
Abstract
Mothers of children with attention deficit/hyperactivity disorder were studied with regard to employment status, workplace characteristics, and depressive symptoms. Self-complexity theory proposes that complex self-representations buffer against depression; however, maternal employment may challenge mothers’ ability to attend to the many needs of their children. Findings from our cross-sectional study of 176 mothers revealed that employed mothers reported fewer depressive symptoms than unemployed mothers and those employed part time, providing support for the self-complexity buffering hypothesis. Furthermore, low levels of parenting stress were associated with fewer depressive symptoms. Implications are provided for career counseling and future research.
Keywords
Mothers of children with attention deficit/hyperactivity disorder (ADHD) are 3 times more likely than mothers of children without ADHD to be depressed, with approximately 50% of these mothers meeting lifetime criteria for major depressive disorder (Chronis et al., 2003; Chronis-Tuscano et al., 2013). Many of these mothers may be depressed due to the strain of caring for their child, the financial burdens associated with treatment, and the overwhelming responsibility for implementing and managing needed interventions. Employment has been associated with positive mental health for people in general and particularly for single mothers and low-income single mothers (Paul & Moser, 2009; Samuels-Dennis, 2006; Zabkiewicz, 2010). Employed mothers may receive psychological, economic, and social benefits from their work, as participation in both work and family roles can enhance overall well-being (Ford, Heinen, & Langkamer, 2007; Greenhaus & Powell, 2006; Wayne, Randel, & Stevens, 2006). Despite the abundance of research linking unemployment and maternal depression, the role of work in the lives of employed mothers of children with special needs is less understood. Thus, the purpose of this study was to assess differences in employment status and depressive symptoms among mothers of children with ADHD and investigate predictors of depressive symptoms for these mothers.
Parenting a child with ADHD can be very stressful (Gupta, 2007), as this disorder emerges in children prior to age 7 and is characterized by developmentally inappropriate levels of hyperactivity, inattention, and/or impulsivity (American Psychiatric Association, 2013). Children with ADHD often experience impaired academic and interpersonal functioning, and their families often report challenges in parent–child relationships and disruptions in marital and family functioning (Johnston & Chronis-Tuscano, 2014). In U.S. society, consistent with traditional gender roles, mothers often have primary responsibility for caring for children, especially children with special needs (National Alliance for Caregiving, 2009; Parke, 2000). In fact, mothers of children with ADHD are much more likely than fathers to be responsible for administering medication, participating in behavioral therapies, and assuming managerial and supervisory roles regarding daily routines (Fabiano, 2007; National Alliance for Caregiving, 2009; Parke, 2000). Moreover, mothers of children with ADHD are at risk for mental health problems, with depression being the most common psychological disorder among these women (Chronis-Tuscano et al., 2003).
Self-complexity theory provides propositions regarding the underlying mechanisms that may contribute to the prevalence of depression in mothers of children with ADHD. Specifically, the self-complexity buffering hypothesis proposes that complex self-representations buffer against depression, as multifaceted individuals have multiple aspects of self from which they can draw positive thoughts and feelings (Linville, 1985). During negative life events, individuals with greater self-complexity are better protected against the adverse mental health effects of stress (Linville, 1987). It is possible that maternal employment may be associated with lower levels of depression among mothers of children with ADHD, as the dual roles of both parent and employee may increase self-complexity and therefore protect those mothers who are employed against depression.
Consistent with this hypothesis, employment was shown to be a protective factor for mothers of children with special needs (Lewis, Kagan, Heaton, & Cranshaw, 1999). In one study, mothers’ participation in paid work was associated with more effective parenting and fewer problems in children with special needs (Harvey, 1998). Moreover, access to an income may reduce financial burdens associated with caring for a child with ADHD and may lessen some of the risk factors associated with socioeconomic disadvantage, including poor parenting, parenting stress, and negative child outcomes (Jackson, Bentler, & Franke, 2008; Pelham, Foster, & Robb, 2007). Employed mothers also have additional sources from which to draw positive self-appraisals and develop self-esteem (Wayne et al., 2006).
