
Abstract
Pakistan is one of the few remaining countries where wild poliovirus remains endemic, despite decades of eradication campaigns. Yet, vaccine hesitancy persists, not merely due to biomedical skepticism but through digital discourse. Drawing on 6,399 Urdu language tweets, this study uses natural language processing and lexicon based modeling to test four hypotheses on the emotional and symbolic drivers of hesitancy. Emotions are operationalized using the NRC Emotion Lexicon, treating trust and fear as measurable affective signals. The findings challenge Western behavioral models such as the Extended Parallel Process Model (EPPM): trust is negatively associated with hesitancy, whereas fear is positively associated with it even when trust is present. Notably, fear’s effect weakens in security framed tweets, which express moral resolve and collective strength rather than panic. Religious framing also predicts hesitancy, but it is often based on misquoted or misinterpreted religious references. In many cases, such discourse misaligns with the actual teachings of the religion, which historically endorse disease prevention and public health. Vaccine hesitancy in this context emerges not as an individual risk judgment, but as a culturally embedded form of communicative resistance, requiring discourse based, context sensitive approaches to global health communication.
Keywords
Introduction
In early 2025, Pakistan remained one of only two countries globally, along with Afghanistan, where wild polio virus transmission is still endemic, despite concerted immunization campaigns and surveillance efforts (Jorgensen et al., 2025). The virus continues to persist particularly in regions affected by low institutional trust, insecurity, and cultural resistance. However, the polio challenge today is not only biomedical but also discursive. In online discussions, vaccine resistance is increasingly expressed through anger, suspicion, and ideological dissent (Ittefaq et al., 2021). This study rethinks dominant public health frameworks by analyzing Urdu language digital discourse through a lens that foregrounds cultural narrative, religious symbolism, and localized emotion which are the dimensions often overlooked in Western behavioral models (Dubé et al., 2013; Krishna & Thompson, 2021; Witte, 1992). Urdu, as Pakistan’s national language and a key medium of informal digital discourse, offers access to culturally embedded expressions of fear, trust, and resistance that are often absent in English language analysis. پولیو کے قطرے یا زہر کے قطرے ہیں۔۔جو بندوق کی نوک پر پلائے جاتے ہیں۔۔ یہ درحقیقت امت مسلمہ کو بانجھ کرنے کی دجالی سازش ہے۔ (“Are these polio drops or poison? They’re being forced upon us at gunpoint… it’s truly a Dajjalic plot to sterilize the Muslim ummah.” - April 22, 2019) کیا کوئی بتا سکتا ہے کہ پولیو کے قطرے نہ پلانے سے پاکستان میں کوئی بچہ مرا ہو؟ یقینا نہیں۔ لیکن پوری قوم جانتی ہے کہ ہر سال پولیو کے قطرے پلانے سے بعض علاقوں میں بچے مر رہے ہیں اور محکمہ صحت ذمہ داری بھی قبول نہیں کرتا۔ (“Can anyone prove that a child in Pakistan has died because they weren’t given polio drops? Of course not. But the whole nation knows that every year, in some areas, children die after being vaccinated and the health department never takes responsibility.” - April 22, 2019) ژوب، مسلح افراد کی فائرنگ، پولیو ڈیوٹی پر مامور 3 پولیس اہلکار شہید (“Zhob: Armed assailants opened fire, martyring three police officers assigned to polio duty.” - September 22, 2024)
These posts portray polio vaccination not as a neutral health intervention but as a symbol of coercion, foreign conspiracy, or institutional failure drawing on collective fears, religious motifs, and security anxieties (Hussain et al., 2016; Rahim et al., 2022). Based on an analysis of over 6,000 Urdu language tweets, this study examines how such affective and ideological framings situate vaccine hesitancy within a broader discursive landscape shaped by mistrust, moral contestation, and historical grievance. Despite a growing body of research on polio eradication and vaccine hesitancy in Pakistan, existing studies have relied largely on surveys, interviews, or English language media, with far less attention to how hesitancy is constructed and negotiated in vernacular social media discourse. This study addresses this gap by analyzing large scale Urdu language tweets and offers computationally grounded account of how fear, trust, religion, and security framings are articulated in Pakistan’s digital public sphere.
While much of the global health communication literature frames fear as a catalyst for compliance encouraging precautionary behavior in the face of infectious disease (Betsch et al., 2010; Rogers, 1975; Witte & Allen, 2000), the findings of the study complicate this view. In the Pakistani context, fear is not merely an alert to risk; it frequently co-occurs with expressions of doubt, harm, and conspiracy, thereby reinforcing vaccine hesitancy rather than overcoming it. Similarly, in several Muslim majority settings, religion is theorized to function as an important element in vaccination programs; for example, Muslim scholars’ perceptions of barriers and facilitators toward polio immunization can influence public acceptance in their communities (Dubé et al., 2013; Khan et al., 2017). Yet, the religious framing the study observes in Pakistani digital discourse tends to invert this assumption: rather than promoting compliance, it often casts vaccination as a theological intrusion or political deception. This suggests a crucial divergence: emotions and religious appeals may not function as universal tools for public health persuasion, but are instead shaped by localized histories, grievances, and discursive traditions. This is especially notable given that Islamic jurisprudence and major religious authorities have repeatedly affirmed the permissibility and social responsibility of vaccination to preserve life and prevent harm (Mardian et al., 2021; Owens, 2025). This study therefore empirically tests how fear, trust, security, and religious framing shape polio vaccine hesitancy in Urdu language digital discourse.
In light of the above, this study pursues the following objectives: (1) to examine how fear and trust are expressed in Urdu language social media discourse on polio vaccination in Pakistan; (2) to assess how these emotional cues relate to the presence of vaccine hesitancy framing in digital texts; (3) to analyze the role of religious and security framing in shaping hesitancy narratives; and (4) to evaluate the extent to which the observed patterns align with or diverge from the expectations of dominant health behavior models such as the Extended Parallel Process Model in a low trust, conflict-affected context. On the basis of these objectives and the theoretical expectations, the study formulates the following hypotheses:
Tweets with higher expressions of trust
1
are less likely to exhibit polio hesitancy.
Tweets with higher expressions of fear are more likely to express polio hesitancy, even when trust is present.
Fear is more strongly associated with hesitancy when tweets also reference security threats.
Tweets that invoke religious framing are more likely to express polio hesitancy, even after controlling for fear and trust.
The Extended Parallel Process Model (EPPM) provides the primary theoretical lens for this study. EPPM posits that responses to fear appeals depend on perceived threat and perceived efficacy: when both are high, individuals engage in danger control (protective action), whereas high threat combined with low efficacy produces fear control (defensive avoidance) (Witte, 1992; Witte & Allen, 2000). In this analysis, fear related language captures perceived threat, while trust related expressions approximate perceived efficacy and confidence in institutional solutions, allowing to assess whether EPPM’s core expectations hold in Pakistan’s low trust digital vaccine discourse. This framework is complemented by insights from the Health Belief Model (HBM), which emphasizes perceived susceptibility, severity, benefits, and barriers in shaping health behavior (Becker, 1974; Champion & Skinner, 2008; Rosenstock, 1974). These perspectives guide this examination of how cognitive appraisals and emotions are articulated in vernacular social media discourse.
At the same time, prior research suggests that fear encourages protective action only when accompanied by strong efficacy cues (Rogers, 1975; Witte & Allen, 2000), but the present study anticipates that this relationship may be complicated in contexts marked by distrust and conflict. In Pakistan’s vaccine discourse, fear frequently coexists with frames of betrayal, harm, and uncertainty rather than self-efficacy. Instead of motivating compliance, fear may signal vulnerability or perceived victimization, reinforcing suspicion of both the vaccine and the state. Similarly, although religious appeals are often viewed as tools for building normative support for public health (Dubé et al., 2013; Grabenstein, 2013), Urdu language tweets suggest a different dynamic: religious language is frequently used by the twitter users in ways that do not legitimize vaccination but to challenge its authority, casting polio campaigns as moral violations, colonial impositions, or threats to spiritual sovereignty. This theoretical tension motivates the empirical tests that follow.
