
Abstract
The purpose of the study was to determine the effects of motivational interviewing as based on Pender’s health promotion model (HPM) on diabetes self-management behavior among individuals with Type 2 diabetes. Apart from their routine care, the individuals in the intervention group were given a 30–45-minute motivational interview based on Pender’s HPM once a week for three months. Statistically significant differences were determined between the groups in the total score of the scales and its sub-dimensions (p < .05). The intervention applied in the present study can be used as an effective and easy method through which to develop and maintain diabetes self-management behaviors.
Keywords
Diabetes mellitus (DM) is a chronic, complex, and devastating disease affecting many people worldwide. It is also a disease that requires constant medical and nursing care (Vakilian et al., 2021). According to International Diabetes Federation (IDF) 2021 data, an estimated 537 million people aged between 20-79 years worldwide had diabetes. Individuals with Type 2 DM (T2DM) usually have difficulties in performing diabetes self-management behaviors, such as accessing an appropriate diet, exercising, self-monitoring of blood sugar, maintaining daily foot care, taking medication, and ensuring regular doctor control. T2DM requires attention to self-management behaviors (McDaniel et al., 2022). One of the biggest challenges faced in improving the health of individuals with T2DM is the invoking of behavioral change (Muslu et al., 2022). The role of nurses is important in preventing, treating, and controlling T2DM. This is because nurses develop strategies with individuals with T2DM, thereby involving them in their care and supporting their decision-making as to required behavioral change (Muslu et al., 2022). It has been reported that the giving of advice on disease management can create behavioral change among individuals with T2DM while mitigating disease complications that negatively affect the treatment being delivered. In addition, it has been stated that empowering individuals with T2DM through an understanding of the disease and by providing psychosocial education is beneficial in facilitating behavioral change (Harvey, 2015). To improve the self-management behavior among those with T2DM, enhanced focus should be given to activities such as their eating habits, physical activity, and regular use of diabetes-treatment drugs (e.g., insulin and oral antidiabetic). In addition, behavioral interventions, such as cognitive behavioral therapy and motivational interviewing, have been shown to instigate improvements in the diabetes control witnessed (Cradock et al., 2017). However, interventions such as special education programs and cognitive behavior-based programs for individuals with T2DM are not found to be integrated into the delivery of regular care. Thus, evidence-based and low-cost interventions must be integrated into existing care systems. Knowledge as to such interventions should be widely disseminated and their provisions should be open to all individuals with T2DM. A growing body of literature also indicates that nurse-led interventions within healthcare settings are well-received by patients and can be effective in achieving positive outcomes (Al Ksir et al., 2022). For this reason, interventions that employ behavioral strategies can support and help improve diabetes management among a significant proportion of the adult population affected by diabetes.
Pender developed the health promotion model (HPM) in 1982 to achieve improved health promotion behavior (Pridham & George, 1986). Pender’s HPM includes predictive and explanatory constructs of health behavior, perceived benefits, perceived barriers, behavioral emotions, perceived self-efficacy, and interpersonal and situational effects (Pridham & George, 1986). Pender’s HPM is among the most widely used models in identifying and changing unhealthy behaviors and in improving the health of individuals (Ren & Li, 2022). The model is particularly effective in reducing the risk factors and disease symptoms encountered among patients suffering from chronic diseases, therein promoting a healthy lifestyle among this group (Moshki et al., 2022). HPM assists patients receiving nursing care in choosing and performing behaviors that will improve their well-being (Pridham & George, 1986). One way through which to address lifestyle changes via Pender’s HPM, and thereby to achieve health promotion, is the use of motivational interviewing. Hence, this study considers whether motivational interviewing is useful as an aspect of nursing care whereupon it is integrated into the HPM.
Motivational interviewing has been used widely in the management of behavioral disorders. Previous studies spanning the past 30 years have reported motivational interviewing as an effective approach in improving health-related behaviors, thus having attracted attention as a patient-centered approach that can result in recommendations for behavioral change when individuals with T2DM feel uncertain toward the adaptation needed in their diabetes self-management behavior or lifestyle choices. Motivational interviewing is a highly effective approach for individuals who are ready to change their lives but who need such change to be encouraged (Ramadan et al., 2019). Motivational interviewing is thus a technique requiring evidence-based practice and the employment of a collaborative communication style administered by a person appropriately trained. It is only in this context that motivational interviewing can help individuals make decisions as to what changes are needed in their lifestyles and what motivations must be held (McDaniel et al., 2022). Motivational interviewing is “patient-centered” in nature, therein encouraging patients who identify themselves as facing a negative situation to explore their ambivalent feelings and subsequently to find appropriate solutions. Although motivational interviewing has shown benefits in improving outcomes for many diseases, its potential effectiveness in influencing outcomes in various adult populations with T2DM is particularly significant (Ekong & Kavookjian, 2016). When using motivational interviewing, it is important to plan for changing behaviors that are not suitable for diabetes self-management and to observe the disease adaptation process. In this regard, it is appropriate to use nursing models to develop diabetes self-management behavior and to change unhealthy behaviors. The power of Pender’s HPM in defining health does not limit nurses and other healthcare team members to specific interventions in reducing disease risk. Instead, the model offers nurses greater opportunities through which to study individuals, families, and communities in working toward better health, functional ability, and quality of life (Vakilian et al., 2021).
