
Abstract

Xylitol has been demonstrated to be a safe and effective tooth-decay-preventive agent when used habitually. Nevertheless, its application has been limited by absence of formulations that demand minimal user adherence and are acceptable and safe in settings where chewing gum may not be allowed. A substantial body of literature suggests that a minimum of 5 to 6 grams and 3 exposures per day from chewing gum or candies are needed for a clinical effect to be achieved. At the same time, there is conflicting evidence in the literature from toothpaste studies suggesting that lower doses and less frequent exposures might be effective. The simultaneously growing use of xylitol as a sweetener in low amounts in foods and other consumables is increasing the overall exposure of the public to xylitol and may have additive benefits.
INTRODUCTION
In this paper, the authors address the questions: (1) What are the minimum dose and frequency for the use of xylitol-containing chewing gum for significantly lowering mutans streptococci levels? (2) Can delivery vehicles be produced that are applicable in settings where chewing gum or similar confections might be permitted?
Chewing gum
A randomized controlled trial was carried out to determine the dose-response of S. mutans in plaque and unstimulated saliva to xylitol gum (Milgrom et al., 2006). Participants (N = 132) were randomized into four groups: controls of 9.83 g sorbitol/0.702 g maltitol/day (G1), 3.44 g xylitol/day (G2), 6.88 g xylitol/day (G3), and 10.32 g xylitol/day (G4) in the form of 12 pellets (3 pellets/4 times/day). Plaque was collected in a standardized manner from specific sites, but was not weighed. Baseline, five-week, and six-month samples of plaque and unstimulated saliva showed decreasing levels of S. mutans across treatment groups of increasing dose. Xylitol at 6.88 g/day and 10.32 g/day reduced S. mutans in plaque at 5 wks, and in plaque and saliva at 6 mos (Figs. 1A, 1B). Results suggested a plateau effect for both plaque and saliva, indicating that exceeding the daily dose of xylitol 10.32 g/day is not likely to increase effectiveness. Alternatively, a dose of 3.44 g/day is not likely to show reductions in S. mutans levels.
A five-week randomized controlled trial was conducted to determine the reduction in S. mutans levels in plaque and unstimulated saliva to increasing frequency of xylitol gum use at a fixed daily dose of 10.32 g (Ly et al., 2006). Participants (N = 132) received either 10.32 g xylitol/day in the active group or 9.83 g sorbitol/0.7 g maltitol/day in the control group. The 10.32 g dose was used because it clearly would allow the hypothesis to be tested, even though a smaller dose (e.g., 6.88 g) might also have been possible. The number of pieces of gum did not change, and frequency of chewing (times per day) varied from 2 to 4 times/day within the active group; the control group chewed gum 4 times/day. There were no significant differences in S. mutans levels among the groups at baseline. At 5 wks, there was a linear reduction in S. mutans in plaque and unstimulated saliva to increasing frequency of xylitol gum use at a constant daily dose of 10.32 g (Fig. 1c). Although the difference observed for the ‘xylitol 2 times/day’ group was consistent with the hypothesis, the difference was not statistically significant.
Alternative vehicles
Study 1 of a recent experiment compared the potential of pediatric topical syrup to deliver xylitol vs. chewing gum. The basic rationale was that if the salivary xylitol concentrations were similar to those of chewing gum over a similar period, the effect on the oral flora should be the same, and a xylitol delivery system for the very young is desirable. Others have also considered syrup or a child’s dummy (pacifier) as a delivery vehicle (Uhari et al., 1996, 1998; Taipale et al., 2007).
