
Abstract
Thirty-six patients on peritoneal dialysis (PD) for more than ten years in six North American centers were analyzed retrospectively. In the six centers, the percentage of patients surviving for more than ten years varied between 0.8% and 7.3%. The study group included 27 females and 9 males aged 38.6 ± 14.2 years [mean ± standard deviation (SD)] at the start of treatment. Of the 36 patients, 28 were Caucasian.
The most common cause of end-stage renal disease (ESRD), present in 12 patients, was chronic glomerulonephritis. Only 4 patients had diabetes. At the beginning of the study, 19 patients had hypertension (the most common comorbid condition); 11 had no comorbid conditions at the start.
Creatinine clearance at the start was 4.12 ± 3.5 mL per minute, and the mean duration to anuria was 51 ± 25 months. Mean initial body weight was 55 ± 9 kg, and mean body surface area was 1.5 ± 0.2 m2. Serum albumin levels showed an increase from 33.8 ± 3.6 g/L at the start of the study to 38.2 ± 3.9 g/L at the end.
Hospitalization rate was low at 0.5 ± 0.3 admissions per patient–year, and duration of hospitalization was 4.8 ± 3.7 days per patient–year. Peritonitis was the most common cause of hospitalization. The mean peritonitis rate was 1 episode every 52 ± 48 patient–months.
There were 36 catheter changes in 18 patients; 16 patients had a single PD catheter throughout the period of study. Autonomous hyperparathyroidism was the most common long-term complication.
At the end of the study period, 11 patients were still on PD, 9 had died, 5 had been transferred to hemodialysis (HD), 1 was alive with a functioning allograft, and 1 was lost to follow-up.
We conclude that patients who survive longer than ten years on PD are most likely to be young Caucasian females, small in body size, who are non diabetic, with few comorbid conditions. These long-term survivors have few hospitalizations, and their peritonitis rate is low. In this group of patients, severe autonomous hyperparathyroidism is the most common long-term complication.
In a recent international review of patients who had been on CAPD or automated PD (APD) for more than eight years, the prevalence of such patients was between 0.4% and 4.8% (2). The main reason for the low prevalence was a high failure rate owing to peritonitis, ultrafiltration (UF) failure, access problems, and patient or family fatigue.
This paper describes a group of 36 patients who have been on CAPD or APD for ten years or more at six North American centers. We sought to identify the characteristics of these patients that may have contributed to their long-term survival on CAPD and APD.
Patients and Methods
A questionnaire was sent to eight North American centers with long-term experience. Five of them responded (Table 1). The participating centers were asked to state
Participating Centers and Prevalence of Long-Term Peritoneal Dialysis Patients
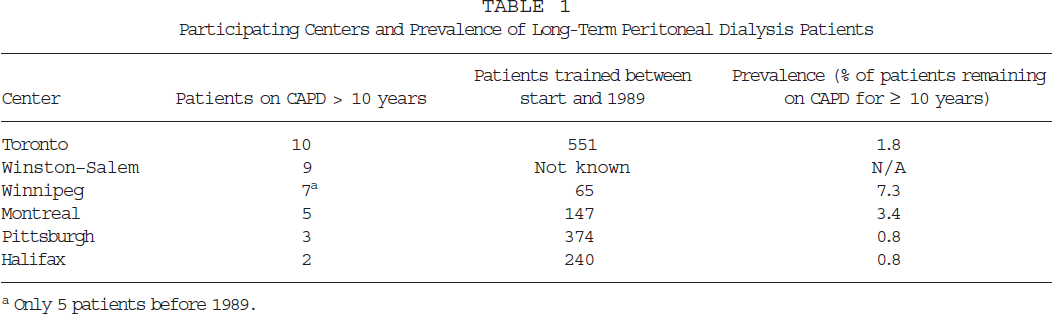
Only 5 patients before 1989.
the total number of patients trained from the beginning of the center's CAPD/APD program to the end of 1989, and
the number of patients who had been on PD for ten years or more.
