
Abstract
Patient abuse in healthcare is an emerging phenomenon in need of explanation and further analysis. Preventing abusive incidents in healthcare requires identifying structural imbalances that make mistreatment of vulnerable individuals possible. A theory synthesis of the vicious violence triangle and the socioecological model provides a framework to investigate factors that influence nurses’ abusive behavior toward patients in hospitals. Concepts include direct violence, structural violence, cultural violence, and intrapersonal, interpersonal, and organizational factors. The patient abuse in healthcare theory supports empowerment and transformation of nursing and nursing science and offers a blueprint for research that promotes health equity.
Violence is among the most prevalent health problems worldwide, and affects all stratums of society (World Health Organization, 2013). Patient abuse in healthcare is an emerging violence phenomenon in need of explanation and further analysis. Abusive behavior can impact a patient’s psychological, emotional, and physical well-being (Miltenburg et al., 2018; Wijma et al., 2016). Patient abuse by healthcare professionals takes different shapes. Abuse is frequently thought of as being physical; however, verbal abuse is common and may weaken a patient’s mental health and dignity (Albina, 2016). Another form of abuse is patient neglect. The World Health Organization (2010) defined neglect as “the absence of minimal services or resources to meet basic needs” (p. 130). Lachs and Pillemer (1995) noted that neglect occurs when the healthcare professional fails to fulfill the patient’s needs. Exposure to abuse in healthcare settings leads to immediate and long-term suffering and can diminish a patient’s confidence in healthcare professionals (Miltenburg et al., 2018).
Patient abuse in healthcare is an international problem. Researchers across the globe report that patients experience suffering secondary to violence in the healthcare setting (Alzyoud et al., 2018; Brüggemann & Swahnberg, 2013; Brüggemann et al., 2012; Oluoch-Aridi et al., 2018; Swahnberg et al., 2009; Vedam et al., 2019). This abuse occurs regardless of gender, disease, and appropriateness of the medical treatment.
Rates of patient abuse vary across countries. Vedam and colleagues (2019) reported that in the United States, one in six women (17.3%) experience one or more types of mistreatment by a healthcare professional during pregnancy and childbirth. In Sweden, 20% of female and 8% of male patients reported lifetime experiences of abuse across healthcare settings (Swahnberg et al., 2009). In Jordan, 32.2% of women reported feeling neglected by healthcare professionals during their last childbirth, while 37.7% of women were exposed to verbal abuse (Alzyoud et al., 2018). These findings lack consistent and conclusive evidence as to the causes of patient abuse in healthcare. Additionally, the patient abuse violence phenomenon is further complicated by the absence of a theoretical framework to guide research and practice.
Statement of the Problem
Healthcare professionals are called on to relieve patient suffering through the ethical principle of nonmaleficence. Although healthcare professionals swear to a professional oath, violence against patients still occurs. Patient abuse in healthcare is related to hierarchical structural factors (Wijma et al., 2016), in which healthcare professionals assume a patriarchal role, taking a position of power over patients. This position of dominance and holding authority over patients creates a power dynamic that can lead to disrespectful behavior (Miltenburg et al., 2018).
Healthcare workers themselves may be victims of healthcare organizational challenges and unfavorable working conditions (Grissinger, 2017). According to Reader and Gillespie (2013) organizational factors (high workloads, staff shortage, burnout, poor teamwork) and problems in the relationships among staff and patients are often the causes of patient neglect. Preventing disrespectful and abusive incidents in healthcare requires attention to address all of these structural imbalances, which result in conditions that make mistreatment of vulnerable individuals possible (Miltenburg et al., 2018).
The healthcare system was established to assist patients and reduce suffering (Wijma et al., 2016). Families trust healthcare professionals to treat their loved ones with respect and dignity (Albina, 2016). In a recent U.S. survey of professional honesty and ethical standards, nurses were rated highest for ethics and honesty of all professionals (Gallup, 2019). Registered nurses are advocates for patients in the face of wrongdoing, and the public trusts them because of their competency and caring skills (Albina, 2016). Nonetheless, disrespectful and abusive behaviors, including physical abuse, psychological abuse, neglect, and invasions of privacy, still happen in clinical settings (Miltenburg et al., 2018).
