
Abstract
This paper reports on the finding of a systematic review and meta-analysis of studies from around the world on burnout of nurses working rotating shifts compared with fixed shifts. The present systematic review and meta-analysis was registered in PROSPERO with ID No. CRD420261380531. CINAHL Complete, PubMed, Scopus, and Web of Science were used. We included all quasi-experimental, observational, cross-sectional, retrospective, and prospective studies recording scores in burnout and related dimensions comparing nurses who worked fixed shifts and those who worked day shifts. Our findings revealed no statistically significant differences between the two groups across all analyses, despite the presence of high and statistically significant heterogeneity (.0001 ≤ p ≤ .03). Additional research is needed to assess shift work factors that may contribute to burnout.
Keywords
Nursing is well understood to be a stressful profession (Decker, 1997), in part because most nurses are caring for persons who are ill and suffering and many nurses care for persons who are at the end of their life (McGrath et al., 2003). In addition, nurses often deal with emotionally charged requests from patients, heavy workloads, long shift and rotation schedules, and organizational and interpersonal conflicts (Zhang et al., 2025). All of these are occupational stressors that can contribute to mental health disorders (Dewa et al., 2014; Portero & Vaquero Abellán, 2015).
Among these disorders, burnout is the most frequent (Vitale et al., 2020). Burnout has been described as a psychosocial syndrome due to exposure to chronic occupational stress involving three main subdimensions: emotional exhaustion (EE), depersonalization (DEP), and reduced professional achievement (PA) (Maslach et al., 2001). The evidence is clear that burnout reduces work productivity and increases absenteeism (Dewa et al., 2014). Burnout also increases restrictions in nursing practice, intention to leave the profession, poor quality of care, and clinical errors and weakens patient safety (Getie et al., 2025).
Because of recent economic changes, nurses’ working conditions have become worse. In many countries, nurses’ workloads have increased as staffing shortages, work uncertainty, and job insecurity have increased (Velando-Soriano et al., 2024). Additionally, demographic and occupational factors like age, gender, marital status, income, educational level, years of experience, department assignment, shift patterns, nurse-to-patient ratios, and job category negatively affect burnout levels (Alenezi et al., 2019). These results underline the crucial requirement for strategies aimed at supporting the mental health and well-being of nurses.