The information obtained about each patient included sex, race, age at start of dialysis, date of onset of PD, underlying renal disease, major comorbid conditions at the start of PD, initial residual renal function, dialysate-to-plasma (D/P) creatinine, duration of PD, cause and duration of hospitalizations, and number of peritonitis episodes. This information was available in most, but not all, patients.
Experience at the Toronto Western Hospital
Of a total of 551 PD patients, 10 were on CAPD or APD for more than ten years. In addition to the data obtained from the participating centers outside Toronto, we undertook a detailed evaluation of these patients’ various clinical and biochemical markers. The markers studied included: PD regimen at the start and end of the follow-up, weekly Kt/V and weekly creatinine clearance (WCC) whenever available, the reason for not undergoing renal transplantation over the ten years, the nature of family support available, various anthropometric parameters such as height and weight [body mass index (BMI) and body surface area (BSA)] at the start and end of the follow-up; and the average supine blood pressure (BP) at start and at the last two visits, together with the number of antihypertensive medications at the start and at the end of follow-up.
We recorded single hematological and biochemical parameters such as hemoglobin (Hb) and hematocrit (Hct), blood urea, serum creatinine, serum albumin, serum cholesterol, low-density lipoprotein (LDL), serum triglycerides, serum calcium (Ca), and serum phosphate (PO4) at the start, at five years, and at the end of the study. Finally, we looked at the long-term complications in each of these patients. Detailed data for the 10 Toronto Western Hospital (TWH) patients will be presented with the data from the participating centers.
Results
Our study found 36 patients were on CAPD or APD for ten years or more. The percentage of patients surviving on long-term CAPD or APD (Table 1) varied between 0.8% and 7.3%.
Age, Sex, Race
The mean age at onset of APD was 38.6 ± 14.2 years (median: 37 years; range: 1 – 63 years). Of the 36 patients, 27 were female, and 9 were male. The racial origins were Caucasian, 28 patients; African-American, 4 patients; Asian, 3 patients; and Native American, 1 patient.
Anthropometric Data
Anthropometric data was available only for the TWH patients (n = 10).
Mean weight was 54.7 ± 9 kg (median: 55.6 kg; range: 42 – 70 kg). Mean height was 160.1 ± 11.2 cm (median: 156 cm; range: 145 – 180 cm); mean BSA, 1.55 ± 0.18 m2 (median: 1.53 m2; range: 1.29 – 1.88 m2); and mean BMI, 21.3 ± 2.2 kg/m2 (median: 21.4 kg/m 2; range: 17.6 – 24.8 kg/m2).
Underlying Disease
Chronic glomerulonephritis was the most common cause of end-stage renal disease (ESRD) in this population, occurring in 12 of the 36 patients. Hypertensive nephrosclerosis was the cause in 5 patients. Four patients had diabetic nephropathy, 2 of whom had type 1 diabetes. Reflux nephropathy, chronic pyelonephritis, hypoplastic kidney, and amyloidosis were present in 2 patients each. Miscellaneous causes were present in 7 patients.
Comorbid Conditions at the Beginning of Treatment
At the start of PD, the most prevalent comorbid condition was hypertension, present in 19 of the 36 patients. Eleven patients had no comorbid conditions. Severe peripheral vascular disease was present in 2 diabetic patients. Only 1 patient had documented coronary artery disease at the start. Only 3 patients were chronic smokers. Two patients had amyloidosis, and 1 patient each had subaortic stenosis, mental retardation, and renal osteodystrophy.
Blood Pressure Control
Initial mean supine BP in the TWH patients (n = 10) was 136/80 mmHg; the final BP (average of BP recordings in the last two visits) was 141/80 mmHg. Of the 10 patients, 6 did not initially require antihypertensive medication. One patient was on two antihypertensives, and 2 patients were on more than two. At the end of the follow-up period, only 2 patients did not require an antihypertensive agent; 4 patients needed one antihypertensive, and 4 needed two or more.
