
Abstract
Completed as part of a larger dissertational study, the purpose of this portion of this descriptive correlational study was to examine the relationships among registered nurses’ clinical experiences and clinical decision-making processes in the critical care environment. The results indicated that there is no strong correlation between clinical experience in general and clinical experience in critical care and clinical decision-making. There were no differences found in any of the Benner stages of clinical experience in relation to the overall clinical decision-making process.
Decision-making is an essential process of human nature (Tanner, 2006). Clinical decision-making (CDM) is a phenomenon that is fundamental to healthcare practice. While CDM influences the entire spectrum of healthcare practitioners, nurses, as frontline clinicians, are faced with important clinical decisions on a daily basis (Ramezani-Badr, Nasrabadi, Yekta, & Taleghani, 2009; Tanner, 2006). The overall goal of CDM is to provide the highest quality patient care based on the available resources. Knowing the factors that influence the CDM process increases the likelihood of providing high-quality, safe patient care. Nurses are accountable to their patients, the profession, and the organizations for which they work; therefore, it is imperative that there be an understanding of the mechanisms involved in reliable CDM (Tanner, 2006).
CDM is defined as the thought process of choosing alternatives in providing care to patients involving both diagnostic reasoning and clinical judgment (Banning, 2008; Florin, Ehrenberg, & Ehnfors, 2008). It involves managing a variety of information from varied sources in order to make a clinical judgment. In CDM, nurses must accurately assess and identify deviations from a normal clinical picture of health or illness and make a decision based on the data presented (Cranley, Doran, Tourangeau, Kushniruk, & Nagle, 2009). This complicated process can mean the difference between life and death for patients (Gillespie & Paterson, 2009).
According to Benner, experience is paramount when looking at the CDM process (Benner, 2001, 2004). Experience, intuition, education, and environment all influence the overall decision-making process. Experience, however, remains the ultimate contributor when making clinical decisions (Benner, 2001). Benner’s ideas were used to guide this descriptive correlational study, which examined the relationship of clinical experience and CDM in the critical care environment.
Significance of the Study
With changes in healthcare delivery, increased patient acuity, and increased accountability in practitioners’ decisions, it is vital to better understand how nurses make clinical decisions and what factors influence them (Gillespie & Paterson, 2009). Patients in acute care settings are sicker and require experienced nurses who will provide the highest levels of quality care (Florin et al., 2008). This is particularly true in critical care. In this environment, decisions are made frequently and quickly, and a delay in the decision-making process can be a matter of life or death. This study contributed to the existing body of knowledge about decision-making and its relation to clinical experience in the high-stress critical care arena.
Theoretical Framework
The theoretical framework of this study was based on Benner’s “From Novice to Expert” model (Benner, 2001, 2004). Benner (2001) developed an intuitive, humanistic decision-making model that described five stages of skill acquisition in nursing clinical knowledge: novice, advanced beginner, competent, proficient, and expert. These five stages reflect changes in three general aspects of skilled performance and decision-making: (a) a move from reliance on abstract principles to the use of past concrete experiences, (b) a change from viewing a situation in multiple fragments to seeing a more holistic picture, and (c) a movement from detached observer to active performer (Benner, 2001). Each level is characterized by increased reliance on past clinical experience. The five stages are novice (less than 6 months’ clinical experience), advanced beginner (6 to 12 months’ clinical experience), competent (1 to 3 years’ clinical experience), proficient (4 to 5 years’ clinical experience), and expert (over 5 years’ clinical experience). When making a clinical decision, novice nurses look to the hospital or unit protocols to assist with decision making; the advanced beginner looks to the preceptor to guide the decision; and the competent nurse bases his or her decision on previous real-life clinical experience. Proficient nurses make a decision very quickly and move forward with that decision, and expert nurses look at a given clinical situation and act without conscious thought as to need. No one needs to guide the expert nurse in this decision.