This study has evaluated the effectiveness of motivational interviewing based on Pender’s HPM in improving T2DM self-management behavior. The hypotheses held are thus:
Materials and Methods
Study Objective and Type
The study was designed and conducted as an interventional design with a pre-test/post-test control group to determine the effects of motivational interviewing as based on Pender’s HPM when applied to diabetes self-management behavior among individuals with T2DM.
Place and Time
The study was conducted between January 2019 and December 2020. The data were collected in a state hospital in Turkey (Gümüşhane State Hospital) between September 2019 and May 2020.
Population and Sample
The population of the study consisted of individuals diagnosed with T2DM. The sample of the study was determined via the power analysis method. The minimum sample size required for the study was calculated as 23 in each group, with a margin of error of 0.05 at a two-way significance level with an 80% representation power and a 95% confidence interval (Cohen, 1988). However, the study was conducted with 30 people in the intervention group (n = 30) and 30 people in the control group (n = 30). Participants were randomly assigned to the intervention group and the control group by a person other than the researcher, as arose in accordance with the participants’ order of admission to the outpatient clinic. The study was completed with 51 individuals, as 6 individuals in the intervention group and 3 individuals in the control group left the study.
Participants: Inclusion Criteria
The inclusion criteria of the present study required the participants
to be 18 years old or older,
to have been diagnosed with T2DM at least six months prior,
to have an HbA1c value of 6.5% or greater at the start of the study,
to have received diabetes self-management training in the preceding 6 months,
to be literate and able to speak Turkish,
to live in the city center,
to be able to perform diabetes self-management behaviors (i.e., a healthy diet, exercise, and/or blood sugar monitoring),
to not have any psychiatric disorders or a diagnosis of mental health problems.
Data Collection Instruments
The data collection instruments used in the study were the Descriptive Information Form, Diabetes Self-Management Self-Efficacy Scale, Healthy Lifestyle Behaviors Scale, Motivational Interviewing Importance-Confidence Rating Scale, Stage of Change Evaluation Form (decision balance), Blood Glucose Monitoring Chart, and Walking Monitoring Chart.
Descriptive Information Form
This form was a questionnaire created by the researcher, seeking to gain information on the sociodemographic characteristics of the participants, their diabetes status and diabetes control actions (e.g., type of treatment, duration, drug use, blood glucose monitoring and walking activity, and compliance with treatment status), and some laboratory information (fasting blood glucose [FBG], glycated hemoglobin [HbA1c], low-density lipoprotein [LDL], high-density lipoprotein [HDL], triglyceride, and cholesterol) as obtained from the patient’s hospital records.
Self-Efficacy Scale for Diabetes Self-Management
Van der Bijl et al. (1999) developed this scale and found its Cronbach alpha value to be 0.81. Kara et al. (2006) produced an intercultural adaptation of the scale. The scale consists of 20 items, graded via Likert-style scoring ranging between 1 and 5. The lowest score possible is 20, while the highest score possible is 100. The Cronbach alpha value of the scale for the current study was calculated as 0.94 at the first follow-up.
The Healthy Lifestyle Behaviors Scale
The scale was introduced by Walker, Sechrist, and Pender (1987). The Turkish validity and reliability was conducted by Esin (1999). There are 48 statements on the scale, graded via Likert-style scoring ranging between 1 and 4.
Motivational Interviewing Importance-Confidence Rating
The importance-confidence rating was between 0 and 10 (0 = not important at all; 10 = very important), with the confidence scoring being between 0 and 10 (0 = “I am not ready at all”; 10 = “I am very ready”). This rating determines the importance that individuals attach to the behavior that they want to change and their self-confidence (Dehghan-Nayeri et al., 2018).
Stage of Change Evaluation Form-Decision Balance
The form was created to determine the stage of change witnessed in the motivational interviewing.
Data Collection
The data of the current study were collected between September 2019 and March 2020. The researcher introduced herself to each participant and explained the main purpose of the study. Potential participants who were interested in taking part in the study were provided with an informed consent form and given adequate time to ask questions about the research. The participants’ data were collected using the Descriptive Information Form prepared by the researcher. This information included the metabolic variables of each participant (FBG, HbA1C, LDL, HDL, triglyceride, cholesterol), alongside their Healthy Lifestyle Behaviors Scale and Self-Efficacy Scale scores, to determine the behaviors demonstrated in relation to their diabetes self-management.
Intervention Group Participants
The participants who formed the intervention group were given an appointment by the researcher for a first motivational interview session. This session was produced to follow Pender’s HPM-based motivational interviewing approach in addition to the care they had previously received. This and subsequent sessions were designed by the researcher and conducted according to Pender’s HPM (detail given in the Figure). This intervention was carried out by the researcher for a total of 12 sessions across 3 months, with each session lasting approximately 30-45 minutes. During each session, a change (action) plan was created with the patient. The change plan was prepared specifically for each respective patient in line with their needs. In particular, the self-management behaviors that each patient wanted to change were considered. The walking and blood glucose monitoring forms were presented to the patients to encourage change. In the gait monitoring form, the days of the week and the time (minutes) for which they could walk were noted. The Turkish State provides a measuring device (glucometer) for every individual diagnosed with diabetes, leaving these measurements entirely to the patient’s discretion.