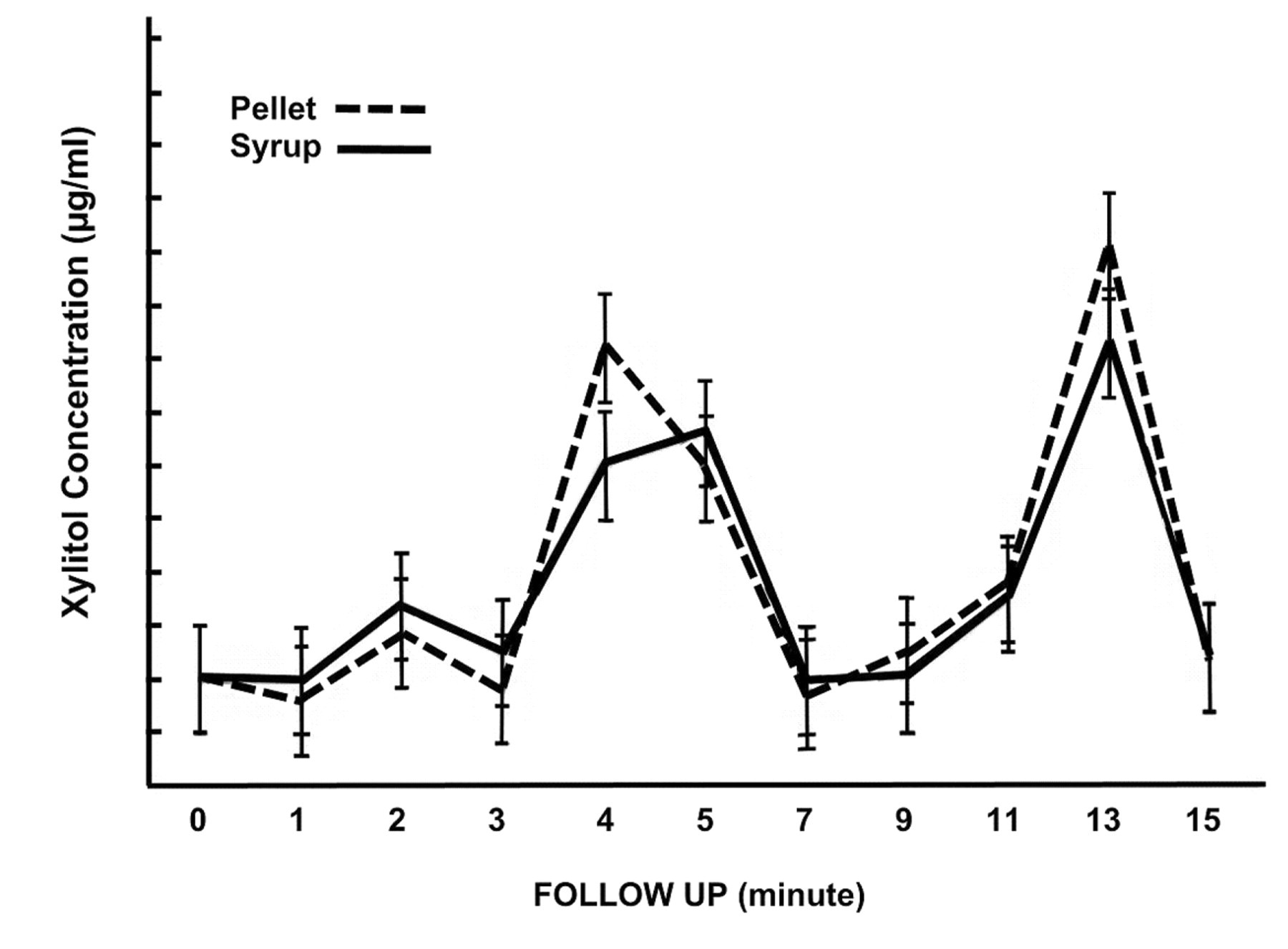
A within-subjects study design was used to compare the presence and time-course of xylitol concentrations in saliva from different delivery methods. Xylitol-containing pellet chewing gum (2.6 g) and 33% xylitol syrup (2.67 g) are presented here (Riedy et al., 2008). Adult study participants (N = 15) consumed one product per visit, with a seven-day washout period between products. Saliva samples were collected according to a standardized protocol at baseline and at 10 regular intervals following exposure. HPLC was used to quantify xylitol concentrations. Mean salivary xylitol concentrations and bimodal time curves were similar for the 2 delivery methods (Fig. 2); the correlation coefficient (r2) between the mean xylitol concentrations at each time-point for xylitol pellet chewing gum and the syrup was 0.96. Total Area Under the Curve (AUC) for the 2 products did not differ significantly (pellet gum—63.0 ng.min/mL, syrup—59.0 ng.min/mL).
A randomized control trial of the effect of xylitol syrup on early childhood caries has been conducted (Milgrom et al., 2009). Children at 9 to 15 mos of age were randomized to three conditions in which all were given syrup orally 3 times per day by their mother/caretaker. The groups were: 3 doses of 2.67 g xylitol each (8 g/day); 2 doses of 4.0 g xylitol per day plus a single dose of a sorbitol placebo (8 g/day xylitol); or a single dose of 2.67 g xylitol plus two sorbitol placebo doses. Results showed that the pediatric topical syrup was highly effective in preventing early childhood caries in a population with very high rates of disease by 24 mos of age.