This divergence from established theory highlights the importance of context in affective health communication. In low trust, conflict affected settings, fear and religion may not function as persuasive levers but instead serve as carriers of resistance. To counter this, public health engagement must draw upon the true ethical principles of Islam which emphasize the protection of life, prevention of harm, and collective responsibility to realign religious discourse with pro-vaccination norms. By empirically demonstrating these deviations, the study extends the literature on vaccine hesitancy by showing that the emotional and symbolic architecture of hesitancy is deeply local, shaped not only by individual beliefs but by collective memories, cultural scripts, and discursive traditions. This shift from universal behavioral models to context sensitive discourse analysis enables a more in-depth understanding of vaccine refusal as a culturally saturated, emotionally coded communicative act.
Literature Review
Global Vaccine Hesitancy and Communication
Vaccine hesitancy, defined as the delay or refusal of vaccination despite availability, has emerged as a pressing global health challenge and was identified by the World Health Organization as one of the top 10 threats to global health (MacDonald, 2015). It is a complex, context dependent phenomenon influenced by cognitive, emotional, social, and structural factors (Betsch et al., 2011; Dubé et al., 2013). The widely cited “3Cs” framework conceptualizes hesitancy as a function of three dimensions: confidence (trust in vaccines and institutions), complacency (low perceived risk of disease), and convenience (barriers to access) (Larson et al., 2014; MacDonald, 2015). Among these, confidence (or the lack thereof) has consistently been shown to exert a strong influence on vaccination behavior. While global trends in vaccine confidence reveal important national differences (Larson et al., 2015), behavioral studies suggest that individual level trust remains a robust predictor of uptake (Quinn et al., 2019).
In parallel, emotional dynamics have gained increasing attention in vaccine research; misinformation environments can intensify fear and uncertainty around vaccination, while narrative accounts of vaccine experiences have been shown to shape perceived risk more strongly than statistical evidence (Betsch et al., 2011; Krishna & Thompson, 2021). Contemporary health communication research emphasizes that vaccine attitudes are not exclusively rational but also deeply affective mediated by cultural narratives, historical memory, and moral worldviews (Betsch et al., 2011; Filsinger & Freitag, 2024). In high income countries, for example, fear based misinformation about adverse effects has fueled vaccine skepticism, whereas confidence in medical institutions has played a stabilizing role (Jolley & Douglas, 2014; Larson et al., 2015). However, the majority of this literature focuses on Global North settings. Far fewer studies examine how these dynamics play out in polio endemic, low trust contexts, particularly in South Asia and sub-Saharan Africa, where public sentiment may be shaped by security concerns, religious beliefs, and legacies of coercion. This review synthesizes prior research on four key drivers of vaccine discourse (trust, fear, security, and religious framing) laying the foundation for the hypotheses tested in this study.
Trust as a Cornerstone of Vaccine Acceptance
Public trust is widely recognized as an essential precondition for successful vaccination campaigns. Trust in vaccine safety, healthcare providers, and governing institutions correlates strongly with vaccine acceptance across diverse settings (Larson et al., 2014; Quinn et al., 2017). A systematic review by Larson et al. (2014) concluded that higher trust in health authorities and the medical system generally predicts lower vaccine hesitancy. Likewise, large-scale surveys during the COVID 19 pandemic found that individuals who trusted government and scientists were far more willing to accept vaccines, whereas mistrust was a salient predictor of refusal (Jennings et al., 2023; Lazarus et al., 2021). For instance, a 23-country study identified mistrust in government as a key driver of COVID 19 vaccine hesitancy worldwide (Lazarus et al., 2023). These findings echo earlier work on childhood immunization: parents with confidence in pediatricians and public health agencies are more likely to vaccinate their children on schedule (Dubé et al., 2013; Opel et al., 2011). In contrast, erosion of trust can sharply undermine vaccination efforts. Historical cases show that when communities suspect authorities of hiding information or acting against their interest, even well established vaccine programs can falter (Jegede, 2007; Kata, 2010). In the global North, episodes like the UK’s MMR autism controversy illustrate how loss of confidence (spurred by misinformation) led to drops in vaccine uptake and subsequent disease outbreaks (Larson et al., 2015). In the global South, trust deficits are often linked to colonial history or political marginalization, which can make public health campaigns appear suspect (Basharat & Shaikh, 2017; Obadare, 2005). Overall, the literature consistently indicates that bolstering trust through transparency, community engagement, and credible messengers is critical to counteract hesitancy. This strong empirical consensus informs first hypothesis (H1), expecting that expressions of trust in institutions or health workers will correspond with lower levels of polio vaccine skepticism.
Fear, Risk Perception, and Misinformation
If trust is the positive linchpin of vaccine acceptance, fear serves as its negative mirror. In health communication, fear operates as a double edged sword: while fear of disease can motivate protective behavior, fear of vaccines often deters it (Tannenbaum et al., 2015; Witte, 1992). Decades of research on fear appeals suggest that such messages may backfire unless individuals also feel empowered to act and have confidence in the recommended solution (Ruiter et al., 2014; Witte, 1992). In the context of vaccination, this implies that fear based messaging increases uptake only when people believe the vaccine is both safe and effective; otherwise, heightened fear can trigger avoidance, anxiety, or denial.
Research has shown that anxiety over rare or unverified side effects is a persistent concern among hesitant individuals. Experimental studies also reveal that fear based messaging, especially vivid descriptions of vaccine risks, can backfire and heighten hesitancy, particularly among already skeptical audiences (Dubé et al., 2013; Jolley et al., 2025). These anxieties are often amplified by misinformation and emotionally charged anecdotes. For instance, Jolley and Douglas (2014) found that exposure to anti vaccine conspiracy theories, such as claims of hidden harms or nefarious agendas, significantly heightened perceived risks and reduced vaccination intent.
Qualitative studies echo this pattern: parents who delay or refuse vaccines frequently cite fear laden personal stories of perceived injury, indicating that emotional narratives may be more persuasive than scientific reassurances (Hornsey et al., 2018; Kata, 2010). In high income settings, fear has manifested in clustered outbreaks of hesitancy ranging from debunked links between MMR and autism to unfounded panic over COVID 19 vaccine ingredients, especially in contexts of low institutional trust and high uncertainty (Hornsey et al., 2018; Larson et al., 2015).
The interplay between fear and trust is thus critical. When confidence in authorities is low, fear appeals about disease severity may be disregarded, while fear of the vaccine can take hold more easily. Empirically, this translates to a higher likelihood of vaccine hesitancy among those expressing fear. The study extends this insight in H2, positing that tweets with strong fear cues, such as references to danger, side effects, or death, are more likely to reflect polio vaccine hesitancy, even when some degree of trust is present. This hypothesis aligns with prior findings that uncertainty and negative emotion can override rational risk benefit calculations in vaccine decision making; misinformation can fuel these emotional responses by amplifying fear and doubt in the public sphere (Krishna & Thompson, 2021; Ruiter et al., 2014).
Security Threats and the Politics of Immunization
Vaccination campaigns do not occur in a political vacuum. In polio endemic regions, they unfold amid ongoing security concerns, ranging from conflict and militancy to historical trauma, that deeply shape public perception. Research shows that areas of political instability often overlap with polio outbreaks not only because violence disrupts services but also because it generates fear and widespread distrust toward vaccination programs (Arsenault et al., 2017; Closser, 2010).
In Pakistan and Afghanistan, the Taliban and other militant groups have repeatedly attacked polio teams, killing or threatening health workers and their security escorts (Hussain et al., 2016; Syed & Qazi, 2025). These assaults do more than suspend campaigns, they politicize vaccination itself. Polio drops become associated with danger, coercion, or espionage rather than healthcare (Martinez-Bravo & Stegmann, 2022; Obadare, 2005).