In the absence of a guiding theory, existing research on patient abuse remains fragmented and difficult to interpret. There is a need for the development of a theoretical framework that identifies key elements of nurses’ abusive behavior toward patients in the practice setting. The authors in this paper present a synthesis of two theories: the vicious violence triangle (VVT) theory (Galtung, 1990, 2004) and the socioecological model (SEM) (McLeroy et al., 1988). The purpose of this theoretical synthesis is to develop a framework to explore the factors that influence nurses’ violence behaviors, in order to better understand and prevent patient abuse.
Method
The patient abuse in healthcare theory was developed with a nursing perspective based on Walker and Avant’s (2011) approach for theory synthesis. This approach depends on a comprehensive analysis of a phenomenon of interest. A thorough review of the literature was conducted to summarize and synthesize appropriate information and concepts of interest related to nurses’ abusive behavior toward patients. Two theories were identified as most relevant and applicable for the development of a synthesis framework that identifies factors linked to nurses’ abusive behavior toward patients. The first theory, the VVT theory (Galtung, 1990, 2004), captures important aspects of abusive behaviors toward others and provides a theoretical foundation for the proposed theoretical synthesis. The SEM (Bronfenbrenner, 1979, 1997) was the second theory identified and analyzed for additional concepts (intrapersonal, interpersonal, and organizational) not captured by the VVT theory.
Both theories were examined for their origin, congruence, relevance, application, and testability (Walker & Avant, 2011). Empirical and nonempirical evidence on abusive behavior toward patients in the literature was also analyzed and evaluated, which improved understanding of the theories and revealed strengths and limitations related to the theories’ congruence and value. The process of theory synthesis includes three phases: (a) identifying the main concepts that have the potential to serve as anchors of the proposed theoretical framework, namely, direct violence (events), structural violence (processes), cultural violence, and intrapersonal, interpersonal, and organizational relationships; (b) reviewing the literature to determine whether there are any variables associated with the central concepts and defining the relationships; and (c) organizing the concepts and statements into an integrated and effective illustration that reveals new insights into nurses’ abusive behavior toward patients in healthcare settings (Walker & Avant, 2011).
Analysis and synthesis of the concepts and assumptions of the VVT and SEM theories led to the development of a new theoretical framework: the patient abuse in healthcare theory (PAHT) (Figure 1). The authors in this paper detail the new theory and its derivative sources, the VVT and the SEM. The authors explore how the synthesis of the two theories improves understanding of nurses’ abusive behavior toward patients and the nursing implications of the new framework.
Patient Abuse in Healthcare: A Theoretical Model.
Theoretical Overview
Vicious Violence Triangle
The VVT is a theoretical model developed by the Norwegian researcher Johan Galtung to study the relationship between direct, structural, and cultural violence (Galtung, 1990, 2004) (Figure 2). Galtung examined the causes of various forms of violence and classified them into three categories: direct violence, cultural violence, and structural violence (Galtung, 1990). Every category represents a specific angle of the violence triangle. According to Galtung, the violence triangle has “built-in vicious cycles” (Galtung, 2004, p. 1). The foundations of direct violence are cultural and structural violence, subsequently “direct violence reinforces structural and cultural violence” (Galtung, 2004, p. 1). Galtung divided the violence triangle categories into visible (direct violence) and invisible (cultural and structural violence) (Galtung, 2004).
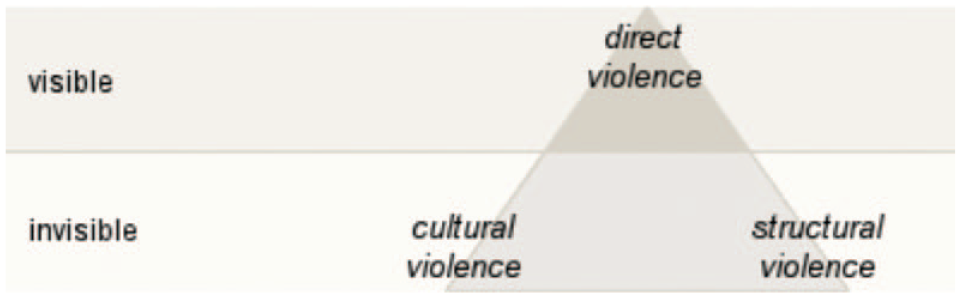
The Vicious Violence Triangle (VVT) (Galtung, 1969).
