
Abstract
A middle-range theory of heart failure self-care, derived from the self-care deficit theory of nursing, was tested among 175 Arab American older adults with heart failure. The middle-range theory achieved good statistical fit, but not all hypothesized relationships were supported. Specifically, conceptualizing basic conditioning factors as a single latent variable was not supported. However, individual factors of depression, social support, and time living with heart failure had a direct effect on both self-care agency and quality of life. Understanding predictors and outcomes of self-care within a theoretical framework is essential in caring for patients with heart failure.
Heart failure (HF) self-care is defined as the engagement of individuals with HF in the actions and behaviors that maintain life, healthy functioning, and well-being (Auld, Mudd, Gelow, Hiatt, & Lee, 2018; Jaarsma, Strömberg, Mårtensson, & Dracup, 2003). Recommended HF self-care behaviors include following a low-sodium diet, adhering to the prescribed medication regimen, restricting fluid intake, exercising regularly, weighing daily, monitoring changes in symptoms, and contacting a health care provider for worsening symptoms (Jaarsma et al., 2003). Effective HF self-care is associated with improved health outcomes including better quality of life (QOL) and health status (Auld et al., 2018; Zhang et al., 2016). However, effective HF self-care requires a complex set of cognitive and physical abilities that are influenced by many internal and external factors including age (Cocchieri et al., 2015). Age-related factors, such as limitations in physical abilities, contribute to the complexity of self-care among older adults with HF (Cocchieri et al., 2015). Understanding the factors that influence older adults’ engagement in HF self-care within a theoretical framework helps in developing appropriate interventional programs that are tailored according to the needs of this population.
Factors Influencing Self-Care Among Older Adults
The factors influencing HF self-care among older adults (65 years and older) include person-related, sociocultural, and health care-related factors. The person-related factors that have been examined for their direct effect on self-care include either personal abilities or characteristics. Being male, having impairments in executive function, and reporting high levels of depression have been found to be predictors of poor HF self-care (Cocchieri et al., 2015). In contrast, high levels of HF self-confidence and HF decision-making have been found to be predictors of high levels of HF self-care (Goodman, Firouzi, Banya, Lau-Walker, & Cowie, 2013). Many older adults with HF reported culture as an influence on their self-care behavior. A prime example is when older adults feel cultural and familial pressure to eat traditional foods, even if they exceed dietary sodium recommendations (Gowani, Gul, Dhakam, & Kurji, 2017). Although social support often enhances self-care, this support may also lead to negative outcomes such as feelings of being a burden to one’s family (Gowani et al., 2017). Health care-related factors include support from the HF health care provider and satisfaction with the care received. Many participants reported specific support needs from a health-care provider, such as assistance in understanding HF-related information (Gowani et al., 2017).
HF Self-Care Health Outcomes Among Older Adults
Older adults with HF engage in self-care in order to improve their health status and QOL. An interventional study that targeted regular exercise demonstrated the positive influence of improved self-care behavior on health outcomes (Zhang et al., 2016). Higher levels of HF self-care are also associated with better overall QOL (Auld et al., 2018) as well as disease-specific QOL (Zhang et al., 2016).
HF Self-Care Among Arab Americans
The number of Arab Americans in the United States is increasing. However, they are underrepresented in the health care literature (Nassar-McMillan, Ajrouch, & Hakim-Larson, 2014). Arab Americans are individuals whose families originated from 22 Arabic-speaking countries that belong to the League of Arab States (Nassar-McMillan et al., 2014). Although Arab Americans vary with respect to religious beliefs, they generally share core values in culture, ethnic, and linguistic ties (Abuelezam, El-Sayed, & Galea, 2018). These values may affect self-care behaviors (Alaloul, AbuRuz, Moser, Hall, & Al-Sadi, 2017). A recent comprehensive review noted that less acculturated Arab Americans have higher dependence on nicotine, engage in less physical activity, have a significantly higher prevalence of diabetes, and seem to have higher cardiovascular disease (Abuelezam et al., 2018). As all of these conditions are known to contribute to HF, Arab Americans are at increased risk of poor outcomes of HF. However, there is a significant lack of reliable and nationally representative data on health behaviors and health outcomes among this understudied population. Further, no literature could be found that specifically addressed HF self-care among Arab Americans. Instead, research on this problem can be informed by studies of Arab Americans with other chronic diseases, such as diabetes mellitus (DM), or studies about health-promoting self-care behaviors among Arab Americans.
Within the available literature, the factors that have been found to influence DM as well as health-promoting self-care behaviors among Arab Americans include self-efficacy, social support, acculturation, and the relationship with health care providers (Aqtash & Van Servellen, 2013; Bertran et al., 2015). High levels of acculturation to American culture, social support, and self-efficacy were found to be predictors of regular exercise (Aqtash & Van Servellen, 2013). Some Arab American patients with DM relate their lack of knowledge regarding DM self-care behaviors to their relationship with their Arabic physicians (Bertran et al., 2015). According to these patients, these relationships are medication- and results-focused rather than patient-centered (Bertran et al., 2015). Increased understanding of self-care within a cultural context is needed to assist this growing population manage their HF and improve their QOL.
Reviewing the literature of HF self-care and its influential factors and outcomes showed that many studies were not developed within a theoretical framework. Greater theoretical development, based on a self-care conceptual framework, is essential for understanding the role of culture and other influential factors on self-care behaviors, as well as the influence of those behaviors on health and QOL outcomes.
Theories of HF Self-Care
The situation-specific theory of HF self-care (Riegel, Dickson, & Faulkner, 2016) has been developed to address self-care and its influential factors. The central idea of this theory is that HF self-care is comprised of naturalistic decision-making regarding maintenance of certain recommended self-care behaviors, such as adherence to a low-sodium diet and management of symptoms (Riegel et al., 2016). Although these are important HF self-care behaviors, a theory with a broader view of HF self-care is needed to enhance understanding of HF self-care. Thus, the middle-range theory of HF self-care (MRT of HF self-care) was derived from the self-care deficit nursing theory (Orem, 2001). According to this MRT of HF self-care (Attaallah et al., 2021), influential factors have an impact on the patients’ HF self-care abilities. Influential factors include gender, religion, length of time living with HF, depression, social support, acculturation, and health care system factors. Influential factors are important as they affect the abilities needed to meet HF self-care. HF self-care abilities include cognitive abilities, HF self-efficacy, and HF decision-making. The outcome of these abilities is the self-care behaviors produced. HF self-care, therefore, is defined as engaging in recommended behaviors necessary to maintain optimum heart health and QOL (Attaallah et al., 2021). A pictorial representation of the MRT of HF self-care is provided in figure 1.
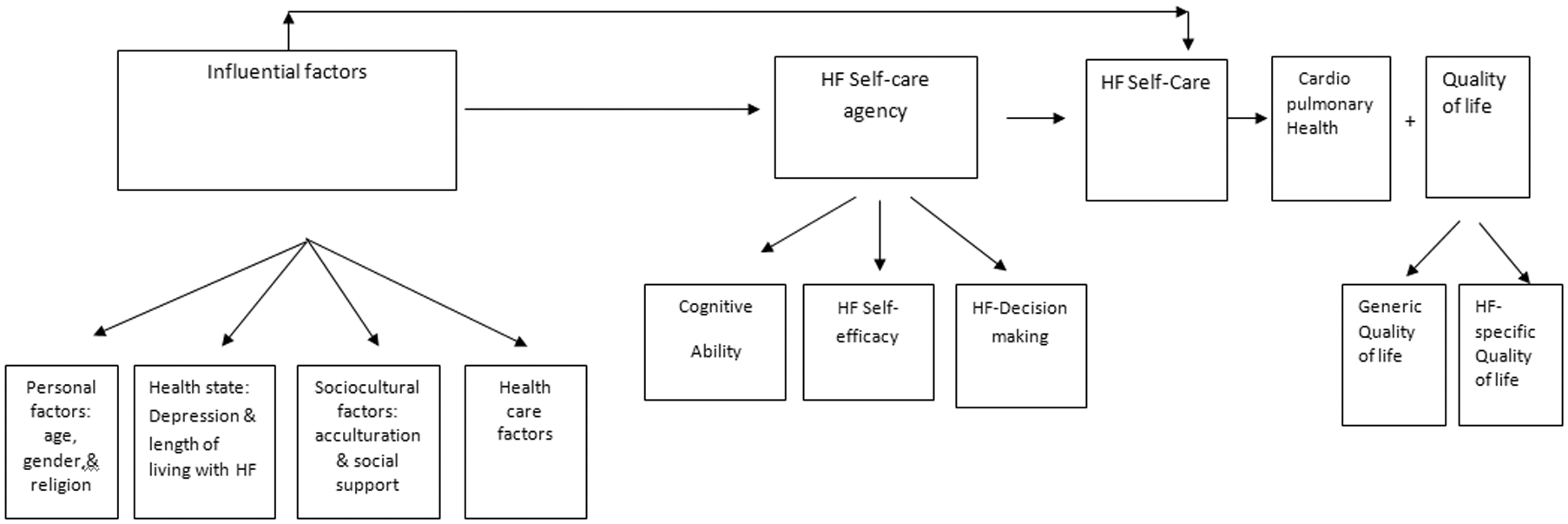
Pictorial Representation of the Middle-Range Theory of Heart Failure Self-Care.
