
Abstract
The basis for hyponatremia is a negative balance for sodium (Na+) plus potassium (K+) and/or a positive balance for water. In patients with normal renal function, vasopressin is needed to prevent the excretion of electrolyte-free water. Vasopressin is not important when there is little residual renal function. If hyponatremia is accompanied by a quantitatively appropriate gain in weight, this implies that a gain of electrolyte-free water was the basis for hyponatremia. In the absence of this weight gain, a loss of salts is to be suspected. If the extracellular fluid (ECF) volume is obviously low, hyponatremia is due to a deficit of NaCl, unless there is a deficit of K+. With a KCl deficit and a contracted ECF volume, there should also be a large shift of Na+ into cells, so metabolic alkalosis would not be an expected finding. In contrast, those patients with no change in weight who have a normal or expanded ECF volume are subdivided into those with a gain of solutes restricted to the ECF compartment (glucose, mannitol), or those with a deficit of solutes of intracellular fluid origin, which implies that a catabolic state (malnutrition) may be present.
The clinical approach to understanding why hyponatremia develops in a given patient has a strong physiological underpinning [see Eq. (1)] (5-10).

It is rare to have only a single reason to explain the basis of hyponatremia, especially in patients undergoing peritoneal dialysis. Nevertheless, for descriptive purposes we shall define the expected basis for hyponatremia as if it had a single cause.
This review will be divided into two parts. In the first, we outline the approach we use in a patient with hyponatremia (Table 1 and Figure 2). This approach is also useful for patients on continuous ambulatory peritoneal dialysis (CAPD). In the second section, we address a quantitative inconsistency in the approach outlined by Edelman and Leibman (11) [Eq. (1)].
Questions to Answer to Determine Why Hyponatremia Is Present
ECF = extracellular fluid.
Hyponatremia: Emphasis on its Pathophysiology
Water Gain as the Only Cause of Hyponatremia
A positive balance for electrolyte-free water (EFW) can cause hyponatremia (8). Electrolyte-free water is retained because vasopressin increases the permeability of the distal nephron to water and thereby prevents EFW excretion (12). In patients without residual renal function, there is no role for vasopressin in the development of hyponatremia. A weight gain is the clinical hallmark of a positive EFW balance (Figure 1). Nevertheless, extreme measures are required to obtain accurate weights in clinical practice [see Ref. (13)]. A quantitative analysis is also essential. Water accounts for close to 60% of body weight in a nonobese adult (14). Therefore, there are close to 40 L of water in a 70-kg person. If the plasma Na+ concentration declines by 10% due solely to a gain of EFW, total body water should rise by close to 10%, or 4 L. As a result, body weight should rise by 4 kg. There is a further adaptation. In most patients, Na+ is excreted to reduce the expanded ECF volume back toward its normal value. Hence the weight gain will ultimately reflect a gain of water only in the ICF compartment (60% – 67% of 4 kg, or close to 2.4 kg). Such a large weight change should be readily detected.
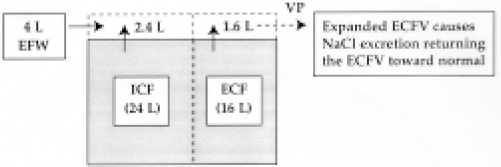
Hyponatremia and weight gain. The shaded central rectangle represents the body. The bold, dashed vertical line separates the intracellular fluid (ICF) (to its left) and extracellular fluid (ECF) compartments (to its right); the normal volumes are shown in the clear rectangles within the shaded area. When there is a gain of 4 L of electrolyte-free water (EFW) (shown in the clear rectangle on the left), it is distributed in both the ICF and ECF compartments in proportion to their size. Vasopressin (VP) is needed to prevent the general excretion of EFW. An expanded ECF volume should lead to the excretion of Na+.
In summary, the process begins as a pure water gain and with time the mass balance is converted to a smaller water gain plus a Na+ deficit when the ECF volume returns to normal (Figure 1).
Reduced Number of “Effective Osmoles” as the Cause of Hyponatremia
If hyponatremia is present without an appreciable change in body weight, its cause would be a loss of Na+ and/or K+ salts. We have subdivided this group into two broad categories based on the change in ECF volume (Figure 2).