Benner (2001) described experience as a process of knowing through repeated exposure to situations that leads to a refinement of earlier thoughts and ideas. Nurses’ experiences provide a knowledge base upon which to reflect and to use in the development of their own practice. Experience over time is mandatory in order to develop expertise in CDM. When engaged in CDM, the expert nurse may make decisions as a result of an intuitive thought process that is based on accumulated expertise. The essence of intuition is the recognition of previously experienced patterns and the detection of subtle clinical changes. It is an understanding without rationale. The expert nurse acts intuitively, based on vast amounts of experience that leads to “knowing how.” When engaged in CDM, the expert nurse may intuit the best way to handle a situation but not be able to explain this CDM process logically (Benner, 2001; Benner, Hughes, & Sutphen, 2008).
A key component of Benner’s work that can be used as a guide when examining the ability to make a clinical decision is the development of intuitive judgment. Intuitive judgment involves pattern recognition (perceptual ability to recognize relationships without prespecifying the components of the situation), similarity recognition (ability to identify problems based on previous similar or dissimilar situations), commonsense understanding (ability to see the subtle nuances of a situation), skilled know-how (decision-making ability based on embodied intelligence), sense of salience (knowing which events and observations are more important), and deliberative rationality (way to clarify perspective by considering more than the given situation; considering the “whole picture”). There are differences that can be seen in the capacities and capabilities of nurses in their decision-making in these six areas depending on where in the five stages of skill acquisition they are (Benner, 2001).
Benner’s work provided a theoretical structure upon which to view application of nursing knowledge to the CDM process. She described how the novice nurse will use procedures and guidelines to guide decision-making, but as the nurse gains a wealth of experience, the decision-making becomes more intuitive. While timely and accurate decision-making is a universal expectation, it is the expert nurse who is able to do this on an intuitive, holistic level. Being able to step back and view the patient as a whole, instead of as a series of tasks, is part of the progression of CDM (Benner, 2001).
Related Literature
Discussion and research about the concepts of clinical experience and CDM are intertwined in the literature (Andersson, Omberg, & Svedlund, 2006; Dowding, Spilsbury, Thompson, Brownlow, & Pattenden, 2009; Ferrario, 2003; Hoffman, Aitken, & Duffield, 2009; Ramezani-Badr et al., 2009). Clinical experience, along with intuition, is often discussed as the main influence on the overall decision-making process. Experienced practitioners are able to make rapid decisions based on like situations (Benner, 2001), while intuition is the basic “knowing” of the patient and being able to decide what to do based on a “gut feeling” related to previous exposure to similar clinical situations.
Ramezani-Badr et al. (2009) interviewed critical care nurses (N = 14) in a qualitative study examining the reasoning strategies and CDM processes used by Iranian critical care nurses. They found nurses used different reasoning and decision-making strategies to evaluate patients’ problems and to plan appropriate care for the patients. Three main themes emerged: intuition, recognizing similar situations, and hypothesis-testing. Intuition was considered a “gut feeling” (Ramezani-Badr et al., 2009) when nurses deliberately recognized similar situations from the past and compared them with the present situations in order to make proper clinical decisions. Previous clinical experience was used by nurses when they found the symptoms from one patient corresponded to those of another. According to the researchers, some nurses generated hypotheses after assessing and examining the patients and tested these hypotheses to determine the main problem and appropriate care (Ramezani-Badr et al., 2009).
Dowding et al. (2009) studied a specific group of critical care nurses, those working with heart failure patients (N = 18), in their qualitative study of CDM through observations and interviews. Their study examined the types of decisions made by these nurses and the involved processes and factors in the real-life and real-time decision-making in pharmacological management of their palliative care patients. Medication titration decisions were found to be conducted through a combination of intuition and analysis. Peer support with decision-making was utilized in palliative care situations reflecting a team approach to the CDM process when faced with a potentially difficult, life-or-death decision related to medication administration.
The qualitative work of Andersson et al. (2006) examined nurses working in an emergency room (ER) in Sweden (N = 19). Their aim was to describe how nurses perform triage when patients enter the ER and the factors considered when prioritizing patient care. All participants had more than 6 months’ experience in performing triage and specialty training for emergency situations and therefore would be considered as advanced beginners and higher in Benner’s (2001) model. Triage nurses have a key position in the ER as their decisions directly influence further treatment and care. Each participant was individually observed and interviewed when carrying out triage work based on a participant observation model. Using content analysis of the data, it was found that the ER nurses’ most important function was to correctly prioritize patients and care within a limited amount of time. Experience, knowledge, and intuition were the three dominant themes. Researchers found “sixth sense” (Andersson et al., 2006, p. 142) as a predominant factor is nurses’ decision-making and prioritization skills, a natural feeling that occurs when assessing a patient’s condition. The external work environment was always a factor in the ultimate decision, but it was this “sixth sense,” this instinctive method of thinking and acting, which occurred in most decisions (Andersson et al., 2006).