Purpose and Research Questions
The purpose of this study was to test the MRT of HF self-care within a sample of Arab American older adults. Particularly, the study addressed the following questions:
Q1: What are the relationships among the influential factors (personal, sociocultural, health state, and health care factors) and the level of self-care agency?
Q2: What is the relationship between HF self-care agency (cognitive ability, HF decision-making, and HF self-efficacy) and HF self-care?
Q3: What is the relationship between HF self-care and level of cardiopulmonary health?
Q4: What is the relationship between HF self-care and level of QOL?
Q5:What are the relationships among the influential factors (personal, sociocultural, health state, and health-care factors) and HF self-care?
Methodology
Design and Sampling Plan
In this descriptive, correlational study, a nonprobability, convenience sampling plan was used to recruit Arab American older adults with HF. Inclusion criteria were (a) a confirmed diagnosis of HF by a cardiologist, (b) between 65 and 85 years of age, (c) ability to read and speak in English or Arabic, and (d) self-identified as Arab American. Exclusion criteria were (a) enrolled in a special interventional program to improve self-care, (b) diagnosed with a confirmed cognitive impairment or a neurovascular deficit, and/or (c) cognitive decline based on the Montreal Cognitive Assessment instrument (MoCA; Nasreddine et al., 2005).
Following Institutional Review Board (IRB) approval, participants were recruited from four cardiology clinics in metropolitan Detroit. The bilingual principal investigator (PI) was available in each of the clinics one day a week. While in the clinic, the cardiologists referred potential participants to the researcher. Interested participants met with the researcher in a private room within the clinic where the researcher explained the study procedures and obtained informed written consent. After obtaining consent, cognitive screening was done. Participants had to score 19 or higher on the MoCA (Nasreddine et al., 2005) to continue in the study. Participants were then given the option of completing self-report measures in English or Arabic language. All participants chose the Arabic versions of the scales described below.
Instruments and Measures
Instruments for Influential Factors
Instruments to assess HF influential factors include a personal survey, health care index, the Center for Epidemiological Studies-Depression Scale-10 (CES-D-10; Andresen, Malmgren, Carter, & Patrick, 1994), Arabic-Speaking Patients’ Acculturation Scale (ASPAS; Rissel, 1997), and Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, 1991).
Personal Survey
Personal factors were measured by the personal survey. This survey was developed by the PI to obtain demographic information about age, gender, religion, and length of time living with HF.
Health Care Index
Health care-related factors were measured by the health care index, which consisted of seven questions developed by the PI that collected information about having (a) health insurance, (b) preference for an Arabic health care provider, (c) access to an Arabic health care provider, (d) preference for information regarding HF in the Arabic language, (e) access to information regarding HF in the Arabic language, (f) satisfaction with HF care, and (g) the profession of the most frequently seen care provider for HF (nurse practitioner or cardiologist). The participants’ responses were either yes or no for the seven questions. The total score range was from 0 to 7; a no response was scored 0 and a yes response was scored 1. Higher total scores indicated increased preference for and access to Arabic-specific health care information and providers.
The ASPAS
The Arabic version of the ASPAS (Al-Atiyyat, 2009) was used to measure participants’ acculturation level. The scores range from 8 to 33, with a score of 21 or more indicating higher levels of acculturation to mainstream U.S. culture (Al-Atiyyat, 2009). The Arabic version of the scale showed good internal consistency, with a Cronbach’s alpha of 0.85 in this sample.
The CES-D-10
Depressive symptomatology was measured using the Arabic version of the CES-D-10 (Andresen et al., 1994). Possible scores on CES-D-10 range from 0 to 30, with a cutoff score of 10 or higher indicating significant depressive symptoms (Andresen et al., 1994). In this study, Cronbach’s alpha for the Arabic version of the CES-D-10 was 0.88.
The MOS Social Support Survey
The MOS Social Support Survey (Sherbourne & Stewart, 1991) was translated into Arabic for this study. The possible total score ranges from 19 to 95 (Sherbourne & Stewart, 1991). The higher the total score, the higher their level of social support. The translated Arabic version was found to have high internal consistency reliability, with a Cronbach’s alpha of 0.96.
Instruments for HF Self-Care Agency
Instruments to assess HF self-care agency included the MoCA (Nasreddine et al., 2005) and the HF Self-Confidence and Self-Management subscales of the Heart Failure Self-Care Index (HFSCI; Riegel et al., 2004).
The MoCA
The available Arabic version of the MoCA (Nasreddine et al., 2005) was used to assess the participants’ cognitive abilities. Total scores range from 0 to 30, with scores of 26 and higher indicating good cognition and a score of 18 or less indicating moderate to severe impairment (Nasreddine et al., 2005). Participants had to score 19 or higher to be included in the study.
The Self-Care Management Subscale of the HFSCI
The Self-Care Management Subscale of the HFSCI (Riegel et al., 2004) was translated into Arabic and used to measure HF decision-making. High scores indicate a high level of decision-making (Riegel et al., 2004). The Arabic version of this subscale demonstrated a good level of reliability (α = 0.77).
The Self-Confidence Subscale of the Heart Failure Self Care Index
The Self-Confidence subscale of the HFSCI (Riegel et al., 2004) was translated into Arabic and used to measure HF self-efficacy. High scores indicate a high level of HF self-efficacy (Riegel et al., 2004). Administering the Arabic version of this subscale showed a high level of internal consistency reliability (α = 0.92).
Instruments for HF Self-Care
To measure HF self-care, the European Heart Failure Self-Care Behavior Scale (EHFScB-12; Jaarsma et al., 2003) was administered. In addition, two items from the HF self-care scale that was used in the study by Artinian, Magnan, Sloan, and Lange (2002) were employed. These additional questions were needed to ensure that all of the health-deviation requisites described by Orem (2001) were assessed in this study. The two added questions were about (a) believing that HF is a condition to which an individual can adjust and (b) talking to the doctor and family about the individual’s condition to make plans for the future (Artinian et al., 2002). For this study, EHFScB-12 and the added two questions were translated to Arabic. The combined questions showed good internal consistency reliability (α = 0 .77).
Instruments for QOL
Two types of QOL were examined in the proposed study. These types are generic and HF-specific QOL.
The Short Form Health Survey–8 (SF-8)
The Arabic version of the SF-8 (Ware, Kosinski, Dewey, & Gandek, 2001) was used to measure generic QOL based on participants’ physical and mental health. Scores on the SF-8 were calculated to provide a physical component summary score for physical health as well as a mental component summary score for mental health (Ware et al., 2001). Higher scores indicate participants have better perceptions of their physical and mental health. The available Arabic version had high internal consistency reliability for the overall instrument, with a Cronbach’s alpha of 0.93 in the current sample.
