-min visit was framed as a standard identity activity ordering resident PCP behavior and symbolizing control and care efficiency. Yet, PCPs often had emotional reactions to universally applying such policies to underserved patients who had enhanced needs. Instead, they (re)shaped this activity into a site of creative problem-solving—manipulating logistics, policies, and materials—in efforts to connect with patients and privilege what they perceived to be compassionate care, despite increased labor and time commitments.
Furthermore, resident PCPs often negotiated temporal layering (e.g., drawing on past training and present constraints to articulate desired future states) in their efforts to improvise office visits, underscoring temporality as central to identity activity. Though chronological time acted as a structure that constrained office visits, time also operated as an interpretive device through which PCPs (re)claimed compassionate care as a meaningful identity resource. By foregrounding temporality as both a fixed, structuring resource and as a construal (e.g., an interpretation and made meaningful through communication), this study adds nuance to SMI’s notion of activation modality—or the relationship between activity and identity (see Ballard et al., 2024). Scott et al. (1998) argue that routine or significant work activities activate particular identity regions and corresponding identifications; thus, activities structure identity by enabling and/or constraining identification. Building on this premise, this study specifies how the temporal organization of activity intensifies the salience of incompatible identity regions. Time is not simply a neutral backdrop for situated activity; it is a structuring feature that can heighten identity tensions, while also providing agents leverage to reposition identity. Temporally standardized activities may therefore amplify identity conflict and become sites of identity reinterpretation.
This extension sharpens SMI’s utility for examining professions organized around temporal scripts, including pilots/flight crews structured by flight schedules, social workers shaped by caseload quotas, call center labor evaluated through average handle time metrics, and teachers structured by class periods. Extending Scott et al.’s (1998) example of John, a professor whose daughter enrolls in his college course, we can now see how the temporally bounded class period intensifies the salience of his father (personal) and professional identities. The activity of teaching—structured by fixed time—heightens the likelihood of incompatible identities. If John’s daughter was struggling in class to grasp course concepts, he likely cannot alter the temporal structure of the class period (e.g., extend class) or manipulate time as a class resource by spending disproportionately more of it on his daughter. However, he could routinely make time (e.g., time as a construal) to connect with his daughter on class material outside of class to manage competing identifications. In this way, temporality structures identity tension while simultaneously affording interpretive space for identity negotiation that leads to structurational change.
Enacting Compassion Drives Identity and Work Appropriations
Finally, this research extends the SMI by showing how employees (re)shape work practices and identifications to sustain compassion—a theoretical construct garnering increasing scholarly interest and linked to generative organizational outcomes (McAllum et al., 2023). Like Leach et al.’s (2024) structuration-based analysis of compassion in healthcare organizations, this study examines how structural barriers—such as managed care logics and productivity pressures—constrain practitioners’ enactment of compassion, and how agentic actions can transform these organizational structures. This study advances that work by specifying the identity-based mechanisms that precipitate agentic action. Constraints specific to offering underserved patients compassionate communication spurred care appropriations that reshaped practice to prioritize underserved patients’ diverse needs. Compassion was an important background for understanding how temporally standardized activities (e.g., the 15-min office visit) and standardized materials activated partially incompatible identity regions due to underserved patients’ heightened communicative needs. Dr. Henry appropriated, rather than reproduced, EHR templates to free up time to sit with underserved patients in their suffering. Dr. Mao set up PillPack accounts for her illiterate patients, discursively reframing care as being their “teammate.” These agentic behaviors, shared across patients and amongst resident PCPs, both reproduced existing identity structures (e.g., professional expectations) and created new norms to sustain compassionate care amid increased communicative challenges. In doing so, this project deepens structuration-based compassion scholarship by integrating identity regionalization, identity-centered constraints, and the identity-activity relationship into explanations of how agency emerges and becomes consequential for the communicative practice of compassion.