However, it is also possible that maternal employment may challenge mothers’ ability to attend to the needs of their children, as they may be less able to attend school meetings and provide appointments during the day. Employed mothers may also not be able to provide assistance with homework or close supervision after school hours (which protects against the development of conduct disorder for children with ADHD; Raggi, Chronis-Tuscano, Fishbein, & Groomes, 2009). In fact, mothers of children with ADHD often report stress related to managing their professional and parenting roles. For instance, mothers of children with ADHD often receive calls at work from school personnel conveying concerns about the child’s academic performance and disruptive behavior, which could lessen work productivity. In addition, mothers often have to miss work for therapist or physician’s appointments and teacher meetings (Brennan & Brannon, 2005). Mothers of children with special needs, who are not employed thus may feel less stressed and more able to respond to the needs of their children, without having to attend to work demands.
Given these competing possibilities, research is needed to better understand the role of employment in the lives of mothers who have children with ADHD. Clearly, there are numerous and complex factors that influence the experience of work in the lives of mothers of children with special needs. This study examines family-supportive organization perceptions (i.e., the degree to which the employer is perceived as understanding and helpful with regard to family responsibilities). Previous research has shown that employees who perceived their organization to be more family-supportive experienced less work–family conflict, more job satisfaction, more organizational commitment, and fewer turnover intentions than did employees who perceived their organizations to be less family supportive (Allen, 2001; Wayne et al., 2006). Family-supportive polices also were related to a sense of control over work and family, low levels of depression, low job dissatisfaction, low work family conflict, and few physiological complaints (Thomas & Ganster, 1995). Similarly, informal workplace practices, such as having a family-supportive environment, were more beneficial to the work–family experience than more formal practices, in part due to the flexibility they provided for individuals and their families (Wayne et al., 2006). Finally, supportive work environments have been correlated with positive benefits in family functioning (Wayne, Grzywacz, Carlson, & Kacmar, 2007).
Building on Linville’s (1987) theory of self-complexity that proposes that involvement in multiple roles (e.g., parenting and work) may protect against negative outcomes, this investigation studied mothers of children with ADHD, comparing those who were employed full-time (FT), employed part-time (PT), and unemployed (UE). Data were collected from a sample of mothers of children with ADHD to investigate the degree to which employment status, parental stress, and workplace characteristics were predictive of depressive symptoms. We hypothesized that employed mothers would report fewer depressive symptoms than PT and UE mothers due to the added complexity of participation in two major roles. We also hypothesized that, in addition to employment status, both parenting stress and family-supportive organization perceptions would be predictive of depressive symptoms with high parenting stress and less supportive workplaces being associated with depressive symptoms. The potential contributions of two-way and three-way interactions among the independent variables on depressive symptoms were assessed as well.
Method
Procedure
A link to a Qualtrics survey was posted on a total of 35 Listservs, blogs, social networking sites (e.g., Facebook), online forums (e.g., addforums.com), and websites for parents of children with ADHD (e.g., CHADD.org). Also, e-mail messages (with a link to the survey) were sent to parents, clinicians, coaches, schools, and camps associated with children having ADHD.
Participants who accessed the link were asked if they met the inclusion criteria (mother of child between the ages of 6 and 13 with ADHD). After completing the measures, they were provided with a list of resources for parents of children with ADHD and the opportunity to enter into a lottery to win one of five US$25 Amazon gift cards. The online survey was accessed by 475 people; 420 met inclusion criteria and provided consent to participate. Only 285 individuals began the questionnaire and responded to items on our survey. The length of the survey may have deterred many participants, which is not surprising, given that mothers often have multiple demands and little free time.
The data from those who did not complete at least 85% of the items were eliminated (consistent with recommendations in the literature; Hair, Toma, Hult, Ringle, & Sarstedt, 2013; Kivlighan, personal communication, April 24, 2015). The remaining 203 respondents had complete data sets (there were no missing data). To ensure the focus on mothers of children with ADHD, 27 participants were eliminated from the sample because their children had serious comorbid disorders (e.g., intellectual disabilities, bipolar disorder, pervasive developmental disorders, and autism spectrum disorders) that would typically preclude them from participation in ADHD studies.