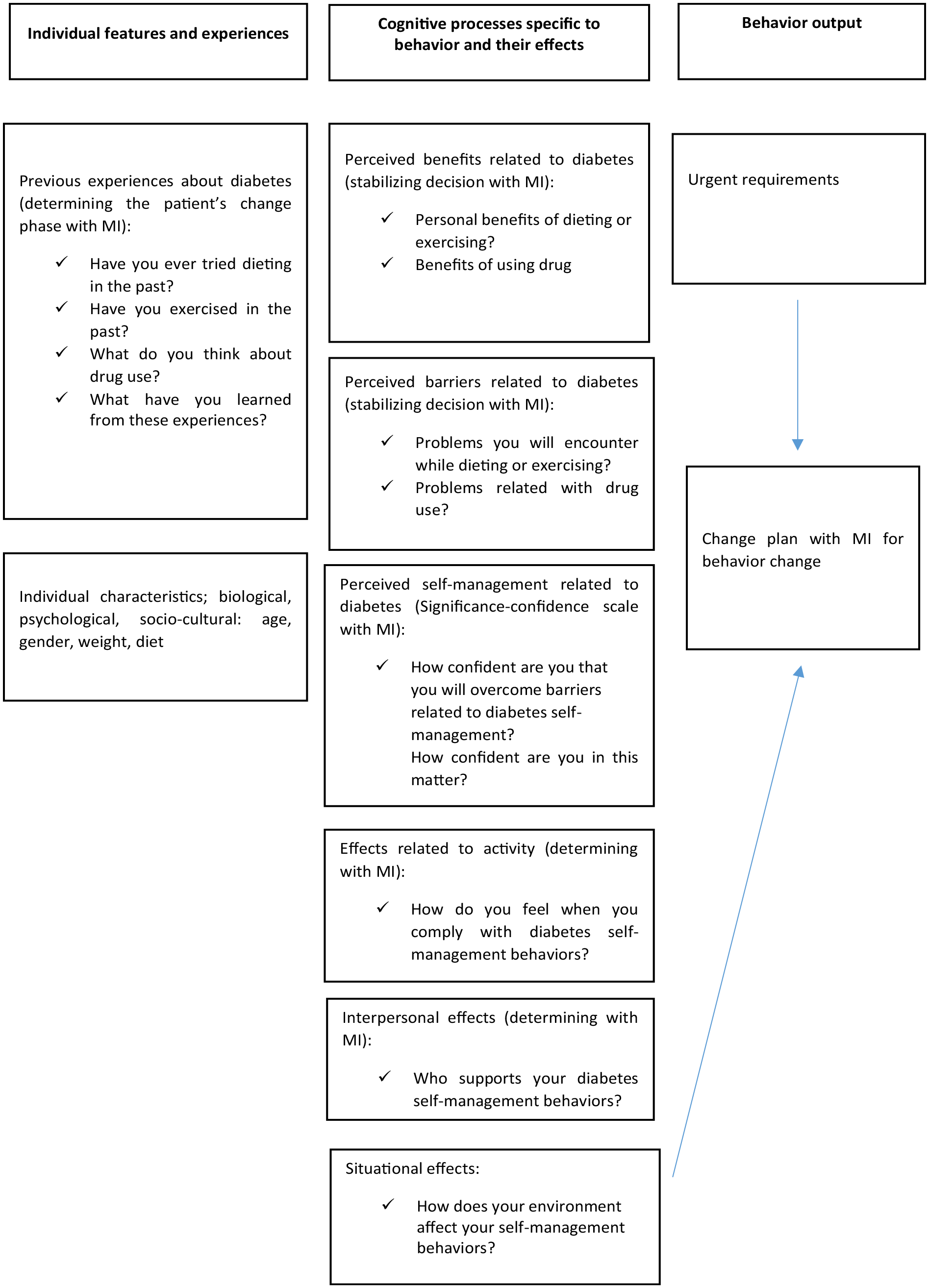
Design of MI for Individuals With T2DM According to Pender’s Model.
Motivational Interviewing Sessions
First Motivational Interviewing Session
Structure
Information was given about the role of the researcher and the goal of the research. The duration of the session was detailed alongside the remaining process of the study. In this context, the researcher asked the patient, “What do you have in mind? What would you like to talk about in regard to diabetes?”
Setting the Agenda
A range of questions were asked, including: “What are we going to talk about today?” “What would you like to talk about today? We can talk about having your blood sugar tested, healthy eating, taking your medications, or exercising/any diabetes self-management behavior?” and “Perhaps there is something else?”
Open-Ended Questions
After setting the agenda, the change stage of the patient was determined by asking open-ended questions about the participant’s prior experience with diabetes, according to Pender’s HPM. Here, a range of questions were asked, including: “Have you ever tried going on a diet in the past?” “Have you exercised in the past?” “What do you think about your medication use?” and “What did you learn from these experiences?”
Decision Balance
A conflict was created for participants by asking them to compare their current health behaviors with that of their ideal/desired health behaviors. After the decision balance was established, a change plan responding to the desired behavior change was prepared at the end of the session, which considered the suitability of the patient. The session was concluded by determining the day and time of the next meeting.