In the second study of the xylitol salivary level experiment above (Riedy et al., 2008), bear-shaped xylitol confections (gummy bears) (2.6 g) were compared with xylitol pellet gum (2.6 g) at a similar concentration. Another set of participants (N = 15) served as their own control. The study method and saliva sampling were as described for Study 1, the ‘pellet gum compared with syrup’ study described above. Mean salivary xylitol concentrations and bimodal time curves were similar for the 2 delivery methods; the correlation coefficient (r2) between the mean xylitol concentrations at each time-point for xylitol pellet chewing gum and the gummy bears was 0.99. Total AUC for the 2 products did not differ significantly (pellet gum—63.0 ng.min/mL, gummy bears—55.9 ng.min/mL).
A randomized trial of the same bear-shaped confection is now being conducted in which the target is prevention of tooth decay in first permanent molars. About 30% of first molars are decayed by the time children reach first grade (around age 6 yrs). This current study is designed to address the targeted use of xylitol when the first permanent molars are erupting (Hujoel et al., 1999). The study is a two-group, 30-month randomized controlled clinical trial designed to assess the use of xylitol gummy bears as snack food during school hours to reduce dental caries among kindergarten children. Nearly all the children have untreated tooth decay in their primary teeth. Three hundred children are being randomized over 2 yrs into one of two treatment groups, receiving either 6 xylitol (1.3 g/piece, 2.6 g/dose—7.8 g/day) or 6 placebo gummy bears, distributed in the classroom evenly 3 times a day, for 9 mos.
DISCUSSION
The work presented confirms the interpretation of data from clinical studies regarding frequency and dose (Isokangas, 1987; Rekola, 1989; Mäkinen et al., 1995). One caution is that the effectiveness of the lowest dose in the Milgrom et al. study (2006) may have been masked, because the study participants had background levels of xylitol exposure, apparently from the diet. The bacterial reductions are a surrogate for reductions in tooth decay, but this is permissible, because the mechanism of action of xylitol is specifically antibacterial, and several studies have demonstrated parallel reductions of S. mutans and tooth decay. Thus, the correspondence between the findings in the Milgrom series and the clinical studies already in the literature means that chewing gum can be used as a vehicle in institutional programs. However, there will still be adherence issues related to those who must administer or supervise use. Gum has been shown to be less effective in individual treatment programs, because of lack of user adherence (Isotupa et al., 1995; Stecksén-Blicks et al., 2004).
A controlled study of complex design with xylitol-containing candies and gum was conducted in children about 10 yrs old (Alanen et al., 2000). This age group was targeted because of the potential to protect erupting second permanent molars. Three xylitol test groups received either candies (xylitol-maltitol or xylitol-polydextrose) or gum at 5 grams per day, divided into 3 doses over several yrs, depending on the group. The results showed 35 to 60% reductions in caries incidence in the test groups relative to the control individuals, and no difference between xylitol delivery vehicles. This study is important both because of its result in the same dosage/frequency range as the previous studies, and because the trial was intentionally sized to have adequate statistical power, even with anticipated attrition.
In contrast, there have been at least 2 studies attempting to demonstrate an effect of lower dosages. A non-randomized trial (Honkala et al., 2006) compared 1 xylitol candy 3 times per day (assumed to be 1.9 g total/day; the paper is unclear as to dose) with an untreated control in children and young adults in a school for those with disabilities. The control group consisted of students whose parents did not consent to the study. Baseline caries scores were fairly high and similar, yet the test group showed a significant reduction in caries incidence relative to the untreated control individuals. This may indeed have been because the test candy, according to the manufacturer’s Web site, was actually a 1:1 mixture of xylitol and maltitol. Other studies have shown that confections sweetened with maltitol alone reduced S. mutans levels in daily use with children (Ly et al., 2008). Thus, it is likely inaccurate to assert that 1.9 g xylitol per day alone is effective.
Oscarson and colleagues (2006) attempted to prevent caries in pre-school children using 0.5 to 1.0 grams of xylitol in lozenges beginning around age 2 yrs. This study failed to show any effect, largely because the underlying caries rate was extremely low (less than 1 dmfs per child at 4 yrs old), and the study had not been designed to detect such small, perhaps clinically insignificant, differences in the first place. Neither of these publications gives any rationale for the low dosages.
