
Abstract
The aim of this study was to gain a deeper understanding of the experience of Saudi informal family caregivers of hospitalized patients who have experienced a stroke. In-depth, face-to-face, semistructured interviews of five family caregivers using open-ended questions were conducted in a major hospital in Saudi Arabia. The interviews were recorded, transcribed verbatim, and analyzed using the unitary-caring hermeneutic phenomenological research method. Data analysis revealed six major essences that were synthesized into one statement reflecting the essence of caring for a family member with a stroke in Saudi Arabia: Living with the uncertainty of ambiguity amid feeling distressed with worries and fears replete with unfulfilled desires while yearning for compassionate caring and overcoming uncertainties through connections and faith honoring abiding commitments. As a means to transform the findings into theory and language of the nursing discipline, the essences were then interpreted within the theory of unitary caring.
Stroke, also called a cerebrovascular accident (CVA) or “brain attack,” is a global leading cause of death and disability (Teasell, Hussein, McClure, & Meyer, 2014). A 2017 study on the global prevalence of stroke found 104.2 million people globally and 795,000 people in the United States experience a new or recurrent stroke annually (Virani et al., 2020). The American Heart Association projects the total cost of stroke, which encompasses both direct and indirect spending, to increase from $105.2 billion in 2012 to $240.7 billion by 2030 (Katan & Luft, 2018). In 2019, stroke was identified as the third leading cause of death and a major cause of disability in Saudi Arabia (Global Burden of Diseases [GBD] and Injuries Collaborators, 2020). There is no recent single study that provides overall population-based stroke incidence and prevalence in Saudi Arabia; however, a few studies have provided a hospital-based annual incidence of stroke in different cities. For example, in the Asir region, an overall rough annual incidence rate of first-time hospitalized stroke persons was 57.64 per 100,000 persons (Alhazzani et al., 2018). In Al-Madinah city, the minimum incidence rate of first-time hospitalized stroke was 13.89 per 100,000 persons (Al-Shenqiti, Ibrahim, Khaled, Ali, & Ahmed, 2017).
Background
Stroke, unlike many other conditions, changes lives in an instant. The stroke survivor is not the only person impacted; family and close friends are as well. A family member can be a wife or husband one day and take on the role of a caregiver the next day. When writing about her mother’s stroke, British actress Mariam Margolyes vividly described how her life changed in an instant from her mother being a “vibrant, alert, shrewd, funny lady” to when “she turned into someone who could barely talk and was unable to move. It was the most terrible, shocking transformation you could imagine” (Margolyes, 2019, p. 4).
Because the nature of stroke disease is sudden and unexpected, family members often have little or no time to assume the caregiving role (Moon, 2017). Consequently, family caregivers report feelings of uncertainty, frustration, fear, and stress (Giosa, Stolee, Dupuis, Mock, & Santi, 2014; Moon, 2017). Thus, the caregivers’ needs are different from patients recovering from stroke and other sudden illnesses. The transition to home without adequate preparation often represents another stressful experience for patients and their family caregivers (Lutz, Young, Cox, Martz, & Creasy, 2011).
Informal family caregivers have an essential role in delivering care for stroke survivors postdischarge to home. An informal caregiver is generally an individual who provides unpaid, ongoing assistance with activities of daily living (ADLs) or instrumental activities of daily living (IADLs) to a person with illness or disability. The informal caregiver can be a spouse, adult child, other relative, or friend (Roth, Fredman, & Haley, 2015). In Saudi Arabia, it is well established that the participation of family members in caregiving for stroke survivors and other patients with disabilities has been widely practiced (Alshammari et al., 2017). Most of the family members are accompanied by their relatives with stroke during inpatient hospitalization because culturally, family caregiving is a strong Saudi tradition. Furthermore, the Islam religion motivates most Saudis to be compassionate and responsible for family members who are in need (Al-Mutair, Plummer, O’Brien, & Clerehan, 2014).
The physical, psychological, social, and financial burdens of informal caregiving are well documented in Saudi Arabia. Roughly 78.1% of the family caregivers of the elderly with disabilities suffered from physical problems, 69.2% had depression or mood swings, 74.9% of them reported work-related problems, and 14.3% had financial problems (Alshammari et al., 2017). Furthermore, a recent study by Alquwez and Alshahrani (2020) reported that approximately 53% of family caregivers of stroke survivors had depression and roughly 40.7% suffered from anxiety. Although these quantitative findings are instructive, they do not offer an empirical understanding of the essence of the family caregiver’s experience.
There is a growing body of phenomenological studies investigating the experience of family caregivers caring for persons who have experienced a stroke (Gertrude et al., 2019; Hesamzadeh et al., 2017; Qiu, Sit, & Koo, 2018; Zhang & Lee, 2019). However, none of these phenomenological studies were specific to family caregivers of the stroke survivors while still hospitalized, nor did any of the studies focus on caregivers of persons with a stroke in Saudi Arabia. More importantly, none of these studies used a caring nursing theory or a unitary caring science perspective as an interpretive lens for creating conceptual meaning of the findings.
Supporting caregivers is important toward enabling the family members to adopt the caregiving role and improve the health and well-being of both caregivers and care recipients (Chuluunbaatar, Chou, & Pu, 2016). In the absence of effective support, the caregiver may be at an increased risk of hospitalization, which may consequently increase the readmission of the patient, thereby increasing healthcare costs (Pauley, Chang, Wojtak, Seddon, & Hirdes, 2018). To provide comprehensive care and support for family members, healthcare professionals need a clear understanding of the experiences of family caregivers; this gap in our knowledge warrants additional study. Therefore, the focus of this study is on the lived experience of family caregivers of a member who is in the hospital after experiencing a stroke in Saudi Arabia.
