
Abstract
Medicinal plants are used by many people with Type 2 diabetes in Iran. The aim of this study was to explore why this is so, from their perspective. Sixteen persons with Type 2 diabetes in Yazd City, Iran, were interviewed in April and May 2020 for this study. A thematic analysis of the transcripts of those interviews was done using MAXQDA 10 software. Six themes were identified: beliefs about medicinal plants, psychological factors, accessibility and economic barriers, patients' knowledge and awareness, social pressure, and the role of family culture. The recommendation of the study is that health counselors and specialists should provide needed information and skills for the proper use of medicinal plants, and the pharmaceutical infrastructures need to be expanded to provide enough drugs to facilitate better access to needed medication and reduce reliance on medicinal plants for persons with Type 2 diabetes.
Keywords
Diabetes is one of the most common chronic diseases in the world. It accounts for nearly 18% of deaths of individuals older than 25, and it is a leading cause of chronic kidney disease, blindness, and lower extremity amputation (Hippisley-Cox & Coupland, 2016). In Iran, the prevalence of diabetes in adults within the age range of 25-70 has been reported to be 11.9%, and it is expected to increase dramatically (Mirzaei et al., 2020). As elsewhere, Type 2 diabetes is the most common type.
Type 2 diabetes mellitus usually requires medication, physical activity, and a healthy diet to delay its progression and the development of complications. However, proper glucose control is difficult for many people to achieve because of the significant changes to behavior and lifestyle it demands. Moreover, diabetic medications are not always available or affordable in many places in the world. Thus, many people use medicinal plants to help them manage living with their disease (Alfian et al., 2016; Azizi-Fini et al., 2016). The authors report that these people use medicinal plants to help them control their blood sugar level, a key biomarker of disease management and secondary prevention of adverse effects of chronic high blood glucose on various organs and body systems. Medicinal plants are used in Iran for this purpose.
Azizi-Fini et al. (2016) reported that as many as 54% of people with Type 2 diabetes in Iran use medicinal plants to help manage their disease. There is also evidence from a study done in Egypt that use of medicinal plants is associated with non-adherence to conventional treatments and is associated with poor blood sugar control (Khalil et al., 2013). This was also found in a study in Pakistan (Raja et al., 2019). Therefore, better understanding of why persons with diabetes use medicinal plants instead of conventional diabetic agents is particularly important and a goal of this study in an Iranian population.
To understand the use of medicinal medication in Iran, it is important to consider the relevant social and cultural factors that are barriers and aids to effective diabetes management, as has been done in Jordan (Al-Sahouri et al., 2019). These authors reported that family, friends, and culture influenced persons with diabetes in Jordan regarding herbal use, as well as their food preferences. A study done in Uganda to determine the reasons persons with diabetes in that country used medicinal plants reported that people said that the shortage of common drugs, the distance from treatment locations, the relatively low price of medicinal plants, as well as advice from friends and traditional healers were the main reasons they gave for using medicinal drugs (Rutebemberwa et al., 2013). While this literature is suggestive, it remains unclear why medicinal plants are used in Iran; therefore, the present study aims to fill this gap in knowledge.
Design
The authors in this study used content analysis of the transcriptions of interviews with persons with Type2 diabetes mellitus in Iran about their use of medicinal plants.
Setting and Study Participants
The recruitment site was a diabetes research and treatment center, where the interviews were also conducted. The inclusion criteria were to be Iranian, be able to speak Persian, and be at least 18 years old. Patients with severe physical and mental complications of diabetes were excluded.
Data Collection
The data were collected by face-to-face in-depth unstructured interviews carried out in April and May 2020. The interview questions were created by experts in diabetes. To encourage the participants to go on, the interviewer used the phrase “can you explain more about this?” If participants were uncomfortable with any question, they could end the interview.
The researcher continued recruiting new participants and doing interviews until data saturation was achieved, which in this study was 16 participants. Efforts were made to include participants of diverse ages, economic status, and educational levels. To ensure confidentiality, all interviews were conducted in a private place in the diabetes center. The duration of each interview varied from 25 to 55 minutes. At the beginning of the interview process, the objectives of the study were explained to the participants. Moreover, the participants’ oral consent was obtained for recording the interviews. Field notes were taken for the purpose of data collection during the interviews to record non-verbal behaviors of the participants. Accordingly, the text of each interview was transcribed and typed in Microsoft Word.