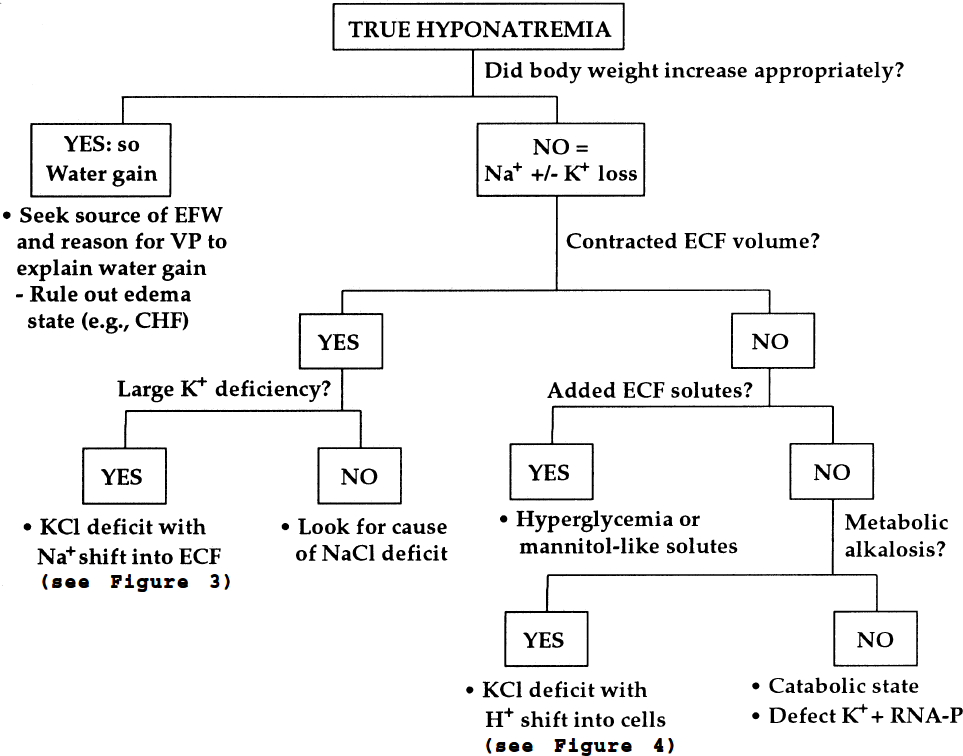
An approach to the patient with hyponatremia is demonstrated in flow-chart fashion. The final diagnosis is shown by statements preceded by a bullet below each terminal rectangle. In all these cases, we assume that there is a single process involved and that vasopressin is acting. EFW = electrolyte-free water; VP = vasopressin; CHF = congestive heart failure; ECF = extracellular fluid; RNA-P= organic phosphates in the intracellular fluid compartment.
Patients with Hyponatremia and a Contracted ECF Volume
Deficit of Na+ Salts: Because Na+ salts are derived virtually solely from the ECF compartment, its osmolality will decline for the briefest moment (Figure 3, left panel). As a result, water will shift from the ECF to the ICF compartment, leading to a decreased ECF volume and swollen cells. This water will not be excreted if vasopressin is present or renal function is absent. In peritoneal dialysis, the patient is usually dialyzed chronically against a bath with a Na+ concentration of 132 mmol/L. The removal of Na+ during CAPD has been studied by Nolph et al. (15). Sodium (and Cl−) was dialyzed away when the plasma Na+ concentration exceeded 132 mmol/L; Na+ was also removed by bulk flow. Mass balance for Na+ will depend as well on Na+ intake.