One particularly stressful part of hospital-based nursing is required shift rotation schedules. Additional studies have associated certain shift schedules and emotional exhaustion (Dall’Ora et al., 2015; Stimpfel et al., 2012). The Job Demands-Resource model suggests that shift work increases job demands without providing sufficient job resources and contributes to burnout (Demerouti et al., 2001). The present systematic review and meta-analysis aimed to assess any differences between work burnout and its related subdimension scores between shift and fixed-shift nurses around the world.
Materials and Methods
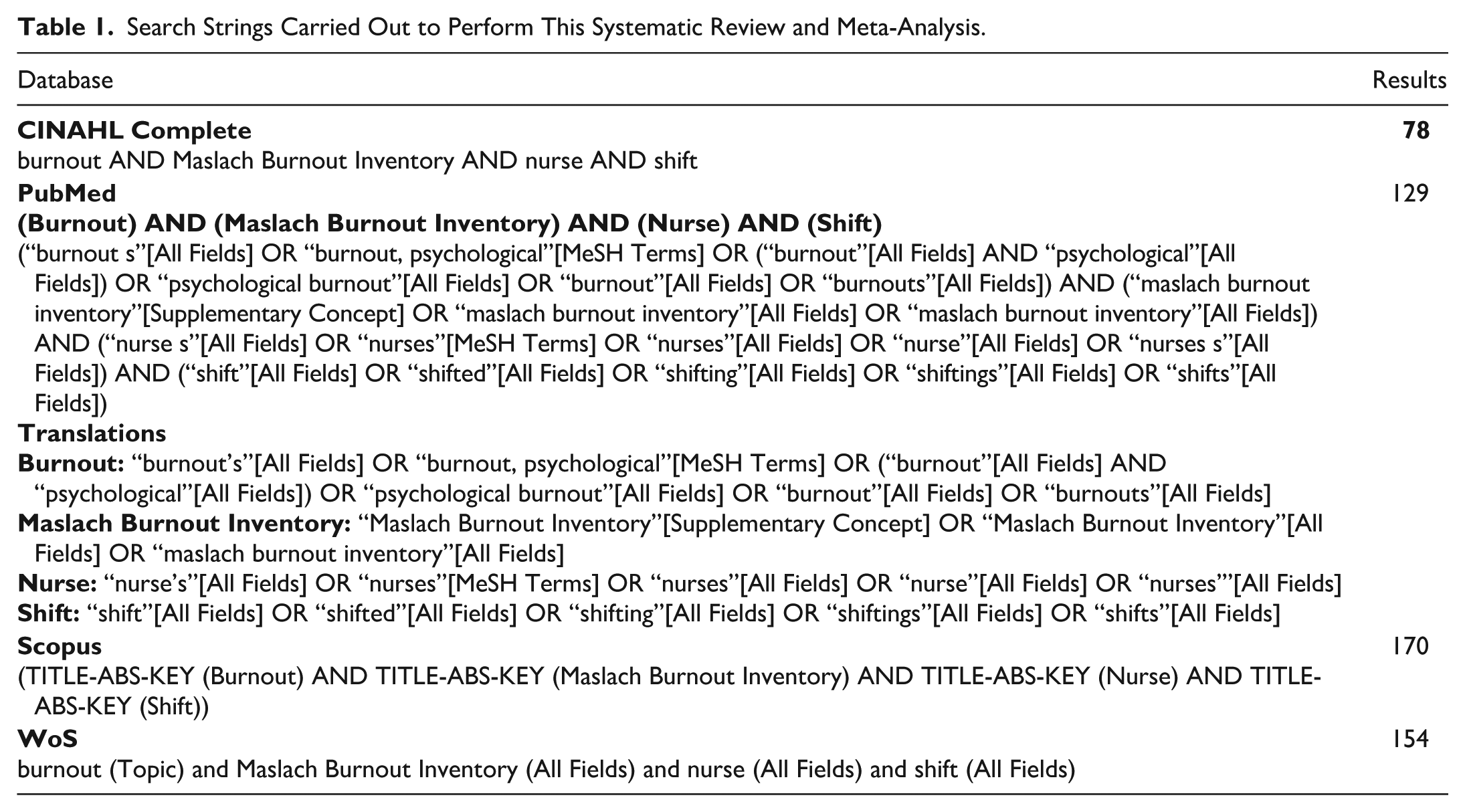
This systematic review and meta-analysis was registered in PROSPERO with ID No. CRD420261380531 and performed according to the PRISMA checklist (Page et al., 2021). CINAHL Complete, PubMed, Scopus, and Web of Science databases were consulted through MeSH terms combined with Boolean terms, as displayed in Table 1, for search strings carried out to perform this systematic and meta-analysis study.
Search Strings Carried Out to Perform This Systematic Review and Meta-Analysis.
Types of Study to Be Included
This review included all quasi-experimental, observational, cross-sectional, retrospective, and prospective studies that recorded scores on burnout and related subdimensions (EE, DEP, and PA) between nurses who worked fixed shifts and nurses who worked during all shifts.
Data Selection and Coding
Initially, records were identified through a systematic database search and uploaded, and duplicate studies excluded. Then, two independent reviewers (E.V. & K.H.) assessed the title and abstract of the identified records, and unsuitable reports were removed. After that, articles were uploaded, and the full text was assessed for eligibility. Any disagreements for the inclusion-related record was resolved by discussion and consensus. Data collection was extracted by considering study characteristics (author, year of publication, aim, design, sample size, setting), participants (age, cancer stage), and means and standard deviations in burnout total scores and subdimensions, like EE, DEP, and PA (see Figure 1 for the PRISMA flow chart).