Participants
The final sample consisted of 176 mothers of children with ADHD. Participants ranged in age from 24 to 56 years (M = 39.95, SD = 6.82). Regarding their employment status, 48.3% were employed FT, 26.2% PT, and 25.6% UE.
In terms of race, 91.5% of sample identified themselves as White, 1.7% Black/African American, 2.8% Hispanic/Latina, 1.1% Asian, 2.3% biracial or multiracial, and 0.6% as “other.” The majority of sample consisted of married women (76.1%), with some single (6.3%), divorced (10.8%), in a domestic partnership (3.4%), in a civil union (1.7%), and widowed (1.7%). Overall, the mothers were well educated: 0.6% attended at least some high school, 6.3% high school graduates, 4% trade/vocational school, 20.5% at least some college, 10.8% an associate’s, 25.6% a bachelor’s, 23.9% a master’s, or a doctoral degree (7.4%). The combined annual household income ranged from 24.4% below US$49,999, 31.8% between US$50,000 and US$99,999, 18.8% between US$100,000 and US$149,999, 12.5% between US$150,000 and US$199,999, 3.4% between US$200,000 and US$249,999, 3.4% between US$250,000 and US$299,999 to 5.7% above US$300,000. Approximately 23% of the participants reported being stay-at-home mothers, 12% were employed in administration, 10% in education, 10% in business, 10% in a medical/health care, and 10% in mental health. Participants also worked in legal fields (4%), administration assistance (7%), and other occupations (13%). The sample came from regions across the United States including the South (32.4%), Mid-Atlantic and Northeast (24.4%), West (20.5%), and Midwest (22.7%).
With regard to ADHD subtype, 12.5% of the children received a diagnosis of the inattentive, 22.7% hyperactive/impulsive or 51.7% combined subtype, and 13.1% were not otherwise specified. Over 51% of the children had individualized education plans or school accommodations, 34.1% received therapy, 79.5% medication, and 8.5% other treatments. Only 5.7% of the mothers indicated that their children were not receiving any form of treatment. In the sample, 22.7% of mothers had received a diagnosis of ADHD, and the majority of these mothers were taking medication for their ADHD (67.5%). Another 35% of diagnosed mothers attended therapy, and 32.5% were not receiving any form of treatment.
Measures
Parenting stress
The Parental Stress Scale (Berry & Jones, 1995), used to measure stress, consists of 18 items, both positive “I enjoy spending time with my child(ren)” and negative “The major source of stress in my life is my child(ren).” Participants responded on a 5-point Likert-type scale from 1 (strongly disagree) to 5 (strongly agree). Eight items were reverse coded, and a total score was calculated by summing the responses to each item, with high scores indicating much parenting stress. Berry and Jones (1995) found adequate reliability (α = .83) and support for convergent validity through correlations, with measures of perceived stress, social support, anxiety, marital satisfaction, and job satisfaction. For this sample, the Cronbach’s α was .88.
Family-supportive organization perceptions
The Family Supportive Organization Perceptions Scale (Allen, 2001) was used to measure perceptions of the supportiveness of their workplace regarding family activities and responsibilities. The measure contains 14 items (e.g., “Employees are given ample opportunity to perform both their job and their personal responsibilities as well”). Participants were asked, “To what extent do you agree that each of the following statements represent the philosophy or beliefs of your organization” on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree); 11 items were reverse coded and a total score was calculated, with high scores indicating positive perceptions of their organization’s family supportiveness. Strong internal consistency was reported (Cronbach’s α = .94). Content validity also was supported, with low scores being related to high work–family conflict, less job satisfaction, less organizational commitment, and high turnover intentions (Allen, 2001). Mothers who were UE completed the family-supportive organization perception measure about their last place of employment.
Depressive symptoms
The Center for Epidemiological Studies–Depression Scale (CES-D; Radloff, 1977) was used to measure depressive symptoms. The scale consists of 20 items; participants report the frequency of depressive symptoms during the past week on a 4-point scale ranging from 0 (less than a day) to 3 (most of the time, or 5–7 days). Scores fall between 0 and 60, with high scores indicating significant depressive symptomatology. The clinical cutoff score for depression using the CES-D is 16 or greater (Lewinsohn, Seeley, Roberts, & Allen, 1997). A study of maternal depression during the first 3 years of child-rearing showed support for adequate internal consistency (Wang, Wu, Anderson, & Florence, 2011) and the Cronbach’s α for this sample was .91. Support for construct validity was found, as high scores were related to low social support and stressful life events (Li & Hicks, 2010).
