
Abstract
Individuals diagnosed with mental health disorders may have work-related difficulties that impact functioning in all life domains. With limited research on the integration of career and mental health counseling, authors used a discriminant function analysis to assess the predictability of accurately identifying diagnostic categories among 258 adolescents with attention-deficit hyperactivity disorder (ADHD) and learning disabilities (LDs) through the use of constructs derived from three career development inventories. Results showed that using an appropriate interpretive T-score from individuals with the same diagnosis enhanced the ability to discriminate between diagnoses of LD and ADHD in young adults. Implications for the practice of career counseling and development are provided.
Keywords
Modern career development practice suggests an inherent blending of career guidance and mental health counseling (Anderson & Niles, 2000; Dagley & Salter, 2004). Yet, many career counselors fear delving out of their specialty area (Chope, 2012), limiting the holistic progress of the career development profession. Undeniably, declining mental health can have reverberating effects on workplace performance and can become a central focus in career counseling sessions (Walker & Peterson, 2012). Understanding how and why symptoms of mental health disorders affect work performance can provide valuable insights to career practitioners and vocational researchers helping to effectively address the needs of the modern worker.
Several authors (Anderson & Niles, 2000; Crites, 1981; Dagley & Salter, 2004; Niles, Anderson, & Cover, 2000; Parmer & Rush, 2003; Zunker, 2006) call for further research that addresses the overlap between mental health and career counseling to allow for more holistic understanding of client needs. Specifically, Schultheiss (2000) encouraged a conceptualization of the career counseling process that includes developmental issues that are salient to clients. Developmental issues that are often intertwined with mental health concerns, noted Schultheiss (2000), include vocational identity development, clarification of attitudes, values, and beliefs. Specifically, attention-deficit hyperactivity disorder (ADHD) and learning disability (LD) diagnoses are two disorders strongly connected with the developmental period of adolescence, with direct linkage to mental health concerns surrounding work performance. Interestingly, research related to negative career beliefs, career attitudes, and vocational identity have been identified as significant concerns for young adults with LD and ADHD (Dipeolu, 2007; Dipeolu, Hargrave, Sniatecki, & Donaldson, 2012; Dipeolu, Sniatecki, Hargrave, & Storlie, 2013; Dipeolu, Hargrave, Deutsch, Sniatecki, & Storlie, under review; Walker & Peterson, 2012). As these youth develop maturity of vocational thoughts, attitudes, and identity, mental health issues may act as barriers, impacting a healthy career development trajectory.
Pace and Quinn (2000) highlighted the association between mental health issues and development and its impact on the early career development of youth. Specifically, dysfunctional career thinking, such as career indecision, may contribute to occupational stress and mental health concerns (Walker & Peterson, 2012). Relationships between depression and career decision making have also been identified in the scholarly literature by Rottinghaus, Jenkins, and Jantzer (2009). In spite of these established relationships, research studies on “… psychological well-being is underdeveloped in the areas of career development and vocational behavior” (Strauser, Lustig, & Ciftci, 2008, p. 22). By assisting clients to resolve work-related and mental health issues, career interventions can become more therapeutic (Crites, 1981), resulting in a holistic approach to working with career counseling clients. The field of career development can address the interlocking relationship of mental health and career development by focusing on accurate assessment of client concerns.
Results of studies addressing vocational thoughts, attitudes, and identity have encouraged researchers to explore the use of vocational assessments that address the existence of mental health issues among career counseling clients (Dipeolu, 2007; Dipeolu et al., 2012; Dipeolu et al., 2013; Dipeolu et al., under review; Walker & Peterson, 2012). Pace and Quinn (2000) support assessing the psychological dimensions of the career decision-making process and promote its examination when planning interventions for clients who present with career concerns. Assessment is central in both career and mental health counseling and a number of existing career assessments concurrently evaluate career and mental health issues. For example, constructs measured by the Career Thought Inventory (CTI; Sampson, Peterson, Lenz, Reardon, & Saunders, 1996) overlap with mental health concepts such as anxiety, decision-making clarity, and interpersonal conflict.
Conversely, vocational identity as measured by the Vocational Identity scale (VI; Holland, Daiger, & Power, 1980) of My Vocational Situation (MVS) is a construct linked with complex developmental tasks of adolescents, which involve issues related to mental health. The development of vocational identity occupies a central role in identity development for adolescents (Skorikov & Vondracek, 2007).This particular task is fundamentally grounded in adolescence, requiring complex cognitive abilities that exceed those in childhood. The acquisition of a strong vocational identity can provide the foundation for a sense of meaning and direction in occupational exploration and goal setting and may be particularly important for adolescents from at-risk and/or minority backgrounds (Skorikov & Vondracek, 2007). VI has been positively correlated with a number of adaptive characteristics and traits, including self-esteem, rational decision making, and directedness toward goal setting. Similarly, VI demonstrates an inverse relationship with negative, maladaptive career constructs including indecisiveness, depression, and lack of stability regarding goals (Skorikov & Vondracek, 2007).