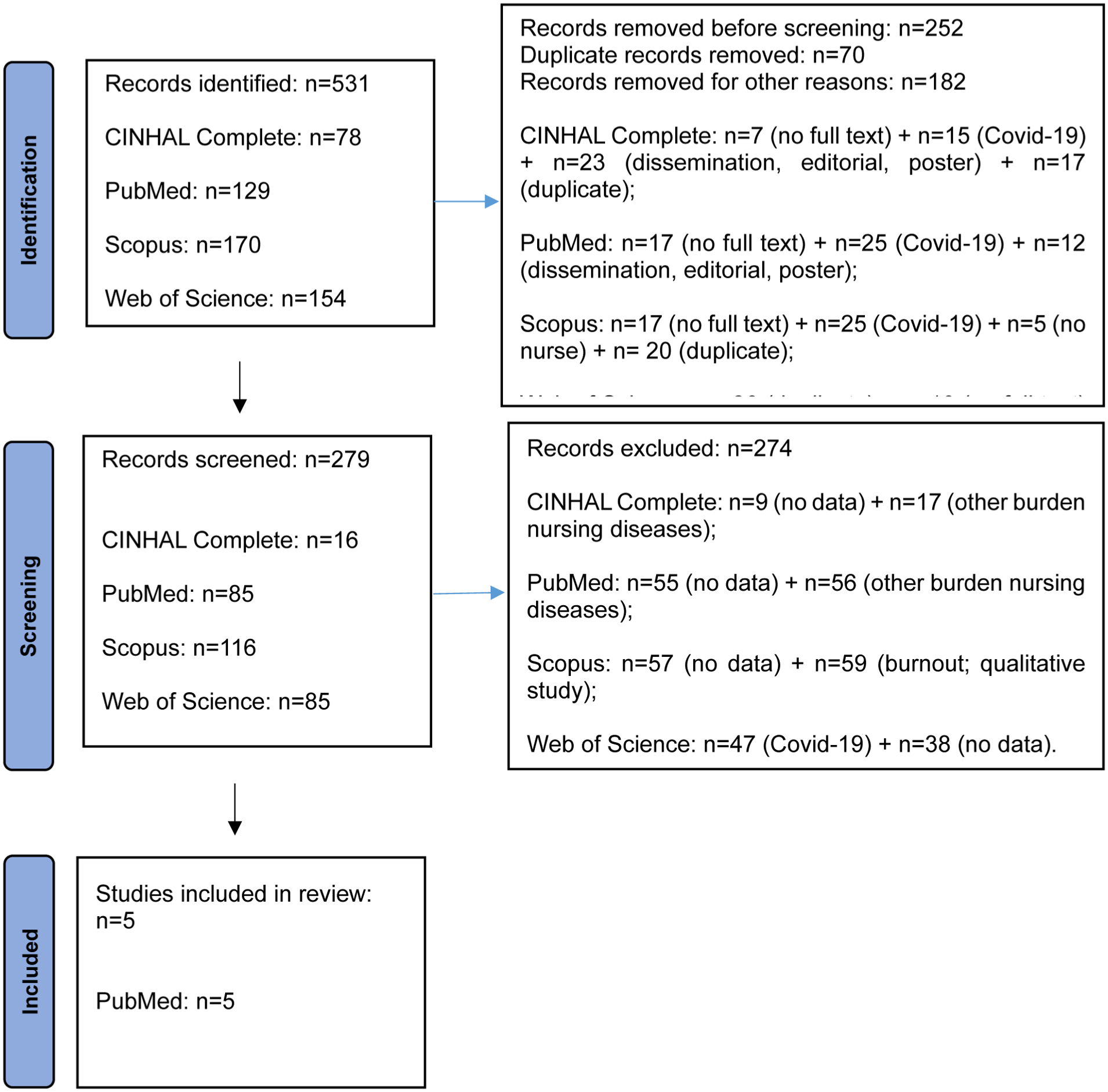
PRISMA flow chart.
Risk-of-Bias Assessment
The presence of risk of bias was assessed adopting the risk of bias in observational studies of exposures (ROBINS-E) tool (Higgins et al., 2024). The tool included a total of seven subdomains through which the presence of bias in the results could be explored: specifically, bias due to confounding, bias arising from measurement of the exposure, bias in selection of participants into the study (or into the analysis), bias due to postexposure interventions, bias due to missing data, bias arising from measurement of the outcome, and bias in selection of the reported result (see Figure 2 for risk-of-bias assessment).