Second Motivational Interviewing Session
Opening
The attitude of the participant toward the change plan previously created (covering their diabetes self-management behaviors in relation to blood sugar monitoring, drug use, nutrition, and exercise, for example) was evaluated. From this, the agenda for the second session was created, and the session was opened. The individual’s perceived competence was strengthened by asking open-ended questions as to the perceived benefits of making change, thereby addressing the “personal benefits of dieting or exercising” and/or the “benefits of medication.” Attention was also given to the perceived barriers encountered, including the “problems faced when dieting or exercising” and the “problems faced with medication use.” Here, reflective listening was employed when appropriate.
Importance-Confidence Rating
The self-management perception of the participant regarding their diabetes was determined through asking questions such as: “How important are diabetes self-management behaviors (e.g., blood glucose measurement, medication use, healthy eating, and exercise) to you?” and “If you thought . . ., how confident are you in achieving it?”
Summarization
The participant and the researcher reviewed the highlights of the action plan of the motivational interviewing session. The next interview was scheduled, and the session was concluded.
Third Motivational Interviewing Session
Agenda
The previous week was reviewed, and a self-evaluation of the previous week was carried out. The session’s agenda was created in line with the change plan created in the previous session. The perceived barriers and how these situations were/could be handled were discussed to strengthen the confidence and competence of the participant. The perceived benefits experienced by the participant regarding the change sought/enacted were discussed. To determine the effects of the change on the participant in following the change plan, it was asked: “How do you feel when you follow diabetes self-management behaviors?” At the end of the session, the researcher offered a blood glucose monitoring form and a walking monitoring form to incentivize change.
Closure
The session was ended by reviewing the change plan. The next session was then scheduled. The other sessions continued in accordance with the Figure.
12th Motivational Interviewing Session
A summary of the previous meeting was undertaken, and the session was opened. General discussion was given as to change. The self-management behaviors of the participant were evaluated (as rated via the Healthy Lifestyle Behaviors Scale and Self-Efficacy Scale). Further, an appointment was made with the hospital to evaluate the participant’s metabolic variables, with these values being recorded later. The session was then ended.
Participants in the Control Group
The participants in the control group did not receive any treatment other than the physician’s recommendations (a regular intake of drugs and a controlled diet). The Healthy Lifestyle Behaviors Scale and Self-Efficacy Scale scores of each participant were collated by the researcher three months later, and the metabolic variables were measured again.