Theory Evolution
In 1969, Galtung developed the triangle of violence. Since then he continued to develop the theoretical framework to study peace and conflict, with the purpose of defining the three main features of violence (cultural, structural, and direct) that shape the triangle (Galtung, 1969, 1990, 2004). The VVT was published (Galtung, 1990, p. 291), and in 2004, Galtung conducted the study “Violence, War, and Their Impact: On Visible and Invisible Effects of Violence” to provide a better and deeper understanding of the VVT (Galtung, 2004).
Theory Assumptions
The VVT includes some underlying assumptions: (a) There are roots for every human act, and violence does not occur out of nowhere; the main roots for violence are a culture of violence (patriarchy, ideologies) and a violent structure (oppressive, manipulative, or alienating hierarchies). (b) “Violence breeds violence” (Galtung, 1990, p. 295). (c) Violence can begin at any angle in the triangle and then spread easily to the other corners. (d) Cultural elements are used to legitimize direct and structural violence; in other words, cultural domains such as religion, ideology, cosmology, arts, and sciences are used to justify the violence (Galtung, 1990).
Key Concepts
There are three key concepts in the VVT, and each has several subconcepts. The first concept is direct violence, and it is defined as an event. Direct violence is visible behavior and can be a physical or verbal act. Subconcepts of direct violence include shouting, neglect, repression, detention, and physical abuse such as killing and beating (Galtung, 1990). Structural violence is the second concept and represents one of the invisible aspects of violence; it is a process with ups and downs (Galtung, 2004). Subconcepts of structural violence incorporate marginalization, hierarchical structures, classism, and discrimination.
Cultural violence is the third major concept in the VVT. It is defined as the aspects of a culture (ideologies) that are often used to legitimize direct and structural violence (Galtung, 1990). Cultural violence also represents an invisible aspect of the violence triangle (Galtung, 2004). It is an “invariant, a permanence” (Galtung, 1990, p. 249) and remains constant for a long time, given the fact that necessary cultural changes take time. One can conclude that cultural transformation is not impossible, but it is a challenging process (Galtung, 1990).
Application and Testing of VVT Theory
Several authors and researchers have incorporated the use of the VVT in their work. Both Confortini (2006) and Dodi (2019) used Galtung’s theory to study the relationship between gender and violence. Confortini (2006) integrated the VVT into feminist theories to explain the missing gender gap when addressing violence. She noted that researchers who use the VVT must integrate gender as an essential concept. Dodi (2019) integrated Galtung’s reasoning to show that patriarchy creates a dichotomy between public and private roles, productive and reproductive, which forms an unequal power relation between men and women. He indicated that violence is carried out not only by men but also by women and that patriarchy is what should be blamed, not men. Dodi concluded that sufficient education about factors, sources, and the invisible types of violence identified in the VVT will help to resolve and end gender-based violence.
These studies demonstrate how the VVT can be used to study the phenomenon of violence toward patients in healthcare settings. Nursing is a predominantly female profession, and the patriarchal sociopolitical powers position the nurse role as subordinate to the physician role. Healthcare structures (hospitals) are hierarchical and inflexible, and regardless of gender, nurses’ participation in decision-making is usually limited (Kellett et al., 2014).
Strengths and Limitations
A key advantage of the VVT is the distinction between the three primary forms of violence: direct, structural, and cultural (Galtung, 1990). The theory also provides an explanation of the diverse ways of organizing the phenomenon of violence. The VVT rejects stereotypes that label entire cultures as violent; instead, Galtung advocated that a specific aspect of a particular culture is an exemplar of cultural violence (Galtung, 1990). The theory is well developed and broad enough to focus on the causes and outcomes of violence (Grewal, 2003) and rejects the widespread misconception that violence is in human nature (Galtung, 2004).
A limitation of the VVT is that the theory discounts the influence of intrapersonal and interpersonal characteristics on direct violence and concentrates only on structural and cultural factors as a direct violence source. The role of gender in the social construction of violence is not addressed (Confortini, 2006), and the VVT does not explain how direct violence can progress and occur in a hospital system (Brüggemann & Swahnberg, 2013). Thus, synthesizing the VVT with another theoretical framework that acknowledges social and systematic structures assists in more fully understanding the phenomenon of interest.
