
Abstract
The practice column focuses on incorporating a nursing theoretical framework into nursing care in a clinical scenario involving intimate partner violence. Accordingly, as exemplified by utilizing Virginia Henderson’s theory, there is guidance to define, focus, and evaluate nursing care in these multifaceted clinical cases.
Intimate partner violence (IPV) refers to conduct by an intimate partner, or ex-partner that causes physical, sexual, or psychological harm, including physical aggression, sexual coercion, psychological abuse, and controlling behaviors (World Health Organization [WHO], 2023). IPV is identified as one of the most common forms of violence against women and represents a significant global public health issue in both developed and developing countries, including Pakistan. The impact of IPV expands beyond the act(s) of IPV and has been correlated with both short- and long-term medical problems, including loss of a pregnancy, depression, digestive problems, urinary tract infections, vaginal infections, and other stress-related medical issues (Campbell et al., 2002). Globally, intimate partner violence is estimated to occur in about 1 in 3 (30%) women worldwide (WHO, 2023). In Pakistan and other developing countries there are higher prevalence rates, sometimes as high as 43% (Akter, 2022; Hassan et al., 2020). A cross-sectional community-based study performed in Karachi, Pakistan, reports that the prevalence of all forms of IPV was high in the low- and middle-income strata (Ali et al., 2011). A team of researchers reported on IPV from a multi-country study on women’s health and life experiences questionnaire; 80% of participants reported psychological abuse, physical, and sexual violence, while 44% reported exposure to psychological, physical, and sexual abuse (Ali et al., 2011). This study and other reports highlight the importance of the healthcare community taking a lead in screening for associated symptoms of IPV and subsequent planning for safety. Nurses are uniquely positioned to screen, respond, and assist in these sensitive situations. The authors in this article approach an IPV case scenario through emphasizing the importance of nursing theoretical frameworks; and this case scenario accentuates the importance by utilizing Virginia Henderson’s (1991) theory to guide the care provided by nursing.
Nursing Theory
Fawcett (1984) and Chin and Kramer (2018) described nursing as a facilitating process with a primary focus on interpersonal interactions between nurses and other individuals. The important and interrelated concepts of interest are person, environment, health, and nursing. Jacqueline Fawcett (1984), in the article titled The Metaparadigm of Nursing: Present Status and Future Refinements (pp. 84–85), and in the book Contemporary Nursing Knowledge: Analysis and Evaluation of Nursing Models and Theories (Fawcett & Desanto-Madeya, 2013, pp. 6–8), further explicated the concepts as summarized here from the above sources:
Human being – The term persons has been updated to read human being. Human being refers to individuals that live within a culture, family, community, and other pertinent groups.
Environment – The physical surroundings of human beings and their significant others and groups and includes the settings which can range from local, regional, national, and worldwide cultural, social, political, and economic conditions that are associated with health.
Health – The central concept of nursing and defined as human process of living and dying inclusive of wellness, illness, and diseases within those living and dying processes.
Nursing – The study of the interrelationships among human being, environment, health, and nursing. Nursing has a commitment to the compassionate and knowledge care of persons and families with a belief that each person is unique with a focus on providing, assisting and/or providing knowledge to persons/families/communities for the purposes of improving health.
A main implication from the discussion above is that theory and practice are not artificially separated; rather, nursing theory informs and guides the actions of nursing practice. Simply stated, nursing theory directs the way nurses are present with persons, theory organizes approaches to understanding the needs of persons. A description of Henderson’s (1991) theory will serve as background to demonstrate the way Henderson’s guiding functions serve to direct and meet the needs of persons experiencing intimate partner violence.
Overview of Henderson’s Theory
Henderson regarded nurses as independent practitioners accountable for independent judgments focusing on providing knowledgeable nursing care. Nursing focuses on activities and establishing the conditions under which persons can perform the activities unaided (Henderson, 1991). The term “nursing functions” was referenced for providing basic nursing care and was defined as the following 14 functions below.
Breath normally
Eat and drink adequately
Eliminate body wastes
Move and maintain desirable postures
Sleep and rest
Select suitable clothes—dress and undress
Maintain body temperature within normal range by adjusting clothing and modifying the environment
Keep the body clean and well-groomed and protect the integument
Avoid dangers in the environment and avoid injuring others
Communicate with others in expressing emotions, needs, fears or opinions
Worship according to one’s faith
Work in such a way that there is a sense of accomplishment
Play or participate in various forms of recreation
Learn, discover, or satisfy the curiosity that leads to normal development and health and use the available health facilities. (Henderson, 1991, pp. 22–23)
Henderson’s independent functions of nursing emphasize that nurses provide the patient with knowledge, determination, or strength to perform daily activities to achieve health and independence or a peaceful death (Henderson, 1991). These principles and functions serve as a framework to practice, evaluate, and improve the nursing care systems, supports, and delivery.