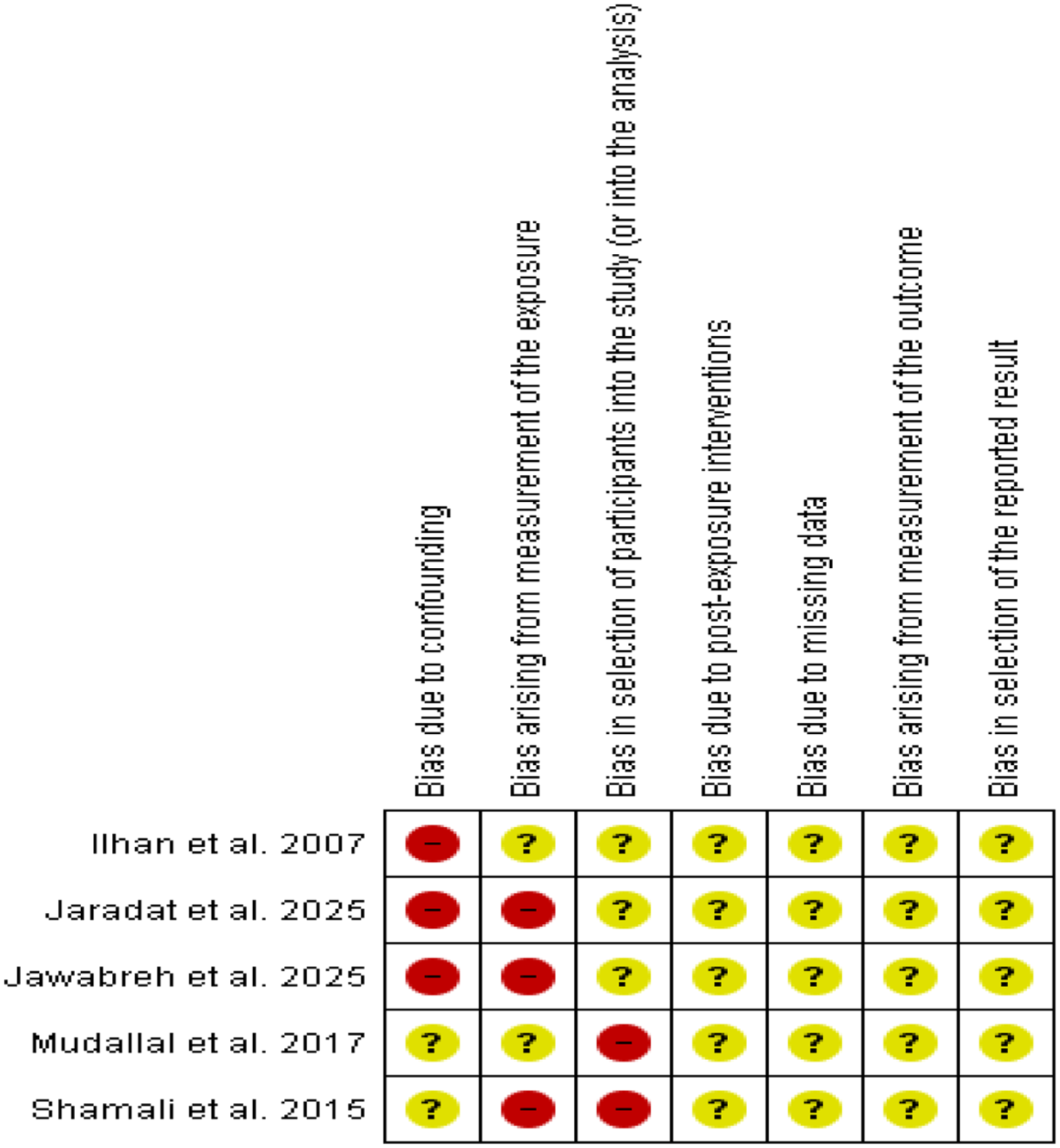
Risk-of-bias assessment.