Purpose and Significance
The purpose of this study was to (a) describe the experience of Saudi family members caring for a family member in the hospital after they have experienced a stroke as a means to gain a deeper understanding of the meaning of their experience and (b) interpret these findings from the perspective of Smith’s (2020) unitary caring theory as a means to advance nursing science and the application of unitary caring science. Understanding the experience of family caregivers using the lens of the unitary caring theory contributes to the body of nursing knowledge about the phenomenon of caring for a family member who has experienced a stroke.
Research Question
The research questions that guided this study were as follows: What is the meaning of the experience of caring for a family member hospitalized with a stoke in Saudi Arabia, and what is the meaning of this experience from the perspective of Smith’s unitary caring theory?
Researchers’ Perspective
In this study, the researchers were informed by Smith’s (2020) unitary caring theory. Smith’s (1999, 2020) unitary caring theory is situated within the unitary-transformative paradigm and was used to interpret the findings as a means to create a theoretical structure of the lived experience of family caregivers who are caring for a family member hospitalized after experiencing a stroke within a unitary nursing science perspective. Unitary caring theory was developed to describe the theoretical nature of caring within a unitary science perspective (Smith, 1999, 2020). Smith (1999) developed the theory using a rigorous process of concept clarification and a synthesis of literature from both caring and unitary science resulting in expressions of caring in language consistent with unitary science. The theory has a set of seven assumptions, five concepts, and propositions that are organized by concept. The five concepts describing unitary caring are manifesting intentions, appreciating pattern, attuning to dynamic flow, experiencing the infinite, and inviting creative emergence (Smith, 2020). Manifesting intentions is the process of “creating healing environments, commitment to alleviate another’s vulnerabilities, preserving dignity and humanity, and reverence for human life, love, and co-presence, expressing compassion and courage, and being an authentic presence” (Smith, 2020, p. 494). Appreciating pattern, the second concept in the theory, is the “apprehending and understanding the mysteries of human wholeness and diversity with awe” (Smith, 2020, p. 495). Pattern is reflected in meaning; thus, discovering what is meaningful to the other is essential to apprehending the pattern while appreciating the pattern coming to know the uniqueness and grasping the wholeness of another, not through analysis but by sensing, co-exploring experiences, and listening to the other’s story. Attuning to dynamic flow is “sensing where to place focus and attention in mutual process” (Smith, 2020, p. 496). Within the context of attuning to dynamic flow, “caring is flowing with the cocreated rhythms of relating in the moment” (p. 496). Attuning to dynamic flow is accomplished by being truly present in the moment and is a “back and forth movement of relationship building through a vibrational seeing of where to place focus and attention” (p. 496). Smith (2020) stated that caring “is not taking the lead and telling the person what he or she needs to do”; rather, caring is “understanding where the other wants to go and being with him or her through the struggle to get there” (p. 496). Experiencing the infinite is defined as a pandimensional awareness of coextensiveness with the universe in the context of human relation (Smith, 1999, 2020). Smith (2020) explained that experiencing the infinite “is the recognition that the nurse-person relationship is sacred, we meet the Holy in it, and when we are with others