The concept of career maturity/readiness is generally measured by the Attitudes Subscale of the Career Maturity Inventory–Revised (CMI-R; Crites & Savickas, 1996). The utility of this concept in career development with adolescents has been widely recognized and supported empirically (Patton & Creed, 2007). Research findings have shown a link between level of career readiness and several constructs related to mental health, including career decision making (Patton & Creed, 2007). The lack of career readiness may lead to indecision about career selection among adolescents. Altogether, strong links exist between dysfunctional career thoughts, vocational identity, career readiness operationalized using concomitant career assessments, and mental health. Undoubtedly, career instruments can be used to supplement client information in counseling and to help pinpoint client strengths, needs, and areas for improvement (Swanson & D’Achiardi, 2008) while providing a foundation for individualized intervention (Meyer et al., 2001).
Understanding the use of diagnostic categories while using career instruments can help strengthen the connection between mental health and career concerns. Although research using career inventories in career counseling is well established, there is little evidence that links the use of career instruments with mental health diagnoses in aid of the career counseling outcomes. The use of assessment, while focusing on diagnostic categories, may also link mental health and career counseling practices, particularly when the instrument is appropriately normed. Generally, test results have rarely been interpreted utilizing norms derived from individuals with disabilities. For young adults with disabilities, counselors need access to test results based on representative norms (Dipeolu, 2011) to ensure meaningful interpretation that can significantly impact session outcomes.
Despite the preponderance of evidence suggesting a strong connection between mental health disorders, career assessment, and development, little research has been conducted to help advance this understanding. In one university’s counseling center, over 11% of students presenting with career counseling issues also received treatment for mental health concerns (Pace & Quinn, 2000). As noted in the Diagnostic and Statistical Manual of Mental Disorders (DSM) 5th Ed. (DSM-5; American Psychiatric Association [APA], 2013), work-related difficulty is an important clinical diagnostic consideration for several psychiatric disorders, such as autism spectrum disorders, eating disorders, schizophrenia, ADHD, LDs, bipolar disorder, and major depression. Specifically, the symptoms associated with ADHD and LD diagnoses have direct impact on work effectiveness and performance. Symptoms within LD diagnostic categories interfere with work-related activities that require reading, mathematics, or written expression. Individuals with ADHD often experience the symptoms of inattention and impaired concentration in the workplace. To help highlight the connection between specific career assessments and mental health diagnoses, authors used a discriminant function analysis to assess the predictability and accuracy of identifying the diagnostic categories of ADHD and LD among young adults using three career assessments associated with relevant career constructs tied to the period of vocational development in adolescence.
Holistic Perspectives in Career Interventions
Parmer and Rush (2003) noted the full continuum of career counseling services extend beyond the more traditional services of career interest assessment, decision-making assistance, and goal-setting support. Career interventions should be centered on reducing work-related stress and improved coping with workplace difficulties such as anger, depression, work–life role imbalance (Parmer & Rush, 2003). Interventions addressing unemployment, one of the most serious and troublesome problems facing modern society (Creed & Klisch, 2005), are also part of the career counseling continuum. Unemployment is associated with lowered levels of psychological well-being and may lead to issues of grief or clinical depression (Creed & Klisch, 2005). Since many clients use career and workplace issues as an entry into discussing mental health concerns (Niles et al., 2000), counselors should be aware that these intertwined matters need to be concurrently explored in session.
Career professionals desiring to effectively address clients’ needs should seek proficiency in the diagnostic criteria of various mental health disorders, along with accompanying evidenced-based career interventions. This requires familiarity with the DSM-5 (APA, 2013) and the International Classification of diseases (ICD), 10 revision (ICD-10) in order to enhance a more holistic perspective on how current diagnostic classifications can be utilized in career counseling. The DSM fourth Edition Text Revision (APA, 2000) has been used across several professions to determine and help communicate client diagnoses. Diagnostic criteria in most mental health disorders identify the potential for occupational and work limitations and provide clinicians with clear understanding of how symptoms can impact work effectiveness and performance. Occupational and work-related concerns are the foundation of DSM-5 Code 62.29 (Other Problem Related to Employment) or ICD 10 Z. code 56.9 (Unspecified Problems Related to Employment). For example, problems around unemployment, threat of job loss, stressful work schedule, difficult work conditions, job dissatisfaction, job change, discord with boss or coworkers, and uncertainty about career choice fall under this specific code (APA, 2013). It is evident that work-related issues interfere with life roles (Super, 1984) and subsequently one’s mental health and well-being. By drawing special attention to work-related concerns, the DSM-5 continues to embrace work-related difficulties as significant contributors to the sizable number of existing mental health conditions.
Work Adjustment Needs of Youth With Disabilities
Adolescents begin to make important career decisions that they may not be developmentally ready to make during this stage of life (Savickas, 2005). Thus, career attitudes/readiness is considered to be a particularly important construct to assess during career exploration with young adults. Negative attitudes and stigma associated with having a mental health diagnosis are often internalized as dysfunctional beliefs and thoughts, resulting in increased stress for individuals with psychiatric disabilities (Saetermoe, Scattone, & Kim, 2001; Vash & Crewe, 2004). This increase in stress may exacerbate existing mental health conditions and career concerns, thereby influencing postschool transition readiness and work performance of young adults with ADHD and/or LD.
