
Abstract
Objective
We analyzed residual renal function (RRF) in a large number of new peritoneal dialysis (PD) patients to prospectively define the time course of decline of RRF and to evaluate the risk factors assumed to be associated with faster decline.
Study Design
Single-center, prospective cohort study.
Setting
Home PD unit of a tertiary care University Hospital.
Patients
The study included 242 patients starting continuous PD between January 1994 and December 1997, with a minimum follow-up of 6 months and at least three measurements of RRF.
Measurement
All patients had data on demographic and laboratory variables, episodes of peritonitis and the use of aminoglycoside (AG) antibiotics, temporary hemodialysis, and number of radiocontrast studies. Adequacy of PD was measured from 24-hour urine and dialysate collection and peritoneal equilibration test using standard methodology. Further data on RRF was collected every 3 to 4 months until the patient became anuric (urine volume < 100 mL/day or creatinine clearance < 1.0 mL/min) or until the end of study in December 1998.
Outcome Measure
The slope of the decline of residual glomerular filtration rate (GFR) (an average of renal urea and creatinine clearance) was the main outcome measure. Risk factors associated with faster decline were evaluated by a comparative analysis between patients in the highest and the lowest quartiles of the slopes of GFR, and a multivariate analysis using a stepwise option within linear regression and general linear models.
Results
There was a gradual deterioration of residual GFR with time on PD, with 40% of patients developing anuria at a mean of 20 months after the initiation of PD. On multivariate analysis, use of a larger volume of dialysate (p = 0.0001), higher rate of peritonitis (p = 0.0005), higher use of AG (p = 0.0006), presence of diabetes mellitus (p = 0.005), larger body mass index (BMI) (p = 0.01), and no use of antihypertensive medications (p = 0.04) independently predicted the steep slope of residual GFR. Male gender, higher grades of left ventricular dysfunction, and higher 24-hour proteinuria were associated with faster decline on univariate analysis only.
Conclusion
Faster decline of residual GFR corresponds with male gender, large BMI, presence of diabetes mellitus, higher grades of congestive heart failure, and higher 24-hour proteinuria. Higher rate of peritonitis and use of AG for the treatment of peritonitis is also associated independently with faster decline of residual GFR. Whether the type of PD (CAPD vs CCPD/NIPD) is associated with faster decline of residual GFR remains speculative.
The best means for assessing adequacy of PD remain ill defined (6). The concept of adequate dialysis should include some defined level of solute removal, adequate fluid removal to achieve normal volume homeostasis and blood pressure (BP) control, maintenance of adequate nutrition, normal acid–base balance, normal mineral metabolism, minimal anemia, normal lipid metabolism, and prevention of atherosclerosis. Small solute clearance has traditionally been an integral part of the overall definition of PD adequacy; most other measures appear to parallel solute removal. The importance of small solute clearance in PD has been confirmed by a variety of studies (7,8), most notably CANUSA, which showed that Kt/V and corrected creatinine clearance independently predict patient survival. All these studies have been confounded by residual renal function (RRF). Solute removal by PD may not be clinically equivalent to an equal quantitated solute removal by RRF. For example, the increased fractional secretion of creatinine during declining glomerular filtration rate (GFR) can be extremely misleading if other solutes do not show a fractional increase in excretion. Conversely, the increased secretion of organic solutes during chronic renal failure may far exceed the diffusive losses of the same solute during PD. Hence, the relative effects of renal versus peritoneal clearance on survival remain to be elucidated.
There is consensus that RRF has a major impact on the ability to achieve small solute clearance targets (9). Residual renal function contributes to approximately 25% of total Kt/V and 40% of total weekly creatinine clearance (WCCr). This numerical contribution is even greater for high and middle molecular weight solutes. As RRF deteriorates, failure to compensate for this loss will result in an increasing frequency of inadequate dialysis. Even with increasing dialysis prescription, as many as 40% of continuous ambulatory peritoneal dialysis (CAPD) patients fail to meet the target (10,11). Small changes in RRF with time on PD may account for major differences in quality of life and dialysis outcome. Data from the CANUSA study showed that the overall outcome was worse for patients who lost their RRF (12,13). The adverse impact of loss of RRF on outcome in PD patients could be due partly to loss of residual diuresis and difficulty in managing fluid status, hypertension, and left ventricular hypertrophy (LVH), all of which contribute to cardiovascular mortality (14). Residual renal function has also been shown to have a greater influence on dietary protein intake and nutritional status than peritoneal clearance (15-17).