Strategy for Data Synthesis
The included studies were initially coded and entered into Microsoft Excel using a double-entry method to minimize data entry errors, after which the data were transferred to RevMan software (version 5.4.1) for analysis. Standardized mean differences were calculated to determine the individual study mean differences and corresponding weights after adjusting for the standard deviation. Heterogeneity among studies was assessed using the chi-square (χ2) test with 95% confidence interval (CI) and significance level of p < .05. The degree of heterogeneity was quantified using the I2 statistic and classified as high (>75%), moderate (50%-75%), or low (<50%). Given the presence of heterogeneity, a random-effects model was used to generate pooled estimates.
Results
Study Characteristics
A total of 5 descriptive and observational studies were included in the present systematic review and meta-analysis.
Meta-analysis
As shown in Figure 3, burnout total scores were not significantly different between shift and fixed-schedule work across two studies (Jaradat et al., 2025; Jawbarah et al., 2025), including a total of 260 participants. The overall standardized mean difference was 0.14 (95% CI [−0.57, 0.86]), indicating no statistically significant difference between the two groups, as the confidence interval included zero. Notably, heterogeneity was considerable (I2 = 91%, τ2 = 0.24; p = .001), suggesting substantial variability in effect estimates between the included studies (see Figure 3 for differences in burnout total scores between shift and fixed-schedule work).
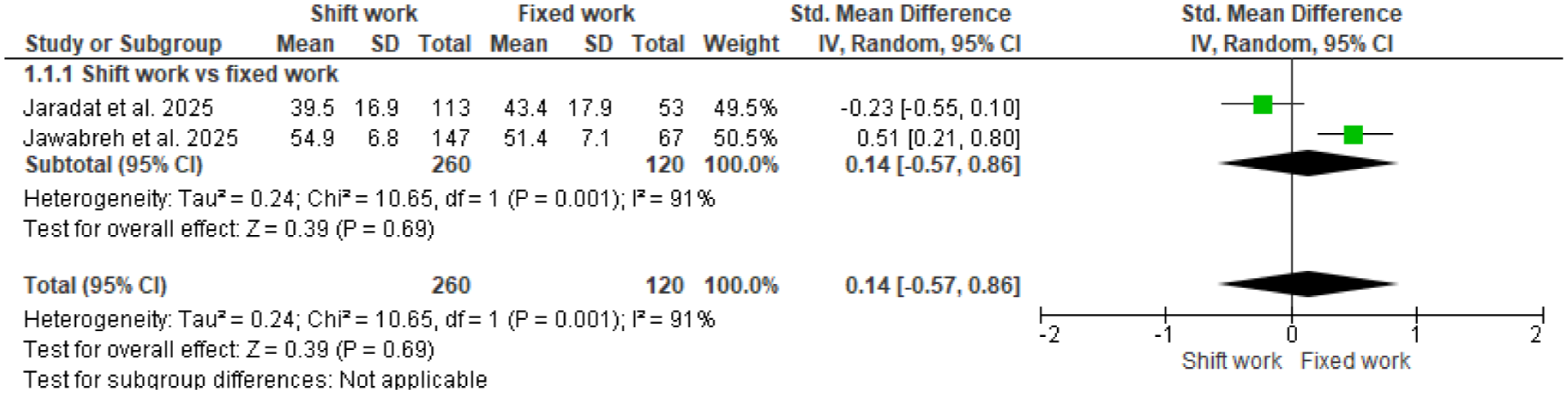
Differences in burnout total scores between shift and fixed-schedule work.
Figure 4 displays differences recorded between shift work and fixed-schedule work across five studies (İlhan et al., 2007; Jaradat et al., 2025; Jawbarah et al., 2025; Mudallal et al., 2017; Shamali et al., 2015), including a total of 872 participants in the shift work group and 463 in the fixed-schedule group. Individual study estimates are shown with their corresponding 95% confidence intervals, along with the pooled effect size. The overall standardized mean difference was −0.01 (95% CI [−0.36, 0.33]), suggesting no statistically significant difference between the two groups, as the confidence interval included zero. Substantial heterogeneity was observed among the included studies (I2 = 88%, τ2 = 0.13; p < .00001), suggesting considerable variability in effect estimates across studies (Figure 4 shows differences in EE scores between shift and fixed-schedule work).
