
Abstract

Long-term patency and improved cost effectiveness have been associated with the early placement of vascular access in prospective hemodialysis (HD) patients approaching end-stage renal disease (ESRD) (1). Conversely, pre-ESRD patients desiring peritoneal dialysis (PD) have peritoneal access withheld until a few weeks prior to the anticipated need for PD. While optimal timing would allow this practice to succeed, recognition of the need to initiate dialysis is, at times, delayed. This can result in more costly, urgent interventions, including placement of temporary vascular access (HDC) for treatment with HD. In our experience, this patient frequently never makes the transition to PD.
In 1993, Moncrief et al. described a technique whereby PD catheters (PDCs) implanted subcutaneously remained buried for 6 – 8 weeks prior to anticipated need for PD (2). Reduced infections, improved PDC longevity, and lower cost have been demonstrated with this technique (3). This methodology also allows nephrologists and their patients a larger window of time during which to consider initiation of dialysis. We queried whether time of placement to explantation of buried PDCs could be extended for longer than 6 – 8 weeks to provide an even larger window during which to prepare patients for dialysis.
Methods
Twelve pre-ESRD patients having residual renal function between 12 and 15 cc/minute creatinine clearance, determined by 24-hour urine collection and/or the Cockroft–Gault formula, were included in the study. Peritoneal dialysis catheters were placed in the usual fashion (2) and remained buried until need for dialysis, characterized by uremic symptoms plus creatinine clearance less than or equal to 10 cc/minute. The implanting surgeon then explanted the PDC. Prolonged hibernation was defined as a PDC remaining buried for at least 3 months.
Thirty-five pre-ESRD patients were followed prospectively by their nephrologist until residual renal function was less than 12 cc/minute and/or the development of overt uremic symptoms. A PDC was then placed in the usual way, with intent to begin PD 3 – 6 weeks after catheter placement.
Successful PDC flow was defined as unimpeded inflow/outflow of PD fluid. Impaired flow resulted in an abdominal x ray to determine PDC malposition or constipation. In the absence of these problems, obstruction of the PDC with fibrin was presumed and treated with urokinase 75 000 U in 40 cc normal saline, instilled into the PDC. After a 60-minute dwell, PDC function was reassessed. If successful, the procedure was repeated over the next 4 days. If urokinase was unavailable or unsuccessful, laparoscopic repositioning (LSR) was employed to establish PDC function. Usual PDC care was then employed for all patients. Patients were followed until PDC failure, transplantation, change to HD, or death. Exit-site (ES) infection and peritonitis rates were defined as the number of episodes per 100 patient-dialysis months. Positive ES culture and the presence of ES erythema, tenderness, or purulent drainage defined ES infection. Peritonitis was defined by the presence of cloudy PD fluid and greater than or equal to 100 white blood cells/mL, with 50% or more polymorphonuclear leukocytes. Immediate complication and PDC-related infection rates were compared using two-tailed Fisher's exact test. Relative risks and rates are expressed with 95% confidence intervals. Statistical significance corresponds to a p value of 0.0125 or less.
Results
Clinical features of the 12 patients with prolonged PDC hibernation are shown in Table 1. Average time of PDC hibernation was 9.2 months. Eight of the 12 PDCs functioned immediately after explantation, and 4 (Patients 2, 5, 7, and 9) did not drain after initial inflow. Patients 5 and 9 underwent LSR of the PDC, resulting in free flow of PD fluid. Hemodialysis via a HDC supported Patient 5 until this could be done. Urokinase infusion successfully restored function in the other two PDCs. Because of continued sluggish outflow, PDC LSR ensued in Patient 7, restoring function.
Demographics and Catheter History of 12 Patients with Prolonged Subcutaneous Catheter Hibernation
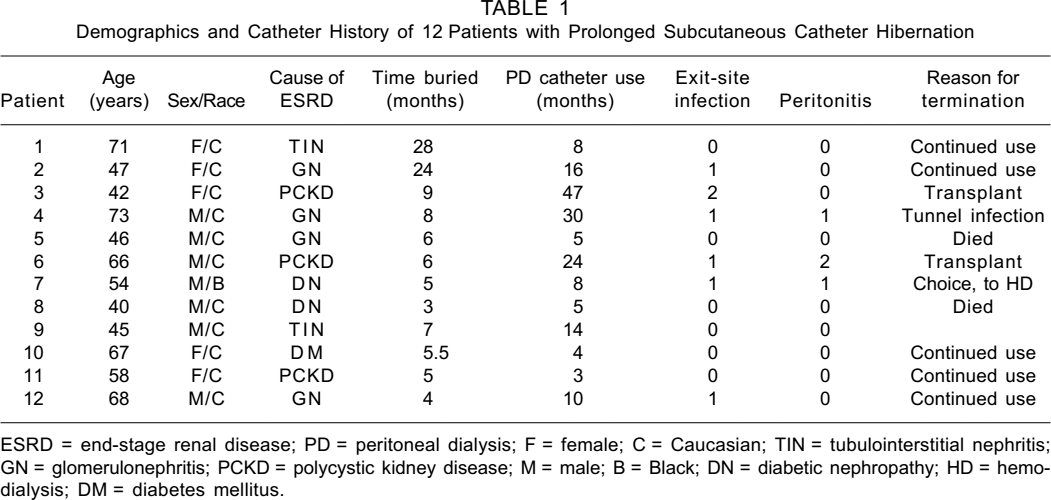
ESRD = end-stage renal disease; PD = peritoneal dialysis; F = female; C = Caucasian; TIN = tubulointerstitial nephritis; GN = glomerulonephritis; PCKD = polycystic kidney disease; M = male; B = Black; DN = diabetic nephropathy; HD = hemodialysis; DM = diabetes mellitus.