in this way, there are no limits to the possibilities” (p. 496). Experiencing the infinite may be accomplished through awareness, deep connectedness, belief, and spiritual rituals. The last caring concept is inviting creating emergence and is “attending the birth of innovative, emergent patterning through affirming the potential for change, nurturing the awareness of possibilities, imagining new directions, and clarifying hopes and dreams” (Smith, 2020, p. 497). Caring, according to the theory of unitary caring, is “inspiring the other to birth oneself anew in the moment” (p. 497), and this transformation may occur through some activity, realization, decision, a new role, or a new life pattern.
Method
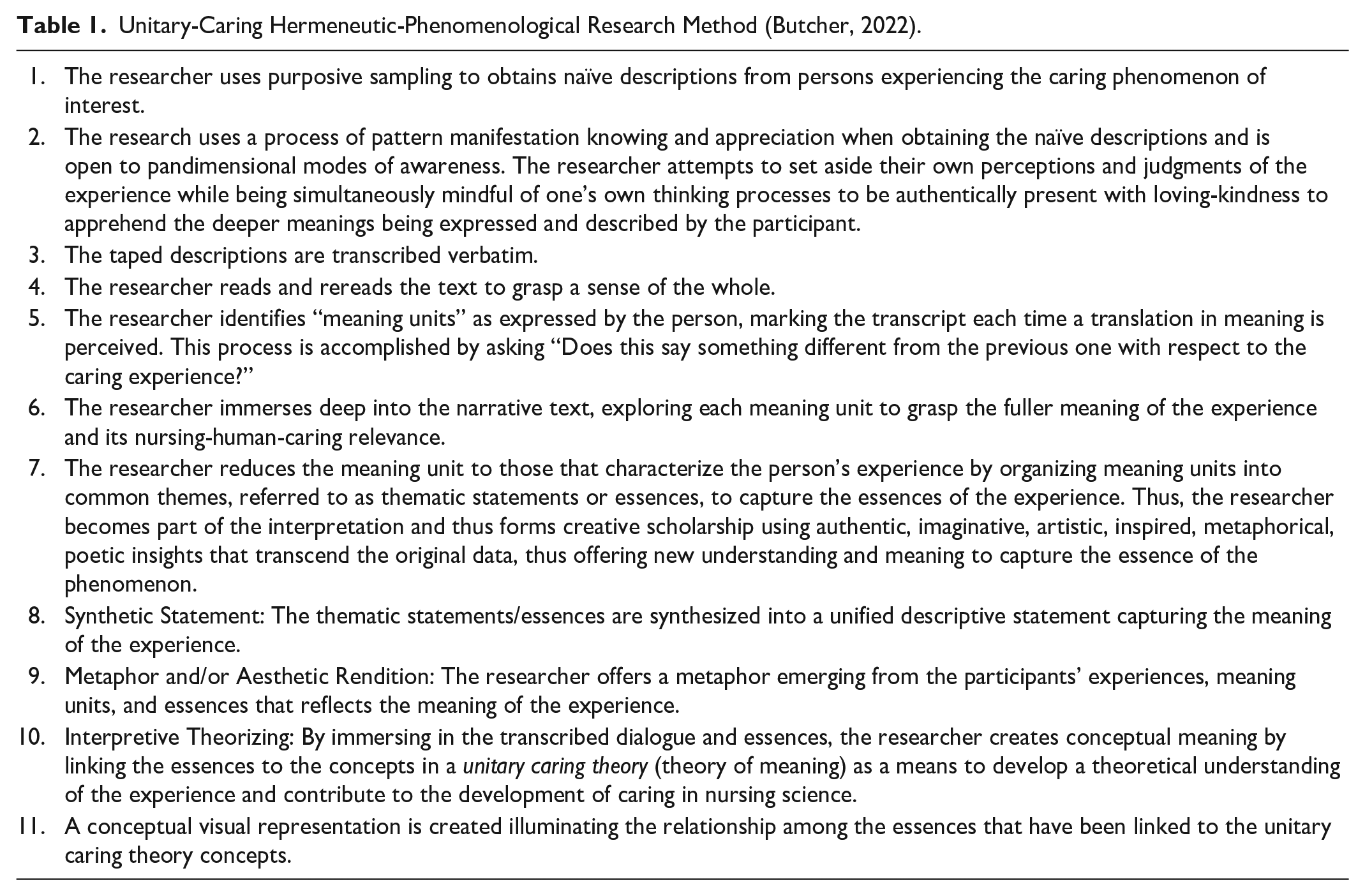
Smith (2020) does not specify a particular research method; however, theories within nursing’s unitary transformative paradigm, where Smith’s (2020) unitary caring is situated, are most consistent with hermeneutic-phenomenological approaches to inquiry (Butcher, 2006; Parse, 2016; Watson, 2012). Butcher’s (2022) unitary-caring hermeneutic- phenomenological research method was used in this study (see Table 1). The method is a revision and expansion of Watson’s caring science-based descriptive-empirical phenomenological research method (Watson, 2012, pp. 97-98). A unique feature of the unitary caring hermeneutic phenomenological research method involves “interpretive theorizing,” which involves interpreting the thematic statements/essences from the perspective of a unitary caring nursing theory—in this case, Smith’s (1999, 2020) theory of unitary caring.
Unitary-Caring Hermeneutic-Phenomenological Research Method (Butcher, 2022).
Sampling and Participants
A purposive sampling strategy (Creswell & Poth, 2018) was used to recruit participating caregivers from three medical inpatient units in a tertiary general public hospital in Saudi Arabia, Western region. The participants were Saudi informal caregivers of a family member who had a stroke and were identified through a nurse manager working at the medical inpatient units. The researcher recruited five Saudi informal caregivers who are family caregivers of hospitalized stroke survivors. The inclusion criteria for the family caregivers were as follows: (a) identified as a primary family caregiver for patient with stroke; (b) present with the patient during the course of hospitalization; (c) adult child, a spouse, other relative, or friend of the stroke survivor; (d) have Saudi citizenship; (e) either men or women aged 18 years or older; and (f) able to give consent and willingness to participate in the study. The exclusion criterion for this study was being formal caregivers such as nurses.
Collecting Naïve Descriptions for Participants
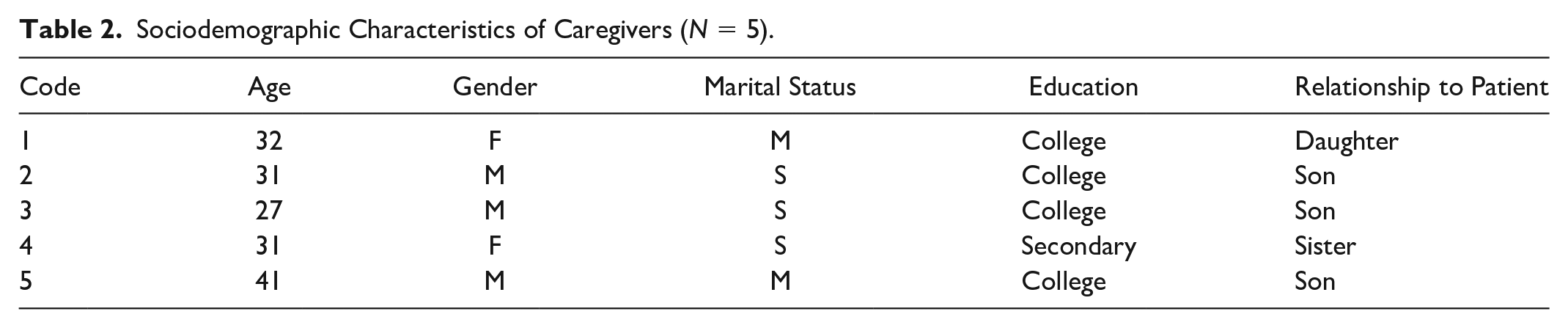
The researcher used a process of pattern manifestation knowing and appreciation with pandimensional modes of awareness to obtain naïve descriptions of the experience from each participant. Pattern information were collected through open-ended, in-depth interviews between December 2019 and January 2020 by the primary researcher. An interview schedule was based on the participants’ preference, and all interviews were conducted in a private area of the hospital. Interviews ranged from 20–60 minutes and were conducted in the Arabic language. The open-ended questions revolved around areas relevant to the research question focusing on the family members’ thoughts and feelings in caring for a family member with a stroke, followed by more probing questions to allow participants to speak more fully and deeply about their experiences. The researchers set aside their assumptions, perceptions, and judgments about the experience to be fully engaged with the participant and hear the deep meaning being expressed and described by the family caregiver (see Table 2 for demographics of participants).