The Kansas City Cardiomyopathy Questionnaire (KCCQ)
HF-specific QOL was measured using the KCCQ, with possible total scores ranging from 0 to 100 (KCCQ-12; Jones et al., 2013). Higher scores on this scale reflect higher levels of HF-specific QOL. The available Arabic version that was used in this study had a Cronbach’s alpha of 0.94.
Physiologic Measures
Four physiologic measures were used to assess cardiopulmonary health. These measures included heart rate, blood pressure (BP), respiratory rate, and the 6-minute walk test. Participants’ heart rate and BP were measured using the Omron HEM 907XL digital BP monitor. Respiratory rates were obtained manually. Using the guidelines of the American Thoracic Society (Holland et al., 2014), a 6-minute walk test was performed within the cardiologists’ clinic space. The researcher made sure that the participants’ BP, respiration, and pulse were within safety parameters for performing the walk test (Holland et al., 2014). For the 6-minute walk test, the dichotomous categories are good cardiopulmonary status (0), associated with a walk distance between 310 and 427 meters, and impaired cardiopulmonary status (1), associated with a distance less than 310 m. The results for the other measures were also dichotomous scores of 0 and 1. These results were combined and recorded as a cardiopulmonary index with scores of 0 to 4, with higher scores indicating poorer cardiopulmonary health.
Procedure
Once consented, eligible participants (those with MoCA scores 19 or greater) had their heart rate, BP, respiratory rate, and distance walked in 6 minutes measured. All walk tests were performed within a safe zone at the cardiology clinic where a rapid and appropriate response to emergency was possible. Then, the participants completed the self-report instruments. Based on the participants’ stated preferences, the Arabic versions of the instruments were administered in an interview format to all participants. Upon completion, participants received a $20 gift card to CVS pharmacy as a “thank you” for their time.
Data Analysis
Before running data analyses, data cleaning was conducted. Descriptive statistics (frequencies and means) were computed to describe the characteristics of the sample. Structural equation modeling (SEM), using the latest version of AMOS, tested the proposed MRT of HF self-care. SEM was chosen because it examines the covariance and correlations among the independent and dependent variables to determine if the hypothesized relationships between concepts within the model are supported (Byrne, 2013).
Four indices were used to measure model fit: chi-square (χ2), the chi-square minimum value of discrepancy divided by its degrees of freedom (CMIN/df), the comparative fit index (CFI), and the Root Mean Square Error of Approximation (RMSEA). A nonsignificant chi-square, CMIN/df values lower than 2, a CFI value equal to or greater than .95, and a RMSEA value ≤ .05 are recommended for a good fit (Byrne, 2013). However, an RMSEA value between .05 and .08 is considered reasonable (Byrne, 2013). When the model did not achieve good fit, modification indices, combined with theoretical considerations, were used to improve model fit. Finally, parameter adequacy, appropriateness of standard errors, and the statistical significance of parameter estimates were assessed. The parameters of the model are acceptable and adequate when estimated values of the correlations are not greater than 1.00, all the variances are positive, and covariance or correlation matrices are positive (Byrne, 2013).
Results
Sample Description
Demographic Data
The 175 participants ranged in age from 65 to 82 years (Mdn = 69 years), and the majority were married (78.3%) and Muslim (86.9%). Participants were fairly evenly split by gender; results revealed several significant gender differences. Specifically, male participants were significantly older than females, t(173) = 2.94, p = .004, had been living in the United States for a longer period of time, t(173) = 2.59, p < .01, and had a higher level of education, t(173) = 4.02, p < .001. Most participants had HF Class II or III (82.9%). There were no gender differences in the HF class and the length of time living with HF among participants (Table 1).
Demographic Characteristics of the Sample by Gender (N = 175).
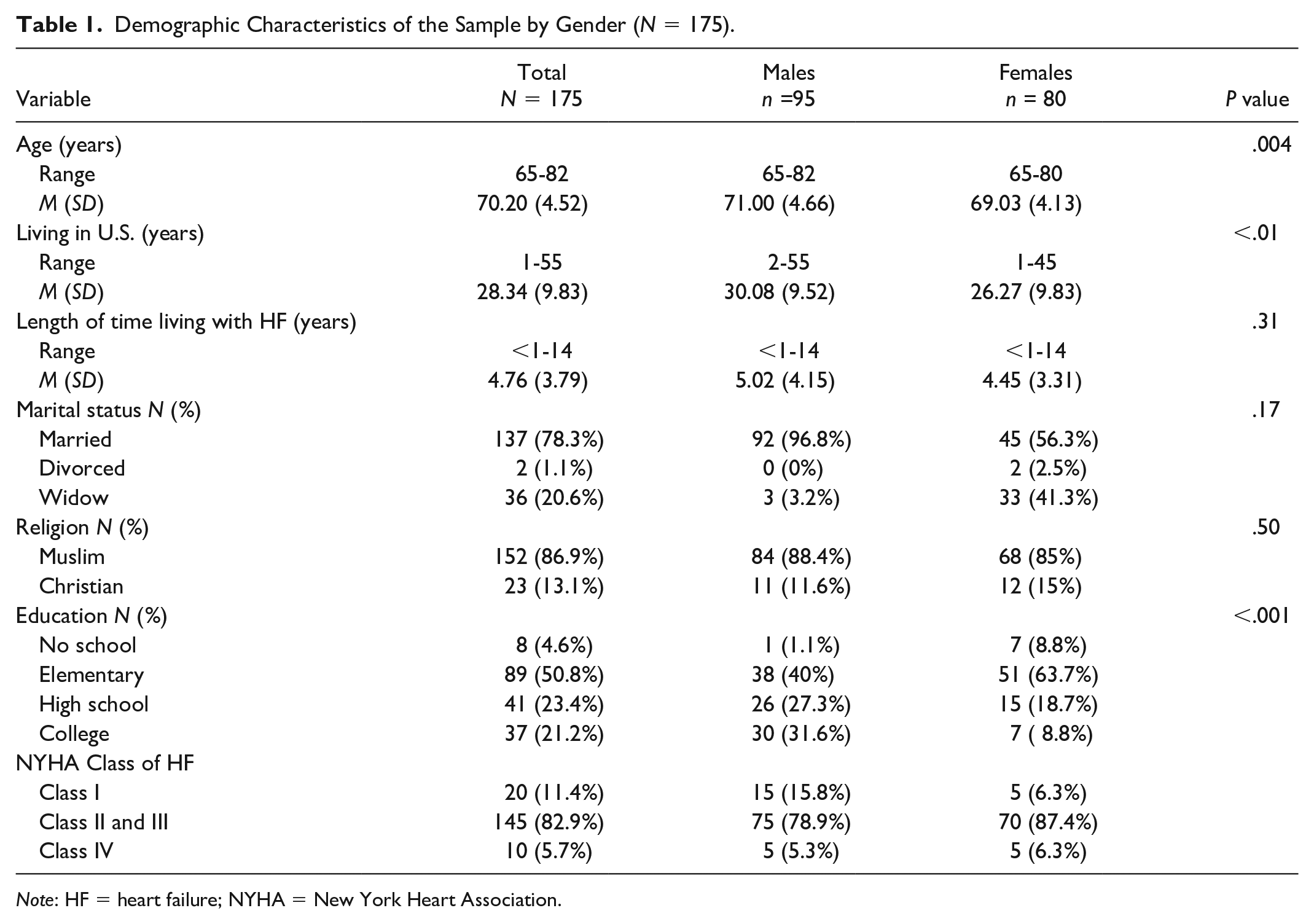
Note: HF = heart failure; NYHA = New York Heart Association.
Cardiopulmonary Health
The participants’ cardiopulmonary health was reported using the cardiopulmonary health index. The participants had good cardiopulmonary health (males: M = 0.77, SD = 0.89; females: M = 0.98, SD = 0.90) with no significant gender differences (p = 0.13).
Health Care-Related Factors
The participants’ health care-related factors were reported using the health care index. There was no variability in health care-related factors since all the participants had health insurance, preferred and had access to Arabic health care providers, and preferred and had access to HF information in the Arabic language. Given the lack of variance, health care-related factors were not included in the analysis.