A notorious example is the 2011 revelation that a CIA operation used a fake vaccination drive to track Osama bin Laden. This severely eroded trust and fueled propaganda portraying polio campaigns as Western intelligence tools (Lenzer, 2011; Martinez-Bravo & Stegmann, 2022). Subsequent declines in immunization highlight how security entanglements produce lasting skepticism.
Insecurity also shifts public priorities: people may fear both the vaccine’s effects and the violence around its delivery. During Nigeria’s polio efforts in the early 2000s, similar distrust flourished. Local leaders linked vaccination to geopolitical hostility against Muslims during the “War on Terror” (Jegede, 2007; Obadare, 2005).
However, this dynamic is complex. Framing immunization as a national security issue can also generate compliance but in other contexts, it intensifies resistance by validating suspicions of foreign or state-led coercion (Akhavein et al., 2025; Kaunert et al., 2022; Rollet, 2014). The third hypothesis (H3) reflects this nuance: the study expects that fear will more strongly predict hesitancy when paired with references to security threats. Rather than additive, the effect is interactive fear acquires new potency within a securitized narrative frame.
Religious Framing and Vaccine Resistance
Religious discourse has long shaped attitudes toward vaccination. In many cases, faith leaders endorse immunization such as rulings by the Vatican or Islamic scholars emphasizing health as a moral duty (Grabenstein, 2013; Tiwana & Smith, 2024). However, in some contexts, skepticism toward vaccination is expressed through religious reasoning that includes selectively quoted or inaccurately interpreted religious references, as well as links made between vaccination, cultural identity, and moral boundaries.
In the global North, some insular communities, like ultra-Orthodox Jews, Dutch Protestant enclaves, or faith-healing groups, have seen outbreaks linked to doctrines about divine will, bodily purity, or opposition to external intervention (Grabenstein, 2013; Ruijs et al., 2012). In these contexts, refusal is often seen as moral or communal fidelity.
In the global South, religious framing has had even greater public health consequences. In Northern Nigeria (2003), self-claimed clerics and politicians claimed the polio vaccine was a Western sterilization plot, leading to a boycott that stalled global eradication efforts (Jegede, 2007). Similar dynamics emerged in Pakistan and Afghanistan, where some clerics branded polio drops as haram or as assaults on religious sovereignty (Basharat & Shaikh, 2017; Rahim et al., 2022).
Religious framing is powerful because it taps into deep seated worldviews transforming vaccines from medical tools into symbols of moral corruption or eschatological threat. Hornsey et al. (2018) observe that vaccine conspiracies frequently fuse with religio-cultural narratives, offering emotionally resonant alternatives to biomedical explanations. During the COVID 19 pandemic, some misinformation and hesitancy narratives drew on broader cultural and belief-based themes, with uncertainty, mistrust, and misinformation contributing to public skepticism toward vaccines (Hou et al., 2021; Pertwee et al., 2022).
Building on this, the study hypothesizes (H4) that religious framing will independently predict polio vaccine hesitancy even after accounting for fear and trust. Urdu tweets that use religious language within skeptical or conspiratorial narratives are more likely to express vaccine skepticism. This aligns with evidence that moralized health behavior often resists factual reassurance unless reframed in culturally resonant ways (Hou et al., 2021; Pertwee et al., 2022).
Methodology
The study collected all publicly available tweets in Urdu containing the hashtag #polio, using the search query #polio lang:ur. This was accomplished through a customized Python script that accessed X’s frontend search interface and parsed the returned HTML content using BeautifulSoup (Richardson, 2007). The script was configured to paginate through results month by month, beginning from X’s launch and iteratively looping forward to retrieve the complete archive of tweets up to July 21, 2025. To ensure stable access and data continuity, the script handled session management via cookies and respected rate limits throughout the scraping process (Morstatter et al., 2013). Each tweet’s HTML was parsed to extract the visible text, metadata (e.g., timestamp, user handle, and text of the tweet). All extracted data was cleaned, structured, and exported to CSV format for downstream analysis. All data were collected exclusively from publicly accessible posts on X using the author’s own standard user account. The scraping procedure relied on ordinary web access to X’s search interface and did not require developer credentials, private APIs, or any form of elevated or unauthorized access. No protected content was accessed, and no technical safeguards, paywalls, or platform restrictions were circumvented. The procedure programmatically retrieved only content that is visible to any logged in user through a regular browser session. This approach is comparable to established browser based collection tools used in prior social media research, such as the Mozilla extension Zeeschuimer (Rieder et al., 2024), which captures publicly displayed posts during manual scrolling for research archiving and analysis. In line with prevailing ethical standards in computational social science, the study treats these posts as public textual data, and analyzes them only in aggregate.
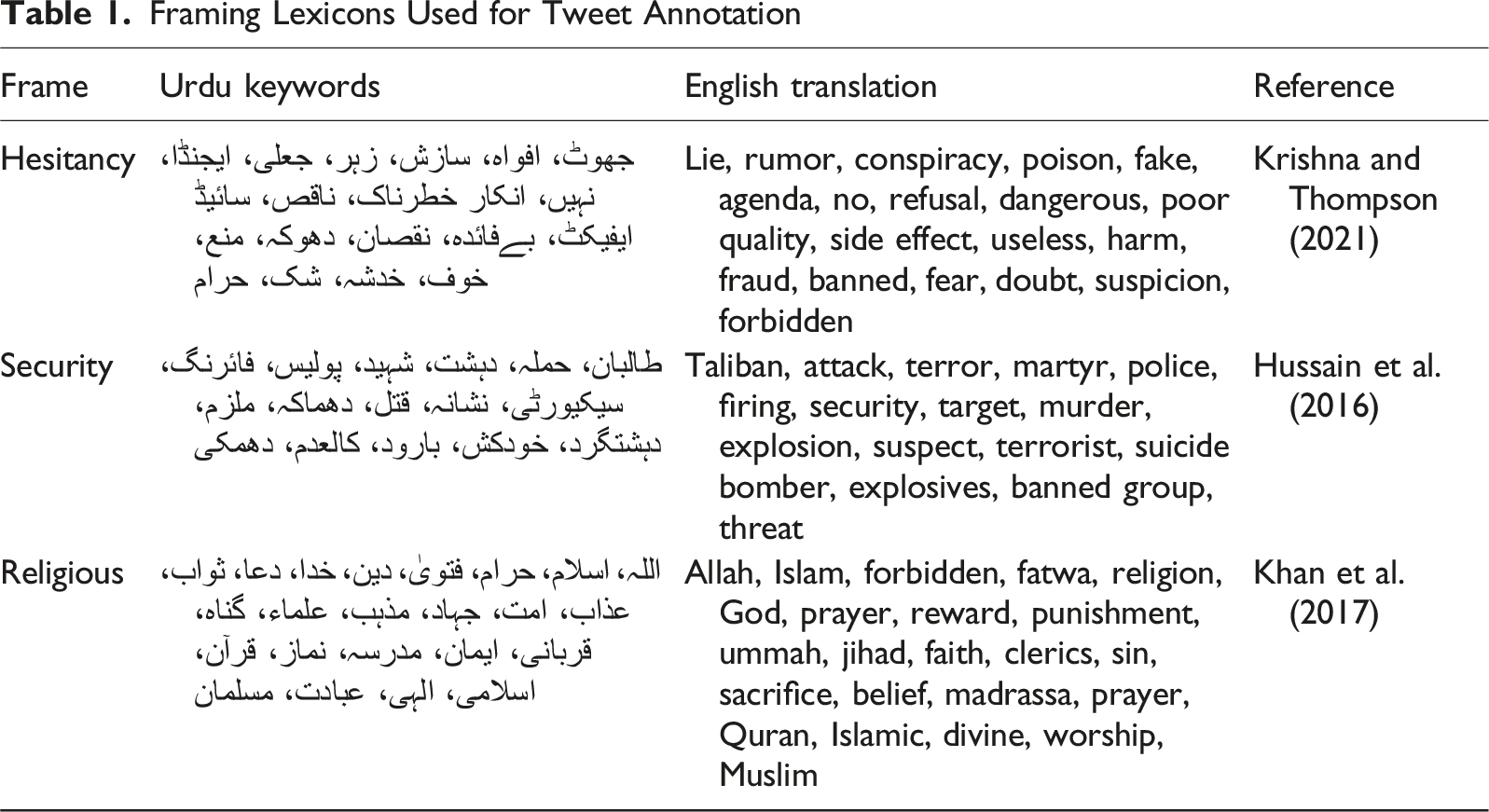
Following data collection, the tweet corpus was imported into R for preprocessing and emotion analysis. To identify emotional expressions in the Urdu language tweets, the study applied the NRC Emotion Lexicon (Urdu version), which assigns lexical associations across 10 canonical categories: anger, anticipation, disgust, fear, joy, sadness, surprise, trust, negative, and positive (Mohammad & Turney, 2013a). Each tweet was tokenized into individual words, and tokens were then matched against the lexicon using an inner join to detect emotion bearing words related to trust and fear. Emotion2 scores were aggregated at the tweet level. The emotion labeled data was then merged back with the original dataset for further analysis (Mohammad & Turney, 2013b).