Following the initial observation of Rottembourg et al., a number of studies have shown that the decline in RRF is more protracted in patients on PD than those on HD (18-22). However, the changes in RRF with time are not uniform in all patients. The issue of which factors affect preservation of RRF in patients with chronic renal failure once dialysis is started has received very little attention (23-27). The present study was designed to prospectively define the time course of decline of RRF in a large number of new PD patients.
Patients and Methods
A single-center, prospective cohort study was done at the Home Peritoneal Dialysis Unit of the Toronto Hospital (General and Western Division), Toronto, Canada. All patients starting PD between January 1994 and December 1997 were eligible for the study. Of the total of 309 patients, 67 patients were excluded for various reasons (Table 1). All the remaining patients (n = 242) with a minimum of 6 months of follow-up and at least three measurements of RRF were included in the study.
Reasons for Exclusion from the Study
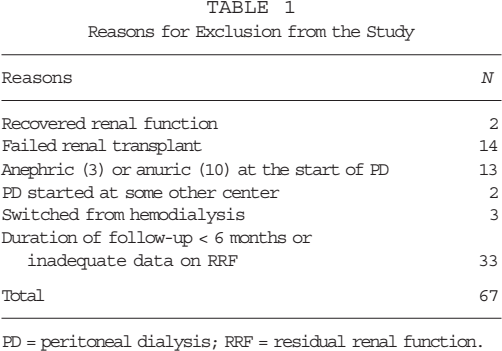
PD = peritoneal dialysis; RRF = residual renal function.
The demographic data recorded at enrollment included age at the start of PD, gender, height, weight, body mass index (BMI), race, underlying cause of end-stage renal disease (ESRD), presence of diabetes mellitus (DM), peripheral vascular disease (PVD), and LV dysfunction graded as class I through IV on echocardiography. Left ventricular ejection fraction of 60% or more was classified as class I and 40% – 59%, 20% – 39%, and < 20% as classes II, III, and IV, respectively. The diagnosis of PVD was based on clinical observation as well as Doppler and/or angiographic evidence The dialysis modality was chosen after repeated discussion with the patient and family on feasibility, social circumstances, advantages, and disadvantages of each modality. The dialysis prescription was that prescribed by the individual patient's physicians with changes made based on clinical condition and clearance data. Patients were evaluated in the outpatient PD clinic every 1 – 3 months.
Laboratory data included hemoglobin, serum urea, creatinine, albumin, corrected calcium, phosphorus, intact parathyroid hormone level, and lipid profile. Additional data included BP measurements and medications, including antihypertensives, angiotensin-converting enzyme (ACE) inhibitors, diuretics, lipid lowering drugs, and erythropoietin. All laboratory data and BPs were recorded as means of all measurements for every 6 months.
All episodes of peritonitis in each patient were recorded, including time of onset from the start of PD, causative organism, and dose and duration of antibiotics for the treatment. Use of aminoglycoside (AG) was classified according to days of treatment: AG use 0 = no use of AG; AG use 1 = AG used for less than 5 days at a time; AG use 2 = AG used for more than 5 days at least once during the follow-up. Number of patients who required discontinuation of PD and short-term HD for mechanical or infective complications were also recorded. Number and time of radiological studies using intravenous radiocontrast agents were recorded.
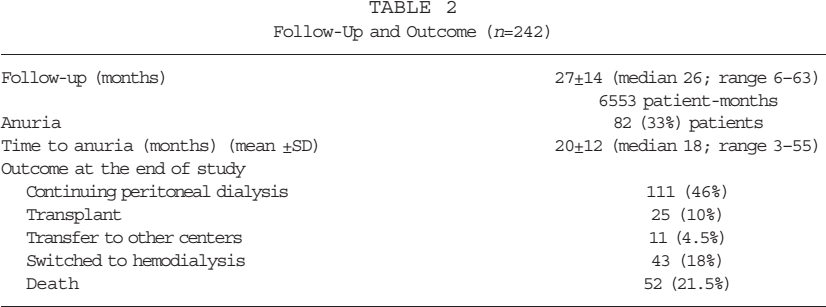
Adequacy of dialysis was measured using PD Adequest (Baxter Healthcare Corp., Deerfield, IL, U.S.A.). Renal and peritoneal urea and creatinine clearances were measured from 24-hour urine and dialysate collections and a simultaneous serum urea and creatinine determination obtained during the collection period. Dialysate creatinine excretion was corrected for glucose interference by using a validated correction factor. The renal contribution to creatinine clearance was estimated as the average of renal creatinine and urea clearance (residual GFR). The peritoneal equilibration test (PET) was done during each PD Adequest study using standard methodology (28). Further data on RRF were collected once every 3 – 4 months until the patient became anuric. Anuria was defined as 24-hour urine volume of less than 100 mL or creatinine clearance less than 1 mL/min on two consecutive occasions. All patients were followed until death, transfer to HD, transplant, or transfer to other centers for follow-up. All patients who continued PD were censored at the end of the study in December 1998 (Table 2).