Theoretical Variables
The variables of the MRT of HF measured by self-reported tools included HF influential factors, HF self-care agency, HF self-care, and QOL. Gender differences for all these variables are presented in table 2.
Description of the Variables of the Middle-Range Theory of Heart Failure.
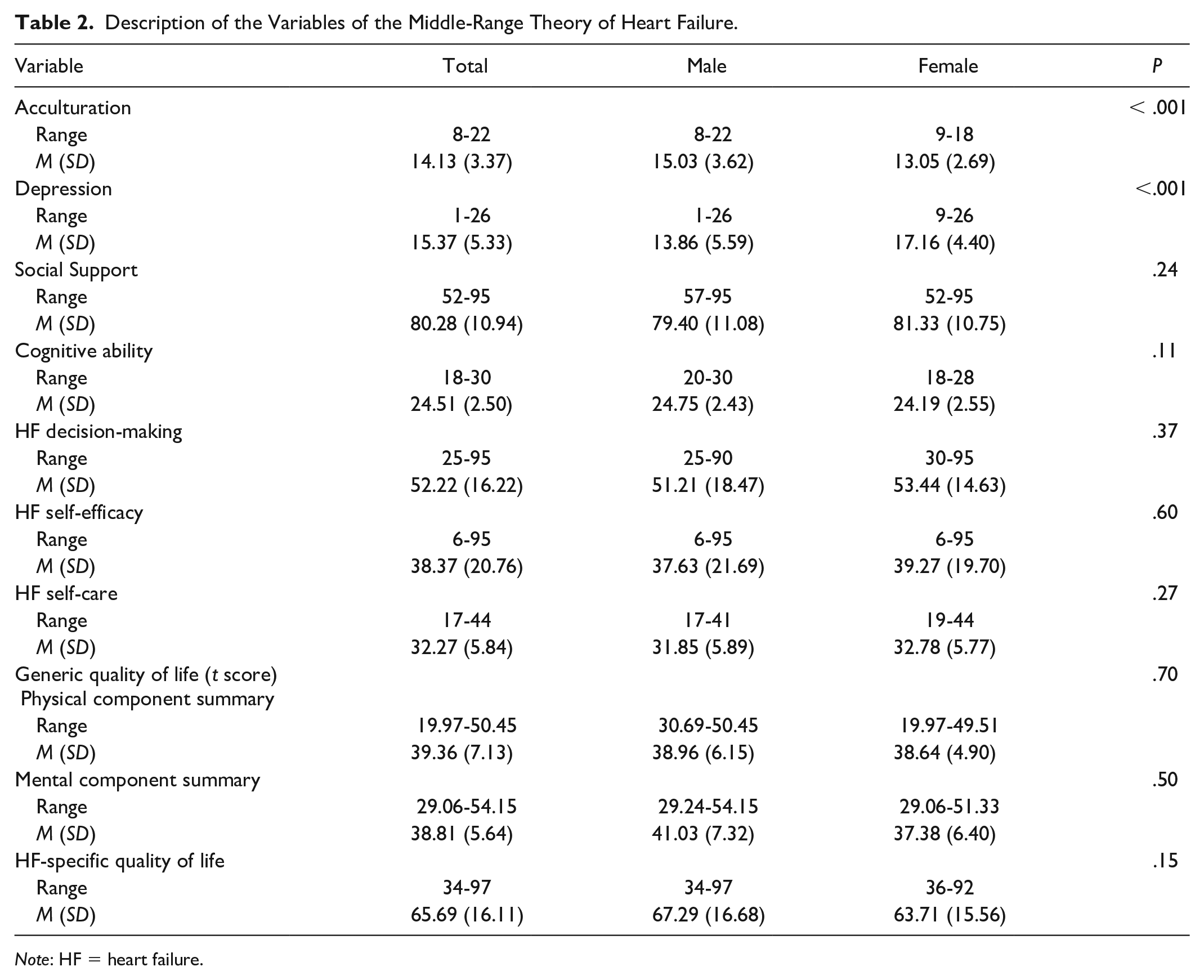
Note: HF = heart failure.
Influential factors included acculturation, depression, and social support. In this study, the participants’ acculturation level did not indicate a high acculturation level. Also, males were more highly acculturated than females, t(170.43) = 4.14, p < .001. The results of this study showed that 48% (n = 84) of Arab American older adults with HF reported high levels of depressive symptoms. Females reported significantly higher mean level of depression than males, t(172.25) = 4.36, p < .001. The results indicated a high level of social support among both male and female Arab American older adults with HF (p = .24; males: M = 79.40, SD = 11.08; females: M = 81.33, SD = 10.75) (Table 2).
HF self-care agency included cognitive ability, HF decision-making, and HF self-efficacy. The majority of participants (61.7%, n = 108) had moderately good cognition (scores 19-25). There was no significant difference in the mean cognitive ability between males and females (p = .11; males: M = 24.75, SD = 2.43; females: M = 24.19, SD = 2.55). Arab American older adults with HF had a low level of both HF decision-making and HF self-efficacy. There was no significant gender difference in the mean level of HF decision-making (p = .37; M = 51.21, SD = 18.47 men; M = 53.44, SD = 14.63 women) and in the mean level of HF self-efficacy (p = .60; males: M = 37.63, SD = 21.69; females: M = 39.27, SD = 19.70) (Table 2).
In this study, the mean total score for EHFScB-12 with the addition of the two questions from the study of Artinian et al. (2002) was 32.27 (SD = 5.84). There were no significant gender differences in HF self-care; both men and women had similar levels of HF self-care (p = .27; males: M = 31.85, SD = 5.89; females: M = 32.78, SD = 5.77) (Table 2).
Two different measures of QOL were used in this study (generic QOL and HF-specific QOL). Generic QOL had physical and mental components (Ware et al., 2001). The final scores for the physical and mental component summary is a t score, which is standardized using the means and standard deviations from the 1998 and the 2009 U.S. general population (Ware et al., 2001). Since mean t scores for the participants were less than 50 on both physical and mental components, the participants in this study had a lower level of QOL than the U.S. general population. In this study, the participants had a good level of HF-specific QOL with no significant gender differences (p = . 15; males: M = 67.29, SD = 16.68; females: M = 63.71, SD = 15.56).
Testing Model Fit
A two-step SEM analysis was conducted. The measurement model was tested before testing the structural model (Byrne, 2013).
Measurement Model
The initial measurement model had three latent variables: influential factors, HF self-care agency, and QOL. Influential factors had six indicators: gender, religion, social support, acculturation, depression, and length of time living with HF. The seventh hypothesized indicator, health care index, was deleted from this latent due to a lack of variance. Self-care agency had three indicators: cognitive ability, HF self-efficacy, and HF decision-making. QOL had two indicators: generic QOL and HF-specific QOL.
The fit indices for the initial measurement model indicated poor fit: chi-square 178.48, p ≤ .001, CMIN/df = 4.35, CFI = 0.78, and RMSEA = 0.14 (0.12-0.16). In addition, four of the indicators of the latent variable influential factors were not statistically significant and had low factor loadings: religion (β = 0.05, p = .39), acculturation (β = 0.14, p = .07), social support (β = 0.10, p = .16), and length of living with HF (β = 0.16, p = .07). Also, one indicator (depression) was significant but had a nonacceptable factor loading value (β = 1.20, p = .04). A second latent variable, HF self-care agency, had one indicator (cognitive ability) with a low factor loading value and was not significant (β = 0.11, p = .16). This was not unexpected given that participants had to score 19 or higher to participate, which restricted the range of this variable.