Sociodemographic Characteristics of Caregivers (N = 5).
Data Synthesis
After completing each interview, the primary author reviewed the data collected from the participants by listening to the tape, and then the researcher transcribed and translated the taped interview verbatim from Arabic to English. The translated language was validated by a bilingual nurse who was an expert in both languages. Upon completing the data’s transcription and translation, the researcher began the data synthesis process guided by the unitary-caring hermeneutic- phenomenological research method. The transcribed interviews were imported into ATLAS.ti Version 7 software for data management and to organize the codes and meaning units. The researcher read each transcript fully to gain a sense of the whole content. Then, the statements and phrases related to informal stroke caregiver experiences were highlighted in the text in each transcript. Additionally, statements were identified after reading the transcripts several times. Statements were then organized and grouped into “meaning units” identified as a coding category. The researcher then examined each meaning unit, adding comments related to the interpretive meaning to provide an in-depth understanding. The researcher reflected upon each meaning unit to determine if it was either essential or incidental by determining whether each meaning unit was supported by the participants’ descriptions of the experience. The researcher reached pattern repetition during the analysis of the fifth participant interview when no new themes (meaning units) emerged, and there was a repetition of previous identified meaning units. In interpretive phenomenological analysis (IPA), Smith, Flowers, and Larkin (2009) stated that experienced IPA researchers now have sample sizes in the 3 to 6 participant range. An experienced phenomenological and hermeneutic researcher, the second author of this paper, reviewed and read the transcribed interviews, coded, and reduced meaning units into themes. Using imaginative, artistic, inspired, metaphorical, and poetic insights, the researchers collaboratively transformed each meaning unit into an essence to capture the full meaning of the participants’ experiences. The researchers then integrated the essential themes into a structure by synthesizing the essences into an integrated whole that embodied the structure of the experience and then compared the structure of the experience to other literature. Lastly, conceptual meaning was created by linking and interpreting the essences within Smith’s (1999, 2020) unitary caring as a means to develop a theoretical understanding of the experience and contribute to the development of caring in nursing science.
Trustworthiness
To assure trustworthiness, Lincoln and Guba’s (1985) criteria of creditability, transferability, dependability, and confirmability were used. Credibility of data was achieved through prolonged involvement and thick, written descriptions of participants’ experiences. In addition, peer debriefing, reflexivity, and collaborative analyses were also used to ensure the credibility of findings. Dependability was reached by creating an audit trail using the ATLAS-Ti Version 7 qualitative data management program, while confirmability was achieved by maintaining a reflexive journal where both the researcher’s thoughts and reactions were documented. Transferability is enhanced by the inclusion of verbatim statements, ensuring the accuracy of audiotapes by transcribing the tapes immediately, and comparing the transcriptions to the audio recordings. In addition, the authors invited readers to use de Witt and Ploeg’s (2006) expressions of rigor in hermeneutic phenomenological research: balanced integration, openness, concreteness, resonance, and actualization.
Ethical Considerations
Ethical approval from the Institutional Review Board (IRB) at Florida Atlantic University (No. 1511703-1) and the hospital in Saudi Arabia was obtained prior to conducting the study (No. H-02-J-002). The researcher provided a verbal and written explanation of the study to the participants before obtaining a signed, written consent form. Participants in the study were informed that confidentiality of all data collected would be honored and that they had the right to withdraw from the study at any time.
Findings
Participants in this study included three males and two females (N = 5). Their ages ranged from 27 to 41 years old. The majority of the family caregivers were single (N = 3). All of the family caregivers were children of the stroke survivors, except one was a sibling (see Table 2). After reading the transcripts as a whole, a selective highlighting approach was used to identify a total of 66 statements that were coded and then organized into 11 categories or meaning units, which were then synthesized into six essences. Six essences that emerged were as follows: living with the uncertainty of ambiguity, feeling distressed with worries and fears, yearning for compassionate, unfulfilled desires, overcoming uncertainties through connections and faith, and honoring abiding commitments. Each of the six essences was present in all five participants’ descriptions of their experiences of caring for a family member who was hospitalized with a stroke.
Living With the Uncertainty of Ambiguity
Living with the uncertainty of ambiguity reflects the profound sense of uncertainty experienced by family caregivers while they were at the bedside with their family member in the hospital. The participants expressed how uncertain they felt about the future, not knowing what would happen from one moment to the next. The family caregivers lived unstable and unpredictable patterns due to unfamiliarity about their family members’ condition and whether they might improve or become even worse day after day, while not understanding what was happening or what to do. One family member captured this experience in saying: Honestly, as a caregiver of a patient with stroke and for the patient as well, it is important that we feel that they [nurses] are caring about you. This is the first time he’s had a stroke, and also the first time for me to be hospitalized with him, I don’t know what is going on? What should I do? Totally, I don’t know. (P3)
Furthermore, the participants expressed feelings of being unsure about the caregiving role and the resources available to the patients when discharged due to ambiguity and a lack of information provided by healthcare providers. A participant who was the son of a stroke survivor expressed concerns and kept asking about poststroke resources that would be available to his mother: I don’t know when my mom gets discharged to home, if the hospital will provide her with a bed, wheelchair, or any home visits. (P5)
Another participant said: I don’t want to find out this by myself when I get discharged to the home. I need someone to come and speak with me, explain to me that she will have this, and she needs one, two, three . . . it will be hard for me to find this out by myself. (P1)
Feeling Distressed With Worries and Fears
Amid the uncertainty, a lack of interaction with health providers, and a lack of information provided by the healthcare team about the stroke survivors’ condition, family caregivers experienced numerous concerns and a tremendous amount of emotional distress. The son of a stroke survivor described his experience as “I am worried that my father may get complications from this stroke. No one assures us or tell us if my father’s condition is stable or tells us that he will get better, no one says that” (P2). Also, family caregivers expressed fear of what exactly to expect regarding their relative’s condition: “I am very anxious that my mom will have another stroke because she is not aware, so if she has another one, it will be difficult for me to detect it” (P1).