Four of the routinely placed PDCs were nonfunctional (Table 2), three of which were ultimately lost to HD. One patient requested maintenance HD after her PDC failed to respond to urokinase infusion in the face of uremic symptoms. Another patient requested maintenance HD after continued PDC dysfunction despite LSR and urokinase infusion. The third patient underwent two unsuccessful LSR procedures to free the PDC of obstructing fibrin. Peritoneal dialysis catheter patency was established in the fourth patient after LSR. Three of the 35 patients also experienced leakage from the ES, mandating delay in PDC use and backup HD. In total, 4 of the 35 patients required backup HD for immediate PDC problems, compared to 1 of 12 patients with extended PDC hibernation. There was no significant difference in immediate PDC function between groups.
Immediate and Long-Term Complications of Hibernated and Nonhibernated Peritoneal Dialysis Catheters
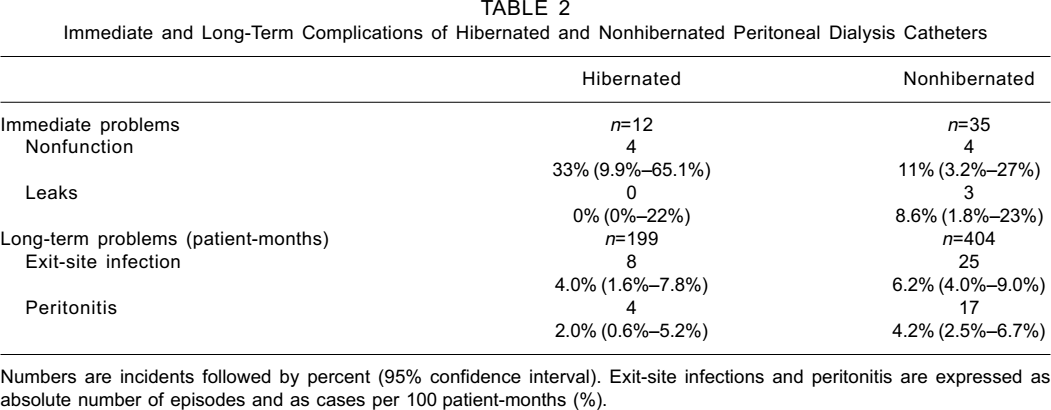
Numbers are incidents followed by percent (95% confidence interval). Exit-site infections and peritonitis are expressed as absolute number of episodes and as cases per 100 patient-months (%).
As 3 of the 35 patients with routinely placed PDCs never underwent PD due to catheter malfunction, infection assessment was performed only on the remaining 32. Median time of PDC use in these 32 patients was 8.5 months, compared to 9 months in the 12 patients with prolonged PDC hibernation. Infection rate was lower in the latter group, but this was not statistically significant (Table 2). There was no statistical difference in patient demographics between the two PDC groups with respect to time on dialysis, age, sex, race, or cause of ESRD.
Discussion
Delayed PDC placement can result in a need for temporary HDCs and HD, delay in dialysis initiation, or premature use of PDCs. The latter can lead to leakage from incomplete pericuff healing, early bacterial colonization, and subsequent infection. Such complications were seen with greater frequency in our group of routinely placed PDCs. Previous studies suggest that allowing PDCs to remain buried for periods up to 6 – 8 weeks improves PDC overall outcome (3). Our data suggest that this time period can be safely extended beyond 8 weeks. While not reaching statistical significance, prolonged hibernation resulted in a lower incidence of infection, lesser need for temporary HD, and no immediate loss of patients to long-term HD. These factors, coupled with less than ideal follow-up of pre-ESRD patients and imperfect methods of predicting the cadence of renal loss, make early PDC placement and prolonged subcutaneous hibernation an approach that deserves expanded consideration.