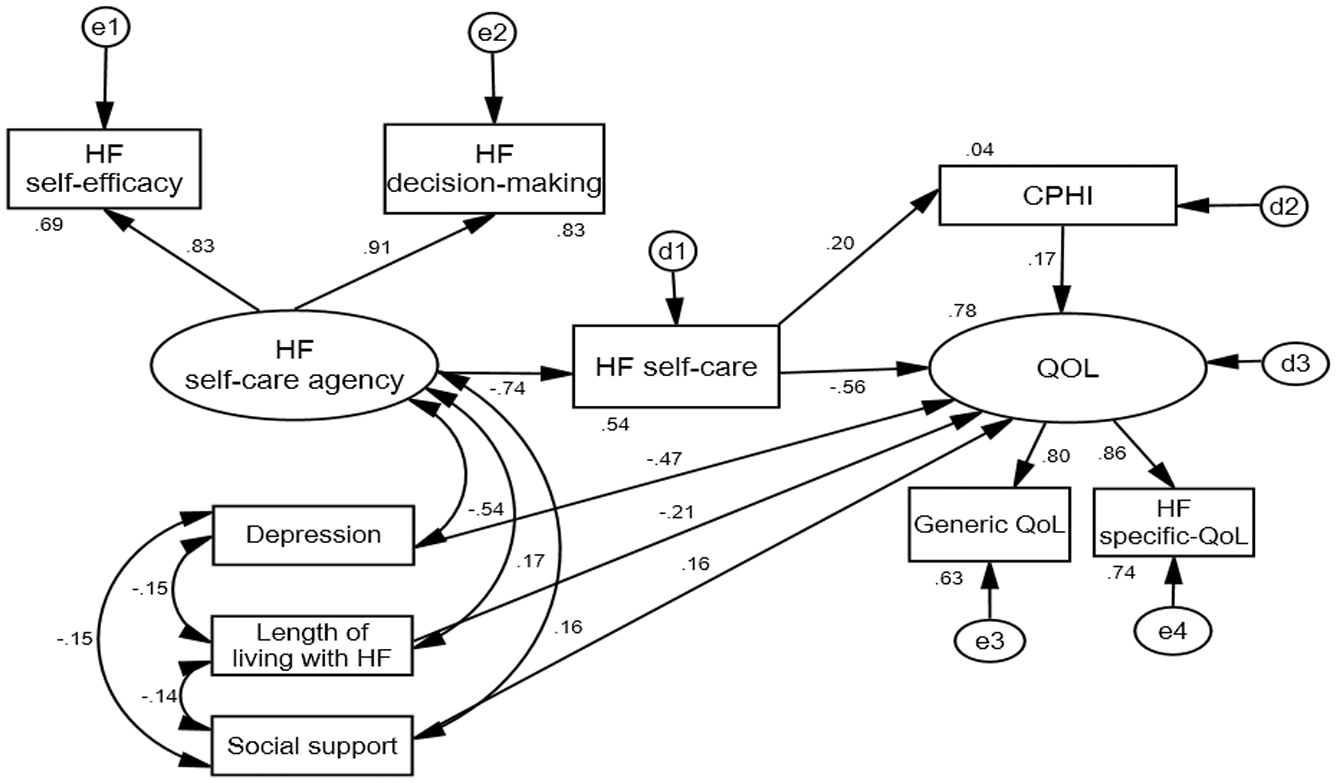
In order to improve the fit of the initial model, changes were made based on both statistical and theoretical considerations. Initially, indicators with a p value > .10 were deleted. Two additional measurement models were run, but neither achieved acceptable fit. After dropping cognitive ability from the HF self-care agency latent variable, issues of fit were all related to the latent variable of influential factors. Although theoretically important as predictors of self-care agency, the indicators did not support the underlying latent variable (influential factors). Thus, in the final measurement model (Figure 2), the latent variable of influential factors was deleted, resulting in good model fit:χ2 = 2.37, p = .37, CMIN/df = 0.79, CFI = 1.00 and RMSEA = 0.00 (0.00-0.19) (Table 3).
The Final Measurement Model.
Fit Indices of Measurement Models.
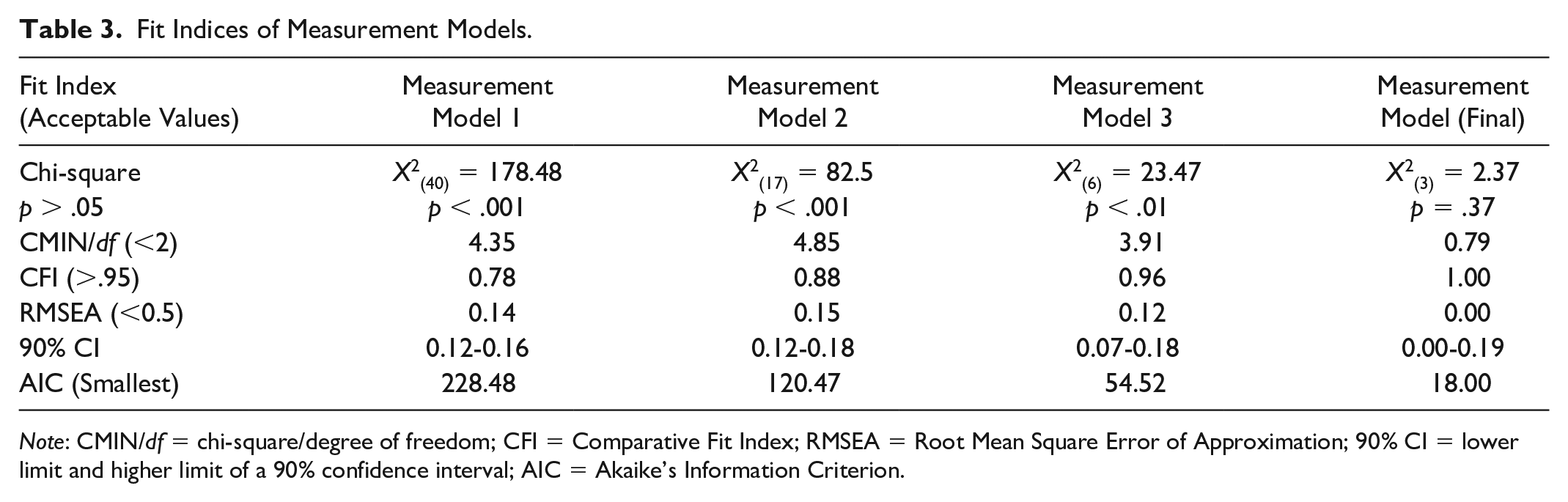
Note: CMIN/df = chi-square/degree of freedom; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation; 90% CI = lower limit and higher limit of a 90% confidence interval; AIC = Akaike’s Information Criterion.
Structural Model
Based on the results of the measurement model testing, it was clear that the latent variable of influential factors needed to be deleted from the proposed structural model. However, indicators of influential factors are theoretically important, so decisions needed to be made as to how to model these indicators. Using the analytic strategy of structural modeling with prespecified covariates (Byrne, 2013), the following changes were made. Three indicators with low factor loadings were deleted from further SEM analysis: religion (β = 0.05, p = .39), acculturation (β = 0.14, p = .07), and gender (β = 0.22, p = .04). Acculturation and religion were dropped not only because of nonsignificant and low factor loadings but also due to a restricted range of the participants’ responses (see Table 2).
Since there were significant gender differences noted in the sample characteristics, instead of using gender as a covariate, it was decided to conduct multigroup SEM analysis. Multigroup analysis allowed us to determine if the final model fit differently in men and women.
The three remaining indicators of the latent variable influential factors (i.e., social support, depression, and length of time living with HF) were modeled as additional exogenous variables. These variables were treated as covariates of each other as well as with the latent variable HF self-care agency. This covariation was based on a statistical perspective, as the three factors were highly correlated with each other during measurement model testing. Further, the association between these three indicators and the latent variable HF self-care agency is empirically supported (Goodman et al., 2013; Gowani et al., 2017; Riegel et al., 2016). In addition, empirical evidence supported allowing social support, depression, and length of living with HF to be modeled as having a direct as well as an indirect relationship with QOL.
The latent variable of HF self-care agency was modeled with two indicators: HF decision making and HF self-efficacy. The indicator cognitive ability was deleted during measurement model testing given its nonsignificant and low factor loading (β = 0.11, p = .16). Finally, QOL was left as originally proposed, with both generic and HF-specific QOL having strong loadings on the latent variable. Figure 3 shows the structural model that was tested following changes made based on measurement model results. Fit indices indicated poor fit (Table 4).