Initial Residual Renal Function
Data on residual renal function at the start of CAPD was available for only 15 patients. Four patients were anuric at the start of dialysis. Among the remaining 11 patients, mean creatinine clearance was 4.12 ± 3.46 mL per minute (median: 5 mL per minute; range: 0.5 – 10 mL per minute). The onset of anuria after start of PD was calculated in 9 of these 11 patients. Mean duration to anuria was 51 ± 25.2 months (median: 57 months; range 16 – 94 months).
Peritoneal Permeability
The D/P creatinine (D/PCr) at the start of PD was available in only 5 TWH patients. Mean D/PCr was 0.72 ± 0.07 (median: 0.7; range: 0.6 – 0.8).
Biochemical and Hematological Data
Biochemical and hematological data, which were available only for the TWH patients (n = 10), are shown in Table 2. Mean hemoglobin levels rose. However 6 patients were on erythropoietin (EPO) by the end of the study period. Mean blood urea nitrogen (BUN) showed a persistent fall. A similar trend occurred in serum creatinine levels. Serum total protein and serum albumin levels, which showed an upward trend during the study, were accompanied by an increase in mean body weight.
Biochemical and Hematological Changes During Long-Term Continuous Ambulatory Peritoneal Dialysis at the Toronto Western Hospital (n = 10)
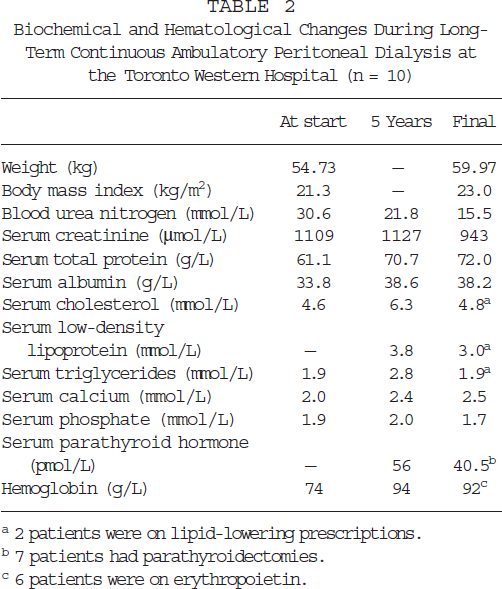
2 patients were on lipid-lowering prescriptions.
7 patients had parathyroidectomies.
6 patients were on erythropoietin.
Mean serum calcium levels rose, and mean serum phosphate levels fell. These trends were accompanied by lower mean values of serum parathyroid hormone (PTH) at the end of the study. However, of the 10 patients, 7 had a parathyroidectomy during the ten-year period.
Serum cholesterol levels rose at five years, but fell at the end of the study. The LDL and serum triglycerides also showed a downward trend at ten years compared to the values at five years. Only 2 of the 10 patients were on lipid-lowering drugs.
Causes for and Duration of Hospitalization
Hospitalization data were available for 33 of the 36 patients. Two patients needed no hospitalization during the entire ten years. The mean number of hospital admissions per patient–year was 0.5 ± 0.3, The mean duration of hospital days per patient–year was 4.8 ± 3.7 days.
Peritonitis was the most common reason for hospital admission. Other major causes were parathyroidectomy, various other surgeries, PD catheter replacement, various investigative procedures, and pulmonary edema (Table 3).
Major Causes for Hospitalization (n = 31 a )
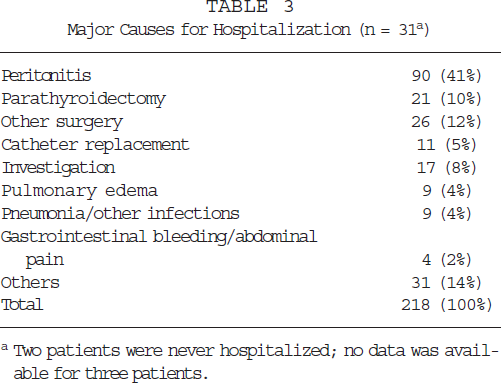
Two patients were never hospitalized; no data was available for three patients.