Data Analysis
The data collected in the research were inputted into the SPSS 22.0. Shapiro-Wilk normality analysis was used to determine the conformity of the measured parameters with the normal distribution witnessed. It was determined that all the measured parameters were in line with the normal distribution. The percentage, mean, and standard deviation values derived from the descriptive statistical methods employed were utilized in the evaluation. Statistical calculation methods, such as the t-test in paired groups, the t-test in independent groups, and the chi-square, were further used. The statistical significance level was set as p < .05.
Ethical Considerations
Prior to the commencement of the study, permission was obtained from Atatürk University, the Faculty of Nursing Ethics Committee (No: 2019-1/12) alongside the institution where the study was conducted (No: 49229421-044). The study complied with the principles of the Declaration of Helsinki. Verbal consent was obtained from the individuals participating in the study after the purpose of the research was explained to them. After the completion of the study, a motivational interviewing session based on Pender’s HPM was also performed with the respective participants in the control group.
Results
The descriptive characteristics of the participants (age, gender, marital status, educational status, occupation, income status, and household composition) are presented in Table 1. At a level of p > .05, the two groups were similar in terms of these characteristics.
Distribution of descriptive characteristics of the participants. a
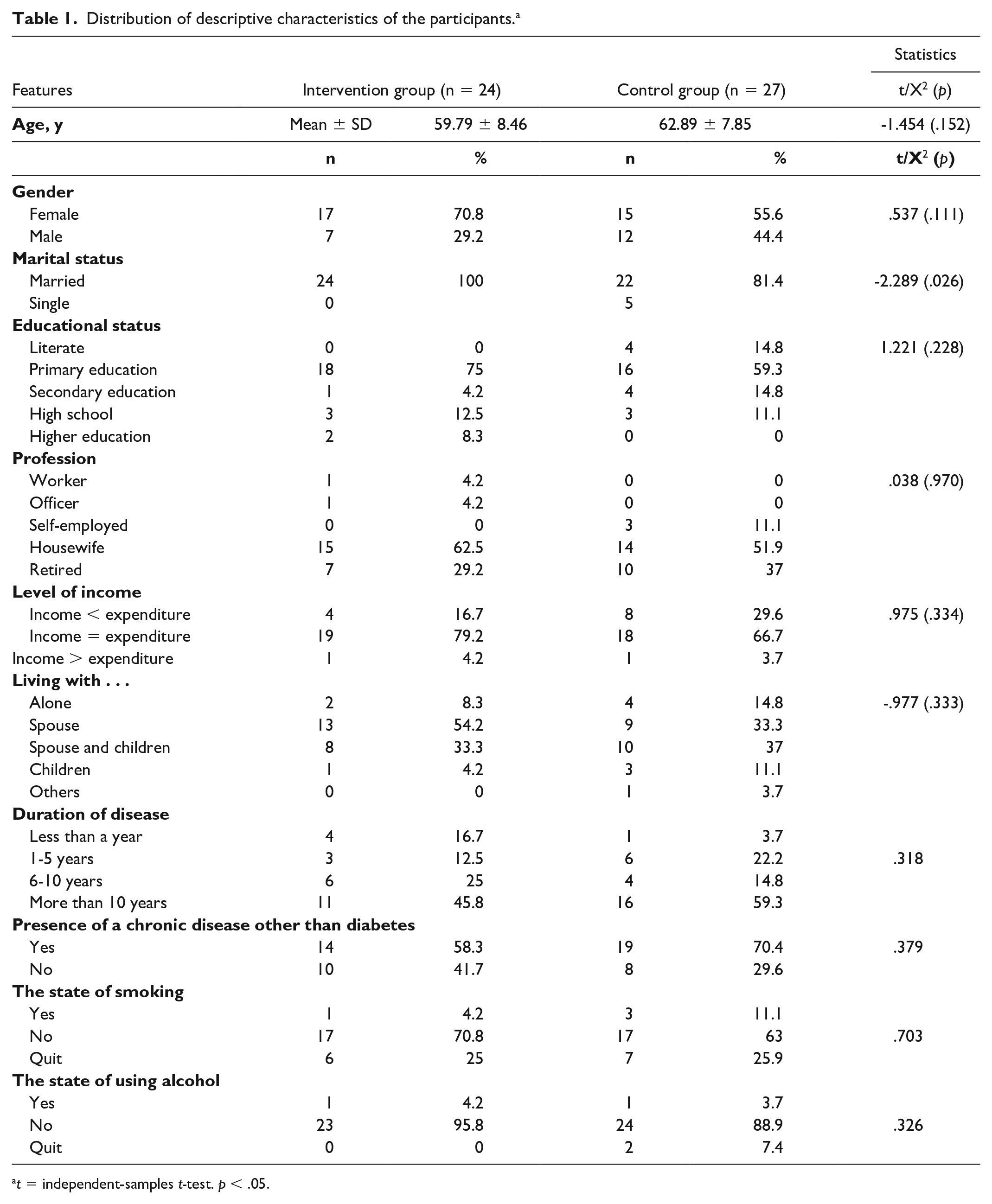
t = independent-samples t-test. p < .05.
The pretest/posttests related to the characteristics of T2DM (e.g., the duration of the disease, treatment, diet, regular drug use, frequency of blood glucose measurement undertaken) among participants of the intervention group and control group were calculated, with the results presented in Table 1.2. In relation to the pretest results, no similarity was found between the two groups in terms of the treatment type being received, with the difference between the groups being measured at .028 < p. Table 1.2 illustrates the significant difference witnessed between the types of treatment received, regular use of drugs, status and frequency of blood glucose measurements, exercise status, current diet compliance status, doctor control for diabetes, and current treatment compliance in the posttest results of the two groups (p < .05). There was no significant difference in the nutritional status recorded (.117 > p).
Pretest-posttest distribution of the T2DM-related characteristics of the individuals in the intervention and control group. a
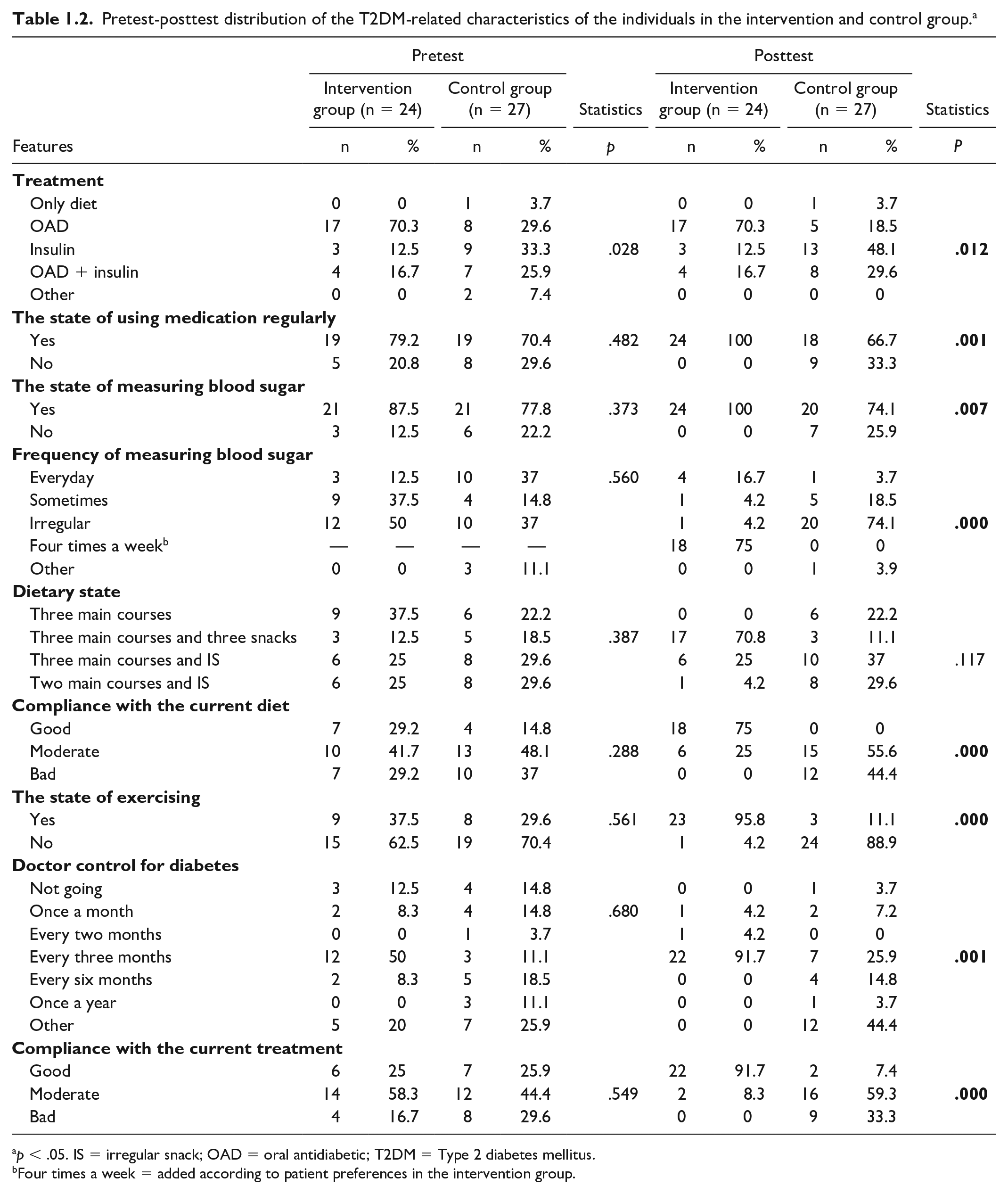
p < .05. IS = irregular snack; OAD = oral antidiabetic; T2DM = Type 2 diabetes mellitus.