As highlighted by Schultheiss (2000), developmental issues such as vocational identity development, attitudes, and beliefs influence the career counseling process among young adults seeking assistance. These constructs can be accessed through the use of career assessments. The use of vocational assessment, while focusing on diagnostic categories, may help connect mental health and career counseling practices, particularly when using appropriately normed instruments. Hence, these authors examined three developmentally linked career constructs of vocational identity, career attitude/readiness, and negative career thoughts as measured by associated vocational inventories in young adults with ADHD and LD.
Vocational identity helps strengthen and solidify reality-based vocational aspirations (Sarriera, Silva, Kabbas, & Lopes, 2001) and psychological adjustment (Skorikov & Moore, 2001; Turner & Lapan, 2008) in young adulthood. Uncovering negative career beliefs and thoughts is considered one of the many goals to be addressed in career counseling (Zunker, 2002). Career maturity on the other hand is associated with career decision-making readiness connected to vocationally relevant developmental tasks in young adulthood (Super, Savickas, & Super, 1996; Savickas, 2002). Taken together, career readiness, vocational identity, and negative career thoughts among youth with specific mental health diagnoses, such as ADHD and/or LD, are vital developmental constructs to understand the career aspirations of young adults (Dipeolu, 2007; Dipeolu et al., 2012; Dipeolu et al., 2013; Dipeolu et al., under review; Walker & Peterson, 2012).
The purpose of this study is to examine how well group membership in a diagnostic category can be accurately predicted using scores on career assessment instruments collected from young adults with a diagnosis in either the LD or the ADHD category. Information gleaned from this might help empirically make the case for the connection between mental health disorders and career concern and promote the concurrent exploration of associated concerns in career counseling. The following two questions guided this research: (1) Is there a significantly different pattern of responses for scores on career instruments by young adults with diagnoses of LD versus ADHD? and (2) Which instrument variables contribute most to the group differentiation? These authors hypothesized that the three scales of the CTI, with interpretive scores renormed for the individuals diagnosed with ADHD and LD, would have a larger impact on the discriminant function analysis than the nonnormed scores of the other instruments.
Method
Sample
The sample consisted of 258 high school students, 119 diagnosed with ADHD (40.6%) and 139 (47.4%) with various LDs. The students with ADHD were recruited from three high schools (grades 8–12) in the northeastern United States and consisted of 35 (29%) females and 84 (70.6%) males. Students diagnosed with ADHD qualified for special education services under existing disability categories as defined in Part B of the Individuals with Disabilities Education Improvement Act (IDIEA; 2004) and as defined by Section 504 of the Rehabilitation Act of 1973. Student experiences were assumed to be similar in participating schools based on uniform federal guidelines for special education and disability services across the United States. Participants self-identified as White, non-Hispanic (45.4%, n = 54), African American (37%, n = 44), Hispanic (7.6%, n = 9), Native American (2.5%, n = 3), Asian (.8%, n = 1), and Other (4.2%, n = 5). The average age of the participants was 15.7 years (standard deviation [SD] = 2.01) and included freshmen (34.5%), sophomores (20.2%), juniors (16%), and seniors (21.8%).
Students identified as having LDs were 47 (34%) reading; 39 (28%) written expression; 36 (26%) mathematics; 7 (5%) written expression and reading; 6 (4%) math and reading; 3 (2%) math, reading, and written expression; and 1 (1%) unknown. Students diagnosed with LDs were recruited from two school districts (10 schools total) in the Midwest and consisted of 39 (28%) females and 100 (72%) males. The sample included 49 (35%) freshman, 26 (19%) sophomores, 35 (25%) juniors, and 29 (21%) seniors. The mean age for the sample was 16.4 years (SD = 1.5).
Procedures
Three hundred letters were sent to parents/guardians of students with ADHD requesting participation; 123 (41%) were returned. Four students did not sign the assent form. Three hundred eighteen parents/guardians of students with LDs were targeted for recruitment and contacted via mail. Of these, 150 (47.1%) gave permission for participation. The research team obtained assent from each participant. Three students decided that they did not want to participate and eight did not sign the assent form. Thus, 139 total students participated. A school transition specialist and a graduate assistant administered the instruments. Accommodations (periodic breaks and the use of a reader) were offered to students as they completed the instruments. Yet, no students utilized such accommodations during data collection.