Hoffman et al.’s (2009) qualitative work examined the ways both novice (N = 4) and expert nurses (N = 8) working in an ICU used cues, or patient assessment data, during decision-making while caring for postoperative patients. Different from Benner’s classifications, novice nurses had no more than 2 years’ experience working in nursing. Expert nurses had more than 3 years of nursing experience and more than 6 months’ experience in their current unit. They found expert nurses were more proactive in collecting relevant cues and anticipating problems that may help identify patient problems. The expert nurses planned ahead in the care for their patients, anticipating what might happen and collecting cues in anticipation of problems. The accurate detection by nurses of cues that may indicate a change in patient status is a vital aspect of CDM, particularly in critical care (Hoffman et al., 2009).
Ferrario’s (2003) quantitative work looked at CDM processes and thought patterns of nurses working in the ER (N = 219). Consistent with Benner’s (2001) definition of novice and expert nurses, Ferrario grouped nurses as experienced (5 or more years of ER work) and inexperienced (less than 5 years of experience). Using a 16-item questionnaire called the Clinical Inference Vignettes for Community Health Nurses (O’Neill, 1992) that was modified for use with ER nurses (internal consistency reliability coefficient = .82), it was found that experienced nurses used the heuristic, trial-and-error approach—mental short cuts based on prior experience—as the primary method of decision-making, more so than the inexperienced nurses (x² = 3.98, df = 1, p = .046). These findings support Benner’s (2001) model and the role of clinical experience.
The majority of the reviewed research on clinical experience and CDM has been conducted using qualitative methods (Andersson et al., 2006; Dowding et al., 2009; Hoffman et al., 2009; Ramezani-Badr et al., 2009). The quantitative study (Ferrario, 2003) that was conducted utilized instruments on small samples, thus making generalizability difficult. However, most studies were consistent in identified themes. The most commonly identified theme was that clinical experience was the most frequent indicator of CDM. These gaps in the current literature support the need for the study that quantitatively examined the relationships between clinical experience and nursing CDM processes with a large national sample.
Research Design
A descriptive correlational research design was used to investigate the relationships among the study variables. The research question for this part of the study was: What is the relationship between nurses’ clinical experience and CDM in a critical care environment? A descriptive correlational study design does not determine causality between or among variables but instead describes the strength and extent of the relationships (Polit & Beck, 2008). Since no quantitative studies were found in the literature related to clinical experience and CDM in the critical care environment, this design was selected to investigate the potential relationships among selected variables.
Definitions of Variables
For this study, a
Population and Sample
The population and sample for this study were limited to registered nurses currently employed in a critical care environment (ICU, CCU, PACU) in the United States, able to read and write in English, and have access to the Internet. Those working exclusively in ERs were not included. A convenience sample was solicited through the American Association of Critical Care Nurses, or AACN (N = 94,000). There were 539 people who started the survey and 413 people who completed the survey in its entirety (76.6% completion rate).