Participants also expressed fear regarding their own preparation for assuming a full-time caregiving role and meeting the patients’ needs. A daughter of the stroke survivor stated: My mom here is under medical supervision here, so when we will get discharged home, what I am concerned by is how to provide the care to my mother, she needs someone to be with her when she eats, when she uses the toilet, when she walks or goes back to the bed. Before, she was able to walk so during the night, I was just assisting her to go to the bathroom, but now she is totally confined to her bed, I am concerned that she will be like that forever. Also, I am concerned that I don’t know and I can’t understand her needs because before, she was able to speak, but now no. (P1)
In addition, due to feelings of worry and being intensely focused on their loved ones’ needs, family caregivers experience difficulty sleeping. “Even here when I am with her, I woke up during the night 2-3 times to check her, it is really hard to have a relative with stroke” (P1). A son of one of the stroke survivors stated: “Through the whole night, I didn’t see anyone come and check my father, I know there is a call bell if he needs something, the nurses will come if he calls. But what if my father has another stoke and he can’t use the bell, and I am not here or I am asleep . . .” (P3).
Yearning for Compassionate Caring
This essence revealed the lack of sufficient care that caregivers experienced from healthcare providers. Most participants complained about the lack of genuine care they received from physicians and nurses. As they were at the patients’ bedside, the nurses were not greeting them or indeed having any interactions with them or indeed had any interactions with them. They were “busy” and focused primarily on the patient’s physical care: Most of the nurses here are busy, they don’t have time to speak with us or explain what is going on, what is this medication, for what is this injection, they don’t assure us, they don’t show that they are caring for the patient or for the patient’s relatives, and they don’t even smile. (P1)
Further, family caregivers perceived that staff members were inattentive to their questions and concerns and felt that they were perceived as bothersome. This led to family caregivers experiencing difficulty in getting information about their loved ones. A daughter reported, “when I ask them any question, like for what is this medication, they answered, but they got annoyed, so even if I have other questions, I do not ask, I get silence” (P1). Another participant tried to justify the reason for the staff’s insensitivity to their questions, however he did not justify their action: Nurses answer when I ask, but sometimes you feel from the body language of the person if they want or don’t want to help you. Also, sometimes you feel that that even if you want to ask something, their body language indicated, like she said quickly, I don’t have time. They may be busy, have a lot of work, nobody likes to come to the hospital for any reason. So, we need them just to be kindliness with us. (P3)
Unfulfilled Desires
Participants expressed the needs related to information and to accessing resources relating to care received and the hospital environment. Information needs were related to disease signs and symptoms, patients’ needs, the care provided for the stroke survivors postdischarge, and available poststroke resources. A son of stroke survivor asked: I need the clinicians to teach me how I care for him [my father] when he gets a discharged to home. Which aspects of care he needs, for example, what are the activities that allow for him to do and he can tolerate, how I can know if he has another stroke, and what to do with the patient who passes this period? (P2)
Family caregivers relied on physicians and nurses to address and meet their needs related to information concerning the patients’ care. However, the necessary information was not always provided in a way that was understandable for family caregivers. This hinders the opportunities to ask more questions. A son of a stroke survivor commented: They answered us when we asked, but you know, I feel still they need to explain to us more in a clear language. For example, when I asked the doctor about my father’s stroke, he answered. He [physician] informed me about the results of the CT scan and blood work. But I don’t have a medical background, that is why I become silent and not ask more. (P3)
Another reason that hinders the opportunities for the family caregivers to ask more questions was explained by the following participant: There is nothing clear, and when I asked, they [doctors/nurses] seem that they didn’t want you as a family member to ask, they wanted us to wait. (P1)
The majority of the participants reported a need for having genuine care from the healthcare team. This includes taking care of the psychological aspect of family caregivers, having their questions answered honestly, and offering assurance to them. Furthermore, they wanted the staff members to acknowledge their fears. A daughter of a stroke survivor said: Also, nurses need to provide emotional support to us through this experience to deal with it because we are as a family caregiver living in a stressful situation. All healthcare providers need to treat us kindly. Being patient with us when we ask or when we are in distress. But in fact, no one considers our questions, our fears, our even emotional distress that we are experiencing when we see our relative suffers. (P1)
Furthermore, participants identified a need for a comfortable physical environment during the stay with their loved ones in the hospital. Family caregivers wanted more comfortable furniture and sufficient space to accommodate family caregivers during their stay. A son of a man with a stroke stated: As a caregiver, I need a comfortable place to stay with my father. The space is small, and the chair is not convenient. It is not comfortable for a person will accompany the patient the whole time. It is a small thing, may not paying attention to it, but can be an important thing for other family caregivers. (P3)
Overcoming Uncertainties Through Connections and Faith
Amid the stressful situation and uncertainty in which the participants lived, they tried to use different resources to manage their situations. Learning by seeking information was one of the approaches that family caregivers used to enhance their awareness about the illness and meet their informational needs. Family caregivers in this study searched the internet. The son of a stroke survivor reported: “The past days, I searched over the internet in Google to know how to deal with the patient who has stroke” (P3). Furthermore, informal social support through learning from the experiences of the others was another source that family caregivers reported as helpful to overcome their concerns. One participant reported: “We asked our friend who has a medical background, or people whose relatives had a stroke. So we can learn from their experiences” (P2).