Measures
Dysfunctional career-related thoughts were measured using the Career Thoughts Inventory (CTI; Sampson et al., 1996). The CTI contains 48 Likert-type scale items to which the respondents identify their level of agreement, with response options ranging from 1 (strongly agree) to 4 (strongly disagree). Three cluster areas of dysfunctional thinking were identified: (a) decision-making confusion (DMC), the inability to initiate or sustain the career decision-making process due to disabling emotions and/or limited understanding; (b) commitment anxiety (CA), the inability to commit to a career choice because of anxiety about the anticipated outcome; and (c) external conflict (EC), the inability to balance self-perception with input from significant others, translating into a reluctance to assume independence and/or responsibility for career decision making (Sampson et al., 1996). Respondents can show evidence of dysfunctional career thoughts in one, two, or all of the three cluster areas. The total score is intended to provide a global evaluation of negative/dysfunctional career thoughts. Research has supported the reliability of the CTI for students with and without LDs. Dipeolu et al. (2012) reported test–retest reliability of .69 for high school students without LDs and .89 for college students without LDs (Sampson et al., 1996). Dipeolu et al. (2012) found further support for the reliability of the CTI with students having LDs, with an α coefficient or reliability of .95 for the CTI total score and coefficients of .89, .80, and .75 for the DMC, CA, and EC subscales, respectively. The current sample resulted in reliabilities of .90, .78, and .74 for the DMC, CA, and EC subscales. According to Vernick (2002), several research studies have found CTI to be a stable and valid instrument for use during the career counseling process for non-LD population.
Career readiness was measured by the CMI-R (Crites & Savickas, 1996). The CMI-Attitudes (CMI-Att) utilizes a dichotomous response format (agree/disagree) and is comprised of 25 questions, with higher scores indicating a higher level of maturity or readiness. Studies have generally supported the reliability of the CMI-Att. For students with LDs, CMI-Att reliability coefficients have been moderately strong. Dipeolu (2007) found coefficients ranging from 0.69 (CMI-Com) to .80 (CMI-Tal). Similarly, Dipeolu et al. (2012) found moderately strong reliability estimates among students with LD of 0.74 for the CMI-Att. A reliability coefficient of .64 was calculated for the current sample. Jepsen and Prediger (1981) reported a convergent validity correlation of .37 with the Career Development Inventory (CDI; Super, Thompson, Lindeman, Jordaan, & Myers, 1981), a measure of career maturity. Busacca and Taber (2002) assumed that the current version of the CMI would have similar validity and reliability as the 1978 version of the instrument.
The VI (Hollandet al., 1980) scale was used to obtain information regarding participants’ vocational identity. The VI scale consisted of 18 items related to vocational identity, which refers to a sense of clarity regarding one’s personality, talents, interests, and goals (Holland et al., 1980). VI uses a dichotomous, true/false response format and the score is obtained by summing the number of false responses. Higher scores indicate a well-developed vocational identity. The developers assert that strong vocational identity is typified by consistent career-related decision making despite unavoidable uncertainty in one’s environment (Holland et al., 1980). According to Holland, Daiger, and Power (1980), internal consistency reliability coefficients for both male and female high school students, workers, and college students range from .82 to .86 and provide support for the construct validity. Additionally, among students with LDs, Dipeolu et al. (2012) found a KR-20 coefficient of 0.82, and 0.86 among students with ADHD (Dipeolu et al., 2013).
Results
A discriminant analysis was conducted to determine whether five variables—CTI-DMC, CTI-EC, CTI-CA scale scores, normed by diagnosis (see Table 1), and CMI-Att scale score and VI scores—could predict the diagnosis grouping for individual participants. Table 2 lists the means and SDs of each group on the variables used in the study. The data were analyzed using SPSS version 21.0 and listwise exclusion was utilized for missing data. The sample means were determined to meet the assumptions of multivariate normality, based on sample sizes. Homogeneity of variance was suspect, based on the significant Box’s M; however, the large sample size, relatively equal group sizes, and assessment of normality indicated to researchers that no transformations were necessary in the current analysis (Tabachnick & Fidell, 2001).
CTI Conversion Comparison.