Framing Lexicons Used for Tweet Annotation
The study estimated a series of logistic regression models to assess how emotional cues and thematic frames shaped expressions of polio hesitancy in Urdu language X (formerly Twitter) discourse. The binary outcome Y
i
was coded 1 if tweet i included any hesitancy-related lexical marker, and 0 otherwise. All models used a binomial logit link:
This modeling approach follows established practices in social media–based behavioral health analysis, particularly in contexts where attitudes are inferred from text level signals (Karafillakis et al., 2021; On et al., 2019; Scannell et al., 2021).
Predictors included frame intensities derived from dictionary-based coding schemes, capturing both emotional (trust, fear) and thematic (security, religion) content. Emotionally framed terms were based on established lexicons validated for social media discourse (Mohammad & Turney, 2013a), while topical dictionaries were tailored for the Pakistani context.
The first model included only the trust score:
The second model added fear as an additional emotional predictor:
This specification aligns with existing research on the dual roles of trust and fear in health decision making under risk (Quinn et al., 2019; Tannenbaum et al., 2015).
The third model introduced an interaction between fear and security:
This interaction tests the hypothesis that fear becomes more predictive of hesitancy in security framed tweets, consistent with theoretical arguments that fear is amplified under perceived threat (Witte, 1992).
The final model added religious framing while controlling for emotional tone:
Religious discourse has been shown to influence vaccine decisions, especially when vaccines are framed in moral, cultural, or conspiratorial terms (Dubé et al., 2013).
All models were estimated in R using the glm() function with the binomial family. Frame scores were computed at the tweet level. All continuous predictors were mean centered prior to estimating interaction terms. Descriptive statistics were reviewed prior to estimation.
Results and Analysis
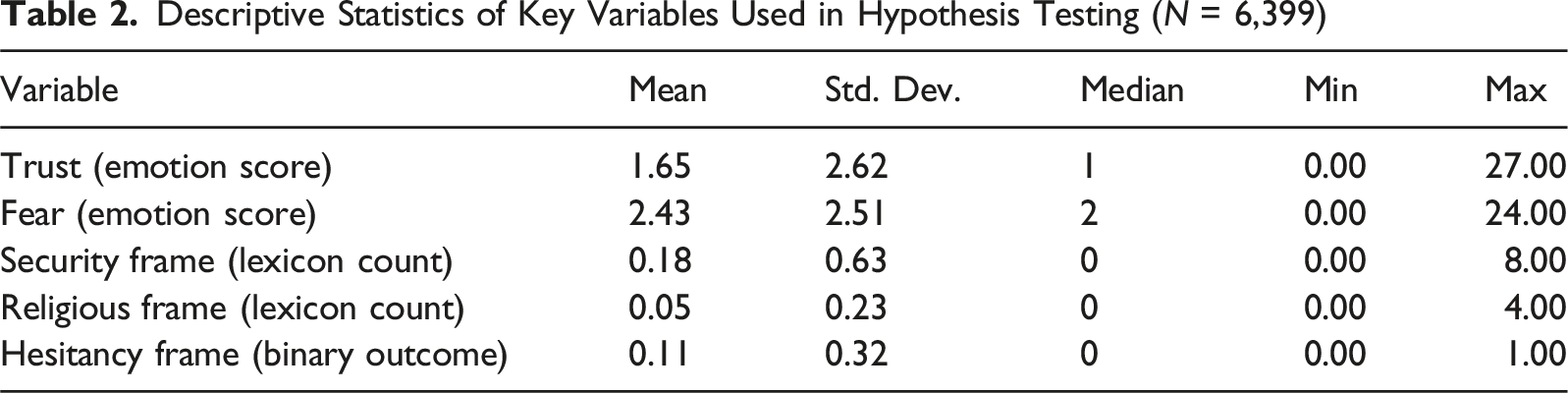
Descriptive Statistics of Key Variables Used in Hypothesis Testing (N = 6,399)
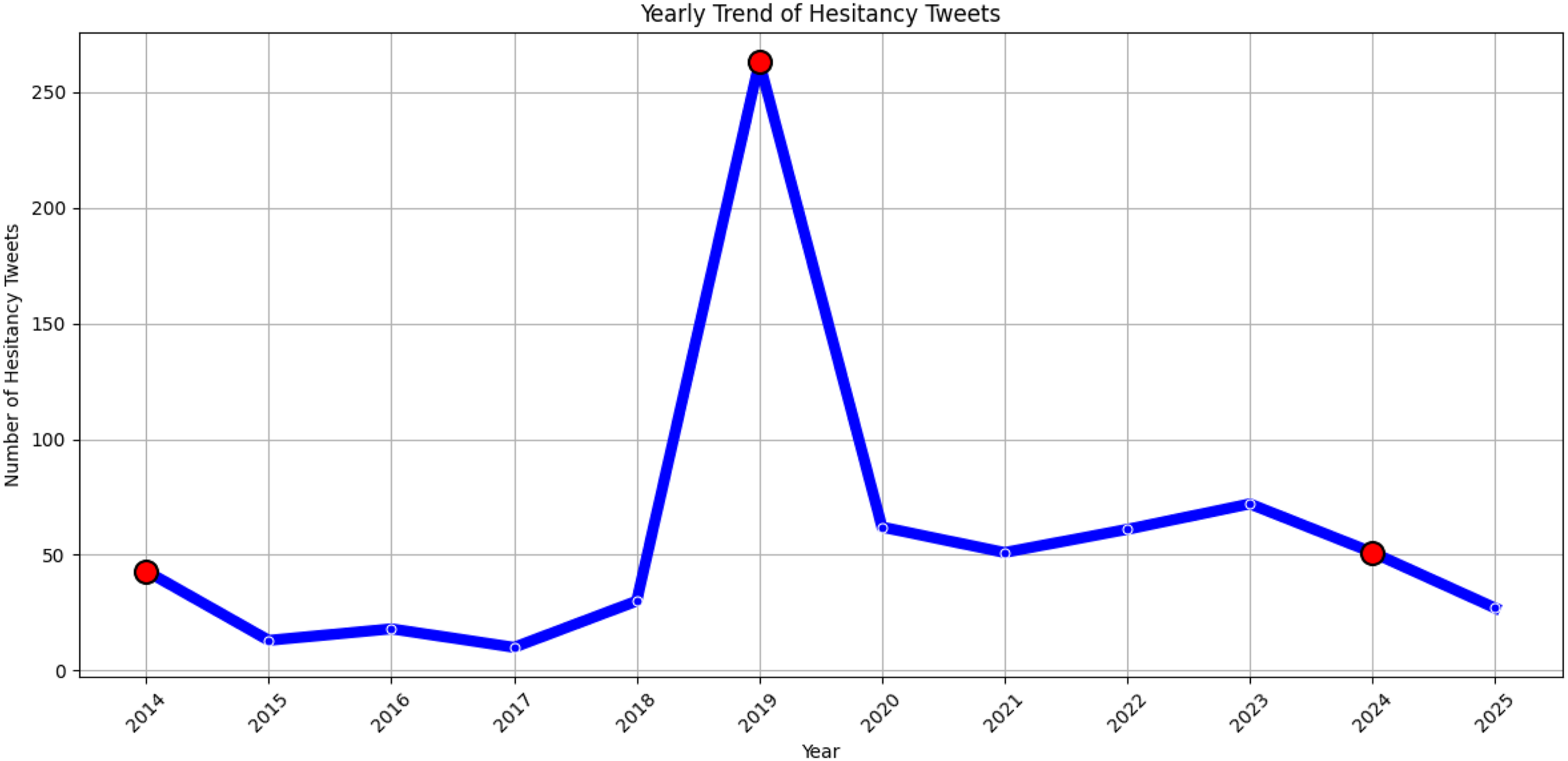
In addition to summary statistics, Figures 1 and 2 visualize the yearly distribution of tweets and hesitancy expressions to contextualize the regression analysis in temporal terms. The figure shows that the overall volume of Urdu language polio tweets increases markedly after 2014, with a pronounced peak around 2019, coinciding with intensified eradication campaigns and heightened public debate. Hesitancy-related tweets follow a similar pattern, with a sharp rise in 2019 and sustained presence in subsequent years. This temporal clustering suggests that expressions of vaccine resistance are not evenly distributed over time but tend to emerge in response to specific campaign phases and socio-political moments, highlighting the importance of situating digital vaccine discourse within its historical and contextual dynamics. Polio tweets over time Polio hesitancy tweets over time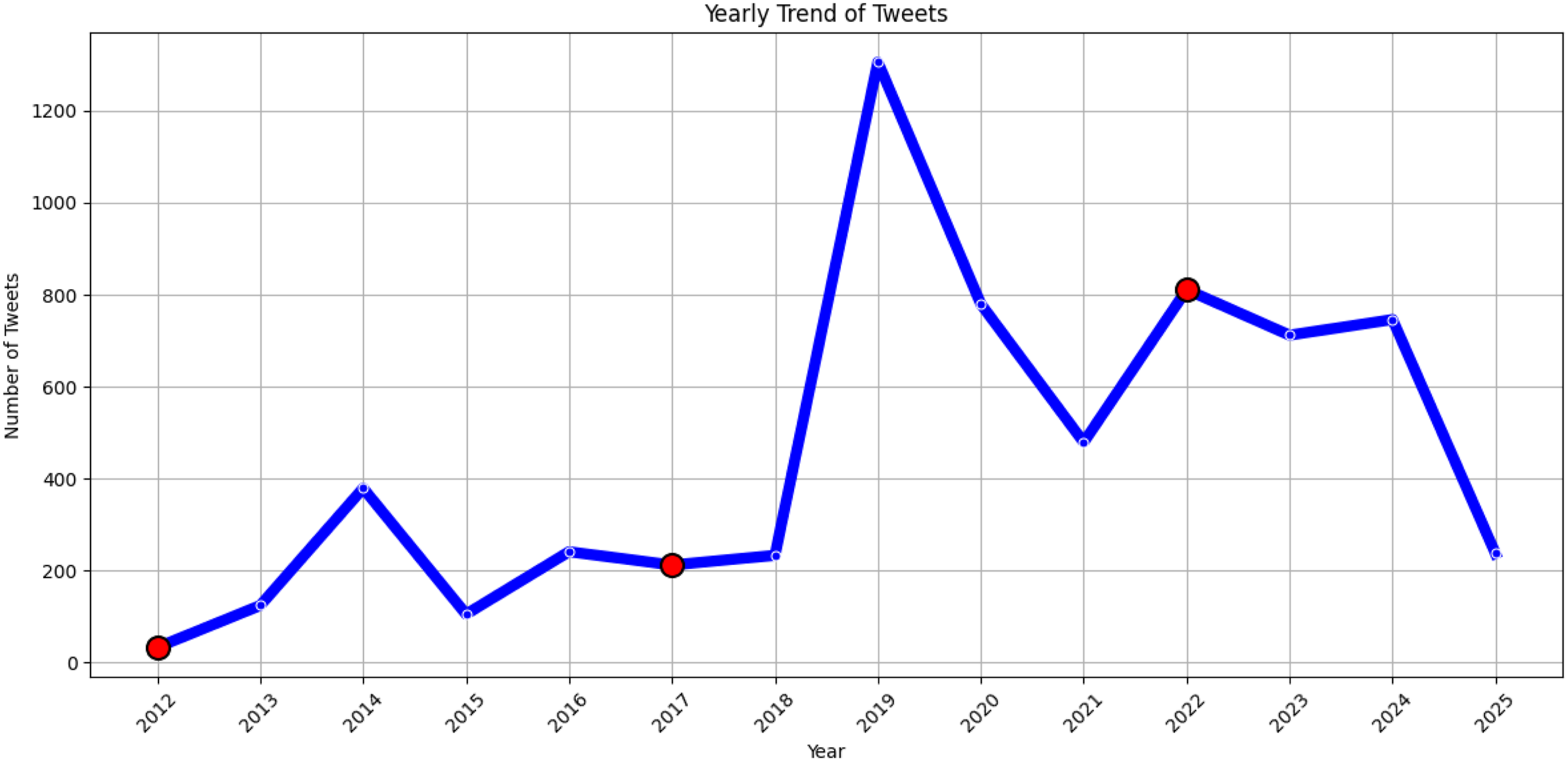