Four times a week = added according to patient preferences in the intervention group.
The calculated pretest and posttest averages of the metabolic variables (HbA1c, blood cholesterol level, and FBG) of the participants in the intervention group and control group are given in Table 2. The groups were found to be similar in the pretest results (p > .05). However, in the posttest results, a significant difference was found in the intervention group in terms of the metabolic variables (HbA1c and FBG) (p < .05). For the blood cholesterol of the respective groups, these values were found to have decreased among the intervention group, yet no significant differences were detected between the groups.
Distribution of pretest-posttest results of metabolic variables related to T2DM in intervention and control groups. a
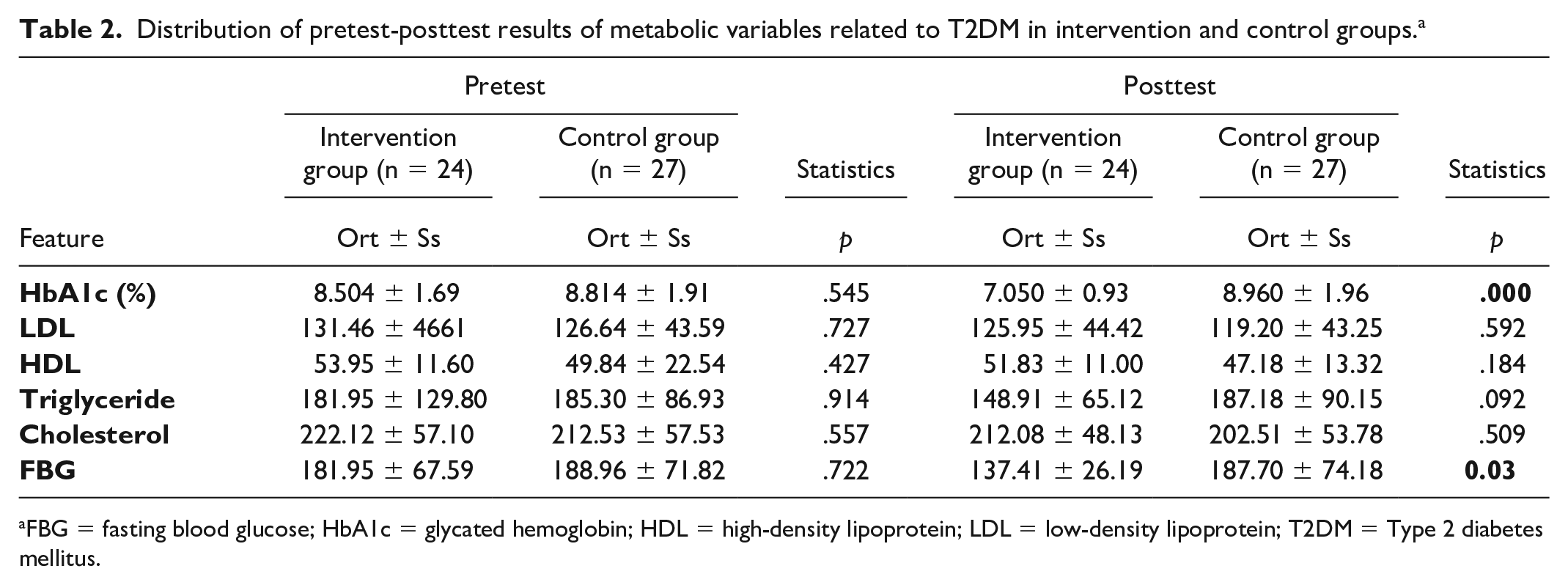
FBG = fasting blood glucose; HbA1c = glycated hemoglobin; HDL = high-density lipoprotein; LDL = low-density lipoprotein; T2DM = Type 2 diabetes mellitus.