Follow-Up and Outcome (n=242)
The clinical outcome measure in the present study was slope of deterioration of residual GFR and urine volume. Statistical analysis was done using SAS computer software, version 6 (SAS Institute, Cary, IL, U.S.A.). Repeated-measures ANOVA was used to see the variability of laboratory data and clearances with time after start of dialysis. A simple linear regression analysis was performed in each patient between calculated residual GFR and urine volume and time after start of dialysis until the last observation or until the end of the study. A comparative analysis between the patients in the highest and the lowest quartiles of the slope for residual GFR was done using chi-square, Fisher's exact test, and Student's t-test where appropriate. Risk factors assumed to be associated with residual GFR slopes were evaluated using multivariate analysis. The stepwise option within linear regression analysis was used for the selection of continuous variables, and all the variables with significance at the level of 0.15 were retained in the model. All these selected variables were incorporated with chosen categorical variables into a general linear model to select the best predictors for the slope of residual GFR with time on dialysis. A p value of less than 0.05 was accepted as statistically significant.
Results
Demographic data of the study cohort are presented in Table 3. Of the total of 242 patients, 211 (87%) started CAPD with mean dialysate volume of 8.3 ± 0.9 L/day. Twenty patients (8%) started continuous cycling PD (CCPD) and 11 (5%) started nocturnal intermittent peritoneal dialysis (NIPD). The dialysate volume in CCPD was 12.9 ± 2.7 L/day (10.9 ± 2.5 in the night and 2.0 ± 0.8 in the day), and on NIPD it was 12.2 ± 1.9 L/day used over 9 hours at night.
Demographic Data (n=242)
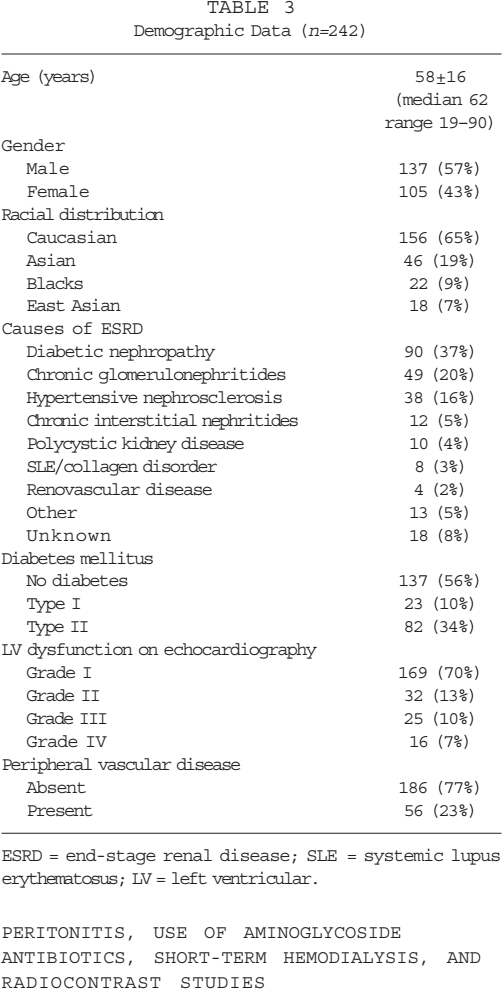
ESRD = end-stage renal disease; SLE = systemic lupus erythematosus; LV = left ventricular.
Dialysis prescription was changed in 61 patients (25%) during follow-up at a median of 12 months (range 3 – 49 months). A second change was required in 11 patients (4.5%) at a median of 20 months (range 11 – 49 months), and a third change was made in 3 patients (1%) at a median of 22 months (range 15 – 33 months). Eighteen patients changed from CAPD to automated dialysis, whereas the rest continued on the same modality with an increase in dialysate volume. In 6 patients who maintained good residual GFR, the volume of dialysate was decreased during follow-up.