Demographics
Data were collected regarding age, gender, race/ethnicity, marital status, income, education, employment status, child and mother ADHD diagnosis, and treatment use.
Results
The means, standard deviations, reliabilities, ranges, and correlations among the measures are reported in Table 1. On average, the mothers reported moderate levels of parenting stress, family-supportive organization perceptions, and depressive symptoms.
Summary of Means, Standard Deviations, Reliability Estimates, and Correlations.
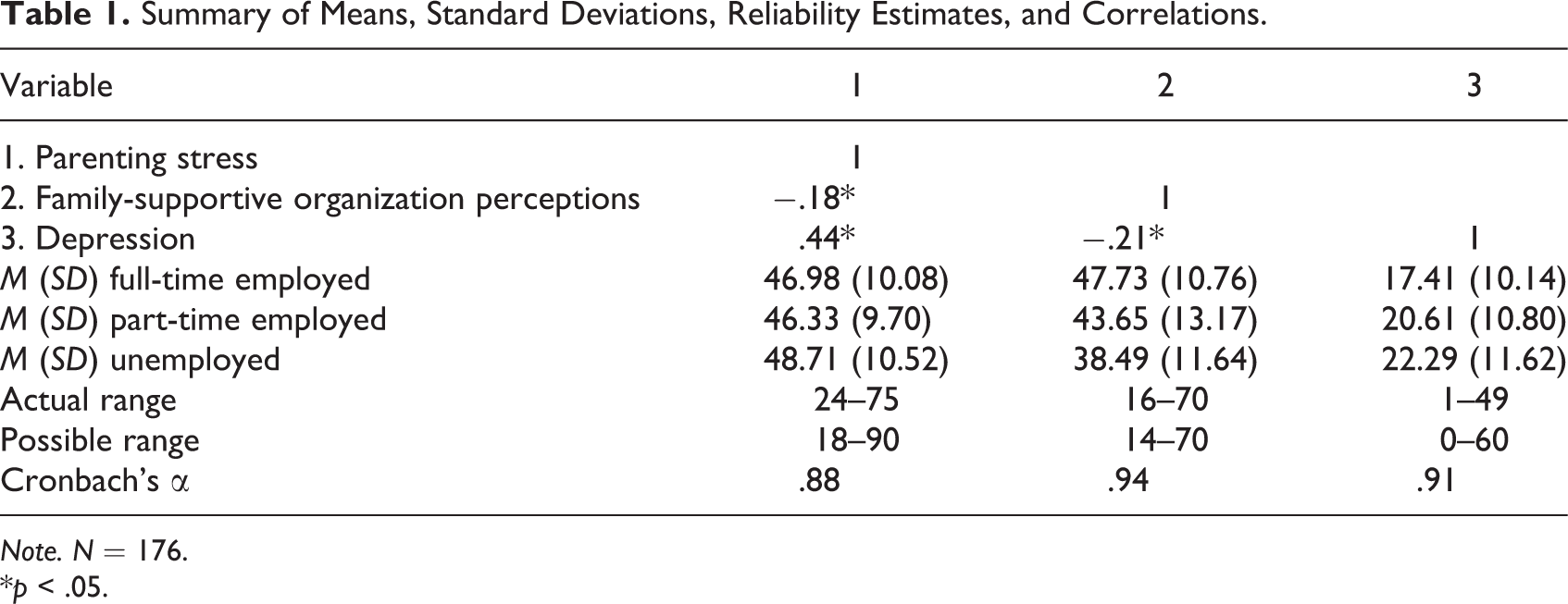
Note. N = 176.
*p < .05.