Socioecological Model
The SEM was developed in the behavioral and social sciences over a long period, through extensive theoretical and conceptual synthesis. Many authors have made significant contributions to the development and refinement of the model (Bronfenbrenner, 1979; McLeroy et al., 1988; Stokols, 1996). The main idea of an ecological model is that human behavior is influenced by several factors. These factors have multiple levels including intrapersonal, interpersonal, organizational, societal, physical environmental, and policy (Sallis et al., 2015). Ecological models propose comprehensive frameworks to further understand the dynamic interaction among the individual and environmental determinants of health behaviors (Bronfenbrenner, 1979; McLeroy et al., 1988; Stokols, 1996).
Theory Evolution
The SEM defines how human beings are seen as a growing multifaceted system; all individuals live in the context of relationships with families, friends, neighborhoods, schools, and society (Bronfenbrenner, 1979). Bronfenbrenner’s socioecological theory of human development was in a continual process of development until his death (Tudge et al., 2009). His initial theorizing featured the concepts of microsystem, mesosystem, exosystem, and macrosystem (Tudge et al., 2009). In the 1990s, Bronfenbrenner described the proximal processes as one of the fundamental factors that influence human behavior (Tudge et al., 2009).
Theory Assumptions
The underlying assumptions of the SEM are that human behavior is affected by multiple factors, including (a) intrapersonal factors (biological, psychological), (b) interpersonal process factors (formal and informal social networking, culture), (c) institutional factors (rules and regulations), (d) community factors (interactions between organizations and institutions), and (e) public policy (local and national laws). Influences on behaviors interact across these different levels (Bronfenbrenner, 1979; McLeroy et al., 1988). Individuals influence their settings, and the transformed settings then impact health behaviors (Stokols, 1996). The characteristics of the person and the environment, “the structure of environmental settings, and the processes taking place within and between them,” are thus interdependent (Bronfenbrenner, 1979, p. 41).
Key Concepts
There are five major concepts of the SEM. (a) The first major concept is intrapersonal characteristics. Individual knowledge, age, gender, attitudes, beliefs, behavior, skills, and developmental history have the potential to influence personal behavior (McLeroy et al., 1988; Stokols, 1996). (b) Interpersonal relationships encompass formal or informal interactions among two or more people as well as social support systems such as family, work cohorts, and friends. These determinants affect human behavior. (c) Institutional influences, which include the social and physical environment inside institutions or workplaces, organizational structure (hierarchies), social norms, value, and shift work, in addition to policies and guidelines for operation, all have direct or indirect effects on human behavior and interactions. (d) Community factors serve as “mediating structures.” They connect individuals with the broader social environment, such as family, informal social networks, church, neighborhood, and voluntary associations. Further, mediating structures connect organizations and agencies within defined boundaries (McLeroy et al., 1988). (e) Public policy incorporates the local and national regulatory policies, procedures, and laws to protect the community, such as a policy that bans smoking in public buildings (Bronfenbrenner, 1979; McLeroy et al., 1988).
Application and Testing of the SEM
Several researchers have used, tested, and developed middle-range violence theories based on the SEM. Gashaw and colleagues (2018) used the SEM to examine the associations among societal, community, family, and individual related factors with exposure to intimate partner violence (IPV) in pregnancy in Ethiopia. Researchers found that the SEM was able to explain and identify societal and community factors associated with IPV (Gashaw et al., 2018). The SEM was also used by Mercer, whose model of maternal role attainment was based on Bronfenbrenner’s (1979) SEM framework (Mercer, 1995). Later Mercer also used Bronfenbrenner’s ecological model in her revised theory, becoming a mother (Mercer, 2004). Mercer’s theory implies that the microsystem (mother, infant, and father relationships) has direct and significant influence on the mother’s maternal role achievement. Mercer’s theory also proposed that the mesosystem (extended family, school, work, church) directly influences the mother and her microsystem, and the macrosystem (the social, political, and cultural stimuli) impacts all systems (Mercer, 1995).