Practical Implications
Rather than framing identity conflicts as disrupting workplace morale or commitment, this study shows they can produce constructive change in healthcare contexts where constraints have previously limited relationship-centered care. Findings deepen our understanding of compassion practices and perceptions in ways that can inform more effective communication interventions across professions—such as social work, education, and legal aid—where workers must balance professional demands for efficiency with advocacy and relational commitment to those they serve.
Results also suggest that organizations should implement systemic changes, such as creating formal spaces for employees to explore identity tensions. For example, managers could incorporate quarterly or biannual “identity dialogue” sessions into professional development initiatives. Led by an HR specialist or trained facilitator, these sessions would foster thematic discussions of identity overlap/conflict (e.g., patient care vs. productivity targets), under confidential, non-punitive ground rules oriented toward collective sensemaking rather than evaluation. Participants would collaboratively problem solve, brainstorm, and share workarounds (see Barrett & Stephens, 2017). Summarized, anonymous insights could inform policy, workflow design, and system-level reform. At the organizational level, employee-reported identity tensions should revise productivity expectations that routinely undermine relationship-centered care. Doing so promotes structuration by allowing employees’ identity negotiations to recursively shape organizational systems and routines. Such insights may also amplify patients’ voices, as resident PCP identity conflicts are embedded within structures that constrain patient agency in organizational service procurement.
Limitations and Conclusion
This study has several limitations. First, this study lacks measures of identity/identification and conflict to quantify how identified PCPs were with various targets and the level of conflict they perceived between targets. Second, conducting interviews after observations or performing on-site interviews during observations may have offered more informed interpretations of observed identifications. Third, though patients were observed, this study primarily focused on residents, and thus, only offers one vantage point to identity conflicts. Fourth, due to the nature of the analysis, this study did not examine conflicts that involved more than two identity levels. Fifth, identity conflict levels were interpreted according to the salient identity targets invoked in participants’ accounts. Participants sometimes described the same structural constraint as occurring at different identity levels, depending on how they framed the tension during interviews, reflecting the fluid and embedded nature of identification as theorized within the SMI. For example, the 15-min visit was sometimes framed as a professional constraint tied to broader changes in physician reimbursement structures and evolving expectations about what it meant to be a physician; at other times, this temporal constraint was framed as an organizational tension linked to workplace performance metrics, routines, and reward structures. Finally, evidence for Path F—(re)positioning identity—was necessarily more limited than evidence for other model pathways. Participants described care appropriations that became shared and routinized, yet documenting how these practices ultimately reposition identities would require longitudinal and historical data beyond the scope of the present study.
In conclusion, this study examined how resident PCPs negotiated multiple identities when caring for underserved patients during office visits. Results offer several key entry points for future organizational communication research. For one, they suggest identity conflict is not only a product of competing identity targets, but also of temporal layering, where past training, present demands/constraints, and desired future selves intersect to intensify tensions. Time is an implicit backdrop to the SMI, as identification processes are continually (re)negotiated. Yet it is not theorized as a structuring resource that agents draw upon to intensify or ease identity conflict, creating avenues for future research. Additionally, past research argues that needs for human connection (i.e., compassion, empathy) and positive self-image are antecedents to job crafting (Niessen et al., 2016). Yet this study suggests emotional responses—i.e., EHR frustration, patient empathy—are better suited as interaction variables associated with identity conflict. Future researchers could test how emotion variables moderate the relationships between identification and employees’ job appropriations in high-stakes organizations. In the end, this study shows how the 15-min office visit is not merely a site of care delivery, but an ongoing arena of identity negotiation where physicians continually reconstruct the practice of compassionate care within the realities of the contemporary healthcare environment.
Footnotes
Acknowledgements
The author would like to thank the National Science Foundation for funding this research and her graduate research assistants, Elizabeth Guttenberg and Grace Hanlon, for aiding in the data collection process.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by The National Science Foundation, Division of Social and Economic Sciences; 2144853.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.