
Abstract
The authors describe the development of a model that focuses on how primary care providers can facilitate health promotion in older adults. The health-promoting self-care in older adults (HPSOA) model was developed through a synthesis of key concepts from the Health Promotion model and the Modeling Role Modeling Theory. Walker and Avant’s strategy for theory synthesis was used in its development. The model prioritizes rapport building to foster a trusting patient-provider relationship and focuses on long-term solutions to health promotion. Further model use through testing, research, and application in practice is recommended.
Older adults are living longer than ever. Across the globe, it is estimated that by 2050, the world’s population aged 60 years and older will double to 2.1 billion and persons aged 80 and over will triple to 426 million (World Health Organization [WHO], 2022a). Longevity is viewed as a positive health outcome, and through maintenance of health and wellness, older adults can lead active and productive lives. However, due to the biological, physiological, psychological, and behavioral processes precipitated by aging, older adults frequently experience less than ideal health trajectories that are fraught with limitations (Daly et al., 2019). Achieving an optimal state of health and well-being becomes challenging for this population.
Aging is the most significant risk factor for chronic illness, with approximately 78% of older adults having at least one chronic illness (American Psychological Association [APA], 2021). Disability secondary to falls also negatively affects older adults. Twenty-five percent of older adults experience a fall annually, and the risk of repeat falls doubles following an initial fall (Centers for Disease Control and Prevention [CDC], 2020). Furthermore, multimorbidity, frailty, and cognitive impairments associated with aging often contribute to decreased quality of life, polypharmacy, reduction in social networks, and increased service use (Daly et al., 2019). Educating older adults on how to engage in health-promoting self-care can improve their health trajectories and quality of life.
Health Promotion in Older Adults
Health-promoting self-care is described in the literature as preventive behaviors used to holistically promote health, optimize functional abilities, and improve overall well-being (Acton, 2002). The definition subsumes health promotion, disease prevention, and disease maintenance and management. It includes actions to promote and maintain health in the absence of illness as well as in response to acute illness or chronic illness management. The National Institute of Aging (2019) reported that health-promoting activities such as proper nutrition, physical activity, and healthy lifestyle choices delay the onset of chronic illness and disability and increase health, function, and well-being. In addition, Greenwood et al. (2019) reported that health-promoting self-care mitigated both the physical and psychological impact of aging among older informal caregivers. The physical and cognitive changes frequently experienced by older adults may make engaging in health-promoting self-care challenging despite the benefits (Daly et al., 2019). Healthcare providers (HCPs) play an instrumental role in educating and supporting older adults to promote their own health.
Primary care providers are well positioned to support older adults with this engagement. The primary care practice setting affords an entry point to the healthcare system and a focal point for all needed health services (American Academy of Family Physicians [AAFP], 2021). Primary care providers are responsible for delivering comprehensive healthcare by not only addressing acute and chronic conditions but also focusing on health promotion and disease prevention strategies (AAFP, 2021). Supporting older adults in health-promoting self-care is a reasonable expectation for primary care providers.
The collaborative patient-provider relationship facilitates engagement in health-promoting self-care (Keyworth et al., 2019). The partnership enables the provider to glean an understanding of the patient’s individualized needs and how best to tailor interventions to address them (Daly et al., 2019). In turn, the patients become motivated to adopt multidimensional, evidence-based, health-promoting self-care practices (Riegel et al., 2012). The patients are empowered to become more independent and attain an optimum state of health and achieve positive health outcomes (Daly et al., 2019). Establishing a collaborative patient-provider relationship mitigates key barriers such as a perceived lack of engagement or unwillingness to change (Keyworth et al., 2019).
The role of the primary care provider in addressing health promotion of the older adult may seem obvious. However, the lack of a clear theoretical framework to guide the execution poses a challenge. The concept of health promotion requires exploration of the individual involved in the activity and the provider facilitating it.