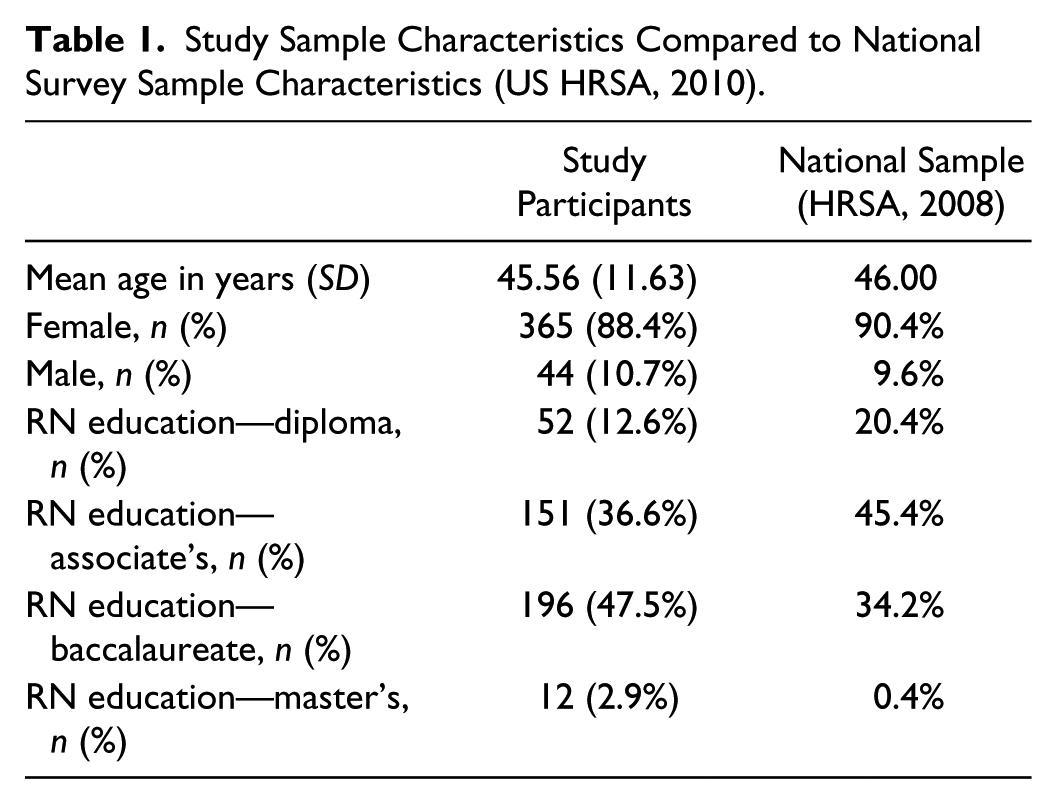
The participants were primarily White (91%), critical care nurses ranging in age from 19 to 68 (M = 45.56) from across the United States. Participants were classified as experts based on Benner’s (2001) classifications, in both experience in nursing in general (88%) and in critical care (82%) in particular. Participants completed two online surveys (Jenkins’ CDMNS and a demographic sheet constructed by the researcher) via Survey Monkey™.
Research Instruments
Study instruments were selected for this study based on several considerations: the overall appropriateness of the instrument for measuring the intended study variables and the instrument’s psychometric and measurement properties, including reliability coefficient, length of time to complete, and availability. CDM was measured using one instrument: the CDMNS. Permission to use this instrument was received from Springer Publishing.
The CDMNS (Jenkins, 1985) is a 40-item Likert-type scale self-report instrument that took approximately 10 minutes to complete. The scale contains 40 items on four subscales (10 items each): the search for alternatives and options, canvassing of objectives and values, evaluation and reevaluation of consequences, and search for information and unbiased assimilation of new information. Answers are provided using a five-item Likert-type scale with both positive and negative items and answers ranging from always (A) to never (N). The potential score on the CDMNS can range from 40 to 200. Lower scores represent a negative perception of decision making, and higher scores represent a positive perception of decision making.
Overall test reliability was established using a Cronbach’s alpha coefficient to measure internal consistency. The initial Cronbach’s alpha coefficient was 0.79. After examination of items for intercorrelations using factor analysis, four items were dropped and the ultimate Cronbach’s alpha for the entire 40-item questionnaire was established at 0.83.
Additional studies that have utilized the CDMNS have consistently shown validity and reliability values similar to the original work. Girot (2000) used the CDMNS to examine CDM in four different groups of nurses (N = 82 total) with various levels of experience. Content validity was established by a group of experienced practitioners considered to be “expert decision makers” in practice. Additionally, reliability of the instrument was demonstrated with a Cronbach’s alpha of 0.78. Bowles (2000) used the CDMNS for examining CDM in her study of baccalaureate nursing students (N = 65). The reliability of the instrument was found to be similar (Cronbach’s alpha = 0.83).