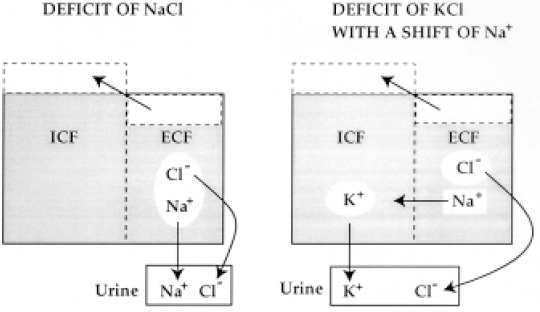
Hyponatremia due to a water shift with a contracted extracellular fluid (ECF) volume. Solutes in white rectangles were retained, whereas those in white ovals were excreted. Vasopressin is present to prevent the excretion of electrolyte-free water (EFW) in both parts of the figure. A deficit of NaCl is illustrated in the left panel. The deficit of NaCl generates EFW, and a portion of this EFW shifts into the intracellular fluid (ICF) compartment to maintain osmotic equilibrium. In the right panel, there is also a deficit of Na+ and Cl− in the ECF compartment, but K+ is excreted and Na+ shifts into the ICF to take its place.
A quantitative example will help to illustrate the magnitude of these changes (see Appendix): In a 70-kg patient who has a Na+ deficit of 400 mmol, the plasma Na+ concentration would fall from 140 to 130 mmol/L. The ECF volume would decline by 1.85 L, and this should be readily detected at the bedside (16). If this patient lost a considerable amount of NaHCO3, all the above findings will be accompanied by metabolic acidosis.
Deficit of K+ Salts: In the patient who has a deficit of KCl and/or KHCO3 along with a significantly contracted ECF volume, the deficit of K+ in the ICF compartment would be replaced by a shift of Na+ from the ECF compartment (Figure 3, right panel). This satisfies the need for electroneutrality in all body compartments. The K+ that shifted out of cells must be excreted to avoid a lethal degree of hyperkalemia. When these K+ are excreted with an anion of ECF origin [Cl− or bicarbonate (HCO3−)], there is a net loss of two solute molecules from the ECF compartment (Cl− and Na+), whereas there is no change in the number of solute molecules in the ICF compartment (gain of Na+ equals the deficit of K+). In quantitative terms, if there is a loss of 400 mmol of KCl, the net changes in compartment volumes and plasma Na+ concentration would be identical to that for a loss of 400 mmol of NaCl (Figure 3, left panel). The only observable difference would be hypokalemia because kaliuresis provided the initial driving force for the overall process. An example of this type of hyponatremia would be the use of a thiazide diuretic in a patient on a low K+, but not low Na+, diet. If an appreciable amount of KHCO3 is also excreted, the patient would have all the above findings for a deficit of KCl, but in addition, metabolic acidosis would be present.
Patients with Hyponatremia who do not Have a Contracted ECF Volume
If there is no change in body weight, the basis for hyponatremia is a water shift. The direction of the water shift will be from the ICF to the ECF compartment (Figure 4). There are two theoretical reasons for having this directional shift of water: a gain of solutes in the ECF compartment, or a loss of solutes from the ICF compartment.
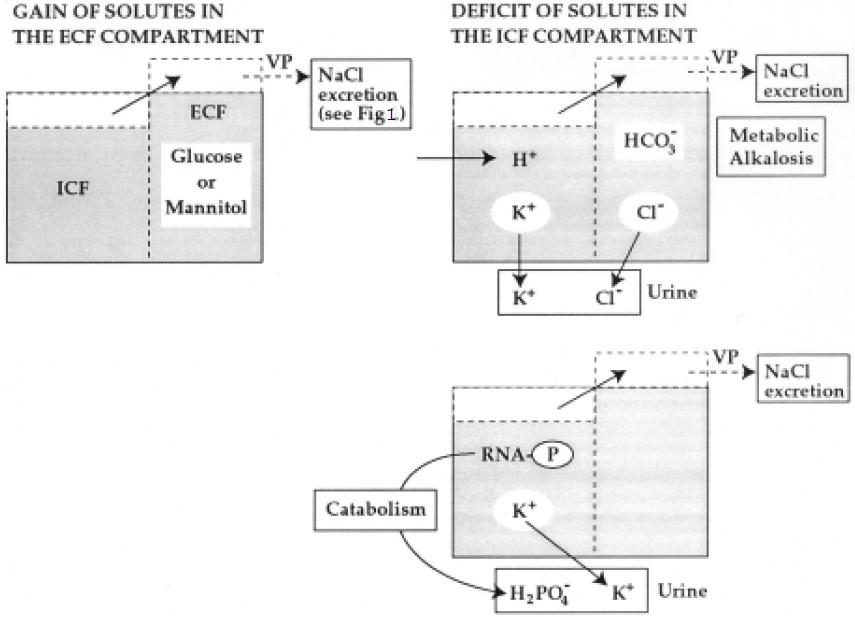
Hyponatremia due to a water shift and an expanded extracellular fluid (ECF) volume. The net gain of hypertonic glucose or mannitol in the ECF caused water to shift from the intracellular fluid (ICF) to the ECF compartment (upper left panel). As shown in the upper right panel, a loss of K+ and Cl− (white ovals) along with a H+ shift into the ICF caused a loss of ICF solutes (K+), a shift of water into the ECF compartment, and metabolic alkalosis in the ECF compartment. The fate of these H+ in the ICF is shown in Figure 5 As shown in the lower right panel, catabolism of macromolecular organic phosphates (RNA-P) led to the excretion of K+ and inorganic phosphate, as well as a shift of water from the ICF to the ECF compartment. Electrolyte-free water was retained in these examples because vasopressin (VP) was present or because there was very poor renal function.