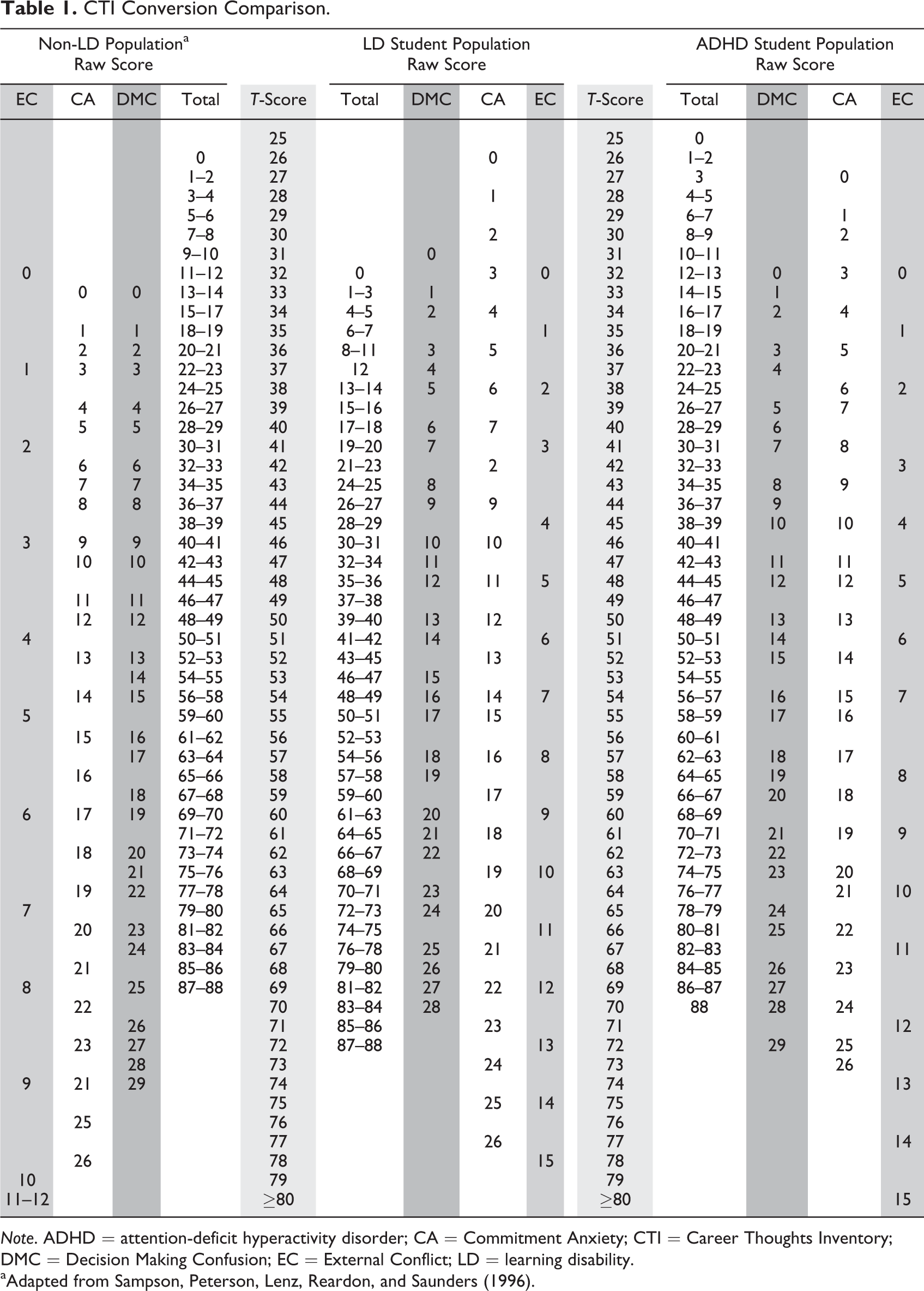
Note. ADHD = attention-deficit hyperactivity disorder; CA = Commitment Anxiety; CTI = Career Thoughts Inventory; DMC = Decision Making Confusion; EC = External Conflict; LD = learning disability. aAdapted from Sampson, Peterson, Lenz, Reardon, and Saunders (1996).
Means and Standard Deviations on the CTI DMC, EC, and CA Scale Scores, the VI Scale Score, and the CMI Attitude Scale Score for Two Groups.
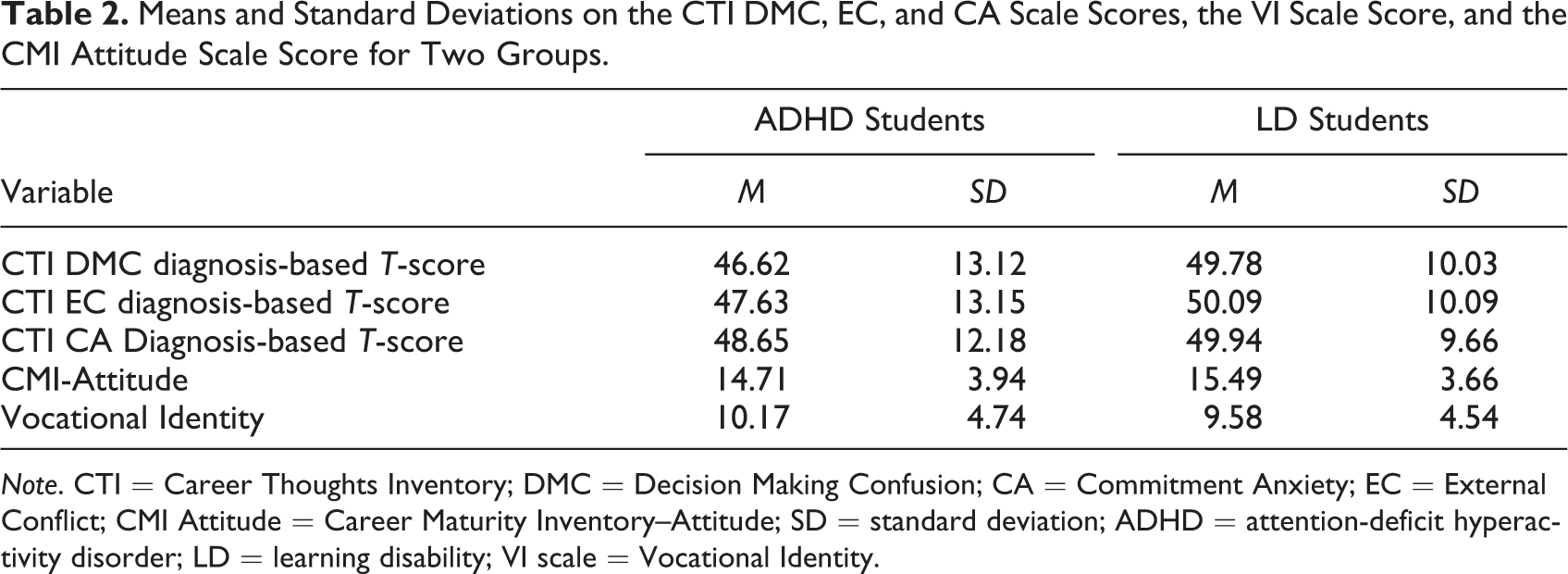
Note. CTI = Career Thoughts Inventory; DMC = Decision Making Confusion; CA = Commitment Anxiety; EC = External Conflict; CMI Attitude = Career Maturity Inventory–Attitude; SD = standard deviation; ADHD = attention-deficit hyperactivity disorder; LD = learning disability; VI scale = Vocational Identity.