Data Analysis
Qualitative content analysis was used for data analysis. The researchers read and analyzed the transcripts of the interviews several times over to identify the meaningful units (codes). Code extraction from texts of the interviews was conducted independently by two researchers. Next, the codes extracted by the researchers were summarized. Accordingly, some categories were defined for the significant units extracted by the researchers based on their internal consistency, with similar units placed in the same category. Next, the themes were defined into categories, and MAXQDA 10 software was used for further analysis. When all data were encoded and the categories were agreed upon, each category was checked for saturation.
Data Trustworthiness and Integrity
Lincoln and Guba's (1985) criteria were used to improve the trustworthiness of the results. These criteria included continuous involvement and comparison, participatory evaluation, researcher triangulation, and data saturation. To improve data transferability, detailed descriptions of the findings and categories were provided. Next, the data were reviewed by an external observer to ensure reliability of the study. To increase data validity, after reviewing the data and conducting the coding, the participants were provided with the results so that they could confirm them.
Ethical Considerations
To meet the ethical requirements of the study, written and informed consent was obtained from the participants, and the individuals were allowed to withdraw from the study whenever they wished.
Results
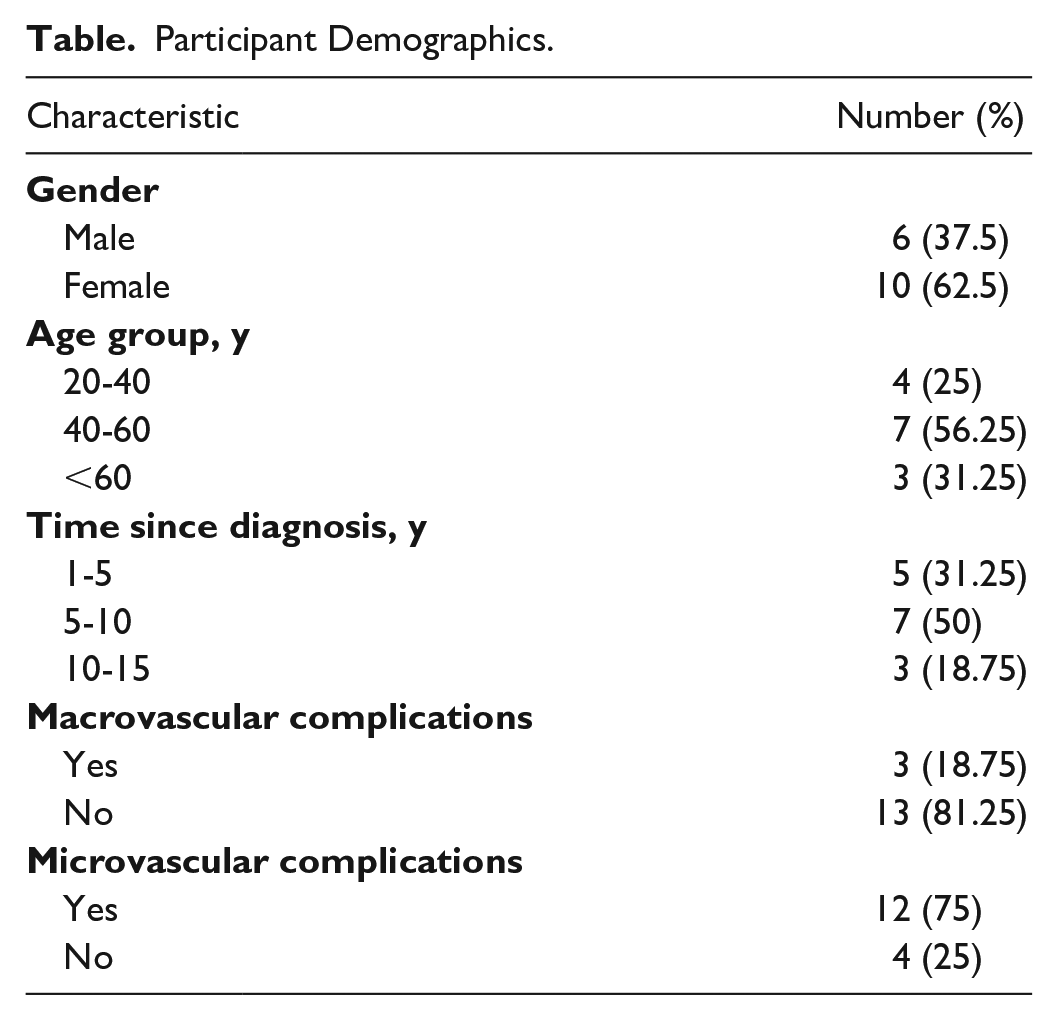
Most of the participants were female (62.5%). The largest age group was 40- to 60-year-olds, which was 56.25% of the participants (see Table for demographic data).