To empirically test the four hypotheses, the study estimated a sequence of binomial logistic regression models using a dataset of 6,399 Urdu language tweets about polio, with the binary dependent variable defined as the presence of vaccine hesitancy framing. Each model incrementally examined the predictive value of emotion related and topical frame intensities derived from a validated Urdu keyword dictionary. Results are interpreted with reference to odds ratios and statistical significance thresholds.
H1: Tweets with Higher Expressions of Trust Are Less Likely to Exhibit Polio Hesitancy
Logistic Regression Model Testing H1 (Trust as Predictor)

Note: Logit coefficients reported. *p < .05, **p < .01, ***p < .001.
Qualitative inspection of high trust tweets further supports the statistical finding. For instance, some users tweeted positively about campaign leadership and institutional reliability. One such post, shared on October 4, 2023, at 07:01 AM, stated, نگراں وزیراعلی خیبر پختونخوا محمد اعظم خان کا پولیو مہم کے حوالے سے اہم اجلاس، انسداد پولیو اقدامات پر مکمل اعتماد کا اظہار (“The caretaker Chief Minister of Khyber Pakhtunkhwa, Muhammad Azam Khan, held a key meeting regarding the polio campaign and expressed full confidence in the anti polio measures,”) reinforcing trust in official coordination without invoking skepticism. Similarly, confidence in public health outcomes was expressed in a tweet posted on April 13, 2025, at 07:36 AM, which read: ملک کے 20 اضلاع سے حاصل ماحولیاتی نمونوں میں پولیو وائرس نہیں پایا گیا، انسداد پولیو مہم کے مثبت اثرات سامنے آ رہے ہیں (“Polio virus was not detected in environmental samples from 20 districts across the country; the positive effects of the anti-polio campaign are becoming evident”).
A third tweet, shared on November 12, 2023, at 06:17 AM, offers another example of community level trust in government institutions and military support: اتمانزئی جرگہ نے سیکیورٹی فورسز اور حکومتی اداروں کا مقامی لوگوں میں اس حوالے سے شعور اجاگر کرنے اور پولیو آگاہی مہم میں مثبت کردار ادا کرنے پر بھی شکریہ ادا کیا۔ پولیو سے پاک وزیرستان ہی خوشحال پاکستان کی ضمانت ہے (“The Utmanzai jirga also thanked the security forces and government agencies for raising awareness among locals and playing a positive role in the polio awareness campaign. A polio-free Waziristan is a guarantee of a prosperous Pakistan”).