Peritonitis, Use of Aminoglycoside Antibiotics, Short-Term Hemodialysis, and Radiocontrast Studies
A total of 234 episodes of peritonitis occurred in 128 patients (53%) (rate 1 episode per 23.8 patient-months); 114 patients (47%) did not have any peritonitis during the follow-up; 75 patients (31%) had only 1 episode of peritonitis, and 53 patients (22%) had 2 or more episodes of peritonitis.
Aminoglycoside antibiotics were given for the treatment of peritonitis in 218 episodes (for less than 5 days in 115 episodes; and for 5 days or longer in 103, maximum 42 days) and for infection of a great toe in 1 (14 days). No AG antibiotics (AG use = 0) were given in 139 patients (57%) because of no peritonitis in 114 patients and peritonitis treated without AG in 25 patients. Aminoglycosides were given for less than 5 days at a time (AG use = 1) in 46 patients (19%) and for 5 days or longer at least once (AG use = 2) in 57 patients (24%).
Twenty-seven patients (11%) required temporary discontinuation of PD and short-term HD for a period ranging between 2 weeks and 3 months. Hemodialysis was done once in 25 patients (10%) and twice in 2 patients (1%).
Overall, 84 radiocontrast studies were done in 61 patients (25%): 45 patients had only 1 study, 11 patients had 2, 3 patients had 3, and 2 patients had 4 studies.
Adequacy of PD
Of a total of 359 PD Adequest measurements, 319 were done before the onset of anuria and 40 were done after anuria. The mean D/P (dialysate-to-plasma) creatinine was 0.68 ± 0.11. On the first PD Adequest done within 6 months of initiation of PD, renal Kt/V urea was 0.62 ± 0.46 and renal WCCr was 35.3 ± 23.7 L/week, contributing 24% and 41% of the total urea and creatinine clearance respectively (Table 4). In patients who developed anuria during follow-up, the total Kt/V (2.11 ± 0.47) and WCCr (58.0 ± 12.0 L/week) were maintained at the target levels, with nPNA (normalized protein equivalent of total nitrogen appearance) of 0.871 ± 0.212 g/kg of actual body weight.
Adequacy of PD at the Time of Initiation of PD
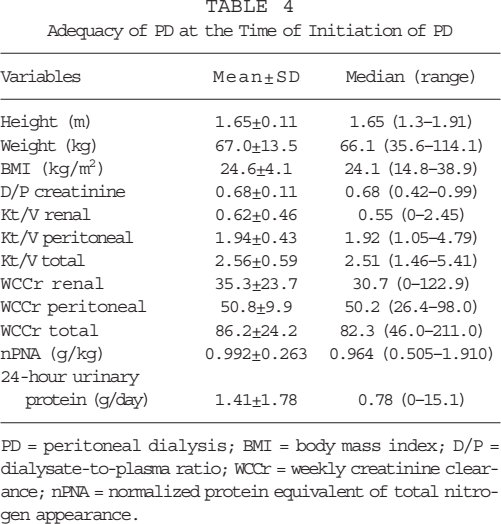
PD = peritoneal dialysis; BMI = body mass index; D/P = dialysate-to-plasma ratio; WCCr = weekly creatinine clearance; nPNA = normalized protein equivalent of total nitrogen appearance.
Medications
Seventy-six percent of the patients needed anti-hypertensive medications and 24% of the patients needed antilipemic drugs (Table 5). Diuretics were used in 37% of patients in an attempt to increase or maintain urine output. Fifty-five percent of patients were on erythropoeitin, with the dose ranging from 1000 to 24 000 units (median 4000 units per week; 84 units/kg/week).
Medications
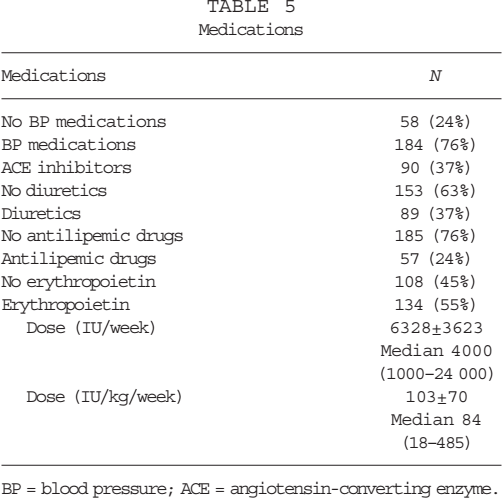
BP = blood pressure; ACE = angiotensin-converting enzyme.