Additionally, participants in this study reported that their belief in God (Allah), trust in God, and being pleased with God’s will was a source of power to relieve and manage their fear. “Thanks to God (Allah), we accept whatever Allah gives to us. There nothing that concerns me, everything is decided by the will of Allah” (P5). Another participant said, “Thanks to Allah, we are satisfied really. . . . Since I came with my sister until now, I haven’t needed anything, thanks to Allah (God). There is a feeling of comfort” (P4).
Honoring Abiding Commitments
Honoring abiding commitments described the participants’ perception and value for providing care to their loved ones. The family caregivers described their obedience in providing the care for loved ones during their illness. This is due to compliance with God’s commands. One participant said, “Caring for my father is an obligation on me, it is not a choice. It is important to stay with him. For me, it is important to be with him, even if I leave my work to be with him” (P3). Also, a daughter of an older stroke survivor added: “This is my mom; I will never leave her alone even if she is not aware now. I must be with her all the time, either here at the hospital or home. My mom can’t speak, do anything by herself so one of her daughters should be with her all the time. We will never leave her alone” (P1).
Additionally, participants in this study felt obligated to support each other as family members and share the responsibility for providing the care. A son of a stroke survivor commented, “When I heard that my father had a stroke, I took my emergency leave from my work and I came from Riyadh city to stay with my father, my brother and I can assist each other” (P2). Furthermore, an older sibling of a stroke survivor said, “My mom and brother-in-law come every day during the visiting hours. . . . But because I am her older sister and I don’t have other responsibilities. So, I need to be with her (my sister) at the hospital” (P4).
Synthetic Statement and Aesthetic Rendition
Step 8 in the method is to develop a synthetic statement representing the essences and integrating the essences into a whole that embodies the structure of the experience in such a way that it can be compared with the structures derived from other experiences. The lived experience of family caregivers of hospitalized patients with stroke in Saudi Arabia is experienced as: Living with the uncertainty of ambiguity amid feeling distressed with worries and fears replete with unfulfilled desires yearning for compassionate caring and overcoming uncertainties through connections and faith while honoring abiding commitments.
In Step 9, authentic language is used to capture the experience, which may be metaphorical, poetic, and artistic in expression. The researchers created an aesthetic rendition of the lived experience of family caregiving for hospitalized patients with a stroke in Saudi Arabia (see Figure 1). When families faced the illnesses of their relatives and experienced uncertainty, they pray for the relative to get well, and prayer serves as a source to strengthen them and go through this difficult journey. The hands also represent the caring experience of yearning for compassionate caring and overcoming uncertainties through the connection to others and maintaining faith.
Aesthetic Rendition of the Lived Experience of Family Caregiving for Hospitalized Patients With Stroke in Saudi Arabia.
Interpretive Theorizing
Step 10 in the method is to create conceptual meaning of the experience by linking the thematic statements/essences to the concepts in a caring in nursing theory (theory of meaning) as a means to develop a theoretical understanding of the experience and contribute to the development of caring nursing science. A way to accomplish conceptual meaning is to illustrate the relationships among the theoretical statements. The theoretical statements were created by interpreting each essence from the perspective of the concepts in Smith’s unitary caring theory as shown in Table 3. To gain an in-depth understanding of the experience of being family caregivers for stroke survivors, the six essences that emerged from the study findings were linked and interpreted with the concepts of the unitary caring theory.
The Theory of Unitary Care Concepts Related to Emerged Themes.
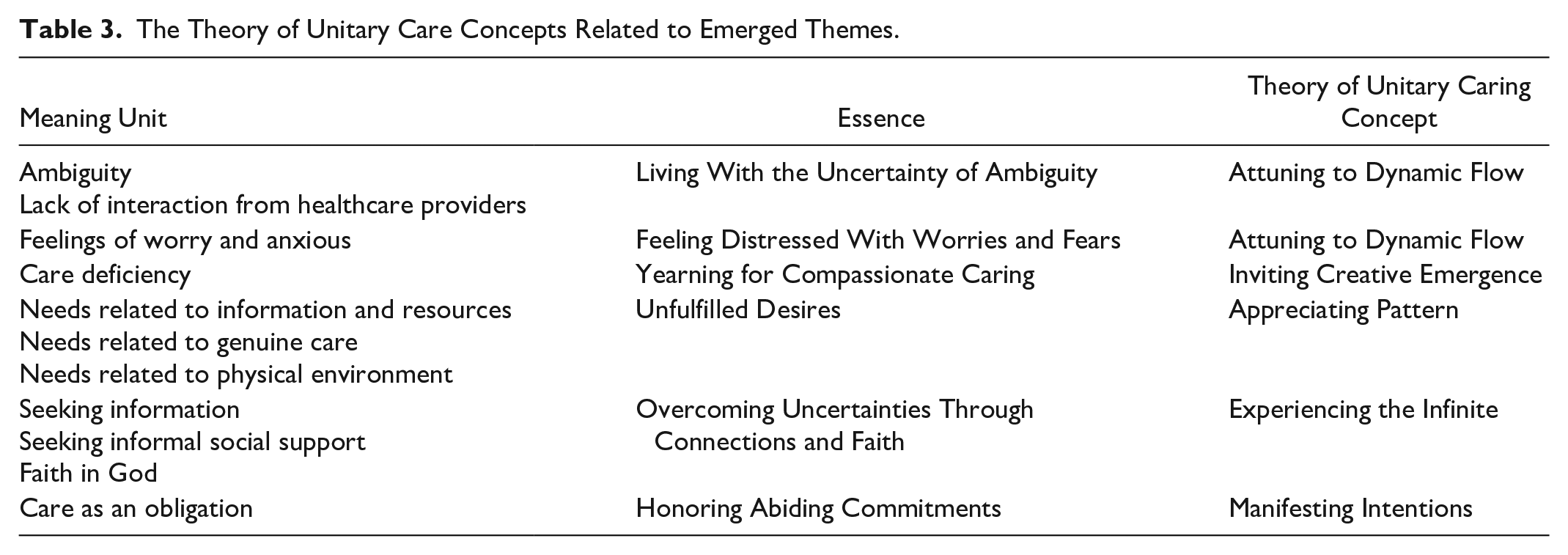
Living with the uncertainty of ambiguity and feeling distressed with worries and fear can be best understood in the context of Smith’s (2020) concept of attuning to dynamic flow. Caring is a process of flowing with co-created rhythms and relating in the moment (Smith, 2020), and family members were attuned with their family members’ experiences of unpredictability and uncertainty describing the living with the ambiguity of unsure outcomes from the stroke itself and their lack of interaction with healthcare providers. As caregivers experienced the rhythms of fear and distress, nurses were limited in their ability to be sensitive to (attuned to) the flow of family’s concerns, fears, and lacked the ability to give voice to the care recipient’s thoughts and feelings. Instead, family members synchronized their rhythms with the loved one who experienced the stroke and reached out for support and knowledge, were fully present, voiced their concerns, and provided love and support.