The Modified Structural Model Based on Measurement Model Results.
Fit Indices of Structural Models.
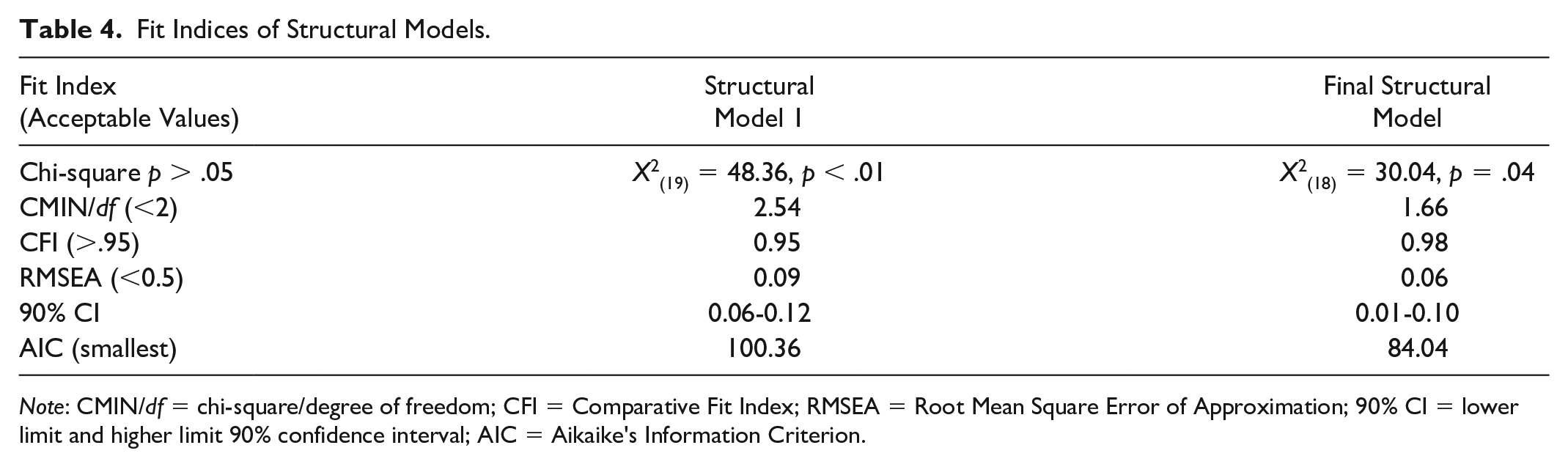
Note: CMIN/df = chi-square/degree of freedom; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation; 90% CI = lower limit and higher limit 90% confidence interval; AIC = Aikaike's Information Criterion.
The Final Structural Model
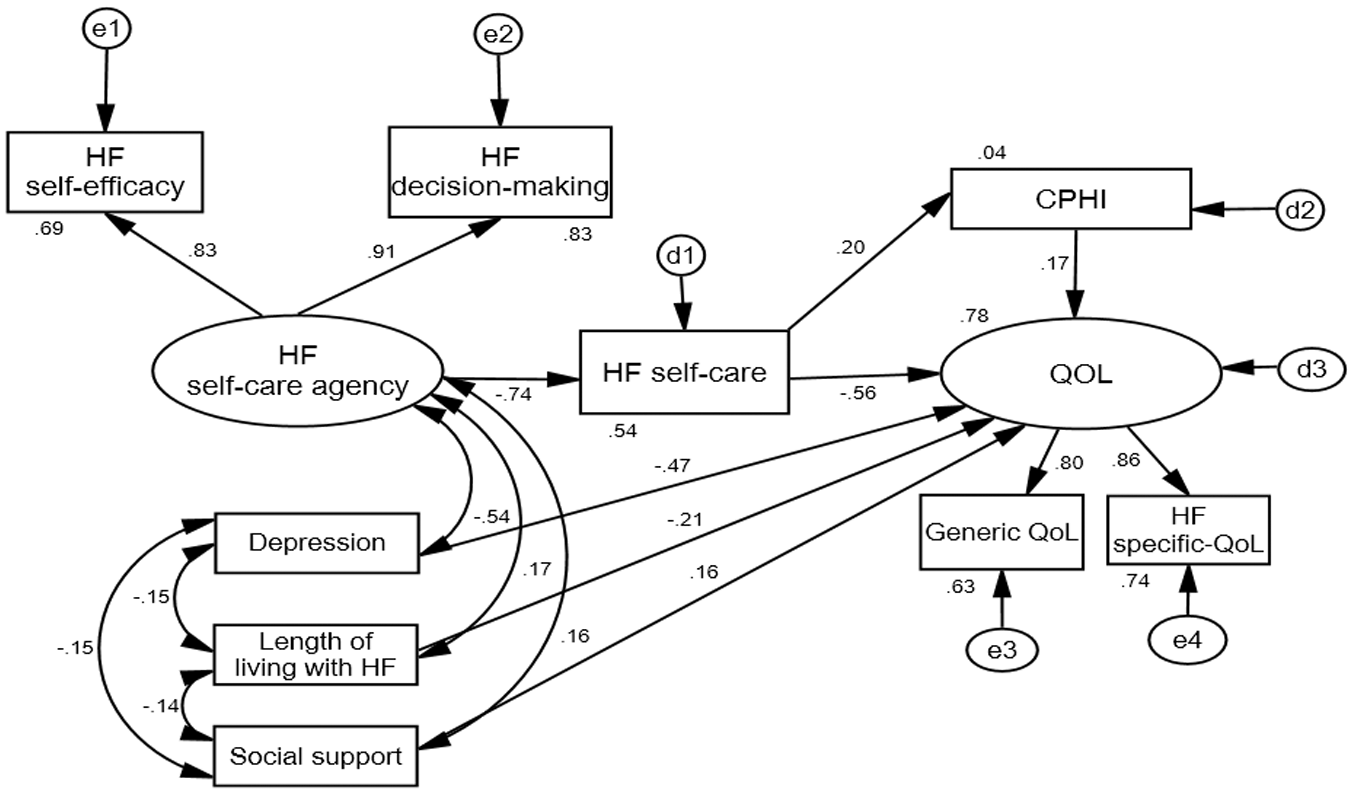
Based on results of initial structural model testing, modification indices were assessed for potential changes to a second structural model. Only one change was needed and that was to allow a correlation between e1 and d3 (error terms). After adding the correlation between e1 and d3, the fit indices were as follows: chi-square = 30.04, p = .04, CMIN/df = 1.66, CFI = 0.98, and RMSEA = .06 with 90% (0.01-0.10) (Table 4). All of the fit indices indicated good fit except for chi-square. Often it is difficult to achieve a nonsignificant chi-square due to its sensitivity to sample size. This is why CMIN/df is always reported (Byrne, 2013). The correlation between the errors e1 and d3 suggests that there is a possibility of unmeasured variables not included in the model between HF self-care agency and QOL. Finally, parameter adequacy, appropriateness of standard errors, and the statistical significance of parameter estimates were assessed and showed that the model met these criteria. Thus, this final structural model achieved good fit. A diagram of the final model with standardized regression weights is presented in figure 4.