Rate of Decline of Residual GFR and Urine Volume
There was a linear decline in residual renal clearance with time, whereas there was not a good correlation between 24-hour urine volume and time on dialysis. Eighty-two patients (33%) developed anuria during follow-up at a mean of 20 ± 12 months of initiation of PD (Table 2). The 24-hour urine volume was maintained unchanged for approximately 30 months of starting PD (Figures 1, 2; Table 6).
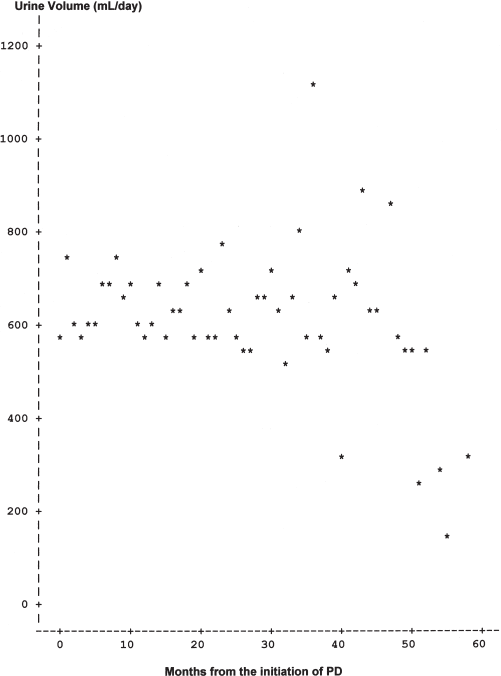
Regression plot of 24-hour urine volume against time on peritoneal dialysis is shown.
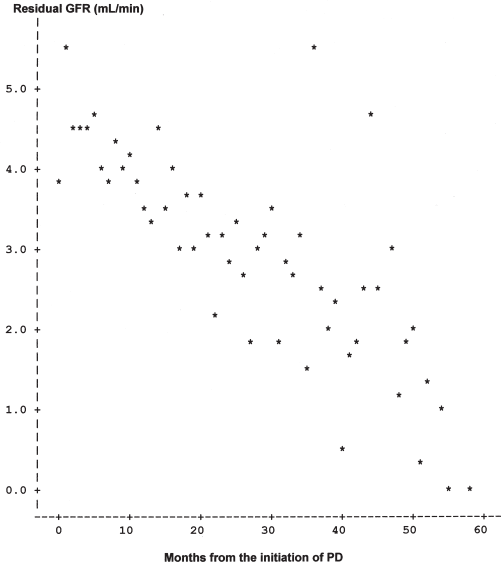
Regression plot of residual glomerular filtration rate (GFR) against time on peritoneal dialysis (PD) is shown.
Rate of Decline of Residual Glomerular Filtration Rate (GFR) and Urine Volume
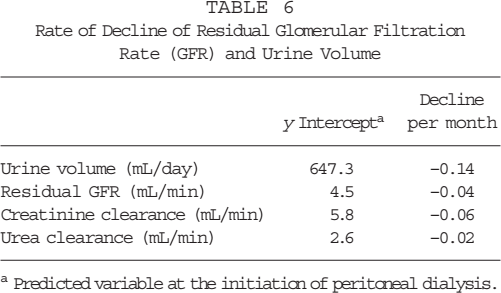
Predicted variable at the initiation of peritoneal dialysis.
Comparative Analysis for Patients in Upper and Lower Quartiles of Slope of RRF
To characterize the properties of patients who had the fastest decline of RRF, we did a comparative analysis between the lowest and the highest quartiles of patients according to the slope of residual GFR (Table 7). Patients with the fastest decline had male gender, DM, higher grades of LV dysfunction, and higher 24-hour urinary protein excretion rate. There was no difference in age, racial distribution, type of PD (CAPD vs CCPD/NIPD), rate of peritonitis, use of AGs, and other biochemical parameters between the two groups. Also, there was no difference in the level of BP control, use of antihypertensive medications, ACE inhibitors, diuretics, erythropoietin, and antilipid medications between the two groups.