Yearning for compassionate care is a process of inviting creative emergence. Family caregivers yearned for more engaged care from nurses and physicians. This essence reflects how nurses and physicians were unable to ease family caregivers’ distress during the crisis. Healthcare providers were limited in helping them to grow, lacked in providing the necessary information, and the caregivers felt the care providers did not teach the necessary skills to care for their family member with a stroke. Instead, family members filled this void through their own creative emergence by providing presence, compassionate care, and supporting their family member’s hopes, dreams, and possibilities in the best they were able to do. Inviting creative emergence manifested in new ways of living created by family caregivers in response to their circumstance.
Recognizing unfulfilled desires is a process of appreciating pattern. In appreciating pattern, family members were able to recognize that they and their family member with a stroke had unmet needs. Appreciating pattern prepares one for participating, knowing in the process of change, sensing their family member’s care needs, and listening to concerns. Caregivers spoke about the various needs such as the need for information, genuine care, and resources available in the community.
Overcoming uncertainties through connections and faith are forms of experiencing the infinite and coexisted in all the participants’ descriptions of caregiving experiences. Family caregivers in this study “experienced the infinite” through their relationship and connection with God (Allah) that maintained their hope and kept them moving through this unpredictable reality. Belief in Allah fueled a sense a hope amid the fear, the sense of loss, and distress. Connection to Allah is pandimensional awareness and connection that transcends past, present, and future, the ultimate source of all that has, is, and will ever happen. Allah listened to their prayers and is an infinite source of care, compassion, mercy, and love and the source for finding meaning in their situation.
Manifesting intentions is honoring abiding commitment, which encompasses the family’s beliefs, feelings, desires, and energetic commitment to care for their significant others day by day through facilitating authentic presence during hospitalization, by not only being physically present but through focused attention to their relatives’ needs and all efforts to alleviate their suffering and vulnerability.
For the last step of the method, the researcher created a conceptual diagram illuminating the relationship among the essences that were linked to the unitary caring concepts. Figure 2 illustrates the conceptualization of the unitary caring lived experience of family caregivers of a family member in the hospital who experienced a stroke. All the theoretical statements are dynamically connected emerging from a caring pandimensional, rhythmical, human-environmental transformational process of well-being.

Conceptualization of the Unitary Caring Lived Experience of Family Caregivers of a Family Member in the Hospital Who Experienced a Stroke.
Discussion
This research described in vivid detail the experiences of family caregivers for stroke survivors during the acute in-patient stay. The findings of this study indicated that within the Saudi society, the sense of obligation, love, and affection was a motivation for caregiving. People are obligated by religion and values to take care of their relatives in need, particularly for their parents. Taking care of loved ones is common practice in Asian countries; this is grounded in culture-based beliefs, values, affection, love, and a sense of responsibility toward caring for their family members in need. This was commonly featured in previous phenomenology studies conducted in Sri Lanka and China (Wagachchige Muthucumarana, Samarasinghe, & Elgán, 2018; Zhang & Lee, 2019). Participants in this study put their own needs aside in order to be beside their relatives and take care of them. This form of self-sacrifice was reported in previous studies also (Qiu et al., 2018; Zhang & Lee, 2019). However, according to Qiu et al. (2018), this can threaten family caregivers’ health and well-being. This is true of the participants in our study, as some of them reported sleep deprivation because family caregivers were staying awake overnight to monitor their relatives with a stroke.
Family caregivers in this study complained of insufficient information about the disease; its signs, symptoms, and consequences; care plan; and available resources offered to their relatives when discharged home. In addition to a desire for a comfortable hospital environment, such as sleeping arrangements, they expressed a desire for authentic care on the part of nurses and other healthcare providers. Some of these findings were supported by previous studies (Camicia, Lutz, Markoff, & Catlin, 2019; Kumar, Kaur, & Reddemma, 2016). According to Camicia and colleagues (2019), family caregivers reported both met and unmet needs regarding the environment and accommodations during hospitalization, as well as communication gaps, and lack of receiving support from staff members, which led them to feel unprepared to care for their relatives after discharge, and unaware of the services available to them. Furthermore, Kumar et al. (2016) described the highest needs of family caregivers were related to health information that included new early symptoms of a future attack, meeting physical needs and problems, rehabilitative and educational needs, and best methods to foster recovery of the patients.