The purpose of this article is to describe the development of the health-promoting self-care in older adults (HPSOA) model. The model was developed through a theoretical synthesis of salient concepts from Pender’s (1996) Health Promotion model (HPM) and Erickson, Tomlin, and Swain’s (1983) Modeling Role Modeling (MRM) Theory. Walker and Avant’s (2019) inductive method of theory synthesis was used to explain how primary care providers can effectively collaborate with older adults to facilitate successful engagement in health-promoting self-care. In this article, primary care providers are identified as the HCPs and are defined as board-certified individuals who deliver care to older adults and can speak to promoting their health through self-care engagement.
Method of Theory Development
The two theories selected for this synthesis are the HPM and the MRM. HPM was chosen as it embraces a proactive approach, integrates self-care as a key concept, and recognizes the many contributing factors to engagement in health promotion behaviors. The MRM theory was selected for its description of a holistic client view and emphasis on the multifaceted role of the healthcare professional in collaborating with the client to successfully promote health. Furthermore, both theories have complementary philosophical and ontological worldviews that facilitate the synthesis.
The HPSOA was developed using Walker and Avant’s (2019) strategy for theory synthesis. The first step in the process is to specify focal concepts. For this synthesis, the focal concepts are health-promoting self-care and collaborative patient-provider relationship. The next step in Walker and Avant’s process is to review the literature and identify factors that are related to the focal concept (Walker & Avant, 2019). Health-promoting self-care is comprised of interrelated factors including health, wellness, and self-care. To understand the focal concept, health-promoting self-care, one must first understand the definitions of these factors. Health is a holistic state of physical, mental, and social well-being. The definition emphasizes that health is not merely the absence of disease or infirmity (WHO, 2022b). Furthermore, to achieve holistic health, one must commit to wellness, the active pursuit of activities, choices, and lifestyles (Global Wellness Institute, 2021). Self-care, described as one’s ability to promote and maintain health, prevent disease, and cope with illness and disability, with or without the support of the HCP, fosters the promotion of health and wellness (WHO, 2020). Self-care is also described in the literature as a process focused on improving health, maintaining optimal functioning, and increasing wellness in both health and illness states (Riegel et al., 2021).
The final step in Walker and Avant’s theory synthesis process is to integrate all factors and form the focal concept (Walker & Avant, 2019). Acton (2002) defined health-promoting self-care as preventive behaviors used to holistically promote health, optimize functional abilities, and improve overall well-being. It involves the active creation of time or opportunities for health maintenance (Oliveira et al., 2019). Health-promoting self-care includes actions taken in response to symptoms and health issues and refers to actions taken by individuals to promote health in the absence of a health problem (Acton, 2002). In this definition, the concept subsumes health promotion, disease prevention, and disease maintenance and management. Health-promoting self-care fosters health and wellness in older adults by mitigating the effects of the aging process and contributing to a longer, independent, self-sufficient quality of life (Golinowska et al., 2016).
Collaborative patient-provider relationship refers to a partnership between patient and provider that involves shared decision-making and cooperative coordination of care (Morley et al., 2017). The relationship is based on trust that creates an ethical responsibility for providers to place the welfare of patients above their own (American Medical Association, n.d.). Heath (2020) described a good patient-provider relationship as one where the provider serves as an advocate, listens, and explains information in an understandable way. A good patient-provider relationship was reported to be positively correlated to patient self-reported improved functional health status (Heath 2020). The relationship fosters collaborative decision-making that facilitates the implementation of an achievable action plan. These focal concepts guided the theory synthesis by depicting how the collaborative patient-provider relationship can successfully engage older adults in health-promoting self-care that results in positive outcomes.
Theoretical Overview
Health Promotion Model
Pender’s HPM embraces a proactive approach and comprehensively describes the contributing factors that affect individuals engaging in health promotion behaviors. Self-care is a key concept in this model. Pender’s (1996) HPM is based on social cognitive theory, and the expectancy-value characteristic assumes that clients will engage in an action if there is personal value, and the outcome is desired. Pender named several categories in the model.