Decker and colleagues (2018) used the SEM as a framework to study the prevention of community violence, IPV, sexual violence, and suicide by recognizing these factors as severe forms of interpersonal and self-directed violence. The researchers included social epidemiology and social ecology in their public health framework to help understand current behavior. Their study provided an understanding of the layers of influencing factors and concepts across the individual, interpersonal, community, and social-structural elements (Decker et al., 2018).
Socioecological factors have been studied with individuals with HIV/AIDS in Ethiopia. Yakob and Ncama (2016) examined the impact on, access to, and acceptability of HIV/AIDS treatment and healthcare services. The SEM provided the researchers with a useful framework to investigate the interaction among multilevel and interactive factors that have an impact on access to healthcare services such as clients, community, institution, and policy (Yakob & Ncama, 2016). This research supported the use of the SEM as a framework for studying the phenomenon of violence toward patients in healthcare settings.
The SEM Strengths and Limitations
The widespread use of the SEM has helped to identify its strengths and weaknesses. According to Sallis and colleagues (2015), an advantage of the SEM is the emphasis on multiple levels of influence, which offers various choices for interventions. Identifying key influences regarding a particular problem, such as unhealthy behaviors, helps researchers to find interventions to solve issues that affect individuals (behavior changes) (Sallis et al., 2015). In the early stages of theory development, the focus of the SEM was predominantly on context and ignored the role that human beings play in their personal development (Bronfenbrenner, 1979). However, in later work Bronfenbrenner provided a more unobstructed view of the individual’s role in changing context (Bronfenbrenner, 1997).
A limitation of the SEM is the lack of specificity about the hypothesized influences (Sallis et al., 2015). For instance, Sallis and colleagues (2015) explained that the use of the SEM in health behavior studies places a considerable burden on health promotion professionals to identify the critical factors for each behavioral application. The SEM does not sufficiently explain how variables interact across levels (Sallis et al., 2015; Taylor, 2016). According to Terry (2014), because of the interaction among all the levels of the SEM, it is hard to implement “a program at one level without impacting the other levels” (p. 6). The main challenge for researchers using the SEM is to design research studies with testable hypotheses that can guide interventions (Sallis et al., 2015).
The SEM allows researchers to develop broad perspectives about certain phenomena, but the problem of patient abuse in healthcare is focused on clinical settings, which indicates the need to use a more specific theoretical framework. Therefore, synthesizing concepts from the SEM with another theoretical framework allows for the development of a synthesized theoretical model that provides a more focused perspective and useful guide for fully understanding the problem.
The Patient Abuse in Healthcare Theory: A Synthesis
The underlying assumptions of the VVT and the SEM share a belief that different factors influence human behavior. Both theories assume that visible or direct behaviors have roots and that they do not come out of nowhere. The scope of the VVT is more focused and investigates the causes of direct, cultural, and structural violence in specific settings, while the SEM presents a considerably broader scope and incorporates multiple levels to investigate. Studying a phenomenon across all levels in a specific setting, such as abuse in the healthcare setting, would be challenging. Therefore, synthesizing the two theories by adding important concepts and assumptions from the SEM to expand the VVT theory provides a strong model to explain what factors influence abusive behavior toward patients in healthcare settings.
Assumptions
The assumptions for the new integrated theory are consistent with, but additive to, those of the VVT and the SEM. They are as following:
There are roots for human actions.
Violence breeds violence.
Violence can start at any angle in the “direct-structural-cultural” violence triangle and then be transmitted to the other corners.
Cultural aspects are used to legitimize direct and structural violence (Galtung, 1990, p. 301).
Human behavior is influenced by intrapersonal, interpersonal, and organizational factors.