Results supported the first hypothesis. One function was generated and was significant, Λ = .949, χ2 (5; N = 246) = 12.72, p < .03, indicating that the function of predictors significantly differentiated between participants with a diagnosis of ADHD and participants with a diagnosis of LD. Diagnostic difference was found to account for 5.1% of function variance. Standardized function coefficients and correlation coefficients (see Table 3) revealed that the variables of CTI-DMC, CTI-EC, and CMI-Att were most associated with the function. Original classification results revealed that 86.3% of the LD diagnostic group were correctly classified, while 38.7% of the ADHD diagnostic group were correctly classified. For the overall sample, 64.3% were correctly classified. The means of the discriminant functions are consistent with these results. The LD diagnosis group had a function mean of 0.21 while the ADHD diagnosis group had a mean of −0.26.
Standardized Discriminant Function and Structure Coefficients for the Two Diagnostic Groups.
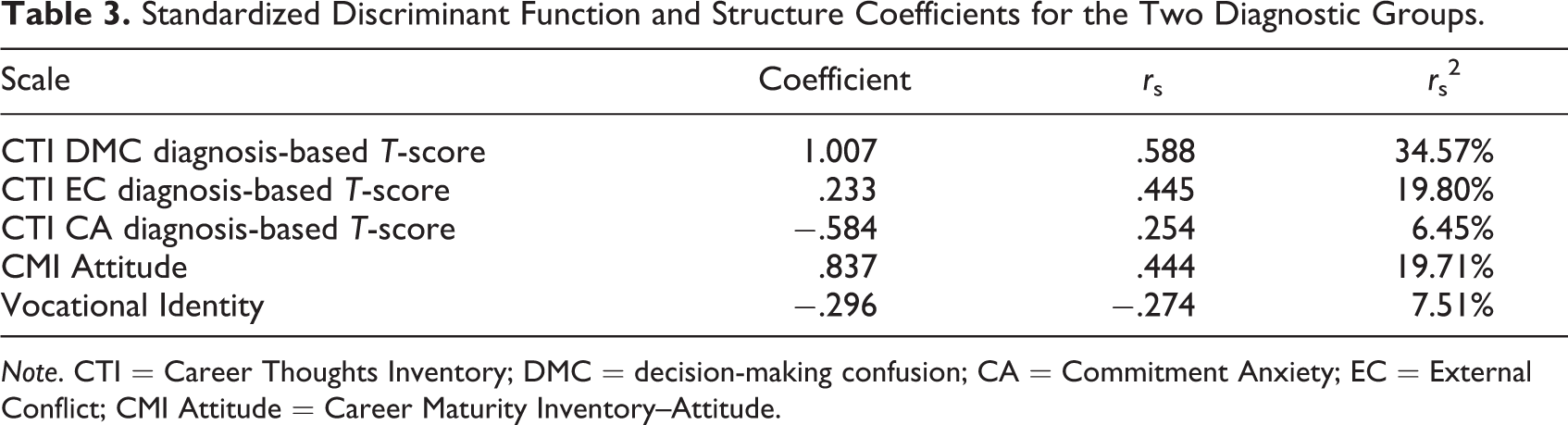
Note. CTI = Career Thoughts Inventory; DMC = decision-making confusion; CA = Commitment Anxiety; EC = External Conflict; CMI Attitude = Career Maturity Inventory–Attitude.