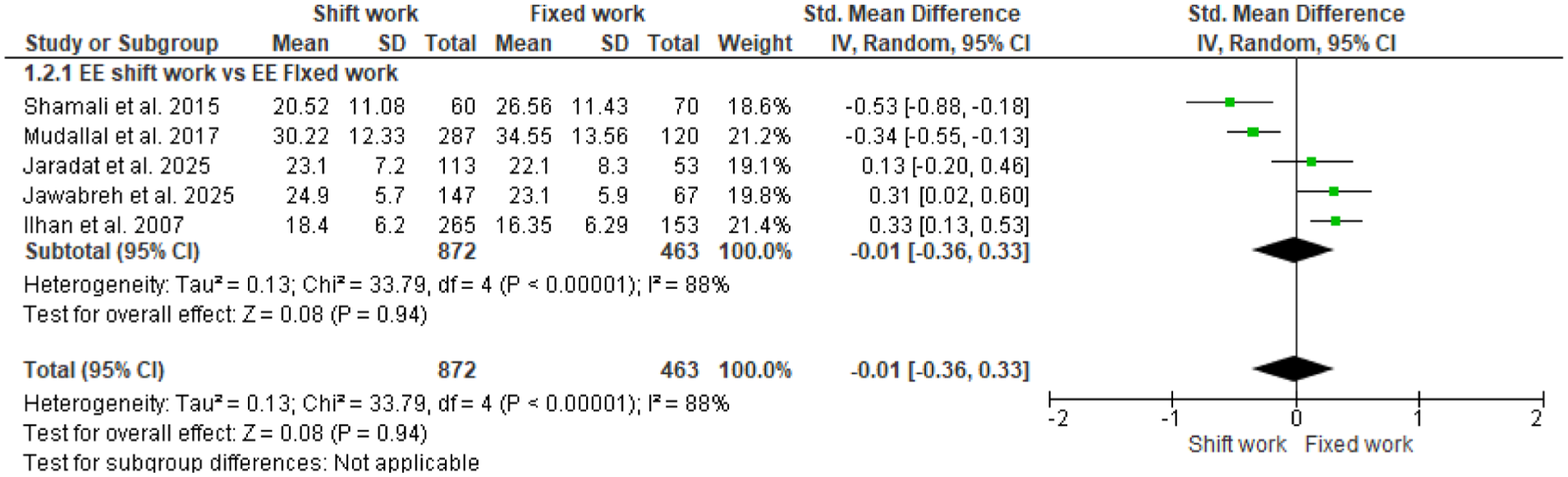
Differences in emotional exhaustion scores between shift and fixed-schedule work.
Figure 5 shows the comparison of outcomes between shift work and fixed-schedule work in the DEP subdimension across five studies (İlhan et al., 2007; Jaradat et al., 2025; Jawbarah et al., 2025; Mudallal et al., 2017; Shamali et al., 2015), including a total of 872 participants in the shift work group and 463 in the fixed-schedule group. Individual study estimates have been displayed with their corresponding 95% confidence intervals, along with the pooled effect size. The overall standardized mean difference was 0.22 (95% CI [−0.10, 0.53]), indicating no statistically significant difference between the two groups. Important heterogeneity was observed among the included studies (I2 = 86%, τ2 = 0.11; p < .00001), suggesting considerable variability in effect estimates across studies.