In the Individual Characteristics and Experiences category of the model, Pender described that unique personal characteristics and experiences affect subsequent action. The variables include prior related behavior and personal, biological, psychological, and sociocultural factors. These elements reflect the client’s experience and will influence future engagement in health promotion behaviors. Pender addressed the motivation needed to engage in health behaviors in the Behavior-Specific Cognitions and Affect category. The client’s perception of the benefits, barriers, and self-efficacy of the behavior contributes to the level of motivation to engage in the targeted health behavior. Furthermore, a positive activity-related affect (attitude) and affirming interpersonal and situational influences will facilitate repeated engagement (Pender, 1996). For example, a client will be highly motivated to engage in an exercise program if they perceive it to be personally beneficial and without participation barriers such as cost or travel time. In addition, acceptance and available time to participate further contribute to a higher motivation level. In the category of Behavioral Outcomes, Pender acknowledged that engagement in a health behavior is initiated by a commitment to a plan of action. The plan includes a targeted behavior, timeframe for completion, and strategies to sustain the behavior and achieve a positive health outcome: for example, an individual choosing to walk for 30 minutes, three times a week during one’s lunch break for 4 weeks to promote stress management and improved sleep. Pender included a competing demand element that affects the commitment to a plan of action and the desired outcome depending on the level of control over it (Pender, 1996). Examples of competing demands include caring for an ill parent or working two jobs. A competing demand with significant control over the individual often leads to a poor outcome, whereas an individual who can mitigate the control of such a demand may experience positive results.
Strengths and Limitations of the Model
Pender recognized the unique needs of clients and focused on a proactive approach to health. However, the usefulness of the model is questioned as it does not clearly delineate the role of HCP. A clear description of this role would enhance generalizability. Although the HPM addresses the complexities of clients engaging in health behaviors, the model fails to explain how the collaboration between the HCP and patient facilitates the development of individually tailored plans of care (see Figure 1).
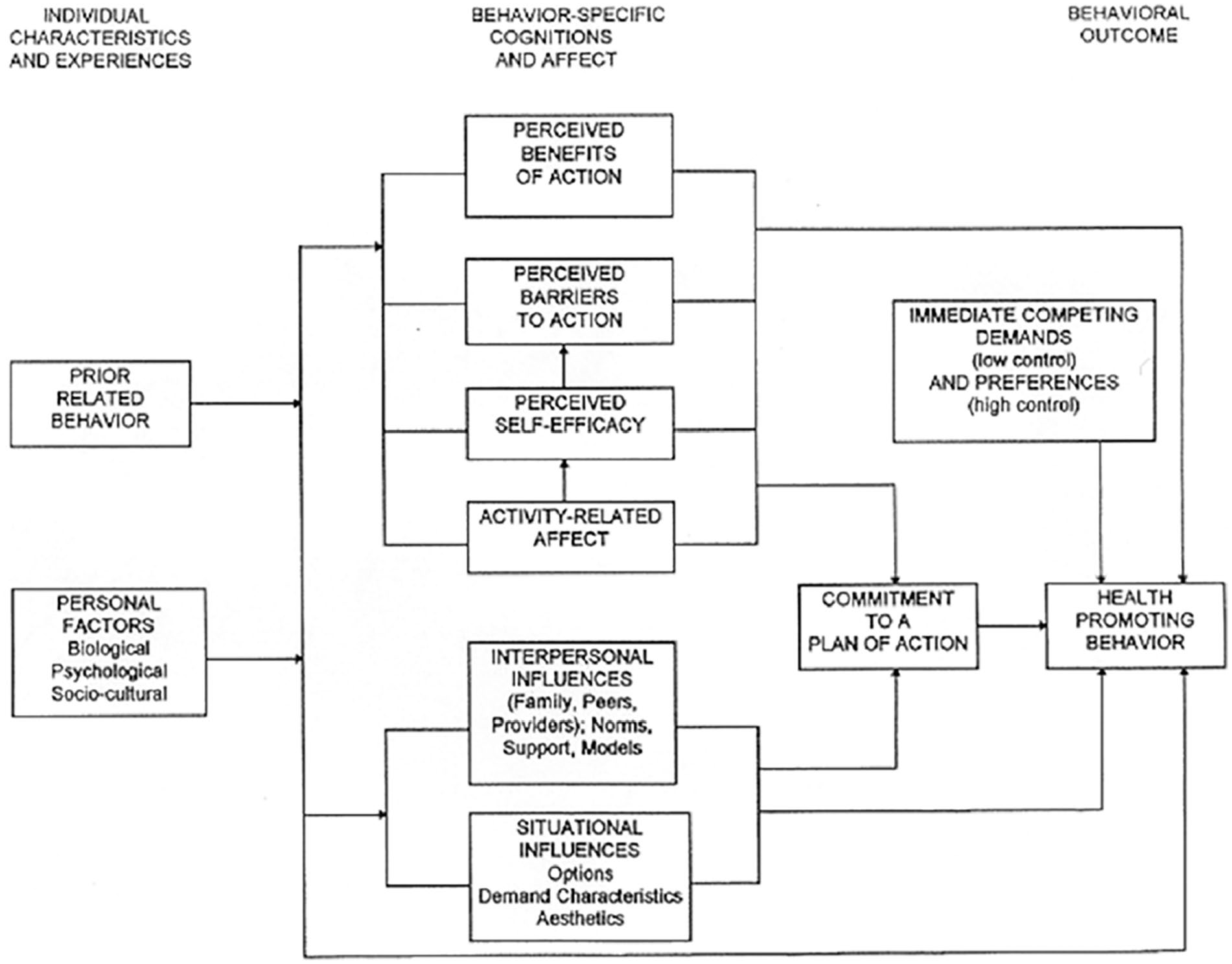
Pender’s Health Promotion Model (adapted from Pender, 1996).
Modeling Role Modeling Theory