The assumptions for using regression were met. We calculated two regressions to investigate the degree to which employment status, parental stress, and family-supportive organization perceptions were predictive of depressive symptoms (and whether two-way or three-way interactions were present among the variables). First, we used contrast dummy coding for the employment status variable to test four comparisons among FT, PT, and UE mothers. The first dummy coded variable compared FT and UE individuals (FT = 1, PT = 0, and UE = −1). The second dummy coded variable allowed comparisons between FT and PT workers (FT = 1, PT = −1, and UE = 0). Next, the third dummy coded variable compared PT and UE mothers (FT = 0, PT = 1, UE = −1). The fourth and final dummy coded variable enabled us to examine the differences between being employed (FT or PT) with being UE (FT = 1, PT = 1, and UE = −2).
In addition, we created interaction terms by first centering the stress and family-supportive organization perception variables and then multiplying these variables by each dummy coded variable. For example, we multiplied the first dummy coded variable by the centered stress variable to create the FT versus UE by stress two-way interaction term. We computed the first three-way interaction term by multiplying the first dummy variable by the centered stress variable by the centered family-supportive organization perceptions variable. The creation of all interaction terms followed the steps provided in these examples.
To ensure independence among comparisons of employment status and to obtain all desired comparisons, two regression equations were calculated. First, the first and third dummy coded variables (comparing FT and UE individuals, and PT and UE mothers, respectively) were entered in the first step of the regression equation, followed by stress in the second step and family-supportive organization perceptions in the third step. The fourth step included the two-way interaction terms and the fifth step included the three-way interaction terms.
Collectively, the variables accounted for 25.5% of the variance in maternal depressive symptoms (see Table 2). Parenting stress was the most salient predictor, explaining 18.2% of the variance with employment status adding 4% to the explanation of depressive symptoms. FT workers experienced slightly fewer depressive symptoms when compared with UE mothers. As predicted, high levels of stress were associated with the presence of depressive symptoms. The two-way or three-way interaction terms were not significant.
Hierarchical Regression Predicting Depressive Symptoms Using FT Versus UE and PT Versus UE Variables.
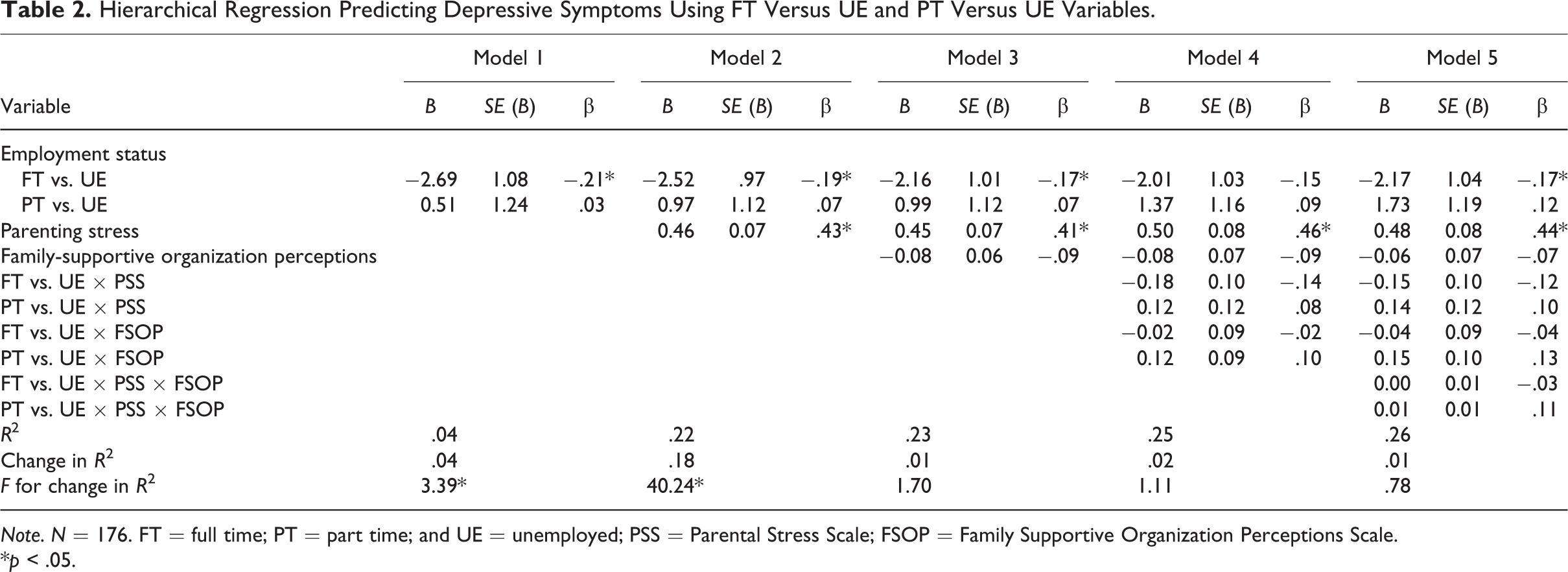
Note. N = 176. FT = full time; PT = part time; and UE = unemployed; PSS = Parental Stress Scale; FSOP = Family Supportive Organization Perceptions Scale.