The second hypothesis was partially supported, with two of the three locally normed CTI subscale significantly related to the group differences in the discriminant function. Standardized discriminant function coefficients and structure coefficients were examined to determine what variables contributed to the group differences. Table 3 represents the set of coefficients for the function. DMC normed score for diagnosis, EC normed score for diagnosis, and CMI-Att were primarily responsible for group differences, with all three correlation coefficients exceeding .40 or r 2 values greater than 19%. These results suggest that participants with higher scores on DMC and EC normed for diagnostic group and higher scores on CMI-Att are likely to be classified as a member of the LD diagnostic group.
Discussion
Our first research question examined significantly different patterns of responses between the two diagnoses with interpretive scores for associated career instruments from similarly diagnosed young adults. Findings from this study show that there are distinct patterns of responses provided by young adults in these two diagnostic categories. Results showed participants with LD scored higher on the CMI-Att and CTI subscales of DMC and EC. As found in previous studies, these two diagnostic groups scored differently when compared with the normative samples presented in the inventory manuals (Dipeolu, Reardon, Sampson, & Burkhead, 2002; Dipeolu, 2007; Dipeolu & Keating, 2010; Dipeolu et al., 2012; Dipeolu et al., 2013). In response to our second research question, results showed there are three scale scores that are markedly related to the differentiation of diagnosis between young adults with LD and ADHD. These are DMC, EC, and CMI-Att with participants with LD scoring higher than participants with ADHD. The three constructs of DMC, EC, and CMI-Att are the largest contribution to the discriminant function.
The DMC and EC scales, as measured by the CTI, are designed to elicit information about dysfunctional thoughts related to career decisions. Based on previous research, students with a diagnosis of LD would be more sensitive to input from significant others while focusing on future goals. This may be due to their experiences of seeking accommodations and the reliance on input from external sources in their formative educational experiences, translating to a higher scores, particularly on the EC subscale (Dipeolu et al., 2002; Dipeolu & Keating, 2010). This would be demonstrated by relative dependent decision making, as students with LD weigh their options against external opinions from significant others in order to achieve the desired goal. Their enhanced need to seek external affirmation and assistance, either in a present or a future situation, is elicited in the particular response patterns on the EC subscale. Additionally, the relatively higher score on the DMC subscale suggests difficulty in making career decisions, which is likely to be confounded by their dependence on external sources as indicated by the higher score on the EC subscale for this diagnostic category.
The CMI-Att scale measures a participant’s readiness to engage the career planning process. In the same way that LD students seek external input from significant others in their career decision-making activities, these results suggest they would also be ready to evaluate options and identify career possibilities. Alternatively, young adults with a diagnosis of ADHD are more likely to have difficulty focusing on tasks and may be less likely to engage in forward-thinking behaviors that are necessary in career planning. Thus, they would be less likely to show difficulty related to the external conflict construct. Additionally, results suggest those with ADHD may be more prone to making premature career decisions.
The response pattern of participants in these diagnostic groups differ from each other, given that associated symptoms are unique for each diagnostic category. ADHD symptoms relate to behavioral difficulties associated with lack of focus or attention, impulsivity, and hasty decision making. In contrast, students with LD often find their disability an inherent component to their daily lives due to its strong association with reading, writing, and math, all significant activities of daily living. Accommodations, alternative ways of completing tasks, and assistance are all important parts of an LD student’s daily lives, emphasizing their dependence on others in order to achieve success. Because of this dependence, it is not surprising that students with LD reported higher scores on the EC scale of the CTI. This suggests difficulty with independent decision making, not related to typical adolescent development.
Implications for Practice
Upon further reflection, these authors found that the associated behavioral patterns, related to the mental health diagnoses, were important elements in understanding how young adults respond on the career inventories. Career counselors should be aware that the vocational identity and readiness to make career decisions may be impacted differently among the ADHD and LD population. A thorough examination of career concerns through the use of career inventory can accurately reflect strengths and weaknesses. It is equally important to pay particular attention to associated mental health concerns, such as indecisiveness, depression, lack of goal setting, self-esteem, and other vocationally relevant developmental tasks during this process.
Career and vocational concerns are directly linked to adolescent development issues (Schaub, 2012). Young adults who are able to demonstrate a higher level of developmentally related construct of career readiness, show a clear sense of vocational identity, and possess positive career-related thoughts are more likely to be successful in mastering the transition from school to work or further education (Hitchings, Luzzo, Ristow, Horvath, Retish, & Tanner, 2001). Based on the results from this study, counselors should expect different patterns of scores on DMC, EC, and CMI-Att for young adults with ADHD and LD and should readily integrate this information into career counseling sessions as well as explore possible connection with mental health concerns to provide effective interventions.
The results of this study found a significantly different pattern of responses on scores of associated career instruments between the two diagnoses of ADHD and LD when key interpretive scores for the CMI instrument scales were utilized. Complications associated with LD, such as one’s ability to read, write, or understand directions or spatial relationships, can color career or vocational choice in ways that differentiate this group’s response from that of the ADHD sample. Even with accommodations, many young adults with LD may perceive that careers requiring excessive writing or college majors requiring abundant reading may be overwhelming. Conversely, a diagnosis of ADHD includes behaviorally associated symptomatology in which medication may alleviate difficulties with inattention and concentration. Therefore, it seems plausible that young adults with ADHD would score relatively lower on DMC and EC scales because symptoms can be effectively controlled evading direct impact on personal and vocational identity. Moreover, the associated symptoms can be effectively managed with work space and structure modifications such as utilizing a strict schedule or minimizing external distraction in the immediate work vicinity. Knowing the particular mental health diagnosis and clients’ response patterns on associated career inventories provides counselors with an understanding of the effective career interventions that may enhance counseling outcomes.