Clinical Scenario
A 42-year-old female patient who, for the purposes of the case scenario description, will be referred to as Sierra, came to the emergency department (ED) seeking medical care. Upon physical assessment multiple bruising and cuts were present on the neck, arms, and face. Sierra was crying to the point of sobbing and having difficulty in breathing. Her vital signs were mildly elevated, and the overall observation was that Sierra was crying and distressed. During the triage and history process it was reported that Sierra has been married for 24 years and, together with her husband, has five daughters. Sierra further revealed that her husband was disappointed at the absence of having a son; and this absence was a source of conflict. The care provided in the emergency department focused on triage and stabilization; upon subsequent evaluation it was determined that there were opportunities for improving nursing care. Guiding the evaluation of nursing care through utilizing a nursing theoretical framework propels nursing care into a more comprehensive, person-centered approach that goes beyond the accomplishment of tasks.
The initial healthcare treatments with the emergency department admission centers on the multiple activities of triaging and administrative tasks and attends to stabilizing breathing status and addressing injuries. This includes monitoring vital signs, attention to assessing and supporting respiration, and maintaining body and nutrition support (see the Table). Evaluation of nursing care with the addition of avoiding danger and proactively addressing safety guided by a nursing theoretical framework extends person-centered care to a comprehensive frame of reference. An analogy to this claim is that just as some healthcare institutions have provided mortality and morbidity rounds for in-depth discussions examining pathophysiology, pharmacology, and other various interventions, a nursing case scenario evaluation offers a systematic review with a focus on proactively improving outcomes. The nursing frame of reference for this case scenario—Henderson’s thoughts on the nature of nursing (Henderson, 1991)—extends nursing care functions to address dangers and safety for the care of patients experiencing intimate partner violence.
Nursing Diagnosis and Care Planning Based on Henderson’s Theory of Nursing.
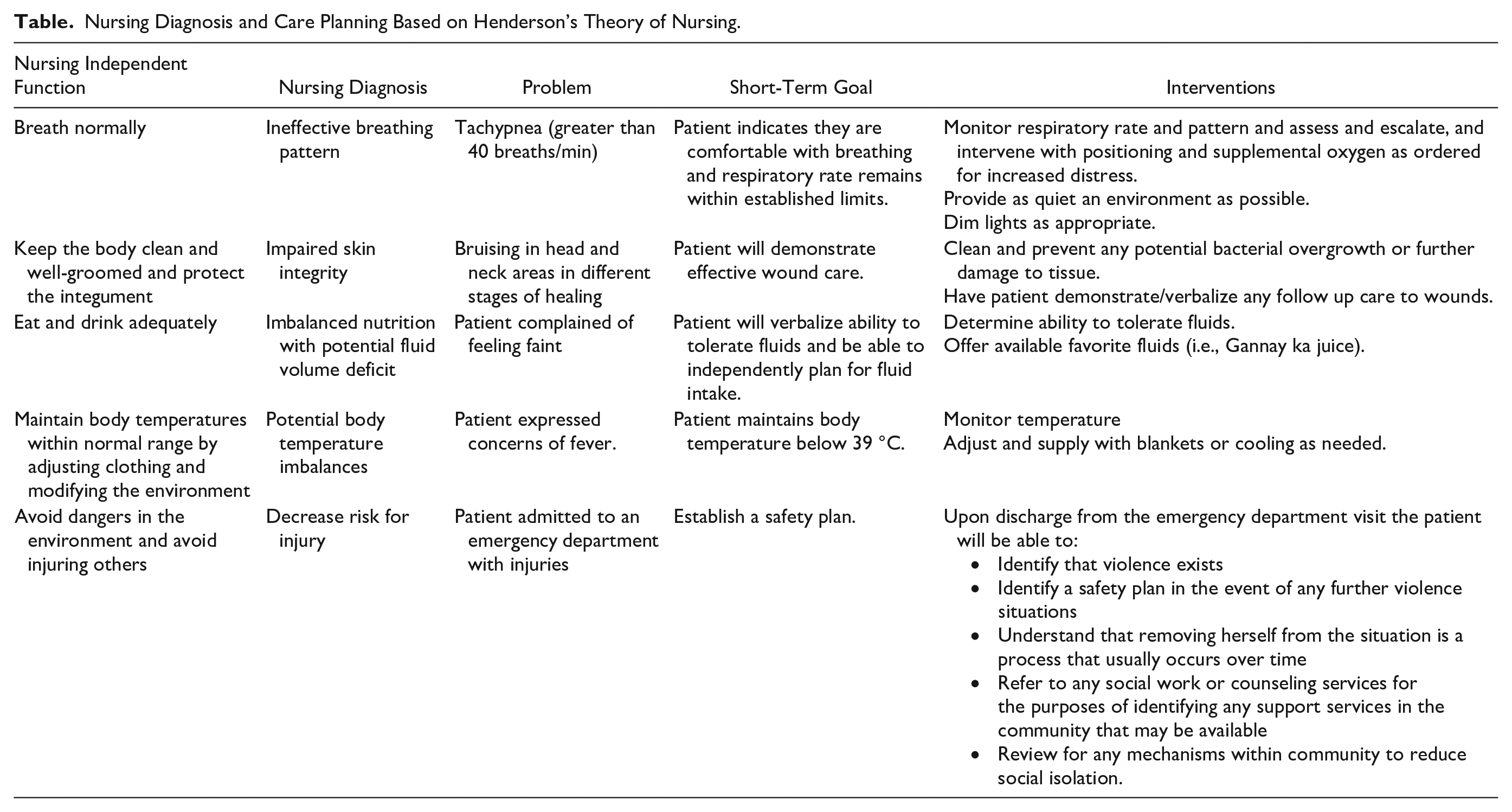
As previously mentioned, as important as it is to adroitly address physical supports and interventions it is also important to establish safety and follow up planning. For example, during the triage process, a pointed screening assessment, based on bruising and risk factors, provides a background to first promote confidentiality upon which safety planning can occur. Confidentiality sounds like a basic environmental intervention; it is worthwhile to keep in mind and, if possible, when there are other persons in the room, provide privacy during the intake process to unearth the person’s story. A couple of other noted confidentially and eliciting the person-centered story interventions include maintaining appropriate eye contact, framing questions so that they are nonjudgmental, providing space/time to answer questions, asking about being hurt, and avoiding phrases like victim, abused, or battered. The focus of the physical exam is to provide an environment promoting encounters secured for privacy. Attention to privacy promote the possibility that the physical exam providies a thorough opportunity to detect the warning signs of abuse. The presence and location of injuries are important. Any injury that does not have a good explanation, particularly