*p < .05.
In the second regression, the second and fourth dummy coded variables (comparing FT and PT workers, and those employed [FT or PT], with UE mothers, respectively) were entered in the first step of the regression equation. The remaining steps included stress (second step), family-supportive organization perceptions (third step), the two-way interaction terms (fourth step), and the three-way interaction terms (fifth step). As would be expected, the findings replicated the first regression as the variables collectively explained 25.5% of the variance in maternal depressive symptoms, and the parenting stress was the most salient predictor (with high levels of stress being correlated with depressive symptoms; see Table 3). Notably, FT workers experienced slightly fewer depressive symptoms when compared to mothers who were employed PT. None of the two-way or three-way interaction terms were significant.
Hierarchical Regression Predicting Depressive Symptoms Using FT Versus PT and FT and PT Versus UE Variables.
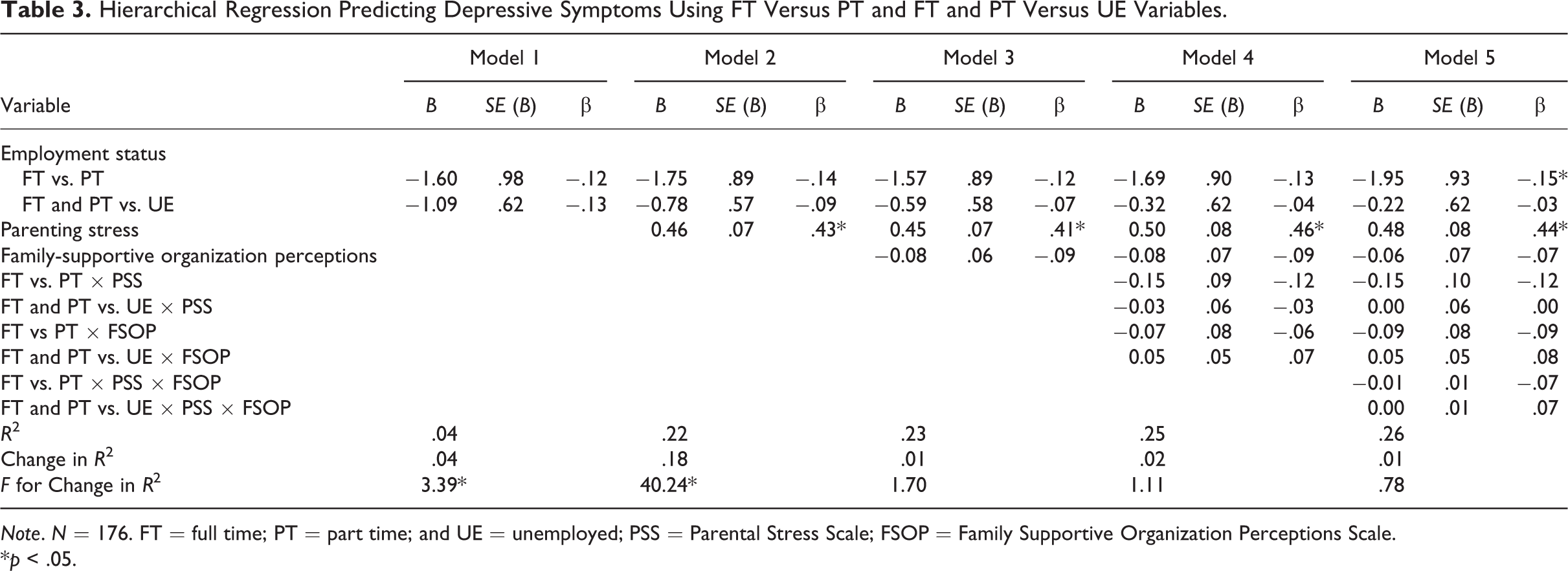
Note. N = 176. FT = full time; PT = part time; and UE = unemployed; PSS = Parental Stress Scale; FSOP = Family Supportive Organization Perceptions Scale.