Peritonitis Rates
Out of 36 patients, 3 patients had no episodes of peritonitis during the ten years of the study; no data on peritonitis was available for 1 patient. The mean peritonitis rate among the remaining 32 patients was 1 episode every 52 ± 48 patient–months (median: 26 patient–months; range: 13.3 – 177 patient–months).
Pd Catheter Changes
Sixteen of the 36 patients had a single PD catheter during the entire period. Thirty-six catheter changes were performed in 18 patients; 3 of the changes were not associated with infection.
Family Structure
Data from the TWH patients (n = 10) shows that all had active family support and participation in the dialysis process. Five of the 10 patients lived with spouse and children, 4 lived with spouse only, and 1 patient lived with parents.
Why Were They Not Transplanted?
Four of the 10 TWH patients refused transplantation; another 4 had previously undergone transplant rejection and were not able to undergo another transplantation. In 1 patient each, we considered that transplantation was contraindicated because of age and multi-system amyloidosis.
Long-Term Complications
The most common complication—found in 21 of 31 patients—was autonomous hyperparathyroidism requiring parathyroidectomy. Among the 10 TWH patients, UF failure developed in 3 patients. In 2 of these patients, UF failure was due to sclerosing encapsulating peritonitis; in 1, to a retroperitoneal leak. Amyloid bone disease was detected in 1 patient.
Duration of CAPD and Final Outcome
Mean duration of CAPD or APD (n = 35) was 12.4 ± 2.4 years (median: 11.8 years; range: 10 – 21 years). Final outcome data was available in only 26 patients. Eleven patients were still on CAPD or APD at the end of the study period; 9 patients had died; 5 were transferred to hemodialysis (HD); 1 patient underwent transplantation; and 1 patient was lost to follow-up.
Discussion
It is important to remember that statistics on patients and technique survival (2-5) do not reflect the number of patients remaining on a treatment after a certain period of time. The reason is that, in calculating patient survival, only death is the end event; transplantation, transfer to another treatment, recovery of kidney function, or transfer to another center are censored events (lost to follow-up). Similarly, in calculating technique survival, the end event is transfer to HD; death, transplantation, recovery of kidney function, and transfer to another center are censored events. For these reasons, the percentage of patients remaining on a treatment is much lower than that calculated from actuarial patient or technique survival.
In Italy, just 3% of patients remained on PD for more than eight years (2). In Canada, among 45 – 64-year-old non diabetic PD patients, the percentage on PD at seven years was 2.2% (69 / 3130) (6). Similarly, data from Australia and the U.K. show that only 0.4% and 1.4% of patients, respectively, remain on PD more than eight years (2). The Japanese have reported 15% survival of patients on PD at eight years, but it is important to note that this nation has a very low transplantation rate (2).
In this study, the percentage of patients on PD longer than ten years varied between 0.8% and 7.3% among participating centers (Table 1). In a similar study of 9 patients on CAPD for more than ten years, De Vecchi et al found that these 9 made up 7.8% of the total (7). In a study of 20 long-term PD patients by Abdel–Rahman et al, 7 patients who had type 1 diabetes were among those who survived for more than 100 months. These type 1 diabetic patients represented 12% of the survivors overall and 16% of all patients with type 1 diabetes. It is interesting to note that none of the 24 patients with type 2 diabetes survived for more than 100 months (8). This survival rate for type 1 diabetic patients is higher than that reported in this paper and those reported by De Vecchi and colleagues, but it should be noted that it refers to survival of 100 months (just over eight years). After eight years of PD, it is possible that a significant number of patients die or experience complications requiring a changeover to HD.
The long-term survivors in this study were much younger at the start of dialysis (mean age 38.6 years) compared to the average age of 55 years and 57.6 years for incident dialysis patients in 1989 in Canada and the U.S.A. respectively (9,10). The patients of Abdel–Rahman et al, who survived past 100 months, also were young (41.6 years), but those in De Vecchi's study had a mean age of 50.8 years.