There is a strong link between vocational identity, career readiness, dysfunctional career thoughts, and mental health. As noted, these developmentally related constructs are positively correlated with a number of adaptive characteristics and traits, including self-esteem, rational decision making, directedness toward goals, and vocationally relevant developmental tasks (Savickas, 2002). Conversely, these constructs demonstrate inverse relationship with negative, maladaptive career constructs including indecisiveness, depression, stress, and lack of stability regarding goals (Bullock-Yowell, Peterson, Reardon, Leierer, & Reed, 2011; Patton, & Creed, 2007; Rottinghaus, Jenkins, & Jantzer, 2009; Skorikov & Vondracek, 2007). Therefore, it is no accident that several studies, including Schaub (2012), have stressed the wisdom, benefit, and need for counselors to be trained to recognize the interconnection of career and personal counseling. Knowledge and awareness of symptoms of mental health diagnoses connected to specific usage of career assessment might help to predict career difficulties and can expand the repertoire of interventions available to the career practitioner. Moreover, career assessment results have rarely been interpreted utilizing norms derived from individuals with disabilities, especially youth with disabilities. There was a marked benefit of using a normed scale (see Table1) for ADHD and LD diagnoses with the CTI, instead of using a nondiagnosed population norm scale (listed in the manual). Being able to interpret young adults’ career assessment results, in relation to their diagnoses, assists with the efficacy of the counseling interventions.
This study supports the need for a broader conceptualization of career counseling services (Anderson & Niles, 2000; Crites, 1981; Dagley & Salter, 2004; Niles et al., 2000; Parmer and Rush, 2003; Zunker, 2006). Betz and Corning (1993) have argued against the separation of career and personal counseling by identifying the significance of the holistic philosophy of counseling relationships addressing career among different genders and cultures and the commonalities in the process of counseling. Schaub (2012) has written about the multiple roles college career centers have taken on in order to provide holistic services to their clients and clearly reports the commonality of emotional issues surfacing during career counseling sessions. Additionally, Schultheiss (2000) points out the similarities in the process of career and personal counseling. Results from this study support the need for career counselors to make the connection between career assessments, constructs, and mental health diagnoses during the counseling process. As evidenced-based practices continue to strengthen the standard of care for individuals with mental health diagnoses, career counselors must continue to holistically apply interventions to support optimal functioning in career decision and work performance. In turn, this may enhance the effectiveness of counseling and allows counselors to focus on career challenges that may impede the career development of individuals with ADHD and LD. This holistic approach enhances the application of best practices in career counseling sessions and interventions.
Limitations
Although the current sample size is similar to the size used to develop the norms of the aforementioned instruments, more participants could have strengthened the power of this study. Nationwide sampling would provide a very meaningful sample for norming purposes. In addition, researchers were unaware whether participants had any additional mental health diagnoses because participants in this study were from a school-based sample. Future researchers may consider collecting data from a clinical population.
Future studies should attempt to either have single diagnosis population sampling or have a third diagnostic group for dual diagnosis interpretation. When grouping students in these diagnoses, researchers in the current study did not identify comorbid diagnoses. Future studies should identify which students, if any, have a comorbid diagnosis of ADHD and LD of any type, in order to determine whether comorbidity creates a pattern of response different from the individual diagnoses explored in the current study. As the use of DSM-5 and ICD-10 continue to filtrate into the counseling profession, future researchers may consider replicating this study with the new criteria added to ADHD and LD diagnostic categories. Despite noted limitations, this study offers one way to help blend mental health issues (Sonnenberg & Chen, 2003) with work-related difficulties (Parmer & Rush, 2000), typifying the practice of career counseling in the 21st century (Dagley & Salter, 2004). Similar research can provide a foundation necessary to assist career counselors in addressing the full spectrum of the human experience by introducing a more holistic service in career practice.
Conclusion
A limited number of studies are devoted to the exploration of the overlap of career and personal/mental health counseling (Gold, & Scanlon, 1993; Niles et al., 2000; Pace & Quinn, 2000; Spengler, 2000). This study addressed this concern by demonstrating the interconnectednessof career concerns and mental health diagnoses. Knowing a particular mental health diagnosis might help predict the career issues that a client brings to the process of counseling, helping to individualize career counseling interventions. By using diagnostic categories and career instruments concurrently, career counselors can gain valuable insights to effectively address the holistic needs of the emerging adults with ADHD and LD.
Footnotes
Authors’ Note
The second and third authors, Stephanie Hargrave and Cassandra A. Storlie, contributed equally in the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.