The calculated pretest-posttest averages of the Healthy Lifestyle Behaviors Scale (and its subdimensions) and the Self-Efficacy Scale (and its subdimensions) among the respective groups are given in Table 3. For the posttest results of the groups, the total mean of the Healthy Lifestyle Behaviors Scale saw a significant difference between the two groups in relation to the subdimensions of self-actualization, health responsibility, exercise, nutrition, and stress management (p < .05). No statistically significant differences were detected between the respective groups in the subdimension of interpersonal support (p > .05). For the Self-Efficacy Scale posttest results of the respective groups, statistically significant differences were detected in relation to diet and foot control, medical treatment, and physical exercise (p < .05).
Distribution of pretest-posttest results of the groups for Healthy Lifestyle Behaviors Scale (HLBS) subdimensions and Self-Efficacy Scale subdimensions in T2DM. a
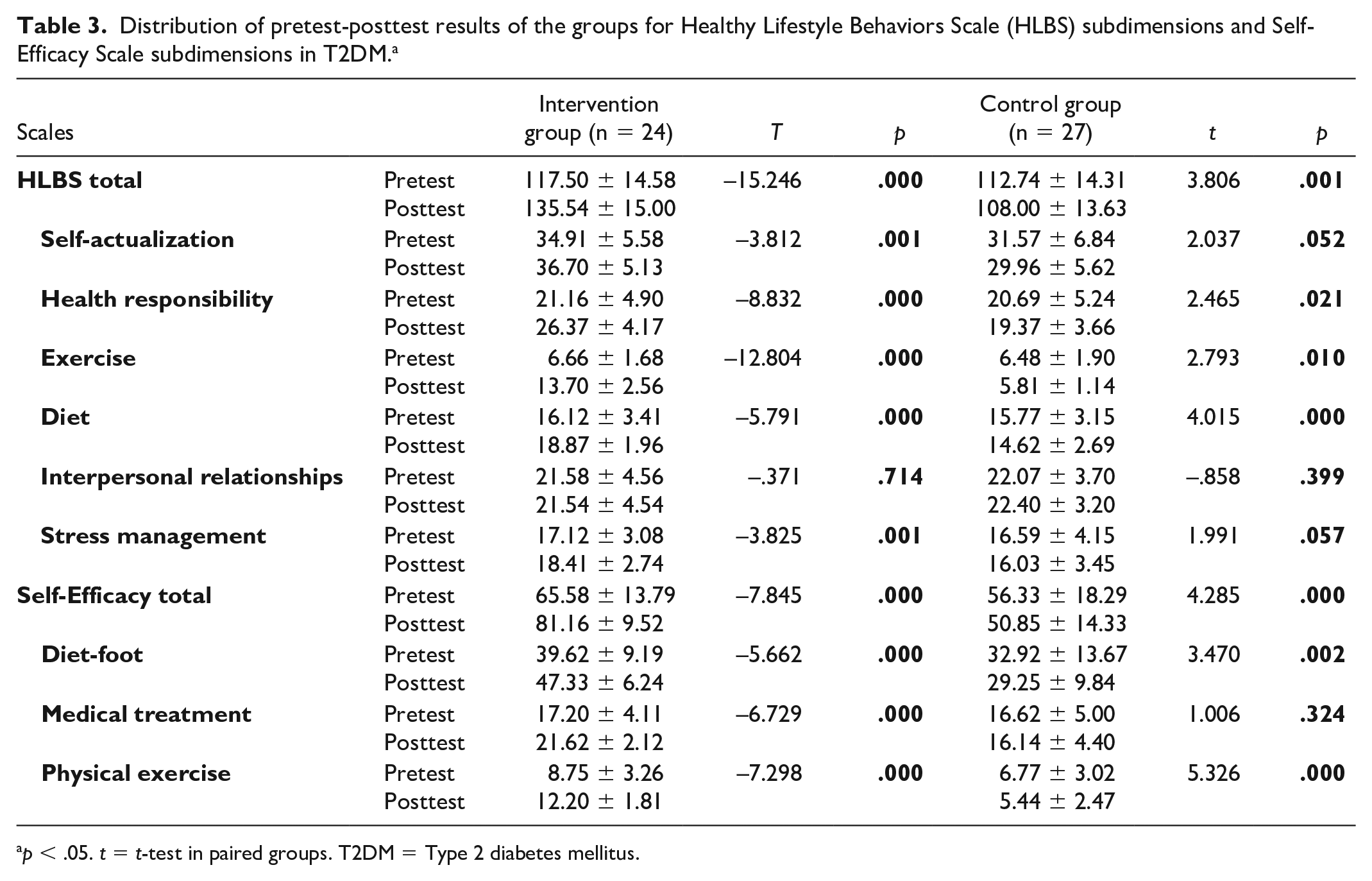
p < .05. t = t-test in paired groups. T2DM = Type 2 diabetes mellitus.
Discussion
In nursing, the use of theoretical models can improve health-disease understanding and may support the performance of nurses. Today, health-promoting behaviors are being focused upon due to their important role in enhancing the care provided to people (Moshki et al., 2022).