The MRM theory is a middle-range theory that outlines the role of the HCP provider in “nurturing biophysical, psychological, social, and spiritual beings” (Erickson et al., 1983, p.2). MRM theory describes a holistic client view and the intimate relationship between client and provider. The theory “guides the healthcare professional in critical thinking, clinical decision making, and interventions” (Erickson et al., 1983, p. 2). Several concepts relating to human nature are incorporated in the MRM theory. Holism refers to the idea that human beings have multiple interacting subsystems. Affiliated individuation is the need to be dependent on support systems while simultaneously maintaining independence from support systems. Adaption is an innate response to stressors and drives individuals toward holistic health, growth, and development. Nurturance is the healthcare professional’s understanding of the client’s personal model of the world, which can be used to facilitate nursing care (Erickson et al., 1983).
MRM theory describes the two concepts of modeling and role modeling (Erickson et al., 1983). Modeling is the process a HCP uses to develop an image and understanding of the client’s world (Erickson et al., 1983). Using strong communication and assessment skills, the HCP gleans an understanding of the client’s perspective and ensures delivery of holistic care (Erickson et al., 1983). Role modeling precedes modeling and is the “facilitation of the client in attaining, maintaining, and promoting health through purposeful interventions” (Erickson et al., 1983). During the role-modeling phase, the HCP integrates assessment findings into individualized interventions that foster positive outcomes. The concept of nurturance is at the forefront in the role-modeling process.
Strengths and Limitations of the Model
The MRM theory explains how HCPs holistically care for clients and provides an understanding of their role in promoting health. The concepts of modeling and role modeling provide a clear process to guide practice. While the MRM theory uses the concepts of holism, adaptation, facilitation, and nurturance to explain the HCP’s role, it fails to address the interrelated and influential elements related to individual needs.
Development of the Health-Promoting Self-Care Older Adult Model
The HPSOA was developed through the synthesis of Pender’s Health Promotion model and Erickson, Tomlin, and Swain’s MRM theory. The selection process for this theory synthesis began with a critical appraisal of several models and theories from philosophical, theoretical, and conceptual perspectives. Pender’s model embraces a positive motivation philosophy to successfully engage individuals in health promotion activities. The model conceptualizes both the individual characteristics and experiences and the behavior-specific cognitions and affects that influence action. In addition to health promotion strategies to mitigate illness, the HPM prioritizes preventive measures to promote wellness. A strength of the model is its use in a variety of vulnerable populations across the lifespan. While the HPM assumes the HCP, in this case the nurse, collaborates with the individual to achieve positive health outcomes, the role of the HCP is not conceptualized and, therefore, is a limitation of the model.