Gain of Solutes Restricted Primarily to the ECF Compartment: The solutes in question are organic molecules with a volume of distribution similar to the ECF compartment (Figure 4, left panel). The commonest solute is glucose [hyperglycemia (17)]. Other examples include the addition of mannitol-like solutes (e.g., after a transurethral resection of the prostate). If these solutes are added in a hypertonic solution (the usual case with cerebral edema), water shifts out of cells. If added as a hypotonic solution (the usual case with a transurethral prostate resection), some EFW enters cells and the ECF compartment is expanded with iso-osmotic organic osmoles solution and, to a minor extent, EFW.
Loss of Solutes from the ICF Compartment: The major solute in the ICF compartment is K+; therefore there are two ways to have a net loss of K+ from the ICF compartment. First, there is a loss of K+ in exchange with H+ from the ECF (Figure 4, upper right panel). These H+ cannot remain as free H+ in the ICF compartment for it to create a deficit of solutes in cells (see KCl deficit below). Second, it is possible to have the loss of K+ plus an intracellular anion (18). These losses of solutes result in a desalination of body fluids (19). The EFW will remain in the body because vasopressin is acting or renal function has been lost. Forty percent of the volume of this EFW will distribute into the ECF compartment. The net result is hyponatremia, an expanded ECF volume, and a contracted ICF volume in those cells that lost solutes. If, for example, these solutes were lost from muscle but not brain cells, muscle cells would shrink and brain cells would swell.
Deficit of KCl with a shift of H+ into cells: To illustrate this setting, consider the “selective loss of HCl” (20). After the postdrainage period, the mass balance is an equimolar deficit of K+ and Cl− rather than a deficit of H+ and Cl−. Moreover, the plasma HCO3− concentration remains equally elevated in both the HCl and KCl depletion phases of metabolic alkalosis. To maintain electroneutrality in the ECF compartment, the deficit of Cl− is matched by a gain of HCO3− (Figure 4, upper right panel). Up to this point, there are two areas where the basis for electroneutrality is not defined: the ICF compartment and urine (both have a K+ content change without an apparent “electrical partner”). The simplest way to achieve electroneutrality in both the cells and urine is to follow the fate of endogenously-produced acids such as H2SO4. Because this subject is Cl− deficient, there is an appreciable delivery of Na+ to the cortical collecting duct with anions other than Cl−. Under the influence of aldosterone, Na+ is reabsorbed but SO42- remains in the lumen. This creates a lumen-negative voltage, so K+ can take the place of Na+ in luminal fluid (21).