The results of the current study offer evidence that the use of motivational interviewing based on Pender’s HPM is more effective than traditional routine nursing practice in improving the health knowledge of individuals with T2DM. This result is consistent with those of Yujia and Menglong (Ren & Li, 2022). When the treatment methods of the participants in the present study were examined, the treatment types differed between the groups, with the use of oral antidiabetic (OAD) being high in the intervention group and the use of OAD, insulin, and OAD + insulin usage rates being close in the control group. This difference is thought to be due to the lifestyle changes undertaken and the treatment protocol initiated via OAD in the early stage of T2DM being replaced by OAD and insulin therapy due to the inability of some individuals to regulate their blood sugar in advanced settings. Literature has shown that the rate of OAD use here is over 50% (Cepeda Marte et al., 2019). This suggests that such an approach is not preferred due to the negative thoughts held by individuals with T2DM toward insulin, the responsibility of using insulin (in employing skills and timekeeping), the bruising common in areas where insulin is applied, and the fear of hypoglycemia. When the pre- and post-motivational interviewing Self-Efficacy Scale scores of the intervention group and the control group were evaluated in accordance with Pender’s HPM, it was found that the perception of self-efficacy had increased. On the other hand, the mean score of the subdimension of medical treatment was lower in the control group than at the pre-intervention stage, yet this difference was not at a significant level. It was found that individuals had the lowest score in relation to the physical subdimension. The fact that this score was much lower, especially among the control group, suggests that as physical exercise requires time and requires behavioral changes, the participants did not have enough motivation to instigate this behavior change. Similar studies to the present research have also demonstrated an increase in the scores of the Self-Efficacy Scale and its subdimensions (Lestari et al., 2022). Regarding the initiation and maintenance of self-efficacy in diabetes management, associated cognitive processes and their effects via the employment of Pender-based motivational interviewing, it is suggested that perceived self-management regarding diabetes management, the effects of important activity, and increased self-efficacy perceptions have been facilitated by inventions designed to invoke healthy lifestyle behaviors.
Motivational interviewing, as based on Pender’s HPM, might thus significantly improve the ability of diabetic individuals to undertake self-management behaviors. The total scores obtained from the Healthy Lifestyle Behaviors Scale, used to determine the diabetes self-management behaviors of the participants, showed a significant increase in the pretest/posttest results in the intervention group when compared to the control group. As a result of the Pender-based motivational interviewing intervention, a significant increase was detected in the total mean score of the subdimensions of self-actualization, health responsibility, exercise, nutrition, and stress management in the intervention group when compared to the control group, yet no significant change was detected in the interpersonal support subdimension. The increased scores in the motivational interviewing group in relation to the Healthy Lifestyle Behaviors Scale suggest that diabetes self-management behaviors (exercise and appropriate nutrition) were adopted, which are important in coping with diabetes. Behavior-specific cognitive processes and their effects, perceived diabetes-related self-management, and activity-related effects in HPM are therefore suggested as being important in initiating and maintaining self-management behavior. On the other hand, it is considered that interpersonal effects are not effective in the initiation and maintenance of diabetes self-management behaviors and that the intrinsic motivations of individuals must be uncovered. In the literature on patients with T2DM, the motivational interviewing intervention has been found to be effective in initiating and maintaining diabetes self-management behaviors (Li et al., 2020; Maslakpak et al., 2020). Here, statistically significant differences between the pretest/posttest results for HbA1c and fasting blood sugar, as the metabolic variables, play a key role in diabetes self-management. In the present study, the HbA1c value decreased by 1.5% in the intervention group and increased by 0.1% in the control group. Meta-analysis and systematic review studies conducted on motivational interviewing have demonstrated a significant decrease in HbA1c and FBG levels among participants accessing this intervention (McDaniel et al., 2022; Ramadan et al., 2019).
This finding is of interest to nurses and nursing management practitioners, particularly those involved in the field of nursing training, as it has implications for the design and teaching of healthcare promotion programs addressing diabetes. The results presented here are also important in the development of motivational interviewing intervention programs and strategies in the field of healthcare. In building upon this study, researchers could design more specific research aimed at promoting healthy lifestyles and identifying key components of health-related behaviors across different age groups, with motivational interviewing being used as a framework. In this way, Pender’s HPM will be enabled to produce a more comprehensive intervention effect.
Conclusion and Recommendations
In the present study evaluating the effects of motivational interviewing structured in accordance with Pender’s HPM on T2DM self-management behaviors, it has been found that the intervention group witnessed an increase in diabetes self-management behaviors when compared to the control group. According to these findings, it can be recommended that further studies are conducted to reduce barriers to health promotion behaviors and to invoke specific programs through which to increase self-management in such patients.
The evaluation of motivational interviewing in line with HPM in positively affecting the perceptions of patients toward chronic diseases besides diabetes may also be explored. In this area, it may also be found that such an approach can invoke lifestyle changes and increase drug treatment compliance. Motivational interviewing in accordance with Pender’s HPM among diabetic patients can become incorporated within training programs and certificate programs for diabetes education nurses. As a further step, motivational interviewing outpatient clinics may be installed. Thus, the findings of this present research may set a paradigm for future studies on the promotion of health and patient satisfaction among individuals with T2DM.
Limitations of the Study
No prior studies have been produced using HPM-based motivational interviewing among individuals with T2DM. Nonetheless, this study’s findings are limited to the sample group. The limitations of the present study pertain to the T2DM self-management behaviors scoring and motivational interviewing effectiveness based on the statements of the participants. To address this, in subsequent research, clinical results could be used as well as questionnaire data.