The second instrument used was a demographic sheet created by the researcher. Demographic variables included but was not limited to descriptive information about the participants such as age, gender, geographic region of practice, program from which the participant received basic nursing education, highest credential held, total time working in nursing in general, total time working in critical care, and average nurse-to-patient ratio at place of employment.
Data Collection Procedures
After full institutional review board (IRB) approval was granted, all data collection was conducted electronically using Survey Monkey™. An online solicitation form was sent to all AACN members who receive the weekly AACN newsletter. A link to the research surveys was embedded within the newsletter. Members opted to participate by clicking on the link. The survey link was sent out 4 consecutive weeks.
Online data collection helps to minimize any potential risks and allows for greater maintenance of confidentiality (Polit & Beck, 2008). Only the researcher was able to obtain the completed questionnaire through a private passcode. Confidentiality and anonymity of participants were maintained throughout the entire data collection process. There is a function of the Survey Monkey online format that is designed to allow for data collection to be anonymous to the researcher. This function was utilized. All collected data were recorded anonymously. The coding system used did not have any identifying information such as names, addresses, or social security numbers. Informed consent was implied by the voluntary completion of the research instruments by all participants. To ensure further confidentiality of all responses, submitted data were stored only on a memory key and kept in a locked, secure place accessed only by the researcher.
Data Analysis Procedures
Collected data were directly imported into IBM SPSS for Windows (Version 20) through a set function of Survey Monkey. Prior to conducting statistical analyses on the research question and participant information, the researcher screened all data for missing values, outliers, and accuracy of data entry, resulting in an analytical sample of 413. Any survey that was not completed in its entirety or had multiple outliers was omitted. Data recoding was used to recode items that required reverse scoring.
Descriptive statistics were computed for all continuous variables. These included the participants’ survey scores, age, and total time working in nursing. Descriptive statistics were also computed for all categorical variables, including gender, race, ethnicity, geographic area of practice, basic registered nursing education program, highest credential held, critical care unit of work, employment status (full-time employment or FTE, part-time employment or PTE, per diem), shift worked, average nurse-to-patient ratio, and ranking of facility for level of acuity.
A total score, mean score, median, mode, standard deviation, and reliability coefficient were obtained for the CDMNS instrument as a whole, and a total score, mean score, median, mode, and reliability coefficient were obtained for each of the four subscales of the CDMNS.
Analyses of the data were conducted to see if the data met all of the assumptions of statistical testing for multiple regression. The testing for normality was conducted using the Shapiro-Wilk test, skewness, and kurtosis. Clinical experience in nursing in general and clinical experience in critical care were not normally distributed as assessed by Shapiro-Wilk’s test (p < .05). Clinical experience in nursing in general and clinical experience in critical care were not normally distributed, with a positive skewness of .120 and kurtosis of .240. Therefore, nonparametric analyses were conducted using the Spearman rho correlation coefficient. Data transformation was conducted using the square-root transformation in order to correct for the nonnormal distribution. The assumption of independence of residuals was met by all variables, as assessed by a Durbin-Watson statistic of 2.128. The assumptions of linearity and homoscedasticity were met by all variables by examining scatterplot diagrams that showed that the residuals were equally spread over the predicted values of the dependent variable.
Results
The following tables display some of the characteristics of the study sample compared to that of a national survey conducted by the U.S. Department of Health and Human Services Health Resources and Services Administration (US HRSA, 2010) on the same subject (Table 1). Also see the sample according to Benner’s classifications (Table 2).
Study Sample Characteristics Compared to National Survey Sample Characteristics (US HRSA, 2010).