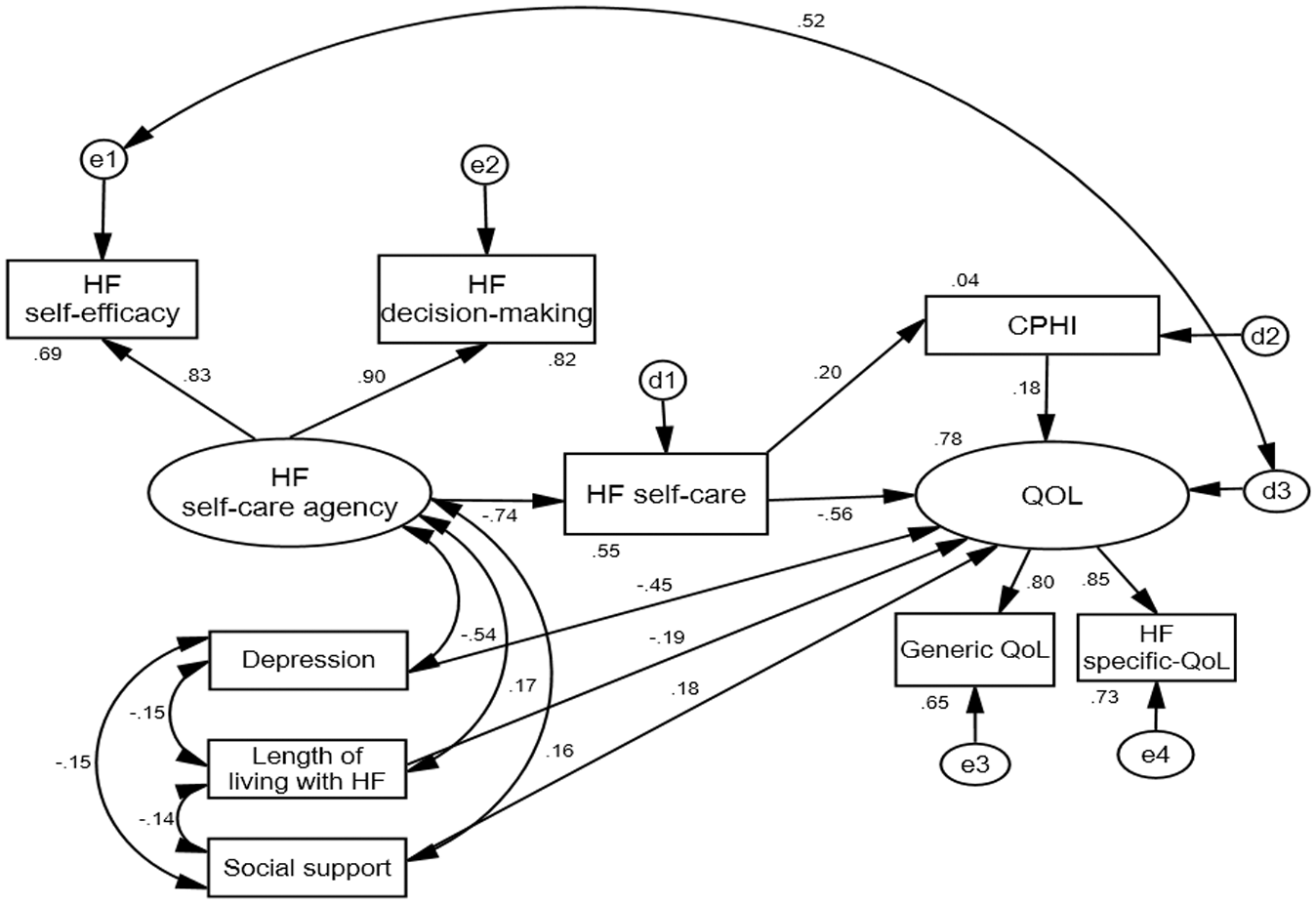
The Final Model for MRT of HF Self-Care.
Testing the Relationships in the Final Model
The Relationship Among Influential Factors and HF Self-Care Agency
The relationship between the latent variable of influential factors and the latent variable of HF self-care agency was not able to be tested. Measurement model results did not support the conceptualization of influential factors as a single latent variable. Thus, the structural model was revised to allow three indicators of influential factors (depression, social support, and length of time living with HF) to be considered as covariates, with a direct path to HF self-care agency. Results revealed that each of those variables had a significant association with HF self-care agency. Depression had a moderate, negative association with HF self-care agency (β = 0.54, p < .01). Both social support and period of living with HF were positively and weakly associated with HF self-care agency (β = 0.16, p = .04, and β = 0.17, p = .04, respectively).
The Relationship Between HF Self-Care Agency and HF Self-Care
HF self-care agency had a significant negative relationship with HF self-care (β = -0.74, p < .01). Taking into consideration that lower scores of HF self-care mean better adherence to HF self-care, the result indicated that patients with higher levels of HF self-care agency (i.e., HF self-efficacy and HF decision-making) had higher levels of HF self-care. However, the indicator cognitive ability was deleted from the final structural model based on the results of testing the measurement model. Cognitive ability had a nonsignificant and low factor loading on the latent variable HF self-care agency (β = 0.11, p = .16).
The Relationship Between HF Self-Care and the Level of Cardiopulmonary Health
It was found that HF self-care has a significant positive relationship with scores on the cardiopulmonary health index (β = 0.22, p < .01). Since lower scores in both HF self-care and cardiopulmonary health mean high levels of HF self-care and cardiopulmonary health, this positive relationship indicated that participants with higher HF self-care had better levels of cardiopulmonary health.
The Relationship Between HF Self-Care and the Level of QOL
HF self-care was found to have negative relationship with the latent variable QOL (β =- 0.56, p < .01). Taking into consideration that lower scores of HF self-care mean better adherence to HF self-care, high levels of self-care are associated with a higher level of QOL.
The Relationship Among Social Support, Depression, and Period of Time Living With HF and QOL
Direct effects of social support, depression, and living with HF on QOL were found. Social support had a weak, positive relationship with QOL (β = 0.18, p < .01). On the other hand, depression had a moderately strong negative relationship with QOL (β = -0.45, p < .01), and length of time living with HF had a weak, negative relationship with QOL (β = -0.19, p < .01).
Multigroup SEM Analysis
When the model was run using multigroup SEM analysis, the model fit indices were calculated as follows: CMIN/df = 2.00, CFI = 0.93, and RMSEA = 0.08 (0.05-0.09). These model indices were considered acceptable, so the researcher proceeded to examine differences between groups (males and females). In multigroup SEM analysis,CMIN is used to determine if there are group differences (Byrne, 2013). A significant CMIN indicates significant group difference between males and females. The CMIN for this study analysis was 19.41 (p = .004).
To find the exact significant differences between groups (males and females), the critical ratio for differences between parameters was used. In this analysis, any value that was greater than 1.96 indicates a significant difference between the groups (Byrne, 2013). Significant differences between males and females were only found in the influence of cardiopulmonary health on QOL. The critical ratio for differences was 2.05, with cardiopulmonary health having a stronger influence on QOL for females than males (β = 0.19 and β = 0.16, respectively).
Discussion
The major findings from this study provide important theoretical considerations when using the self-care deficit theory of nursing (SCDTN; Orem, 2001) to understand self-management of chronic diseases. Specifically, results revealed that BCFs did not fit when conceptualized as a single latent variable and that some BCFs have a direct as well as indirect path to QOL outcomes.
Influential Factors as a Latent Variable
Within this MRT of HF self-care, influential factors were derived from basic conditioning factors (BCFs) and proposed as a latent variable with seven indicators that included gender, religion, depression, social support, acculturation, length of time living with HF, and health care system factors. Reviewing the HF literature showed that this is the first time that BCFs were conceptualized as a single latent variable based on the SCDNT (Orem, 2001). Although some researchers used SCNDT (Orem, 2001) in developing middle-range theories, instruments, and interventional programs, only one other study was found that conceptualized BCFs as a latent variable. That study conceptualized BCFs as a second-order factor comprised of three separate latent variables (named Factors I, II, and III) with a total of six indicators (McQuiston & Campbell, 1997). After testing the theory in a sample of women at risk for sexually transmitted infections, three indicators (socioeconomic status, health state, and influence in the relationship) stayed in the theory. This suggests that for the MRT of HF, the single latent variable of influential factors may need to be reconceptualized as a second-order latent variable in future testing.
In the current study, three indicators of influential factors (depression, social support, and length of time living with HF) needed to be modeled as additional exogenous variables that correlated with HF self-care agency. The relationships of those three indicators to HF self-care agency (decision-making and self-efficacy) are described below, with comparisons to other studies.