Erickson, Tomlin, and Swain’s MRM conceptualizes the patient HCP encounter and supports the uniqueness and holistic view of each patient. The concepts delineated with the theory explain how the HCP, specifically the nurse, garners an understanding of the patient’s perspectives and develops a collaborative relationship. Neither theory alone fully captured the role of the HCP in facilitating health-promoting self-care in older adults. Synthesizing the theories allows better representation of the concept. Key concepts from the MRM were nested into the HPM to better explain the collaborative patient-provider relationship.
Assumptions
The HPSOA carries forward all the assumptions from the HPM and MRM, as listed below.
Assumptions of the HPM (Pender, 1996)
Persons seek to create conditions of living through which they can express their unique human health potential.
Persons have the capacity for reflective self-awareness, including assessment of their own competencies.
Persons value growth in directions viewed as positive and attempt to achieve a personally acceptable balance between change and stability.
Individuals seek to actively regulate their own behavior.
Individuals, in all their biopsychosocial complexity, interact with the environment, progressively transforming the environment as well as being transformed over time.
Health professionals, such as nurses, constitute a part of the interpersonal environment, which exerts influence on people through their life span.
Self-initiated reconfiguration of the person-environment interactive patterns is essential to changing behavior. (pp. 54-55)
Assumptions of the MRM (Erickson et al., 1983):
Nursing is a process between the nurse and client and requires an interpersonal and interactive relationship that is independent and in collaboration with a doctor.
Individuals are “born with an inherent desire to fulfill their self-potential” (p. 46).
Most notably, the HPSOA assumes individuals are born with the inherent desire to fulfill self-potential. In addition, the model assumes the HCP has unconditional acceptance of the patient’s worldview and conducts interactive encounters using strong interpersonal skills (Erickson et al., 1983). Furthermore, HPSOA recognizes that the HCP is part of the patient’s interpersonal environment and exerts influence throughout the life span (Pender, 1996).
Key Concepts of Health-Promoting Self-Care Older Adults
Modeling
The first phase of the HPSOA (Figure 2) involves the HCP engaging in modeling. This concept refers to the process the provider uses to develop an image and understanding of the client’s world (Erickson et al., 1983). The concepts of holism and adaption guide the provider in acquiring the patient’s worldview. Holism refers to the idea that human beings have multiple interacting subsystems, whereas adaption is an innate response to stressors that drives individuals toward holistic health (Erickson et al., 1983). The HCP explores the many interrelated and contributing patient factors that influence engagement in health-promoting behaviors, including family commitments, work obligations, and financial stressors. They must assess for the presence and degree of influence of the factors. The HCPs could inquire about the patient’s work obligations and the impact on family commitments. This may uncover key stressors for the patient. Based on the health issue being addressed during the encounter, the impact of these factors will vary. The HCP uses the concepts of facilitation and assists the patient in identifying antecedents and strategies to minimize interference to health (Erickson et al., 1983). The HCP may discuss with the patient how to integrate exercise into their daily life such as taking a walk at lunch, using the stairs, or parking farther away. This process is depicted in the model by a circle that contains the patient box and the holism and adaptation ovals. When all the pertinent assessment data has been collected, the next phase of the HPSOA begins.