Participant Demographics.
Six main categories emerged from the data: beliefs about medicinal plants, psychological factors, patients’ knowledge and awareness, accessibility and economic barriers, social pressure, and the role of family culture. The first category was beliefs about medicinal plants.
Beliefs About Medicinal Plants
The first category includes five subcategories, which are trust in the medical effects from medicinal plants, feeling peace and refreshed after use of medicinal plants, having few side effects from medicinal plants, the compatibility of medicinal plants, and trust in complementary therapies.
Their trust in medical effects of medicinal plants is their belief that they improve the biomarkers related to their disease, such as improved results on two-hour blood glucose and HbA1c (Hemoglobin A1c) levels. One of the participants stated, “When I eat nettle, I feel that my blood glucose level decreases; besides, I measured it by a glucometer, and my blood glucose level had decreased” (a 60-year-old man). Another participant stated, “I used to brew fenugreek three times a day for 20 days. The test showed that my blood glucose level was around 120, which was very interesting to me” (a 30-year-old woman).
Most of the participants who used medicinal plants said they felt more refreshed and cheerful after taking them. They also believed that if they did not take them, they would feel more lethargic and bored. They said their physical and mental conditions improved, and they could do more daily activities when they took them. One of the participants stated, “Diabetes makes you bored, but when I drink herbal tea, I feel better, and I can do my daily chores much better” (a 62-year-old man).
Many patients thought medicinal plants were associated with less side effects than conventional drugs. They saw medicinal plants as more natural and less harmful. Most of the participants thought that medicinal plants could be used along with common drugs, as a supplement, that when taken together were more effective in controlling their disease. For example, one of the participants stated, “When I found out that drugs prescribed by my specialist failed to control my disease, I felt I needed to use herbal medicines; accordingly, I believe that taking herbal medicines along with the main drugs is very effective” (a 64-year-old woman).
Psychological Factors
The second category of findings was that anxiety about using medicinal plants was reported by many participants as an obstacle to their use. One participant said, “When I use brewed nettles, I feel distressed.” Some were afraid it would increase their risk of having hypoglycemia. One participant said, “When I use colocynth (bitter cucumbers), my blood sugar drops abruptly. This scares me so much and makes me feel so worried that I do not want to use it anymore” (a 52-year-old man).
Patients’ Knowledge and Awareness
The third category uncovered in the findings was that the patient’s understanding about dose and various preparations of medicinal plants were important factors. Participants were aware that the method of taking medicinal plants was important, as was the dose. They also were aware that improper use of medicinal plants could be harmful and damage the body. One of the participants stated, “If my wife does not prepare them for me, I will not use them on my own because I do not know how to brew them and how much of them to use” (a 46-year-old man). Another said, “Since I have studied more about harms and problems of medicinal plants than other people, I use them more cautiously” (a 35-year-old woman).
Accessibility and Economic Barriers
The fourth category relates to the cost of medicinal plants as compared with prescription medication and medical supplies. One participant stated, “Due to the sanctions imposed on our country, insulin pens have become scarce. Thus, I cannot buy them easily and must use fenugreek, nettle, and cinnamon instead of insulin” (a 61-year-old woman). Several participants blamed the high cost of prescribed medication as the reason they used medicinal plants. “I only have a pickup truck and cannot buy fruit because it is too expensive. Thus, sometimes even when I know my blood sugar level is high, I use brewed thymes or fenugreek instead of insulin pens" (a 59-year-old man).
Social Pressure
The fifth category derived from the participants’ comments is on the promotion of the use of medicinal plants by herbal therapists, relatives, and other persons with diabetes, which creates social pressure to use medicinal plants. A number of the participants reported that advice from their family and friends was the most important factor in increasing their willingness to use medicinal plants. Some participants referred to the significant role of traditional medicine practitioners and apothecaries, as well as advice from other persons with diabetes. “I used thyme because it was one of the patient’s recommendations. He said he had already used it, and it had good effects on improving his illness." However, several of the participants also stated that they would not use medicinal plants because their specialists did not find them useful. Accordingly, one of the patients said, “Many of my relatives ask me to use medicinal plants as well, but my doctor does not recognize these plants at all. Thus, I do not use them either” (a 45-year-old woman).