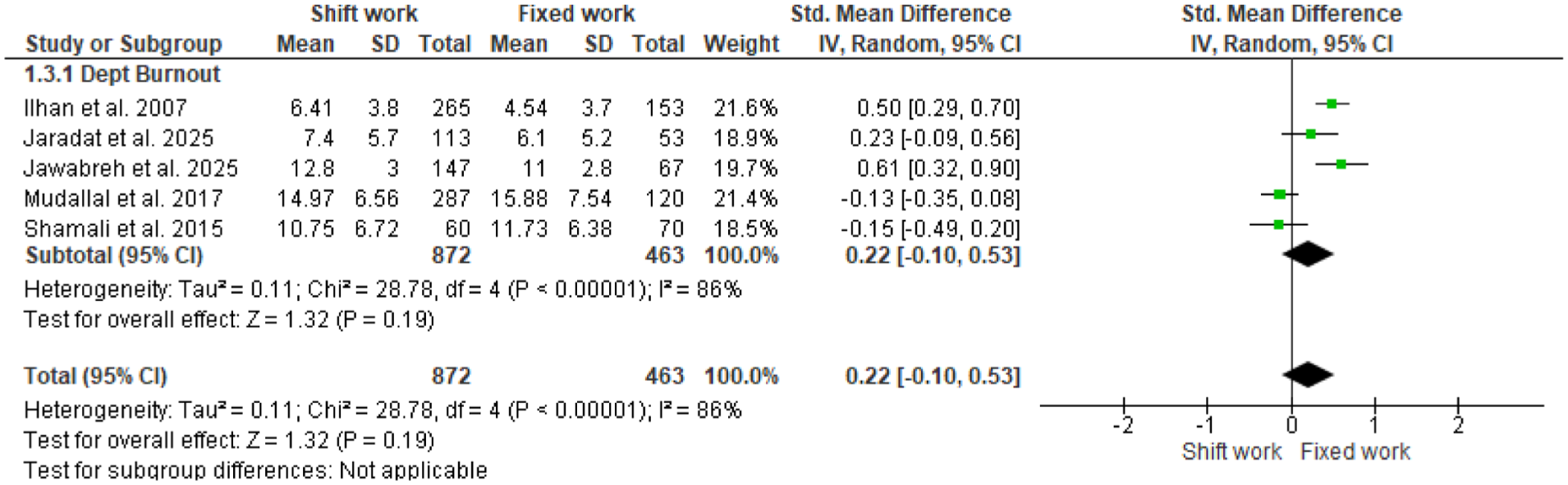
Differences in depersonalization scores between shift and fixed-schedule work.
Figure 6 displays the outcomes of shift work versus fixed-schedule work in the PA subdimension across five studies (İlhan et al., 2007; Jaradat et al., 2025; Jawbarah et al., 2025; Mudallal et al., 2017; Shamali et al., 2015), including a total of 872 participants in the shift work group and 463 in the fixed-schedule group. Individual study estimates have been displayed with their corresponding 95% confidence intervals, along with the pooled effect size. The overall standardized mean difference was −0.07 (95% CI [−0.27, 0.12]), indicating no statistically significant difference between the two groups. Important heterogeneity was observed among the included studies (I2 = 63%, τ2 = 0.03; p < .03), suggesting considerable variability in effect estimates across studies (see Figure 6 for the differences in PA scores between shift and fixed-schedule work).
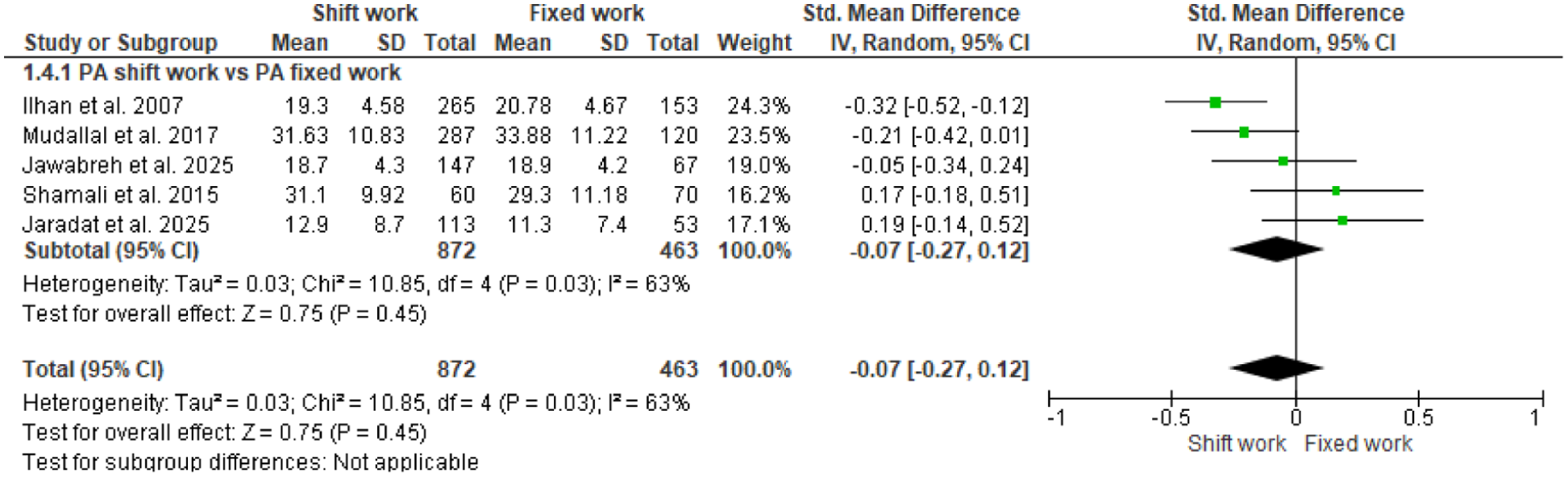
Differences in professional achievement scores between shift and fixed-schedule work.
Discussion
The present systematic review and meta-analysis aimed to assess any differences in work burnout and its related subdimensions between nurses working rotating shifts and those working fixed shifts worldwide. However, these findings revealed no statistically significant differences between the two groups across all analyses, despite the presence of high and statistically significant heterogeneity (.0001 ≤ p ≤ .03). However, both rotating and variable shifts interfere with circadian rhythms and affect physiological stress, muscle pressure, and pain (Redeker et al., 2019; Tojo et al., 2018).
Thus, these findings are in disagreement with the current literature, since burnout has often been recognized as one of the adverse outcomes associated with shift work (Demir et al., 2003). In Iran, research has found a higher rate of burnout among nurses working in rotating shifts compared with those working fixed shifts (Skinner et al., 2012). Conversely, Dwyer and colleagues (2007) suggested that rotating shifts positively affect psychological well-being and job satisfaction among critical care nurses. Shamali and colleagues (2015) reported