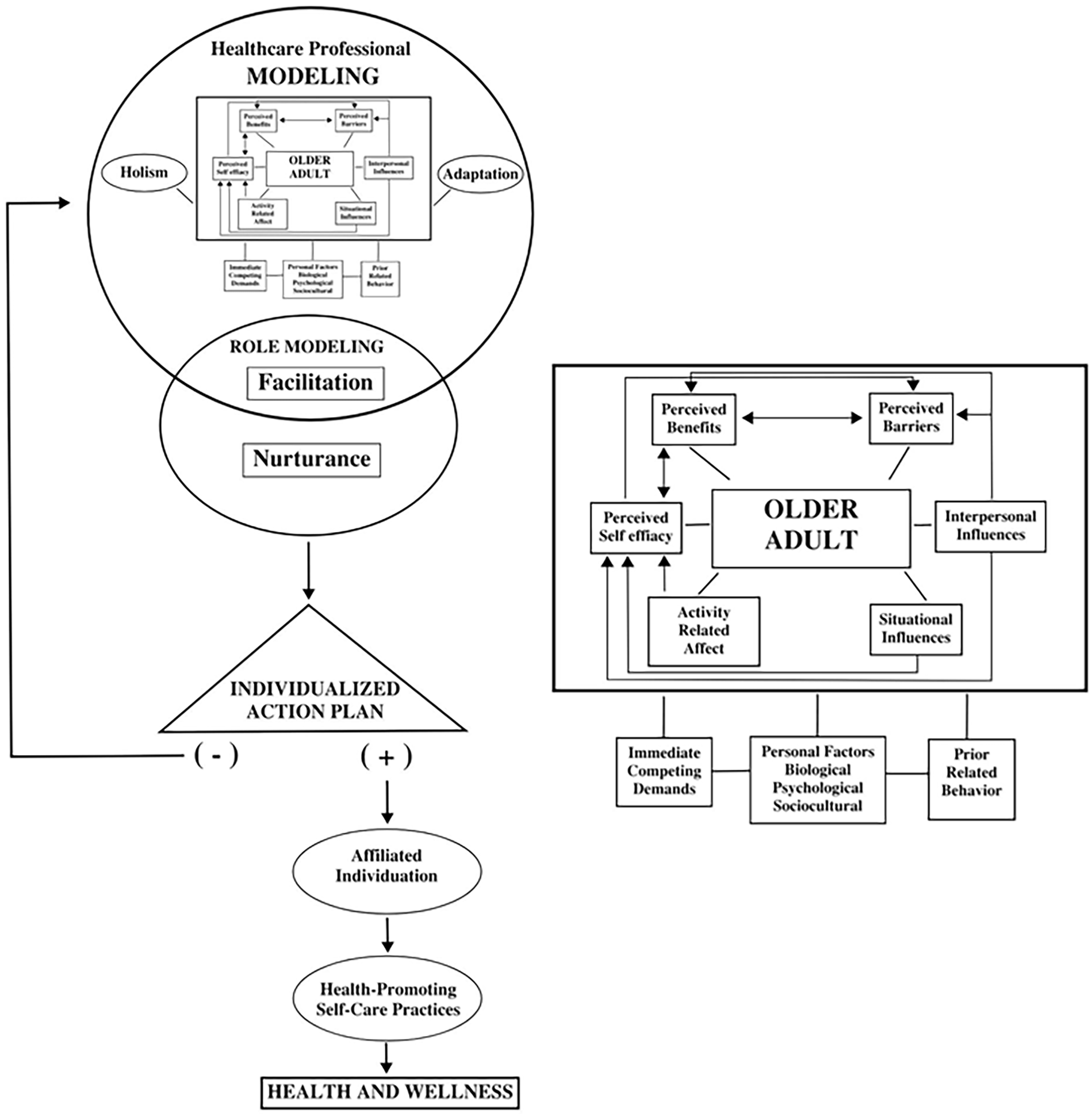
Health-Promoting Self-Care in Older Adults Model (HPSOA).
Role Modeling
The role modeling phase is next and begins with the HCP collaborating with the individual in attaining, maintaining, and promoting health through purposeful interventions. The HCP uses the concepts of facilitation and nurturance. Facilitation involves assisting the patient to identify, mobilize, and develop personal strengths in moving toward health. In using nurturance, the HCP synthesizes the assessment data and obtains an understanding of the patient’s world view (Erickson et al., 1983). Nurturance facilitates the development of an individualized plan of action. In the model, this is depicted by a downward-facing arrow connecting to the older adult’s individualized action plan (triangle). The modeling and role modeling phases may require an iterative process, going back and forth between them to acquire the necessary information. This is depicted by the two intersecting circles. A collaborative patient-provider relationship affords an opportunity to develop an individualized action plan (triangle) and outlines the accessible resources to attain the patient goal of participating in health-promoting self-care.