These examples illustrate how trust-oriented language aligns with the absence of hesitancy framing, thereby confirming the hypothesized inverse relationship between trust and vaccine skepticism in Urdu language X discourse.
H2: Tweets with Higher Expressions of Fear Are More Likely to Express Polio Hesitancy, Even When Trust Is Present
Logistic Regression Model Testing H2 (Fear and Trust)

Qualitative examples further reinforce this pattern. A highly fearful post shared on August 21, 2019, at 2:34 PM stated, پولیو وائرس ہماری آنے والی نسلوں کے لیے خطرناک ہے۔ اگر احتیاط نہ کی گئی تو تباہی یقینی ہے (“Polio virus is dangerous for our future generations. If precautions are not taken, disaster is certain,” emphasizing threat and urgency). Another tweet posted on June 20, 2023, at 1:29 PM read, اکثر لوگ یہ سوالات پوچھتے ہیں کہ پولیو کے قطروں کے بعد بچے بیمار کیوں ہو جاتے ہیں؟ اس میں کچھ نہ کچھ مسئلہ ضرور ہے۔ (“People often ask why children fall sick after receiving polio drops. There must be something wrong”), which reflects medical fear and doubt, even while retaining a moderate level of trust.
These examples illustrate that even when some trust is present, fear can override its mitigating effect and contribute significantly to the expression of vaccine hesitancy in Urdu language tweets.
H3: Fear Is More Strongly Associated with Hesitancy When Tweets Also Reference Security Threats
Interaction Model Testing H3 (Fear × Security)
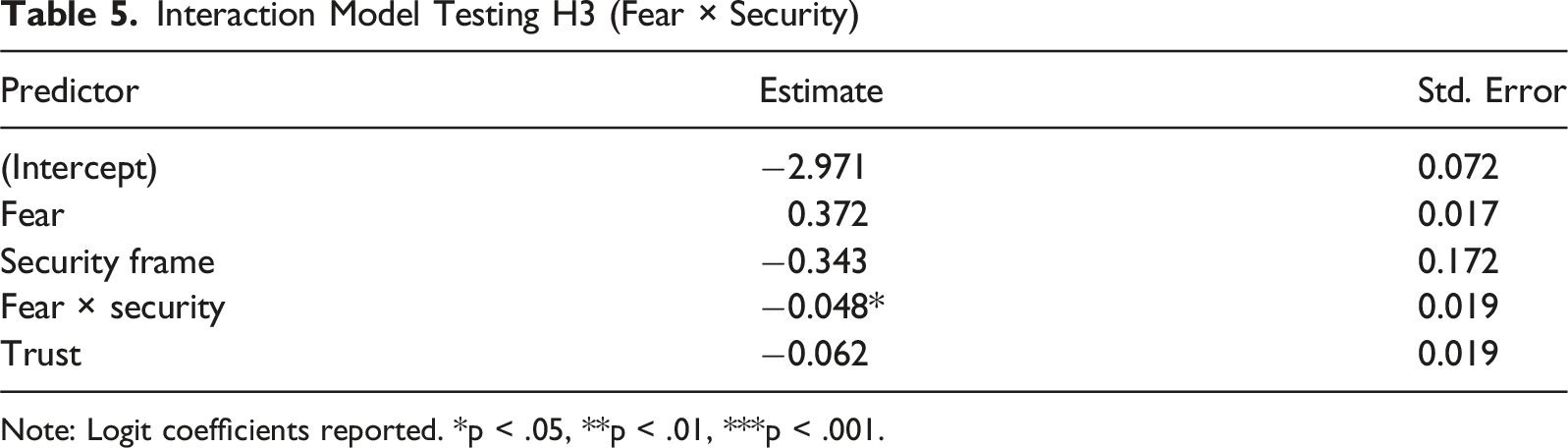
Note: Logit coefficients reported. *p < .05, **p < .01, ***p < .001.
Textual evidence illustrates the complex interplay between fear, violence, and vaccine hesitancy in conflict-affected regions. A tweet from September 10, 2024, warned, فِتنہ الخوارج کے حملے پولیو ٹیموں کو قطرے پلانے سے روک کر لاکھوں بچوں کو پولیو کا شکار بنا سکتے ہیں (“The Khawarij attacks can prevent polio teams from administering vaccines, putting millions of children at risk”). While invoking fear, this framing is embedded within a broader call for collective security, aligning with Model 3’s finding that security cues may suppress the isolating effect of fear.
A February 3, 2025, post similarly reframed militant violence in moral and securitized terms: فتنہ الخوارج بچوں کو پولیو ویکسین سے محروم کر کے ان کے مستقبل سے کھیل رہے ہیں (“The Khawarij are depriving children of vaccines, playing with their future”). This emphasizes not parental refusal but structural victimization and public health sabotage—fear refracted through a lens of collective threat. Another tweet the same day declared, معصوم پولیو ورکرز کا خون رائیگاں نہیں جائے گا۔ ہماری جدوجہد جاری رہے گی (“The blood of innocent workers will not go in vain. Our struggle will continue”), offering a frame of resilience and law and order defiance, which could neutralize fear’s demobilizing effect.
These contrast with a May 2, 2024 tweet: ٹی ٹی پی کے حملوں کا مقصد صحت کے عملے کو خوفزدہ کرنا ہے تاکہ وہ ویکسینیشن میں حصہ نہ لیں (“TTP’s attacks aim to intimidate healthcare staff and stop their participation in vaccination”). Here, fear is not directed at parents but at institutional operability—suggesting a weaker or diffuse hesitancy effect, consistent with Model 3’s moderation dynamic.
One example more directly reflects fear driven avoidance. A tweet from March 20, 2022, stated, پشاور میں پولیو ورکر اور محافظ قتل، والدین بچوں کو قطرے پلوانے سے ڈر رہے ہیں (“Polio worker and guard killed in Peshawar. Parents are now afraid to vaccinate their children”). This tweet isolates fear without accompanying security cues and exemplifies its independent positive effect on hesitancy, aligning with the main effect of fear.
Additional posts situate fear within broader narratives of state fragility. On December 11, 2021, one tweet asked, ٹی ٹی پی پولیو ٹیموں پر حملے کر رہی ہے۔ ریاست کہاں ہے؟ (“TTP is attacking polio teams. Where is the state?”), connecting fear to state inaction and reduced institutional trust. Another noted, ٹانک میں ٹیم پر فائرنگ ہوئی، لوگ اب پولیو ورکرز کے پاس جانے سے بھی ڈرتے ہیں (“Team attacked in Tank; people are now afraid to even approach polio workers”), reflecting disengagement rooted in unbuffered fear exposure.
These tweets demonstrate that fear’s effect on hesitancy is contingent. While fear alone may discourage vaccine uptake, its influence is suppressed when paired with security, moral outrage, or resilience frames. This supports the suppressing interaction found in Model 3: fear is most potent in the absence of counter framing, and most constrained when law and order or institutional narratives are simultaneously invoked.