Influential Factors and Self-Care Agency
This is the first study to model HF self-care agency as a latent variable that included HF self-efficacy and HF decision-making as indicators of agency. Previous research studies examined these predictors of HF self-care separately. However, their results were similar to the results of this study.
In the current study, there was a moderate negative correlation between depression and the latent variable of HF self-care agency. Similarly, other studies also found a negative relationship between depression and HF decision-making and self-efficacy (Goodman et al., 2013; Riegel et al., 2016).
The results of the current study showed a weak positive correlation between social support and HF self-care agency. This was consistent with other studies in which social support was found to have a significant positive association with both HF decision-making and self-efficacy (Gowani et al., 2017; Riegel et al., 2016).
There was a weak positive correlation between length of time living with HF and HF self-care agency. These results reflect other study findings in which length of living with HF was found to have a significant positive association with HF self-care agency (Cocchieri et al., 2015; Riegel et al., 2016). Results seem to indicate that experience gained through living longer with HF provides the opportunity to gain the required knowledge and skills for performing HF self-care (Riegel et al., 2016).
Influential Factors and QOL
Reviewing the literature provided empirical evidence for the need for a linkage between the influential factors and the QOL in this MRT of HF self-care. Previous studies examined the influence of many factors on the QOL among older adults with HF. Several studies found significant associations between QOL and depression, social support, and the length of time living with HF (Alaloul et al., 2017; Seah, Tan, Huang Gan, & Wang, 2016). In the current study, three indicators of influential factors (depression, social support, and length of time living with HF) had a significant relationship with QOL. Thus, current study results support the need to add pathways between influential factors (depression, social support, and length of living with HF) and QOL in order to fully understand QOL for patients with HF.
In this study, QOL was conceptualized as a latent variable that included generic QOL and HF-specific QOL. Depression had a negative relationship with QOL, where social support and length of time living with HF had a positive relationship with QOL. Reviewing the literature revealed similar findings in that depression was negatively associated with HF-specific QOL among older adults with HF (Auld et al., 2018), while social support, as measured by MOS, was found to have a positive influence on generic QOL (Alaloul et al., 2017).
Although the previous studies examined the influence of the influential factors on generic QOL and HF-specific QOL separately, their results were similar to the current study, which examined QOL as a latent variable. Also, the fact that previous studies examined different types of QOL and its predictors, but excluded self-care behaviors, confirmed the need for the MRT of HF self-care. Based on a self-care conceptual framework, this MRT defines overall QOL as being comprised of both generic and HF-specific QOL and also proposes theoretically based relationships between QOL and the factors that influence it among persons with HF.
HF Self-Care Agency and HF Self-Care
The proposed relationship between HF self-care agency and HF self-care was supported in this test of the MRT of HF self-care. Findings revealed that HF self-care agency had a strong, positive relationship with HF self-care.
To our knowledge, this is the first time that the concept of HF self-care agency was conceptualized and tested as a latent variable with three indicators: HF self-efficacy, HF decision-making, and cognitive ability. The fact that cognitive ability did not perform well in this study could be due to the instrument that was used to measure the participants’ cognitive status. Although MoCA is a selective and sensitive tool in identifying patients with cognitive impairments (Nasreddine et al., 2005), it is still a screening tool. More specific neuropsychological tests may be required to capture the cognitive ability that is needed for HF self-care agency. In addition, there was a restricted range of MoCA scores as participants had to score at least 19 in order to be eligible to participate in this study.
The positive relationship between HF self-care agency (HF self-efficacy and HF decision-making) and HF self-care found in this current study is consistent with previous research studies, even though the previous studies examined the HF self-care agency indicators separately. Higher levels of self-efficacy (Goodman et al., 2013) and decision-making have been found to have a positive influence on self-care among older adults with HF (Al-Sutari & Ahmad, 2017). These significant relationships between HF decision-making and HF self-efficacy with HF self-care bring to our attention the need to improve patients’ self-care agency to help them improve their HF self-care behaviors.
HF Self-Care and Cardiopulmonary Health
Arab American older adults with HF who had a high adherence level with HF self-care behaviors had higher levels of cardiopulmonary health. The relationship between HF self-care and health status has been examined primarily through interventional programs. Those studies have demonstrated improved health outcomes, including improved cardiovascular function (Zhang et al., 2016), and decreased frequency of emergency department visits (Al-Sutari & Ahmad, 2017). Although the current study used a cardiopulmonary index to measure health status and the previous studies used different, separated methods to measure health status, the findings of the current study are consistent with prior findings suggesting that high levels of HF self-care have a positive influence on health status.
HF Self-Care and QOL
In this study, participants with higher levels of adherence with HF self-care reported better generic, as well as HF-specific, QOL. In the literature, a positive relationship between HF self-care and both generic QOL and HF-specific QOL has been reported (Auld et al., 2018; Zhang et al., 2016). Furthermore, the positive influence of improved HF self-care on QOL has been reported in interventional studies that targeted HF self-care behaviors such as exercising regularly (Zhang et al., 2016).
Cardiopulmonary Health and QOL
The multigroup SEM results indicated a significant gender difference in the fit of the MRT. Specifically, cardiopulmonary health had a stronger influence on QOL for females than males. However, it is important to note that differences in the strength of the path are small and should be interpreted with caution.
The significant difference in the influence of cardiopulmonary health on QOL by gender could be because males and females with HF connect their QOL with different factors. Older, male individuals with HF tend to connect high QOL with being employed, having high income, having a pension, and having a partner (Baert et al., 2018). However, women may connect their QOL to other factors such as their physical health status (Baert et al., 2018).
Strengths and Limitations
This study is the first to test a comprehensive MRT of HF self-care. It is also the first to use latent variables to assess self-care agency and QOL. Although derived from the SCDNT, this study demonstrated the need for an additional pathway in the SCDNT from BCFs directly to health outcomes. This study also demonstrates that cultural considerations can be tested within a self-care perspective.
As with all studies, there are limitations in the current study that must be considered when interpreting study results. This study was conducted with a sample of older Arab Americans with HF. As such, results are not generalizable to younger, non-Arab individuals. Even among Arab Americans, all participants sought medical attention from an Arabic cardiologist. This limited the ability to test the influence of having a nonculturally congruent health care provider on HF self-care. Another limitation was not obtaining data regarding the participants’ country of origin. Although they may share common Arabic values, it is possible that beliefs about HF self-care may vary among the different Arab countries. Thus, country of origin should be considered in the future research.
Construct validity was an issue in this study; the influential factors did not work as a latent variable. This required the researcher to reconceptualize three indicators of influential factors as exogenous variables that correlated with the latent variable of HF self-care agency. Furthermore, these three indicators were also reconceptualized to directly influence QOL. The new relationships among the influential factors were supported in the last structural model. Although this reconceptualization is a limitation to construct validity, the results provide new insights for studying BCFs and HF influential factors in the future.
Implications
This study has research implications in which the results provide a different approach for studying HF self-care in terms of both influential factors and health outcomes. The need for a theoretically based model was supported; however, suggestions for modifications to the model are presented. These suggestions include conceptualizing influential factors as a second-order latent variable of BCFs rather than as a first-order latent variable and testing the direct relationship between influential factors and QOL. Furthermore, it is recommended that this MRT of HF self-care be tested in other ethnic groups as well as in European Americans.
Regarding clinical implications, understanding HF self-care and its influential factors can help in the development of interventional programs that can improve self-care among older adults with HF. Since HF self-care agency factors are significant predictors of HF self-care, health care providers may build interventional programs that improve HF decision-making and HF self-efficacy. Such programs may help to increase adherence to HF self-care among patients HF.
Conclusions
This study tested the MRT of HF self-care in an Arab American population. Although conceptualizing BCFs as a single latent variable was not supported, results supported other propositions in the MRT of HF self-care. The relationships among the concepts in the final MRT of HF self-care were found to be consistent with the previous studies. Results also demonstrated that increased peformance of HF self-care was associated with improved physical health and QOL.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Blue Cross Blue Shield of Michigan Foundation, Student Award Program (Grant Number 2376.SAP, 2017), and Wayne State University, the Graduate School Dissertation Research Support (2017).