Individualized Action Plan
The comprehensive assessment conducted using modeling and role modeling leads to the development of the individualized action plan. Collaborative decision-making guides the development where patient and HCP cooperatively delineate action items to facilitate successful participation in health-promoting self-care. A lack of mutual agreement on the plan results in the provider and patient returning to the modeling and role modeling phases to garner an improved understanding. The arrow running from the triangle back to the intersecting circles represents this iterative process. Mutual acceptance of the individualized action plan allows the HCP to assist the patient to engage in affiliated individuation.
The iterative process of the modeling and role modeling phases are often the most challenging for HCPs. The following example demonstrates how to integrate into practice. A 76-year-old man is seen by a family nurse practitioner for hypertension. The mutually agreed upon action plan includes continuing on his antihypertensive medication and daily walks, purchasing a home blood pressure cuff, and limiting salt in his diet. During a 1-month follow-up visit, the client shared that the action plan had not fostered health promotion. Engagement in modeling reveals that the client’s health insurance no longer covers blood pressure cuffs, and he lacks the financial means to purchase one. In addition, a decrease in the client’s Supplemental Nutrition Assistance Program (SNAP) benefits resulted in selecting affordable food options that were significantly higher in sodium. Using role modeling, the HCP was able to collaborate with the client and revise the action plan. The client will stop by the senior center, which is on his walking route, for biweekly blood pressure screenings. The senior center partners with the local food pantry, so residents can access healthy, no-salt food options at no cost. The revised action plan included use of the senior center to support health promotion for this client.
Affiliated Individuation
The concept of affiliated individuation describes an individual’s need to be dependent on support systems while simultaneously maintaining independence from them (Erickson et al., 1983). During this phase, the HCP uses confidence building to empower the patient to independently engage in health promotion. At the same time, the HCP assists the patient to access available resources that will support the individual to consistently engage in the health-promoting activity. This phase of the model is depicted by the oval. Affiliated individuation is an individualized process, and the time to achieve it varies among patients. Ensuring that the concept of affiliated individuation has been properly achieved facilitates success with the health-promoting self-care behavior.
Achieving Health and Wellness
The final phase of the HPSOA is achievement of health and wellness through engagement in health-promoting self-care. This is represented by the last oval and rectangle in the process model. This behavior promotes growth and development and meets physical and emotional needs. Patients use their strengths to achieve positive health outcomes. It is during this phase that the patient acquires knowledge and mobilizes resources to maintain optimal health.
Discussion
Individuals across the world are living longer, and older adults now comprise a significant portion of the population demographics. Aging contributes to changes that affects one’s holistic health. Proactive approaches are required to prevent a decline in health, function, and well-being for this vulnerable population. The HPSOA model describes how HCPs can collaborate with older adults to gain an understanding of their unique needs and circumstances to guide them in the implementation of an individualized plan to promote health. Using this model in practice can enhance the quality of care delivered.
HCPs strive to produce positive health outcomes for every patient. Although evidence-based practice guides care delivery, each patient is complex and requires an individualized approach. To achieve success, providers must identify the strategies that align best with needs of each patient. The HPSOA model prioritizes rapport building to foster a trusting patient-provider relationship. This creates a solid foundation for open communication and collaborative decision-making to yield an achievable action plan. Regular follow-up to evaluate action plans is necessary to maintain positive outcomes and promote health in older adults.
The primary care setting may be a limiting factor for the HPSOA model. With an average visit time of 18 minutes, many HCPs are not afforded sufficient time to engage in meaningful conversations around health promotion (Crist, 2017; Neprash et al., 2021). Shorter consultation times have been linked to poorer health for patients (Crist, 2017). This will become increasingly important as our population ages. To ensure affordable, high-quality healthcare for older adults, a strong primary care infrastructure is needed (Crist, 2017). The HPSOA model focuses on long-term solutions to health promotion in older adults. To successfully achieve this outcome, longer patient encounters inclusive of health promotion into routine care are warranted. However, this system-level change will not be resolved immediately, and implementation of mitigation strategies for the current situation should be considered. Including a brief narrative summary of client perspectives and concerns within the office visit note serves as a reminder of topics for further exploration during follow up visits. This strategy minimally affects provider workflow yet conveys that the HCP is actively engaging in the client’s world and is committed to collaborative decision-making.