H4: Tweets That Invoke Religious Framing Are More Likely to Express Polio Hesitancy, Even after Controlling for Fear and Trust
Religious Framing Model Testing H4
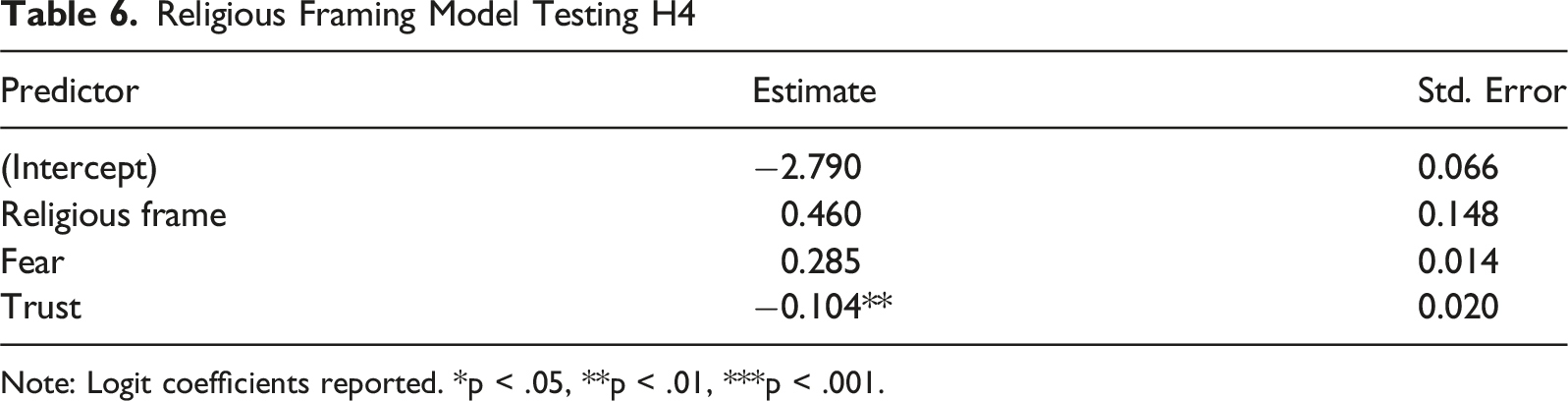
Note: Logit coefficients reported. *p < .05, **p < .01, ***p < .001.
The logic underpinning these tweets reflects not simply spiritual expression, but a reframing of medical interventions through theological and moral lenses. In this sense, religious framing reconfigures vaccination not as a biomedical good, but as a symbolic threat to religious identity and sovereignty.
For instance, a tweet shared on August 29, 2021, at 3:57 PM reads: کیا وجہ ہے کہ ایک غیر مسلم کو آپ زبردستی اسلام قبول نہیں کروا سکتے، یہ جانتے ہوئے کہ آخرت میں بہت بڑا نقصان ہونے والا ہے، انکار کے باوجود ہزار دلائل دینے کے، لیکن یہی غیر مسلم پولیو کے قطرے آپ کو زبردستی بندوق کے زور پر پلا رہے ہیں، یہ کہہ کر کہ اس میں آپ ہی کا فائدہ ہے، بغیر کسی ایک دلیل کے۔ پولیو۔ (“Why is it that you cannot forcibly convert a non-Muslim to Islam—even know-ing they face great loss in the Hereafter—despite offering countless arguments, yet the same non-Muslims are forcibly giving you polio drops at gunpoint, claiming it’s for your own good, without a single argument?”)
This statement draws a direct comparison between religious consent and medical coercion, casting the polio campaign as both illegitimate and spiritually intrusive.
A second tweet, posted on April 24, 2019, at 4:41 AM, amplifies this suspicion by citing anecdotal harm and invoking religious authority: ڈی سی پشاور کو شرم آنی چاہیے کہ وہ اسے افواہ کہہ رہا ہے۔ اب اپنے کیے دھرے پر پردہ ڈال رہا ہے۔ اکثر بچوں کا پیشاب رکتا نہیں تھا، پیشاب میں خون بھی آتا رہا۔ مولانا امان اللہ حقانی۔ (“The Deputy Commissioner of Peshawar should be ashamed for dismissing this as a rumor. He is now covering up what he did. Many children had urinary retention and blood in their urine.”—Maulana Amanullah Haqqani)
The inclusion of a named cleric lends religious authority to a medically dubious claim, reinforcing the legitimacy of vaccine rejection through theological channels.
A third tweet, shared on April 23, 2019, at 11:02 AM, bluntly equates the use of state force in religion and medicine: بندوق کے زور پہ اسلام کا نفاذ منظور نہیں، مگر بندوق کے زور پہ پولیو کے قطرے پلائے جا رہے ہیں۔ (“We reject the imposition of Islam at gunpoint, yet polio drops are being forced upon us at gunpoint.”)
This statement symbolically links opposition to vaccination with broader concerns about coercion and autonomy, positioning both religious and medical authority within a shared narrative of moral and civil resistance.
These tweets illustrate how religious framing does not merely coexist with vaccine hesitancy but actively reshapes public understanding of medical interventions—re-casting vaccination as sacrilegious or politically motivated. This skepticism arises not from religion itself but from how certain individuals deploy belief-based religious narratives to undermine trust in health campaigns. In conservative digital environments, such interpretations perform potent ideological work, fueling doubt and resistance under the guise of moral or spiritual authority.
Discussion
The findings of this study offer critical insights into the emotional and cultural architecture of polio vaccine hesitancy in Pakistan’s digital public sphere. Digital platforms function as affective environments where emotional meanings circulate, intensify, and reorganize across user communities (Awais, 2025a). Rather than confirming generic assumptions about how emotions and religion shape health behavior, the evidence reveals a highly contextualized landscape where fear, trust, and religious discourse function in ways that often defy conventional public health models. This reinforces the notion that vaccine resistance is not merely attitudinal but deeply discursive, a product of historically sedimented narratives, affective scripts, and socio-political anxieties.
Read through the lens of the Extended Parallel Process Model, these findings point to a systematic dominance of fear control rather than danger control in Urdu language vaccine discourse. EPPM predicts that fear should motivate protective action only when accompanied by strong efficacy cues (Tannenbaum et al., 2015; Witte, 1992). Yet, in this study, fear is consistently associated with higher levels of hesitancy even when trust-related expressions are present, suggesting a breakdown of the efficacy pathway. In Pakistan’s social media environment, fear appears to be embedded in narratives of uncertainty, harm, and conspiracy rather than in confidence about effective protection, a pattern consistent with misinformation-rich and low trust contexts (Krishna & Thompson, 2021) and with research showing that fear appeals can fail to motivate protection when efficacy cues are weak (Ruiter et al., 2014). These patterns also resonate with theories of social influence and cultural embeddedness, which emphasize that health attitudes are shaped not only by individual cognition but by socially shared narratives, norms, and identities (Bandura, 1999; Cialdini & Goldstein, 2004; Kleinman, 1980). In Urdu X discourse, fear, trust, and religious cues circulate through collective storylines of moral threat, historical grievance, and communal belonging, suggesting that vaccine hesitancy is socially produced and culturally situated rather than merely the outcome of isolated risk calculations.
Against this broader theoretical backdrop, the individual emotional signals identified in the analysis take on clearer interpretive meaning. First and foremost, trust emerged as a robust negative correlate of vaccine hesitancy, in line with global research highlighting the centrality of confidence in institutions and actors for promoting immunization uptake (Larson et al., 2015; Quinn et al., 2017). In Urdu language discourse, however, expressions of trust did not merely signal institutional legitimacy but often functioned as affirmations of national coherence and community solidarity. Tweets expressing gratitude toward local jirgas, the military, or provincial leadership suggest that trust operates at multiple registers—bureaucratic, social, and moral. This finding is especially significant in a context like Pakistan, where health infrastructure is frequently overlaid with political patronage and localized systems of authority (Closser, 2016). That trust remains salient even amid security threats and misinformation indicates that it may serve not just as a cognitive belief but as an affective anchor in moments of uncertainty.
At the same time, the strong and consistent effect of fear as a driver of hesitancy complicates theoretical expectations drawn from the Extended Parallel Process Model (EPPM). This directly diverges EPPM’s expectations that trust and fear interact synergistically to promote compliance. The EPPM suggests that fear can motivate protective behavior, provided that individuals also perceive a high level of efficacy in the recommended action (Tannenbaum et al., 2015; Witte, 1992). Yet, in the present study’s dataset, fear consistently showed a positive association with hesitancy even when expressions of trust were present. This suggests a breakdown in the efficacy pathway: trust in institutions may not always translate into confidence in the vaccine itself. Instead, fear in Pakistani discourse often co-occurs with uncertainty, trauma, and mistrust—focusing on adverse outcomes like side effects, deaths, and conspiracy rather than on disease prevention. This finding mirrors prior research in low-trust environments where fear becomes a vector for amplifying rumors rather than promoting compliance (Jolley & Douglas, 2014; Krishna & Thompson, 2021).