*p < .05.
Discussion
Parenting a child with ADHD is stressful, and mothers of these children are at risk for depression (Chronis-Tuscano et al., 2013). Self-complexity theory would suggest that mothers with complex self-representations (e.g., those who work outside the home) may be less depressed as employment may act as a buffer against depression. However, equally plausible is the hypothesis that employment is a stressor for mothers of children with ADHD and interferes with their ability to parent their child. This study advances knowledge regarding the role of employment status and parental stress in predicting depressive symptoms among a group of mothers who are at risk for depression. We found that mothers who were employed experienced fewer depressive symptoms than those who were UE or employed PT, and parenting stress was predictive of depressive symptoms.
As hypothesized, the finding that employed mothers of children with ADHD experienced fewer depressive symptoms than UE and PT mothers might be explained by the proposition advanced by self-complexity theory that involvement in multiple roles may play a protective function against negative outcomes. For example, many benefits may be associated with work for mothers employed FT including monetary income, access to health care, social support, opportunities for increased self-confidence, and physical time away from parenting. However, given the correlational nature of the study, it is possible that mothers of children with ADHD who have fewer depressive symptoms may be able to obtain and maintain FT employment more readily than those who endorsed many depressive symptoms. Depression has been shown to be associated with lowered job retention, increased absenteeism, and lowered work productivity (Lerner et al., 2004) as well as challenges in managing time and completing work-related assignments (Adler et al., 2006). Also, it is important to note that the differences in depressive symptoms were small, perhaps due to not being able to recruit mothers with high numbers of depressive symptoms. Furthermore, some of the mothers were in therapy which may have contributed to the low levels of depressive symptoms.
When predicting depressive symptoms, parental stress was the strongest predictor. Parenting a child with ADHD can be overwhelming, and it was understandable that mothers experiencing the most stress had the highest number of depressive symptoms. On average, the mothers in this sample reported only moderate levels of parenting stress (perhaps due to their financial resources and educational levels). Those mothers with high levels of parental stress would likely be at risk for experiencing many depressive symptoms.
Interestingly, family-supportive organization perceptions were not predictive of depressive symptoms. This finding may have occurred because of the sample (who reported moderately supportive workplaces) or the retrospective nature of some of the data (UE mothers reported on their previous employment which could have been negatively affected by memory). If women were employed in less supportive organizations, this construct might account for additional variance in depressive symptoms.
Furthermore, there was a significant relationship between parental stress and depressive symptoms that may have removed variance that could be accounted for by family-supportive organization perceptions. Moreover, numerous unmeasured factors likely influence mother’s employment experiences, including meaningfulness of one’s work, the benefits provided, the amount of flexibility for employees managing work and family, or the type of job. In one study, the prestige of the job in which one was employed was associated with depression with those employed in higher prestige jobs being less depressed (Usdansky, Gordon, Wang, & Guzman, 2012). Furthermore, the support of coworkers may play a salient role in the mental health of employed mothers.
None of the interactions among the variables were predictive of depressive symptoms. This may have occurred because of the sample size that could be increased in further studies.
With regard to additional limitations of this study, the mothers were well educated, mostly White, and financially secure (despite efforts to recruit a diverse group of mothers). Only individuals who had access to a computer and had some free time were able to participate in the study. The homogeneity of the sample did not allow the findings to be generalized to diverse groups of women, as we cannot assume that the experiences of these women are shared by mothers of color, mothers who are living in poverty, those who do not have access to a computer, or those who do not have time to complete a survey. It is likely that women of color and mothers living in poverty would have additional stressors not experienced by a more privileged sample. In the future, researchers should study a more diverse group of mothers to understand the experiences of low-income women and women of color. Also, future research might compare mothers with ADHD to a control group of women whose children do not have ADHD.