Comparative Analysis Between Patients in the Lowest and the Highest Quartiles of the Slope of Residual Glomerular Filtration Rate (GFR)
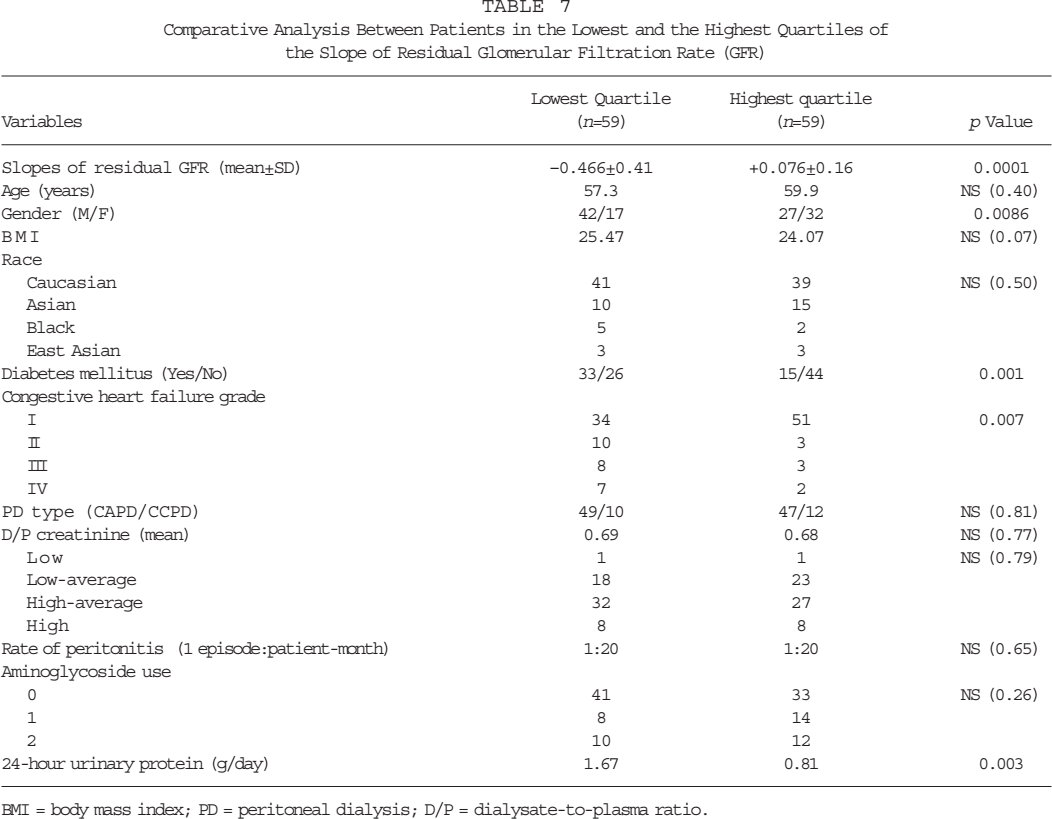
BMI = body mass index; PD = peritoneal dialysis; D/P = dialysate-to-plasma ratio.
Predictors of Decline in Residual GFR: Multivariate Analysis
The stepwise option within linear regression analysis for selection of continuous variables revealed a significant association between residual GFR and volume of dialysate used per day, BMI, high density lipoprotein cholesterol, serum urea, rate of peritonitis, serum calcium, and D/P creatinine. Patients with a larger volume of dialysate, higher rate of peritonitis, and low D/P creatinine had a higher rate of decline of residual GFR. Incorporating selected continuous variables together with chosen categorical variables into a general linear model revealed a significant association of the slope of residual GFR with volume of dialysate, rate of peritonitis, use of AG, presence of DM, higher BMI, and no use of BP medications (Table 8). Other variables that remained in the model but did not achieve the p value of less than 0.05 were nPNA, short-term HD, serum calcium, black race, use of radiocontrast agents, and gender of the patient. The type of PD (CAPD vs CCPD/NIPD) was significantly associated only when volume of dialysate was not included in the model.