Research is instrumental for advancing the HPSOA model. Health-promoting self-care in older adults is defined by a variety of perspectives. Investigating ways to enhance the collaborative patient-provider relationship may contribute to improved health outcomes. Nursing research facilitates comprehension of these concepts to ensure that many dimensions are explored to promote high-quality healthcare for older adults. The model can be studied globally in the context of certain illnesses and conditions such as diabetes, hypertension, arthritis, and depression. In addition, subsets of the older adult population, such as women of color, men, and people with disabilities, should be considered to evaluate this model. An exploration of how this model can be applied to older informal caregivers is detailed below.
The HPSOA model ungirded a study exploring the knowledge, attitudes, and practices of primary caregivers in assessing and supporting older informal caregivers (Sabo et al., 2022). The model appropriately depicted the collaborative patient–healthcare professional relationship essential to promoting health within this population. Sabo et al. (2022) found that despite positive attitudes, knowledge deficit and system-level barriers interfered with the integration of a caregiver assessment in primary care practice. Furthermore, a caregiver identification process, user-friendly assessment tool, and system-level changes are needed to ensure the delivery of high-quality holistic healthcare. Results from this study enhance understanding of the collaborative patient-provider relationship and identify additional concepts to incorporate in the model.
Application in the Sabo et al. (2022) study revealed how HCP attitudes may create potential barriers in successfully using the collaborative patient-provider relationship to promote health. Attitude was a contributing factor in the modeling phase. During this phase, the HCP is garnering an understanding of the patient’s worldview. Therefore, it requires HCPs to have a positive attitude toward their role in the patient encounter. HCPs must value the process of conducting comprehensive assessments to develop tailored plans of care that support unique patient needs. Equally important is a positive attitude toward their ethical responsibility of promoting patient health as an integral component of the healthcare delivery system. Attitude affects the outcome of the modeling phase and the extent to which HCPs are committed to understanding the patient perspective. Sabo et al. (2022) found that despite a positive attitude toward assessing and supporting older informal caregivers, knowledge deficit interfered with engagement in health-promoting self-care.
HCP knowledge is another element that influences the modeling phase. Providers must be knowledgeable of the benefits of a collaborative patient-provider relationship and effective strategies to develop rapport and trust in clinical practice to achieve it. This allows the HCP to understand the key characteristics, lived experience, and potential health risks of their older adult patients. Knowledge deficit interferes with the collaborative process and the HCP’s ability to use facilitation and nurturance. Thus, the HCP fails to glean a true understanding of the patient’s worldview. Patients are not empowered toward health behaviors, and individually developed action plans do not address key health priorities. The outcome of this interaction jeopardizes future patient-provider encounters. This knowledge deficit affects practice. Sabo et al. (2022) found that knowledge deficits among HCPs led to inadequate assessment and support of older informal caregivers.
These research findings lead to further development and testing of the HPSOA model. As additional information is gained from other studies, refinements to the model can be made. Research findings may lead to the integration of additional concepts into the HPSOA model. Preliminary results suggest that knowledge is a concept that may need to be included in the model (Sabo et al., 2022). Exploration of how knowledge is defined and best used by the provider in the modeling phase warrants further investigation. Using the HPSOA model as a theoretical foundation in other research studies will provide further opportunity to clarify the concepts in the model and strengthen the model.
Conclusion
The HPSOA uses the collaborative patient-provider relationship to facilitate patient engagement in health-promoting self-care. The model provides a sound theoretical framework to guide HCPs in empowering patients toward better health. The model delineates how the HCP effectively uses the patient encounter to ensure positive health outcomes. Key concepts instrumental in the process are described. Further application of the model as a theoretical framework for research will clarify the need for revisions. Adopting the HPSOA model in practice can guide primary care providers to actively facilitate older adults to engage in health-promoting self-care behaviors that ultimately improve their health trajectories and quality of life.