Family Culture
Related to but somewhat different from the above, the sixth category is described as the role family culture plays. Participants said that some of their key family members believed in the effects of medicinal plants and that they used them when they became sick. Furthermore, because of their use, they were able to see doctors less. One of the participants said, “In our family, when someone gets sick, my mother prepares some herbal medicines, so no one goes to see a doctor. Besides, my mother controls her diabetes with the same plants. I am very interested in these medicinal plants because our family has been using them for a long time” (a 36-year-old woman).
Discussion
The present study was conducted to explore the reasons persons with Type 2 diabetes give for their use of medicinal plants. Six categories make up the findings. Trust in the therapeutic effects of medicinal plant was mentioned by most of the participants as a reason for their use. In general, if persons perceived a benefit from taking them, it reinforced their use and they would recommend them to others. Thus, evaluation of the perceived outcomes of using medicinal plants is one of the major reasons for their use; this finding has been reported by others (Chang et al., 2012).
Thus, in developing educational programs for patients, it is useful to discuss trial of their use, reporting that some people do find them beneficial. According to this study, some people with Type 2 diabetes report feeling better after their use with low incidence of adverse effects. Some also believe they have less complications of diabetes because they take medicinal plants. However, they do look for and want more information. In addition, taking medicinal plants made them feel more cheerful and refreshed.
Bukhsh et al. (2020) reported that patients with heart disease also believed that medicinal plants improved their quality of life and reduced limitations of prescribed medications. Other studies have reported that many people consume medicinal plants along with prescribed medicines (Hashempur et al., 2015; Sheikhrabori et al., 2017). The participants of the present study believed that medicinal plants had fewer side effects, were safer, and were more compatible with the body than prescribed medications. This finding has been reported in several other qualitative and quantitative studies (Alameddine et al., 2011; Aziato, 2017; Dehdari & Dehdari, 2019; Jaam et al., 2017).
According to a few of the participants, they stopped using medicinal plants because of the anxiety and uneasiness they had taking them. They were aware that plants used for an illness had some side effects. Many participants were aware, and the rest need to be better informed that medicinal plants can cause complications, including gastrointestinal, liver, and neurological problems (Jouad et al., 2001). Thus, it is important for nurses and other health professionals to provide knowledge about drugs and medicinal plants. According to the participants of this study, the method of plant preparation and the dose are important. Some admitted that they did use herbal plants because they knew that they lacked the skill required to use them safely. It is also critical for nurses and other health professionals to ask patients about the dose of the medicinal plants they consume. Patients need to be better informed about the recommended dosage and time to take medicinal plants; this is particularly true for persons with Type 2 diabetes.
A key finding of this study was that several of the patients who take medicinal plants in Iran do so because they lack access to prescription medications, often because they cannot afford them. Dehdari and Dehdari (2019) also reported that cost was a key reason why many people do not take prescribed medication. This is attributed by many to the financial limitations and sanctions imposed on Iran. In Iran, as in many other countries, patients living in remote areas are not near any healthcare facilities or pharmacies and therefore use medicinal plants more (Hasan et al., 2011). Thus, the healthcare system needs public support and needs to be made a national priority. This includes localization of the production of medications and proper effective distribution, especially to remote and deprived areas.
In this study, the participants reported that family, friends, other patients, and some physicians encouraged the use of medicinal plants. This was also reported to be the case in the study of persons with diabetes done in Uganda (Rutebemberwa et al., 2013). In this study, the participants admitted that they often accept the advice of people important to them. Moreover, in Iran as elsewhere, many persons follow the advice of other patients with the same illness, with whom they share similar experiences, and this effects their health-seeking behaviors. According to this study, the cultural practices of the family contribute to the use of medicinal plants and foods in Iran. A similar finding was reported in a study of families of persons with diabetes in Morocco (Jouad et al., 2001). This is especially evident in countries where family ties and tribal customs are highly valued. Since Yazd, Iran, is a city with strong family ties and cultural beliefs, this issue was of high significance among patients with Type 2 diabetes.
Conclusion
The results of the present study showed that the experience of using medicinal plants in patients with Type 2 diabetes led to their continued use. This included the report that some persons with Type 2 diabetes take medicinal plants and they felt better, more cheerful and refreshed. Anxiety and uneasiness were factors that hindered their use for some people in the study. It is a key conclusion of this study that patients and families need more information about medicinal plants, including how to use them effectively. This advice and help should come from persons who specialize in helping people live with diabetes. In addition, the pharmaceutical infrastructures including manufacturing and distribution of medications need to be supported and improved in the country and worldwide. Nurses and other healthcare professionals need to appreciate the influence of family, friends, and other patients in regard to the use of medicinal plants. In addition, cultural factors and family customs remain a significant factor in the general use of medicinal plants for various diseases and aliments.