Future research also should examine further the complexities associated with the relationship between workplace variables and depressive symptoms as desire for and type of employment could contribute to depression. Studies have shown that the link between depression and lack of employment was salient only for those women who want to be employed (Holmes, Erickson, & Hill, 2012; Usdansky et al., 2012).
Moreover, researchers might examine the role of spousal and family support for employed mothers of children with ADHD and the degree to which spouses share in the care of the child with ADHD. Spousal support was related negatively to depression in employed mothers in the United States, Korea, and Israel (O’Brien, Ganginis Del Pino, Yoo, Cinamon, & Han, 2014). It is possible that spousal support may act as a buffer against stress (Barnett & Hyde, 2001) and mental health problems and could enable mothers to remain employed.
With regard to practice, should these findings be replicated, counselors could assist mothers of children with ADHD to reduce parenting stress and maintain employment. Therapists could be encouraged to ask their clients to complete stress inventories, provide specific strategies for reducing stress, and evaluate the effectiveness of these interventions for their clients. Moreover, online interventions might be developed to reduce stress for mothers of children with ADHD (e.g., Chronis-Tuscano et al., 2013). Given the limited time and many responsibilities held by these mothers, online stress management programs might be an effective (and cost-efficient) method for teaching mothers how to improve coping and healthy behaviors (e.g., exercise, meditation, deep breathing, organization, and positive self-statements) to reduce the stress in their lives. Research has shown that online interventions can reduce stress and depression in college students (Hintz, Frazier, & Meredith, 2015); similar methodologies might be applied to working mothers.
Furthermore, mothers who are considering leaving their jobs or seeking employment could be educated about the small effects of employment on depressive symptoms and our finding that employed mothers reported fewer depressive symptoms than UE mothers and those employed PT. Assisting mothers of children with ADHD to be employed could provide families with needed financial resources to reduce poverty and enable access to evidence-based treatment to enhance child functioning. Also, counselors should screen for depressive symptoms in UE mothers who have children with ADHD. Given that maternal depression is associated with negative child outcomes (Chronis et al., 2007; Chronis-Tuscano et al., 2013), interventions to reduce maternal depression may not only assist the clients but also have downstream positive effects on parenting and child functioning.
Importantly, this research has the potential to inform public policy regarding the need for workplace strategies to retain effective employees who have children with special needs. Mothers of children with special needs often want to be employed (Gordon, Rosenman, & Cuskelly, 2007; Shearn & Todd, 2000); however, they have many obstacles preventing them from gaining employment outside of the home. Career counselors and counseling psychologists could advocate for improved work environments for parents on a national level. Employers could be educated about the obstacles faced by parents of children with special needs and encouraged to enact workplace policies that focus on reducing parental stress. Specifically, employers might create parent/employee networks, where people can share information and support each other regarding how to effectively manage work and family. Moreover, managers could ensure the distribution of benefit information, improve the knowledge of the human resource and benefit staff on issues related to working parents, increase supervisor training to improve sensitivity to employees with children having special needs, and continue to assess the workplace culture/environment to ensure that the company responds to the needs of the employees (Perrin et al., 2007).
To conclude, mothers of children with ADHD were studied with regard to employment status, parental stress, workplace characteristics, and depressive symptoms. Employed mothers reported slightly fewer depressive symptoms than UE mothers and those employed PT. Also, high levels of parental stress were associated with the presence of depressive symptoms. Vocational psychologists should continue to investigate how employment might protect against depression for employed mothers of children with special needs. Individual, organizational, and societal interventions could increase the number of mothers of children with special needs, who are able to both care for their children and achieve in the workplace.
Footnotes
Authors’ Note
This article was informed by Erica Merson’s dissertation and Elizabeth Sauber’s undergraduate thesis, and the prior versions were presented at annual meetings of the American Psychological Association.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided to Karen O’Brien from the University of Maryland Graduate School Research and Scholarship Award.