The interactive effect between fear and security framing offers further explanation. Contrary to H3’s expectation that security concerns would intensify fear’s impact, the study finds a suppressive interaction: Tweets that expressed fear in isolation were more likely to indicate hesitancy than those where fear co-occurred with security references. This surprising result suggests that when fear is embedded within narratives of violence, such as militant attacks or martyrdom of polio workers, it may shift the interpretive frame from biomedical doubt to political grievance. In other words, securitized fear does not necessarily delegitimize the vaccine; instead, it may highlight the broader vulnerabilities faced by health systems and frontline workers. Similar dynamics have been observed in conflict zones, where health interventions are interpreted through the lens of state fragility and resistance politics (see Hussain et al., 2016; Martinez-Bravo & Stegmann, 2022).
Religious framing functioned as an independent and potent correlate of vaccine hesitancy, even when controlling for fear and trust. Media representations of religiously charged issues often become arenas where moral authority, legitimacy, and social order are negotiated (Awais & Ali, 2025). This aligns with previous episodes in Nigeria and Pakistan before, where clerics framed vaccines as imperial or theological threats (Jegede, 2007; Rahim et al., 2022). In the corpus, religiously framed tweets did not merely moralize vaccine refusal but reclassified immunization itself as an act of spiritual transgression. Polio drops were depicted as haram, as tools of Western conspiracy, or as assaults on religious sovereignty. What’s notable here is that religious discourse was often entangled with legal and political metaphors—for example, comparing polio campaigns to forced religious conversion—thus transforming biomedical intervention into a symbolic battlefield over faith and autonomy. This supports work by Kasstan (2021), who found that vaccine refusal in a religious communities is less about dogma and more about preserving cultural and moral boundaries. These findings challenge the universal applicability of dominant health behavior theories. In Western frameworks like the EPPM or Health Belief Model, emotions and beliefs are largely treated as individual level predictors. But the Pakistani discourse we analyzed reveals a fundamentally different mechanism: affective expressions like fear or trust are not private sentiments but public narratives, entangled with collective memory, religious meaning, and political struggle. Fear in this context is not just an emotion—it is a form of testimony, a narrative device to articulate injury, abandonment, or resistance.
These limitations point to a deeper theoretical problem: the overreliance on Western behavioral models such as the Extended Parallel Process Model (EPPM) and the Health Belief Model (HBM), which treat health decision making as a rational, individual-level process influenced by perceived threat, efficacy, and trust. While these models have explanatory power in high-trust, high-resource settings, they often fail to account for the emotional, symbolic, and collective dimensions of health discourse in fragile or postcolonial contexts. In the case of Urdu tweets, emotions like fear do not simply represent personal threat assessments—they operate as affective testimonies of systemic betrayal, religious alienation, and geopolitical mistrust. Similarly, religious framing is not reducible to dogma or theological purity. Instead, it functions as a discursive strategy to contest biomedical authority, assert moral boundaries, and resist perceived cultural intrusion. These dynamics fall outside the scope of most Western models, which lack mechanisms for interpreting symbolic resistance or intertextual grievance. The findings therefore call for a reorientation of vaccine communication theory toward discursive, culturally embedded frameworks that can better capture the communicative labor of health resistance in the Global South.
Similarly, religious framing in present dataset rarely operated in isolation. It was often intertextual linked to security concerns, political mistrust, or colonial grievances. For instance, when polio drops are compared to forced religious imposition, the tweet is not simply making a theological point; it is invoking a broader critique of state power and foreign influence. This suggests that in settings marked by distrust and postcolonial trauma, health interventions may be interpreted less as scientific offerings and more as ideological incursions.
Another key insight from this study is the role of discursive layering in shaping public sentiment. Many tweets embedded multiple frames (fear, religion, security) within the same post. This suggests that vaccine hesitancy is not driven by a single variable (e.g., misinformation) but by the interaction of emotional and symbolic cues. The practical implication is that combating hesitancy will require more than fact checking or clerical endorsements. Interventions must address the deeper meanings attached to vaccination—meanings that are emotional, moral, and historical.
Beyond the Pakistani case, the findings contribute to global health communication by demonstrating that dominant behavioral models and message strategies cannot be assumed to travel uniformly across contexts. The results highlight the need for context sensitive approaches that attend to local histories, linguistic practices, and symbolic repertoires through which vaccine meanings are produced. In digitally mediated environments, where emotions and narratives circulate rapidly, effective health communication must therefore move beyond universal fear appeals toward culturally grounded, discourse aware engagement.
And, the use of Urdu language social media data represents a methodological contribution. Much of the vaccine communication literature is based on surveys or English language content. This paper’s approach leverages naturalistic, affect laden discourse from a non-Western, non-English digital space, revealing framings that might otherwise be overlooked. This reinforces the importance of linguistic localization in global health research and offers a template for analyzing vaccine discourse in other multilingual or postcolonial contexts.
This study also contributes to the growing literature on vaccine hesitancy in low- and middle-income countries by providing large-scale, discourse-based evidence from a polio endemic setting. While much prior work in LMICs has relied on surveys or program evaluations, the present analysis shows how vaccine meanings are actively negotiated in vernacular social media spaces through the interplay of trust, fear, security, and religious framing. By tracing how these emotional and symbolic cues co-occur in Urdu digital discourse, the findings illuminate the complex socio-cultural dynamics that shape vaccine attitudes and behaviors in fragile, low-trust contexts, offering insights that extend beyond Pakistan to similar settings across the Global South.
Policy and Communication Implications
The findings of this study carry several important implications for health communication, policy design, and global vaccine strategy especially in fragile states.
First, rebuilding trust in local institutions must precede behavior change efforts. The results confirm that trust is not merely a buffer against misinformation it actively reduces hesitancy. Communication strategies should therefore foreground institutional transparency, promote consistent messaging from community elders, and highlight successful outcomes from previous campaigns.
Second, fear appeals should be approached with caution. While fear is often used to signal urgency in vaccination campaigns, the analysis shows that it may backfire if not paired with credible efficacy cues and emotional reassurance. Messaging that emphasizes vulnerability without solutions can deepen mistrust and catalyze avoidance.
Third, religious engagement must go beyond endorsement. While fatwas and clerical statements are often deployed to legitimize vaccines, these may have limited impact if the framing of vaccination remains contested. Efforts should be made to co-create narratives with religious leaders that frame polio drops as protective of spiritual dignity, not just physical health.
Fourth, security-sensitive messaging must humanize health workers. In securitized environments, highlighting the sacrifices of polio teams (e.g., martyred workers) may shift the narrative from skepticism to solidarity. Rather than avoiding the security discourse, communicators should reframe it to honor commitment and community protection.
Finally, social media monitoring should be expanded to include non-English discourse. The emotional registers of vaccine skepticism vary by language and cultural context. By investing in natural language processing tools for underrepresented languages like Urdu, policymakers can access early signals of hesitancy and design culturally resonant interventions.
Footnotes
Acknowledgments
The author acknowledges the use of Artificial Intelligence in accordance with the journal’s policy. During the preparation of this manuscript, the author used ChatGPT (OpenAI; GPT-4 class large language model) for limited assistance with research conceptualization support, code refinement, data visualization support, and language editing. This use involved generative AI to assist in refining text and code, but did not generate data, results, or theoretical content. At no stage did the use of AI replace, override, or surpass the author’s intellectual contribution, judgment, or responsibility. All AI-assisted outputs were critically reviewed, verified, and edited by the author, who takes full responsibility for the accuracy, integrity, and validity of the final manuscript. This disclosure is made in accordance with the journal’s and SAGE’s Artificial Intelligence policy.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.