In this study, 27 of the 36 patients (75%) were females. The usual male-to-female ratio in the United States for incident ESRD patients was 55:45 in the years 1986–1989 (10). Females are said to have a better long-term survival on PD (2). However, of the 9 patients on long-term PD reported by De Vecchi et al, 6 were males. Abdel–Rahman et al had an equal number of males and females in their long-term survivor group of 20 patients (7,8).
Of the 36 patients in this study, 28 were Caucasian. This finding contradicts a recent study showing that African-Americans do better than Caucasians on PD (11). It is interesting that in Abdel–Rahman's study, all 20 long-term survivors were Caucasian.
Good family support is associated with good clinical outcomes in PD (12). None of the 10 TWH patients lived alone; all had supportive families who actively participated in the dialysis process.
In this study, diabetic nephropathy was the cause of ESRD in only 4 of 36 patients (11.1%). This incidence is much less than the 21% reported in the Canadian registry for diabetic patients within the dialysis population in 1989 (13) and the 33% reported in the United States Renal Data System (USRDS, 10). Our result supports the view that the overall prognosis for diabetic patients is worse than that for non diabetic patients. None of De Vecchi's long-term PD survivors (> 10 years) had diabetes at the start of dialysis. However, in Abdel–Rahman's study, 16% of those who survived past 100 months had type 1 diabetes, while none of the 24 patients with type 2 diabetes survived for this period (8).
The most common cause of ESRD in our patients was chronic glomerulonephritis; the second most frequent cause was hypertensive nephrosclerosis. De Vecchi's study showed a pattern similar to ours, in that the most common cause of renal failure in his patients was hypertensive nephrosclerosis; it was present in 3 of the 9 patients (33%). In Abdel–Rahman's study, however, the most common cause of ESRD was type 1 diabetes (7 of 20 patients) (7,8).
The presence of comorbid conditions at the start of PD has an adverse influence on long-term outcome (12,14). Comorbid conditions also have an additive effect. Eleven of 36 patients in our study had no comorbid conditions at the start of dialysis. Hypertension was the most prevalent comorbid condition, being present in 19 of 36 patients; it was well controlled among the TWH patients (mean BP 136/ 80 mmHg). None of the patients had malignant hypertension at the start of the study. In the study by De Vecchi et al, all of the 9 patients who survived more than ten years were hypertensive at the start. Three patients had ischemic cardiomyopathy, and 1 each had peripheral vascular disease and cirrhosis (7). In Abdel–Rahman's study, 7 patients among the 20 long-term survivors had diabetes, 8 were smokers, 4 had cardiac disease, and 1 patient had peripheral vascular disease (8). Thus, in most of the studies, including the this one, the patients have a small number of comorbid conditions at the start of PD.
With respect to body size, the TWH patients were smaller than the general population—a finding that is in agreement with the reported characteristics of long-term survivors on PD (12) and that supports the role of adequate dialysis in long-term survival. Similarly, Abdel–Rahman's patients had mean body weight of 62.5 kg—a weight that was much lower than that of the short-term survivors (8).
Data about residual renal function was available in 15 of 36 patients. Mean creatinine clearance at the start of dialysis was only 4.12 mL per minute; 4 patients were anuric from the start. In De Vecchi's study, creatinine clearance at the start ranged from 0.5 – 4.7 mL per minute. These findings contradict those of the CANUSA study, which suggests that patients with higher residual renal function are likely to survive on PD for longer durations (15).
Nine of the 10 TWH patients became anuric about 51 months after the start of PD. This decline in renal function is slower than in the overall PD patient population of TWH, whose mean time to anuria was only 20.7 months (16). De Vecchi et al also noticed a slower rate of decline to anuria in his patients. Of his patients, 66% were observed to have residual renal function after three years, 33% after five years, and 11% after ten years (7).