that critical care nurses employed in fixed shifts experienced significantly higher EE levels than nurses employing in rotating shifts. However, no significant differences have been identified between rotating and shift groups in both DEP and PA. Additionally, nurses with greater overtime workloads report significantly increased levels in EE, DEP, and PA (Natvik et al., 2011).
Abdi Masooleh and colleagues (2007) reported higher burnout prevalence among nurses employed in rotating shifts. Khazaei and Sharifzadeh (2006) indicated the same trend as in our meta-analysis, since no significant differences between fixed and rotating shifts were recorded in either EE or PA, but in the DEP subdimension statistically significant associations were reported in nurses working rotating shifts recording higher DEP levels. Although literature remains inconsistent, several results suggest that nurses working fixed shifts may experience higher burnout levels, whereas rotating shifts may moderate burnout when nurses voluntarily choose to work rotating shift (Choobineh et al., 2007). Rotating-shift nurses may display higher flexibility, as many rotating-shift nurses can interchange shifts with colleagues to better organize work-family life (Tavangar et al., 2013). However, nurses working fixed morning shifts often face increased workloads due to the intensity of patient care and providers writing more orders during day shifts.
Shahriari and colleagues (2014) reported a significant association between shift type and burnout among critical care nurses. Specifically, higher EE and DEP levels were significantly associated with fixed shifts. Although PA levels seemed to be higher among fixed-shift nurses than rotating-shift nurses, the difference was not statistically significant.
Conclusion
A systemic review and meta-analysis was performed to compare rotating and fixed-schedule nurses, and our findings revealed no significant differences between the two groups. We hope that more research will be performed to better assess which factors are associated with shift scheduling and contribute to high levels in burnout subdimensions and that, as a result of the findings, healthcare policies are put in place to ameliorate the health of nurses.