With respect to electroneutrality in cells, virtually all the excreted K+ is derived from the ICF compartment. For electroneutrality, the H+ produced with SO42- replace K+ in cells (Figure 4, upper right panel). That this H+ entered cells is reflected by the fact that the degree of elevation of the concentration of HCO3− in the ECF compartment remains constant (20). The fate of H+ in the ICF compartment is to be buffered by HCO3− and/or proteins (22). If the H+ combine with HCO3−, the products are CO2 (exhaled) and water. The net result is the loss of two solutes from the ICF compartment, K+ plus HCO3− (Figure 5, upper panel). On the other hand, H+ can bind to intracellular proteins if the tissue pCO2 does not fall (22). Therefore, these macromolecules will not increase in number, but they will have a larger net positive charge (Figure 5, lower panel). Accordingly, half as much EFW will be formed by desalination with protein buffering because only one solute molecule (K+) is lost in this setting.
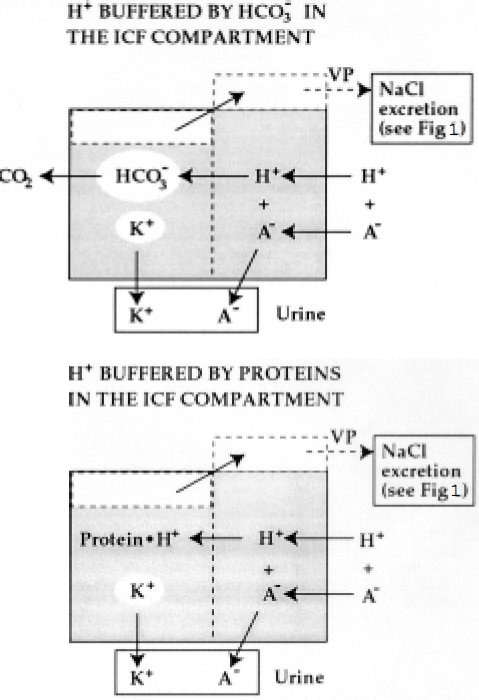
Development of hyponatremia due to a loss of K+ and a gain of H+ in cells. There are two fates for the H+ that entered cells when K+ was excreted. In the upper panel, H+ are buffered by HCO3−, yielding CO2 + H2O; this removes two particles from the intracellular fluid (ICF) compartment when K+ is excreted with the anion (A−) produced along with those H+ (white ovals). In the lower panel, H+ are buffered by intracellular proteins, so there will be a net loss of one ICF particle (K+) when K+ is excreted with the anion (A−) produced with those H+. Twice as much K+ loss is needed in this setting to generate an equivalent volume of electrolyte-free water, which was retained in these examples because vasopressin (VP) was present or because there was very poor renal function.
Loss of K+ plus an anion from the ICF compartment: There are two types of loss of intracellular K+, phosphate and volume from the ICF compartment, each with a different potential influence on the degree of hyponatremia. First, consider a loss of all the ICF constituents of muscle, the major component (50% of body water) of the total ICF compartment. Although there is a major loss of ICF volume with an amputation for example, it will not cause a change in the plasma Na+ concentration. A change in natremia requires a gain of EFW plus a very limited excretion of EFW. The impact of this total cell loss is on the degree of hyponatremia when there is another reason for EFW gain and vasopressin acts. For example, with a 50% loss of ICF volume, total body water that was 42 L in a 70-kg normal person declines to 28 L. If there was a positive balance of 4.2 L of EFW, this could have caused the plasma Na+ concentration to decline to 126 mmol/L before the tissue loss. With the ICF loss, this 4.2-L positive EFW balance will now cause the plasma Na+ concentration to be 119 mmol/L.
The second reason for a lower ICF volume is a loss of intracellular solutes from otherwise intact cells. With respect to solute loss and a water shift, one must lose intracellular electrolytes. The anion that is central to this discussion is intracellular organic phosphates that exist inside cells primarily in a macromolecular form, as DNA, RNA, or phospholipids (Figure 4, lower right panel) (9). Of these, the major form that undergoes catabolism when considering more than 100 mmol of this type of K+ deficit is RNA. RNA catabolism occurs with insulin lack (23). This loss, however, is a net loss of only 1 mOsm/mmol K+ excreted. Nevertheless, there would be no weight loss initially (a shift of water would occur from the ICF to the ECF compartment due to the generation of EFW in the ICF and an intact cell membrane) if there is no renal EFW loss. In patients on peritoneal dialysis who lack sufficient renal function, there is no need for vasopressin. In summary, there would be an increase in the ECF volume and an overall contraction of the ICF compartment to maintain osmotic equilibrium. There would be no appreciable change in body weight unless a negative balance of water was created by dialysis.