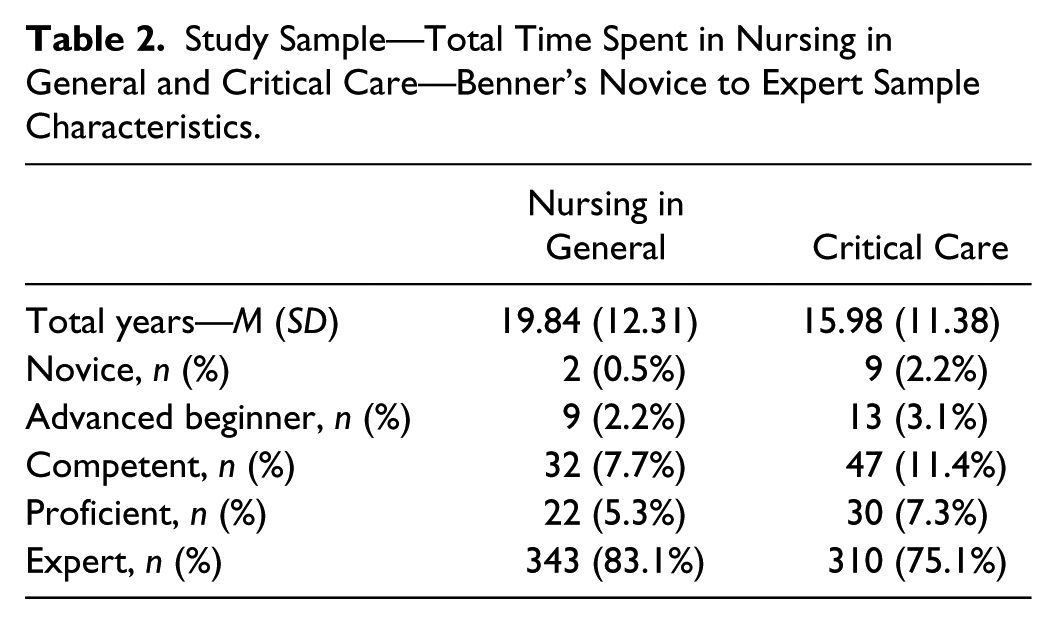
Study Sample—Total Time Spent in Nursing in General and Critical Care—Benner’s Novice to Expert Sample Characteristics.
Discussion of Findings
For the CDMNS, the participants had a mean score of 152.61. For Subscale 1 (search for alternatives and other options), the mean score was 39.68; Subscale 2 (canvassing of objectives and values), the mean score was 39.19; for Subscale 3 (evaluation and reevaluation of consequences), the mean score was 36.85; and for Subscale 4 (search for information and unbiased assimilation of new information), the mean score was 36.90. There were no differences seen in scores between the five Benner (2001) categories (novice, advanced beginner, competent, proficient, and expert). However, when looking at the existing literature that used the CDMNS, this sample scored higher, possibly suggesting that critical care nurses with more clinical experience have more positive CDM skills.
The lower strength correlations are not surprising for several reasons. Based on the description of the sample, it is clear that the participants were a homogenous sample in relation to level of experience based on Benner’s (2001) model. The more homogenous the population from which the sample under study is drawn, the lower the resulting correlation (Polit & Beck, 2008). The majority of the participants (83.1%) were experts according to Benner’s (2001) classifications. The study sample was obtained through use of a professional organization, the AACN, and unknowingly yielded a high number of experts. Another contributing factor to the reduced strength of the correlations may have been the small sizes of Benner’s (2001) subgroups; in nursing in general: novice (n = 2), advanced beginner (n = 9), competent (n = 32), and proficient (n = 22); and in nursing in critical care: novice (n = 9), advanced beginner (n = 13), competent (n = 47), and proficient (n = 30). This may have resulted in an inadequate power to detect a greater strength in the correlations.
Since a skewed sample was noted with the study population, the data were also analyzed using different groupings of the sample to see if any changes occurred in the strength of the study variables. A sample of 45 nurses was extracted using equal cells for the five Benner stages (n = 9 for novice, advanced beginner, competent, proficient, and expert). There were no differences noted in the resulting correlations.
Implications for Future Research
The sampling technique used in this study to garner participants unknowingly solicited a high number of nurses with advanced clinical experience. The overall CDM scores for the sample were high, yet there were no strong correlations found between CDM and clinical experience; the relative homogeneity of this sample likely skewed the results. To avoid a homogenous sample, replication of this study using a different sampling technique, such as nonrandom sampling, is recommended, with attention to recruiting equal numbers of participants from each of Benner’s categories.
According to Benner, experience is paramount when looking at the CDM process (Benner, 2001, 2004). Further investigation looking at these two variables in the critical care environment is needed. As nurses work in a practice-based profession, any variable that may influence this practice needs to be fully understood.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this review
Funding
The author received no financial support for the authorship and/or publication of this review.