Synthesis of Concepts and Propositions
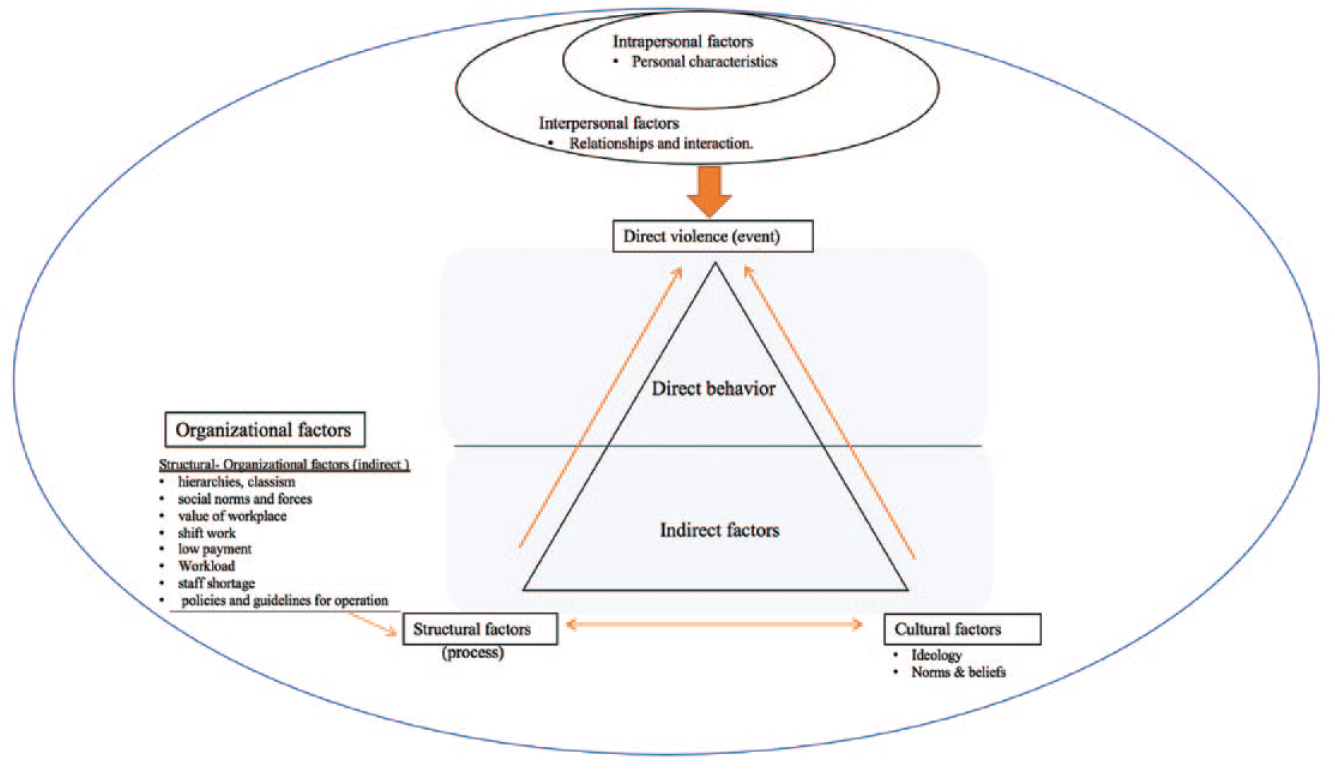
The new integrated theory is based on the VVT with some nested concepts from the SEM added to include essential concepts that identify why abuse develops and occurs in a system that is built to assist patients and deliver the best care possible (Figure 1). The VVT differentiates between direct violence (events or visible behavior), structural violence (processes), and cultural violence (invariants rooted in culture) (Galtung, 1990). Galtung described these three categories in a violence triangle, stressing their interrelatedness.
In the new model, cultural violence is placed at the base of the triangle to show that cultural violence and/or cultural factors legitimize and invoke both structural and direct violence. Cultural factors include ideology, religion, and cultural norms and beliefs. Structural violence, placed at the bottom left angle of the triangle, represents the social structure or institutional structure that may harm individuals by not letting them meet their basic needs. This in turn can stimulate direct violence. Galtung (1990) proposed that structural violence and direct violence are dependent on each other. The outcome of their interdependence is often a direct event (behavior) such as domestic violence, hate crimes, racial violence, intimidation, physical violence, verbal abuse, or war (Galtung, 1990, 2004).
Direct violence is placed at the top of the triangle to represent the visible behavior (events). The placement of direct violence at the upper angle reflects cultural and structural factors as the roots of direct violence, as shown in Figure 1. This is consistent with the original assumptions of the VVT. The use of the VVT in the new theoretical framework allows the researcher to examine the underlying causes of violence in the healthcare setting in three stages: before abuse, during abuse, and after abuse.