Furthermore, through the interactions with healthcare providers, family caregivers in this study found difficulties in getting emotional support, reassurance, and attention for their needs and questions. This may be due to lack of time, high levels of workload, and a shortage of the number of nurses, which leads them to focus on the care of patients without their family caregivers (Bahrami, Etemadifar, Shahriari, & Farsani, 2014). Our findings are consistent with previous studies in which some stroke family caregivers found difficulty in interactions with healthcare providers (Bahrami et al., 2014; Creasy, Lutze, Young, Ford, & Martz, 2013). One important finding of our study indicated that family caregivers experienced emotional distress, such as feelings of worry, anxiety, and fears. This finding lines up with the previous quantitative research conducted among Saudi family caregivers of patients with a stroke, in which more than half of the participants reported feeling mild to moderate depression (24.4% and 29.3%) and more than one third had mild to moderate anxiety (22% and 18.7%), respectively (Alquwez & Alshahrani, 2020). The reasons for these feelings in this study are due to uncertainty, a lack of reliable information, lack of reassurance, and adequate interaction with nurses and other healthcare providers. Therefore, nurses play a pivotal role in easing the crisis lived by families through authentically listening to families’ concerns, recognizing their feelings, and showing ongoing availability and interest in answering their questions.
Living with uncertainty was a common experience among the participants in this study. According to Mishel (1988), changes in disease trajectory can cause a great feeling of uncertainty because of the ambiguous, unpredictable, unknown, and complex nature of the illness. In this study, the main reasons for uncertainty were ambiguity about patients’ conditions and a lack of reliable information about their loved ones from healthcare providers. Most previous qualitative and quantitative studies reported that experiencing uncertainty is common among family caregivers of patients with a stroke (Byun, Riegel, Sommers, Tkacs, & Evans, 2016; White, Barrientos, & Dunn, 2014). White et al. (2014) found that the uncertainty experienced by family caregivers of stroke survivors was related to the extent of recovery, signs and symptoms of stroke, management of risk factors of stroke, financial responsibilities, and formal resources of poststroke care. Further, Byun et al. (2016) found the uncertainty experienced by family caregivers was higher among older age caregivers and people who had relatives with a recurrent stroke. However, this is inconsistent with our findings, where most of the participants who experienced uncertainty were in their middle adulthood.
Family caregivers in this study adopted various strategies, such as seeking information, sharing responsibilities with other family members, and seeking social support from significant others who had similar experiences in order to help them to find meaning in this experience and gain strength. Some of our observations were also supported by previous studies in which family caregivers used informal social networks such as family members, relatives, and neighbors as a source of support and relief for them with caregiving responsibilities (Gertrude et al., 2019; Wagachchige Muthucumarana et al., 2018). Further, believing in Allah also was one of the significant strategies that assisted families in navigating their uncertainty and managing their concerns about their loved ones’ situations. Family caregivers in the current study dealt with their unpredictable reality through their relationship and connection with God (Allah) that helped maintain their hope and strengthened them through this difficult experience. The same finding was reported in family caregivers of patients who suffered from a stroke in Saudi Arabia (Alquwez & Alshahrani, 2020) and in Sir Lanka (Wagachchige Muthucumarana et al., 2018). Alquwez and Alshahrani (2020) found that participants used religious coping strategies more frequently than existing spiritual strategies when dealing with difficult situations, such as illness. However, religious coping strategies did not always lead to positive experiences as they were also found to be associated with poor mental health and depression.
Implications for Unitary Caring Science Practice and Research
Nursing Practice
Nurses bear witness to patients and their families’ lived experiences during an illness trajectory and the period of hospitalization. The findings of this study show how nurses and other healthcare providers can help family members in understanding their situations and keep them going through the crisis in the following ways. Understanding uncertainty and ambiguity that family caregivers face when their loved ones had a stroke or CVA (cerebrovascular accident) can guide nurses and other healthcare practitioners to provide compassionate care by being present in the caring moment with patients and their family members and focus on what is important to them at that moment. Recognizing the struggle of feelings of fear and worry experienced by family caregivers may guide nurses in assisting families in finding meaning in their current crisis and the world they live in, enhancing their transcendence and personal growth, and enhancing wellbecoming. Indeed, knowledge gained from understanding the details described in this study can guide nurses to provide compassionate, family-centered, sensitive, respectful, and genuine care informed by the theroy of unitary caring through appreciating the unpredictable unfolding patterns attuning to the dynamic flow of uncertainties, inviting creative emergence for participating in compassionate care, helping family members in their intentional abiding committements to one another, and providing opportunities for the family to experience the infinte through their faith as a means to overcome uncertainties.
Nursing Research
The findings of this study suggest that future research is needed focusing on the family caregiving experiences when engaged in caring for a family member who has experienced a stroke. One implication for future research would call for using phenomenological research approaches to better understand the experiences of family caregivers of stroke patients after discharge to home in Saudi Arabia. Using research framed by the unitary caring perspective can provide new insights into the meaning of family caregiving, expected as human beings in relationships with others, and expand nursing knowledge. Further possibilities for investigation exist by exploring more deeply the meaning of each essence (themes) that emerged from this study. For example, phenomenological investigations into the theme, the living with uncertainty of ambiguity, can contribute to a deeper understanding of uncertainty among family caregivers. In addition, studies exploring the unitary nature of compassionate care from both the perspective of family caregivers and healthcare providers can reveal new understandings into the family caregiving experience and contribute to expanding knowledge in relation to the unitary caring.