Critique of Edelman's Analysis
In Eq. (1), the presumption is made that the anions that accompany Na+ and/or K+ in the body are monovalent and hence have the same impact on plasma Na+ concentration. While the anions in the ECF compartment are largely monovalent, the anions of intracellular origin are predominantly macromolecular in nature. Therefore, when K+ is excreted with inorganic phosphate derived from catabolism of ICF macromolecules, this loss of K+ is not equivalent to a loss of Na+ in terms of causing an identical deficit of “effective osmoles” in the body (Figures 3, 4, and 5). Hence, the resulting quantitative decline in plasma Na+ concentration and in the volumes of body fluid compartments will not be identical when there is a deficit of Na+ compared to K+ salts. Accordingly, if the loss of endogenous K+ occurred with inorganic phosphate (Figure 4) or in conjunction with H+ entry into cells that were buffered on proteins (Figure 5), there would have to be a twofold greater deficit of K+ to generate the same volume of EFW. Hence it is not correct to equate the loss of Na+ + K+ with its influence on the “effective osmolality” of the body and the change in natremia, as was done in Eq. (1).
Concluding Remarks
Three major steps are taken to deduce why hyponatremia developed (Figure 2). The changes are based on single causes for this electrolyte disorder. First, if the degree of hyponatremia is quantitatively appropriate to the rise in body weight, its basis is an EFW gain. Second, if hyponatremia is present but there is no change in body weight, its basis is a change in the number of “effective osmoles.” At this point, causes are divided into two groups based on changes in the ECF volume. If the ECF volume is contracted, the next step is to assess the K+ status. Without K+ depletion (hypokalemia), one is dealing with NaCl deficiency; otherwise, the basis is KCl deficiency. Finding metabolic acidosis with a normal plasma anion gap indicates loss of NaHCO3 or KHCO3. If the ECF volume is not contracted, a normal or high plasma osmolality suggests ECF solute gain (glucose, mannitol); otherwise, suspect a loss of K+ salts from the ICF compartment. A KCl deficit with a shift of H+ into cells is the cause if metabolic alkalosis is present; otherwise, there is a loss of K+ plus organic phosphate (a catabolic state). In our accompanying manuscript (13), most of the patients undergoing CAPD had hyponatremia without weight gain, suggesting a catabolic state.
Advantages and Disadvantages
Our approach to the patient with hyponatremia was designed to permit a better understanding of its pathophysiology. Nevertheless, it has significant shortcomings when viewed strictly as a clinical tool. First, only a single cause for hyponatremia was considered for each example. Second, one rarely has accurate weights before and after the hyponatremia developed. Third, it is difficult to determine the ECF volume with accuracy at the bedside (16). Nevertheless, in a population of patients, such as those on CAPD, for whom one does have documented weight loss and reasonable estimates of ECF volume, these physiological principles can help the clinician understand the basis of hyponatremia and suggest guidelines for its therapy (13).
Appendix: Sample Calculation
Consider a patient who weighs 70 kg and has 40 L of body water (14). This water is distributed as 24 L of intracellular fluid (ICF) (60% of 40 L) and 16 L of extracellular fluid (ECF) (40% of 40 L). There are 2240 mmol of Na+ in the normal ECF volume (140 mmol/L x 16 L). With a deficit of 400 mmol of Na+ and 400 mmol of chloride, the new “effective osmolality” would be 260 mOsm/kg H2O [40 L x 280 mOsm/L (excluding urea and glucose), or 11 200 mmol minus the 800 mOsm of Na+ + Cl− that were lost, divided by 40 L]. The resulting ECF volume would be 14.15 L: [(16 L x 280 mOsm/L, or 4480 mOsm) – 800 mOsm]/260 mOsm/L. Therefore, the ECF volume is contracted by 1.85 L, the plasma Na+ concentration would be 130 mmol/L, and the ICF volume would be expanded by 1.85 L.