injuries involving head, neck, teeth, or genital area, should raise suspicion. Wounds on the head and neck, particularly neck bruising, in some cases may be caused by attempted strangulation. As another example, wounds on the forearms can often occur when a person is in a defensive position. Bruises of different stages of healing may be present due to repeated instances of violence. Another pattern that can occur in cases of IPV is that persons may deny experiencing violence. Gently probing the nature and sequence of events becomes an important element in obtaining a complete picture. Persons may not feel safe in disclosing information, especially if questioned in an open situation such as an emergency department setting; there is a fear of information not being confidential, and persons might not be emotionally ready to provide this information, or persons might blame themselves. Privacy may provide the space to reflect and answer in a more thorough manner. Of note, there may also be feelings of shame and lack of comfort, and concerns of reprisal by the perpetrators of violence. These valid concerns of persons experiencing IPV points towards follow-up care in which persons are afforded additional opportunities to respond to safety inquires and safety planning in a private, sensitive manner.
The last nursing care plan function and problem addresses avoiding dangers and safety (see the Table). Before the person leaves the emergency room attending to the following elements needs to occur: spefic plans/referrals for follow up care, providing information onany potential local resources, and identification of a safety plan. It is helpful to have a listing within any emergency department of any potential community resources for follow up care. An important point to communicate is that the most dangerous time for persons experiencing IPV is often correlated with the decision to leave. A safety plan usually consists of the following: identifying a friend, neighbor, relative, or community shelter where the person experiencing violence can plan to go once the decision to leave has been made, or when an argument becomes heated. Most often a concentration on travel and keeping essential personal items to take in case there is a need to leave quickly are elements of a planning process. The other element to reinforce with persons experiencing IPV is that that they have the right to live without fear of violence.
While the complexities of interpersonal violence scenarios will not resolve in one emergency department encounter, attention to a nursing practice standards based on a theoretical model guides nursing care impacts in a more coordinated manner for person-centered outcomes. A takeaway from this scenario centers on having IPV screening as part of triage through discharge from the emergency department, particularly for patients with high-risk presentations. Implementing screening into triage workflows, implementing training materials for all nursing staff to review assessment screening triggers pointing potential IPV, and having safety materials concentrating on referral/community resources available are important. These mark independent nursing functions that guide and improve the care of persons. Lastly, a quality review and evaluation of case scenarios encountered by nurses reflects a continuous cycle of bettering nursing care functions, and thus patient outcomes. The usefulness of Henderson’s theory for better nursing care was shown in this scenario.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this review.
Funding
The authors received no financial support for the authorship and/or publication of this review.