General Linear Model for the Selection of Best Predictors for the Slope of Residual Glomerular Filtration Rate (GFR) Incorporating Continuous and Categorical Variables Together
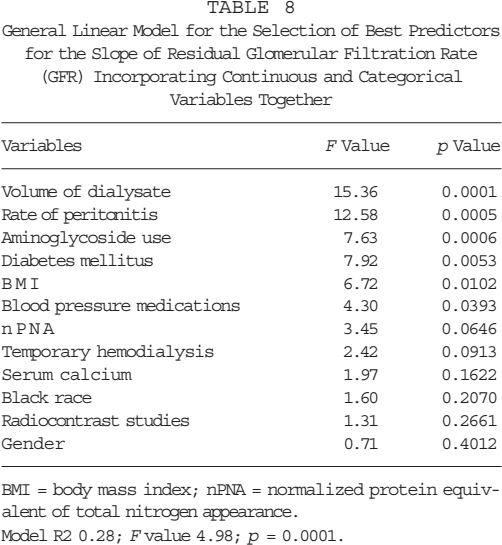
BMI = body mass index; nPNA = normalized protein equivalent of total nitrogen appearance. Model R2 0.28; F value 4.98; p = 0.0001.
Discussion
Our data suggest that there was a gradual deterioration of residual GFR with time on PD, with 33% of patients developing anuria at a mean of 20 months after the start of dialysis. On comparison between patients in the highest and lowest quartiles of slope for residual GFR, male gender, presence of DM, higher grades of LV dysfunction, and higher 24-hour urine protein excretion corresponded with faster decline of residual GFR. On multivariate analysis, use of larger volume of dialysate, higher rate of peritonitis, higher use of AG, presence of diabetes, large BMI, and no use of antihypertensive medications independently predicted the steep slope of residual GFR.
Despite a wide individual variation, the rate of decline of residual GFR in our study was comparable to that previously reported in the literature. Our data did not show a good correlation between the decline of urine volume and renal GFR. Urine volume was well maintained until 30 months after start of PD. This was in contrast to previous studies, where the decline in CCr and urine volume in individual patients was significantly correlated (29). A number of studies have shown that RRF is better preserved in PD patients than in those on HD. However, all these comparisons were made between HD using conventional bioincompatible membranes and CAPD. The advent of newer dialytic techniques such as automated PD and biocompatible HD membranes may alter this relationship. It has also been suggested that PD patients with rapidly falling RRF depart from therapy at a high rate, leaving those with better preservation of RRF on PD after many months (30). This process of informative censoring could make the decline of RRF on PD appear slower. In the present study, 111 patients continued on PD until the end of the study, and 94 patients either died or switched to HD during follow-up. The decline of RRF in patients who continued PD (–0.14 ± 0.20) was not significantly different from those who died or switched to HD (–0.18 ± 0.38, t-test p = 0.47).
Previous studies have not clearly defined the factors that affect the rate of RRF loss in patients on dialysis. In HD patients, Iest et al. reported that the mean rate of decline of RRF was unaffected by weight, gender, age, hypertension status or medications, and by the original disease (31). Lutes et al. also reported (in 32 PD patients) no influence of age, diabetes, mean arterial pressure, peritonitis rate, and initial creatinine clearance at the start of PD, on the rate of RRF loss (23). Davies et al. looked at the half-life of loss of RRF in 303 patients started on PD between 1990 and 1997 (32). Patients with interstitial nephritis, renovascular disease and hypertensive nephrosclerosis had slower decline of RRF. Comorbid conditions did not influence rate of loss of RRF. Moist et al. used the Wave 2 database of the United States Renal Data System (USRDS) dialysis morbidity and mortality study to find predictors of loss of RRF in new dialysis patients (33). Increasing age, female gender, and nonwhite race predicted faster loss, whereas PD and use of ACE inhibitors and calcium channel blockers was associated with slower loss of RRF. However, the primary outcome variable was urine volume, not residual GFR, in this study.
In the present study, we evaluated the risk factors assumed to be associated with residual GFR using univariate and multivariate analysis. There was no effect of age, race, or primary renal disease on the rate of decline of residual GFR. Although there was a faster decline in black patients (–0.24 ± 0.38; n = 22) compared to that in nonblack patients (–0.14 ± 0.29; n = 220), the difference was not statistically significant (p = 0.23). Presence of DM as a cause of renal disease or as a comorbidity was significantly associated with the rate of decline in multivariate analysis. Presence of PVD and higher degrees of LV dysfunction on echocardiography had a significant effect in patients in upper and lower quartiles of slope of residual GFR, but were not significant on multivariate analysis. This could be because of clustering of comorbidity, for example, coexistence of DM, LV dysfunction, and PVD in many patients. Of 105 patients with DM, 38% had PVD and LV dysfunction of grades I to IV in 60%, 13%, 15%, and 12% of patients respectively; compared to 137 patients with no DM where 12% had PVD and LV dysfunction of grades I to IV in 77%, 13%, 7%, and 3% respectively. Similarly, 24-hour urinary protein excretion may also be associated with diabetic nephropathy as a cause of ESRD, hence not significant on multivariate analysis.