Several studies indicate that nurses’ behaviors can be influenced by intrapersonal, interpersonal, and organizational factors (Brüggemann et al., 2012; Grissinger, 2017; Miltenburg et al., 2018). These factors are missing or are not well represented in the VVT; thus, the synthesized theory integrated these concepts from the SEM. The underlying assumptions of the SEM state that human behavior is affected by multiple factors including (a) intrapersonal factors (biological, psychological), (b) interpersonal process (formal and informal social networking, cultural), (c) institutional factors (rules and regulations), and (d) community factors (interactions between organizations and institutions) (McLeroy et al., 1988).
Three of these concepts were chosen from the SEM and nested into a contextualized VVT: intrapersonal, interpersonal, and organizational factors. These concepts have been identified in the literature as variables that could affect nurses’ behaviors in professional settings. Only these three concepts were consistent with the scope of the model under development. The synthesized model does not examine community and public policy factors; therefore, these SEM factors were not included in the theory.
Intrapersonal characteristics such as personal knowledge, age, gender, attitudes, beliefs, ethics, fatigue, burnout, and skills were not well articulated in the VVT. These concepts were included in the new model as they have the potential to influence nurses’ behaviors. Similarly, interpersonal relationships, such as poor relationships with supervisors and coworkers, lack of compassion, and lack of social support systems, can also affect personal behavior in healthcare settings.
Some organizational influences are included in the VVT, such as the structural violence concept (hierarchies, classism). However, additional aspects needed to be examined such as social norms and forces, the value of workplace, shift work, low payment, workload, staff shortage, and policies and guidelines for operation. The SEM offers more details regarding organizational influences, which may assist us to gain a better understanding of their impact on nurses’ behaviors. The organizational and structural factors are nested together as indirect factors; the violence triangle is placed inside the organizational circle since these factors can impact the violence triangle from all angles. Placing intrapersonal and interpersonal aspects at the top of the triangle reflects their direct effect on direct violence (direct behavior). Additionally, intrapersonal and interpersonal factors are mainly visible features. Assimilating the VVT and the SEM into one theoretical model provides a robust, sound framework to recognize and explore factors that influence patient abuse in healthcare settings.
Nursing Implications
Theoretical synthesis provides a unique insight into the phenomenon of interest since the process requires the integration of large amounts of existing knowledge that points the way to new findings (Walker & Avant, 2011). The PAHT is an appropriate framework for healthcare research in various contexts and settings. Initial testing and validation of the model through research will strengthen the framework, which can then be used in nursing education, clinical practice, and policy development.
In nursing education, presenting this patient abuse theory to nursing students in undergraduate and graduate programs will increase their awareness and understanding of the phenomenon and increase mindfulness of the need to provide ethical nursing care. Nurse researchers can use the theory to identify the factors and analyze the causes that lead to patient abuse in healthcare. Findings from research studies can then inform decisions by administrators and policymakers to make appropriate changes to improve staff working conditions.
In the practice setting, nurse managers must understand patient abuse theory in order to promote open discussions on ethical problems regarding patient care with their team members. The current theory gives a thorough definition and description of what contributes to patient abuse, which makes it easier for nurses to recognize and communicate openly with co-workers about this often-hidden phenomenon. In addition, nurses need to be aware of the potential consequences of patient abuse and their effects on the patient’s physical, emotional, and psychological well-being. It is also important to provide educational programs, training, and interventions in all clinical settings to address nurse patient abuse, strengthen moral resources, and increase staff awareness of appropriate ethical behavior (Wijma et al., 2016). The new theory can be used as a guide to develop appropriate clinical interventions for nurses to reduce and prevent patient abuse across healthcare settings.
Conclusions
A high prevalence of patient abuse in healthcare has been reported in the literature, but the factors that contribute to this phenomenon remain poorly understood. To date, there has been a lack of consistent evidence to understand why patient abuse in healthcare occurs and a limited theoretical foundation for the research. The synthesized patient abuse in healthcare theory explores embedded factors that influence nurses’ behaviors toward patients and organizational factors that, if left unexamined, can negatively impact healthcare and patient outcomes. Nurse researchers can use this new theory as the foundation for future research on patient abuse in healthcare, allowing them to identify and address these factors, empower nurses, and transform nursing practice.