The standard PD schedule for the TWH patients (n = 10) was four 2-L exchanges per day. Over the ten-year period, 4 patients needed an adjustment in dialysis “dose”: 3 patients needed 5 exchanges per day to achieve more-adequate dialysis, and 1 needed a change to nightly intermittent peritoneal dialysis (NIPD) for convenience. De Vecchi's patients also performed 4 – 5 exchanges of 2 L each. It is possible that our patients, because of their smaller body size, achieved adequate dialysis with four 2-L exchanges per day, despite their low residual renal function.
It has been reported that “high transporters” have poor long-term survival on PD (17). The mean D/PCr in 5 of the TWH patients was 0.72 ± 0.07. This data suggests that not all high transporters have a poor prognosis; however, the number of patients in our study is too small to permit a definite opinion.
In the TWH patients (n = 10), serum albumin levels rose from 33.8 g/L at the start to 38.6 g/L at five years; this level was maintained at the end of the study. Total protein levels followed a similar trend. In addition, body weights and body mass indices had both increased at the end of the study. While these data support the view that good nutrition is a prerequisite to good long-term outcome, BUN levels fell from an initial value of 31 mmol/L at the start to 22 mmol/L at five years, and to 15 mmol/L at the end, indicating a lower protein intake. De Vecchi found that serum albumin and serum creatinine were maintained at initial levels; Abdel–Rahman did not find any significant difference between initial serum albumin levels of the long-term and short-term survivors (7,8).
As noted by De Vecchi, patients who survived a long time on PD showed no significant change in their lipid profiles over time. At the end of Abdel–Rahman's study, serum cholesterol levels were marginally higher than before dialysis. Similarly, our TWH patients showed no significant change in lipids.
In the full patient group under study (n = 36), 1 episode of peritonitis occurred every 52 months, a rate that is much lower than the usual peritonitis rate (12). Three of the 36 patients had no episodes of peritonitis. The patients in De Vecchi's study also had a low rate of peritonitis: 1 episode every 57 months, close to our finding. In Abdel–Rahman's study, the long-term survivors had significantly fewer episodes of peritonitis than the short-term survivors. These observations emphasize the importance of a low peritonitis rate to the success of long-term PD. Nevertheless, peritonitis was the most common cause of hospitalization, indicating that, although peritonitis rates are low in long-term PD patients, peritonitis is still an important problem.
The hospitalization rate in our patients were much lower than the usual hospitalization rate in the PD population. In fact, 2 patients never needed hospital care. Our reported rates are much lower than those reported in a recent study, and they reflect the low complication rate in the patients (18). Both De Vecchi and Abdel–Rahman reported similar experiences of low hospitalization in their patients (7,8).
In regard to long-term complications in patients on long-term PD, 21 of 30 patients in the present study developed autonomous hyperparathyroidism requiring parathyroidectomy. Similarly, in De Vecchi's study, 6 of 9 patients had severe hyperparathyroidism. Hyperphosphatemia or prolonged use of “low calcium” dialysis solutions probably precipitated the hyperparathyroidism. Other complications seen in the TWH long-term patients included sclerosing encapsulating peritonitis (SEP), ultrafiltration failure, and amyloidosis.
Conclusions
An analysis of 36 patients from six North American centers shows that those patients most likely to survive on PD for more than ten years are relatively young at the start of dialysis, do not have diabetes, and have few or no comorbid conditions. The patients are predominantly females with a low body weight and small BSA, are well nourished, and have good family support. They also have low rates of hospital admission and peritonitis. Severe autonomous hyperparathyroidism, which was present in the majority of the studied patients, seems to be the most frequent complication among long-term survivors.
A high initial residual renal function was not essential to long-term survival, and some high transporters did quite well.
Footnotes
Acknowledgments
We would like to thanks Ms. Maggie Chu for her help in collecting the TWH data, Ms. Joan Tomkins for helping to collect data at the Victoria General Hospital in Halifax, and the nurses of the various PD programs for the excellent care of their patients. We would like also to thank Ms. Sandra Medeiros for her excellent secretarial help.