Xylitol-containing dentifrice
Several studies have evaluated sodium fluoride toothpaste formulations with xylitol. In all, they raise questions, in view of the previous data presented, as to how an exposure of as little as 0.1 to 0.2 g per day xylitol (assuming a 1 g dose of toothpaste that is 10% xylitol and given no more than twice per day) could result in significant reductions of S. mutans and dental caries. Unpublished work by Söderling and colleagues has shown that low-dose xylitol decreases the growth of specific mutans strains in culture during the growth phase, but this is hardly the same situation as in the mouth. An early short-term study of a xylitol-glycerol dentifrice showed reductions in salivary mutans (Svanberg and Birkhed, 1991).
In a study of 155 university students with high S. mutans levels and comparing 3 fluoridated dentifrices (toothpaste with or without triclosan, or triclosan plus 10% xylitol), only the toothpaste with triclosan and xylitol showed significant reductions in plaque and saliva mutans levels from the placebo at 6 mos, although the levels dropped in all groups (Jannesson et al., 2002). In this study, the students were instructed to use about 1.5 cm of the dentifrice (about 1 g) and to refrain from rinsing. The authors argue that the proprietary toothpaste was formulated to optimize the bioavailability of the xylitol, and that the dose used was larger than in other studies (for example, see Twetman and Petersson, 1995). No data were presented on how long the xylitol was present in the mouth after the exposures, nor were there data on adherence. It is possible that the effects of triclosan and xylitol are synergistic. The time-response effect seen in this study is consistent with that in the Milgrom et al. studies of xylitol-containing chewing gum.
A prospective study of 2630 Costa Rican children, initially 8 to 10 yrs of age, brushing twice daily with fluoride toothpaste with 10% xylitol or fluoride toothpaste alone, reported a 12% reduction in decayed/filled surfaces (DFS) and an 11% reduction in decayed/filled buccal and lingual surfaces (DFS-BL) among those children brushing with fluoride toothpaste and xylitol after 3 yrs (Sintes et al., 1995). This study should to be interpreted cautiously, since there was nearly 40% attrition in the study participant population, and the analysis did not use intent-to-treat analytical methods. Another 30-month study, by the same investigators, of 3394 seven- to 12-year-old children who used either fluoride toothpaste with and without 10% xylitol showed DFS and DFT increments of 1.30 and 0.69, respectively, for the 10% xylitol group when compared with the ‘fluoride toothpaste only’ group (Sintes et al., 2002). Again, there were limitations in the study design, and synergy between fluoride and xylitol cannot be ruled out. An additional concern is that these toothpastes contained sodium lauryl sulfate as a detergent, which may decrease the effectiveness of the xylitol (Assev et al., 1997).
Low-dose non-intentional exposure to xylitol
In the US, for example, xylitol is being added in small non-clinical amounts as a sweetener or advertising gimmick to various foods and children’s vitamins. Examples of many of the US products containing xylitol are given in Appendix Tables 1 and 2. It is possible that frequent lower-dose exposure to xylitol is beneficial without the effort of maintaining special programs. It is not possible to answer this question from the existing literature; however, two-thirds of the participants in the Milgrom et al. study (2006) had been exposed to low levels of xylitol in their diets (Roberts et al., 2002).
CONCLUSIONS
In spite of the considerable evidence that xylitol is an effective caries-preventive and cariostatic agent, an effective delivery system for xylitol, especially for children, demanding minimal adherence yet safe, has not been developed. A substantial body of work suggests that a minimum of 5 to 6 grams and 3 exposures per day are needed for a clinical effect to be achieved. At the same time, there is conflicting evidence in the literature from the xylitol toothpaste studies suggesting that lower doses and less-frequent exposures might be effective, but the synergistic effects of xylitol and fluoride or triclosan cannot be ruled out. Studies of new vehicles for xylitol, such as a xylitol-releasing dummy and a pediatric syrup, have been conducted.