Automated PD, being an intermittent therapy akin to HD, may impinge on the beneficial effect of PD on RRF (24,25). However, in a large number of patients, Mujais et al. reported no negative effect of automated PD with overall similar rate of decline and when stratified according to the initial RRF (34). In our study, the type of dialysis (CAPD vs CCPD/NIPD) had significant association only when volume of dialysate used per day was not included in the model. Because the patients on CCPD/NIPD used a higher volume of dialysate, there may be an interaction between these two variables, so that type of PD became insignificant when the volume of dialysate used per day was included in the model. It may also be possible that, in patients with rapidly falling residual GFR, larger volumes of dialysate were prescribed to compensate for rapidly falling residual GFR.
Rate of peritonitis and use of AG have been shown to affect the loss of RRF in two other studies (26,27). Higher rates of peritonitis and higher use of AG antibiotics were independently associated with the steep slope of residual GFR in the present study. A cutoff point of 5 days was used for AG based on the fact that nephrotoxicity of AG is related to the cumulative dose. Aminoglycoside along with first generation cephalosporins is the initial empirical therapy for peritonitis at our center. Aminoglycoside is used for an extended period only if gram-negative bacteria are isolated on Gram stain or culture of PD fluid, which usually takes 3 to 4 days from the onset of peritonitis. Aminoglycoside in our peritonitis therapy is used as a single daily dose, which has been reported to be less nephrotoxic than multiple daily doses (35,36). It is possible that the rate of RRF decline may be even faster with multiple daily doses of AG. The plausible mechanisms by which higher rates of peritonitis can lead to rapid loss of residual GFR remain conjectural. This may be related to the nephrotoxic effect of cytokines released into the systemic circulation by mesothelial cells, fibroblasts and peritoneal macrophages during peritoneal inflammation. Another possible mechanism could be a temporary ultrafiltration failure and extracellular fluid volume expansion during peritonitis, leading to elevation of systemic BP, which could have a deleterious effect on remnant nephrons. There was no effect of temporary HD and number of radiocontrast studies on the rate of decline of residual GFR in the present study.
There was no significant association between the level of BP and the rate of decline of residual GFR; however, patients who were not on any medication for BP control (n = 58) had faster decline of residual GFR (–0.17 ± 0.42) compared to those who were taking medication for BP control (–0.14 ± 0.24, p = 0.62). It may be possible that the patients not on BP medications had slightly higher BP, which may affect remnant nephrons. On the other hand, these patients may have low systemic BP secondary to coexistent LV dysfunction or autonomic dysfunction leading to low renal perfusion pressure and ischemic effects on the kidneys. In the present study, the mean arterial pressure in 58 patients not on BP medications was 92 ± 10.5 mmHg compared to 101 ± 9.4 mmHg in 184 patients taking BP medications. Whether the use of ACE inhibitors can slow the decline of residual GFR once patients have started dialysis is not clear. Although the rate of decline was slower in 90 patients who were on ACE inhibitors (–0.14 ± 0.22) compared to those not on ACE inhibitors (–0.16 ± 0.33, n = 152), the difference was not statistically significant (p = 0.59). The use of antilipemic therapy or erythropoeitin had no effect on the rate of decline of residual GFR.
Chronic administration of high dosages of furosemide is used by some centers to increase urine volume in CAPD patients. Whether this helps preserve residual GFR remains speculative (37,38). In the present study, use of long-term diuretics did not have any effect on the rate of decline of residual GFR.
In conclusion, our data suggest that RRF contributes significantly to total solute clearance and fluid balance in patients on continuous PD. Changes in RRF with time are not uniform in all patients. Faster decline of residual GFR corresponds with male gender, large BMI, presence of diabetes mellitus, higher grades of congestive heart failure and higher 24-hour proteinuria. Higher rates of peritonitis and use of AG for the treatment of peritonitis are also associated independently with faster decline of residual GFR. Whether the type of PD (CAPD vs CCPD/ NIPD) and use of larger dialysate volume are associated with faster decline of residual GFR remains speculative.
Footnotes
Acknowledgments
We greatly acknowledge the help of our nursing and dietitian staff, who looked after these patients and helped in collection of this data. We also acknowledge the help of Sandra Medeiros, who helped in the preparation of this manuscript.