Results of dose and frequency experiments with xylitol chewing gum in humans. Comparison of mean (± Standard Deviation) salivary xylitol concentrations (ng/mL) after the use of xylitol-containing gum and syrup (N = 15). (Adapted from Riedy et al., 2008, under the Biomed Central Open Access License Agreement)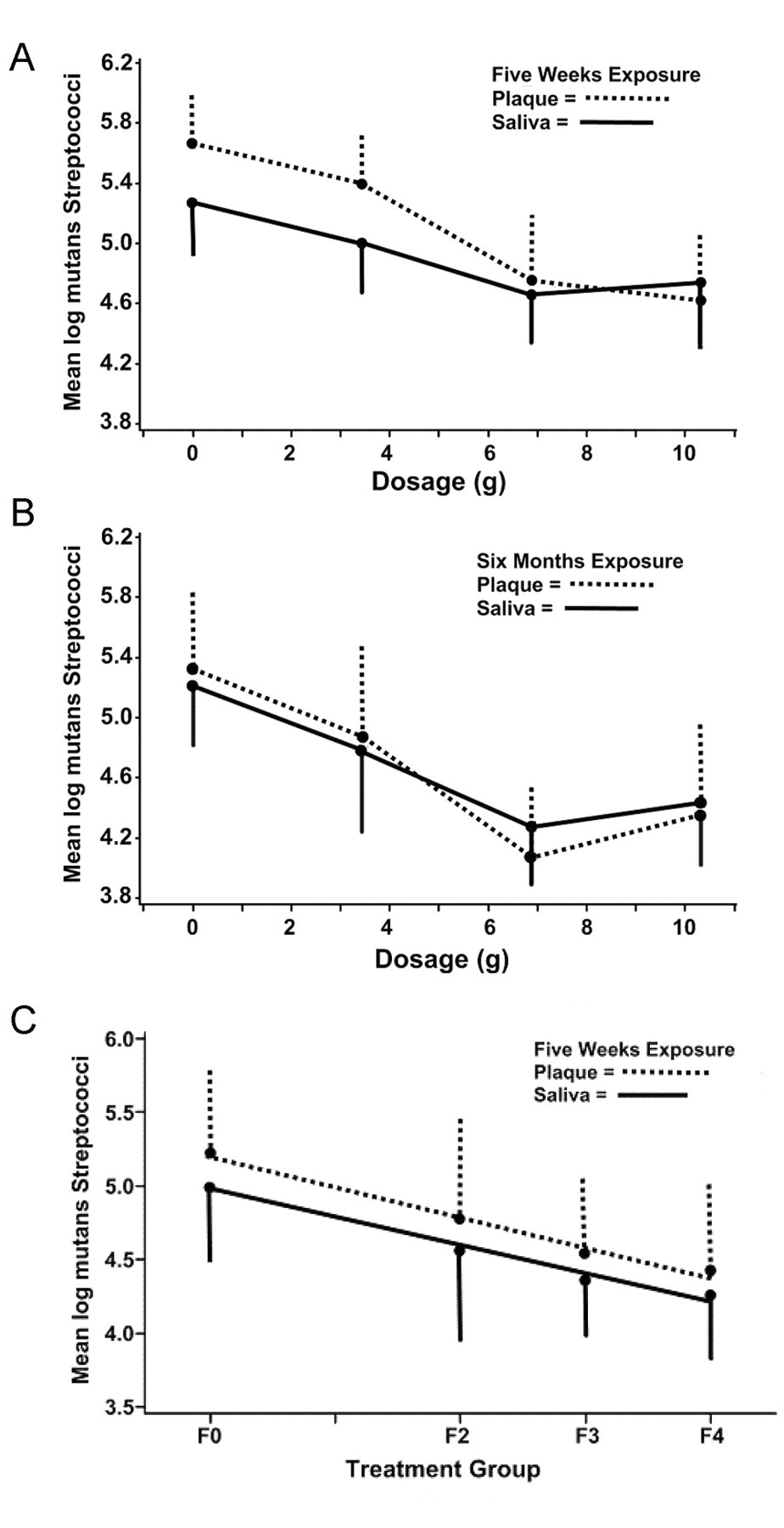
Footnotes
The authors declare no conflict of interest.
Presented at the International Conference on Novel Anti-caries and Remineralizing Agents, held in Vina del Mar, Chile, January 10–12, 2008
Acknowledgements
This work is supported by Grants U54 DE14254 from the NIDCR/NIH, R40MC03622 from the MCHB, HRSA, and by a Head Start IIP Grant 90YD0188 from the Office of Head Start, Agency for Children and Families.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.